Eating Disorders
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
What eating disorders are in the DSM?
Anorexia Nervosa (AN)
Bulimia Nervosa (BN)
Binge Eating Disorder (BED)
Other Specified Feeding or Eating Disorder (OSFED)
Atypical anorexia
Purging Disorder
Subthreshold BN or BED
Avoidant/Restrictive Food Intake Disorder (ARFID)
Rumination Disorder
Pica
What is criterion A for anorexia nervosa (AN)?
Restriction of energy intake, leading to significantly low body weight in the context of age, sex, developmental trajectory, and physical health...
What characterizes low body weight?
BMI<17; subject to clinician.
What would qualify for an atypical anorexia diagnosis instead of anorexia nervosa?
Potentially, someone that meets the other criterion for AN, but their BMI is too high (don't meet criteria A).
* This is especially common for youth that had a previous "overweight" status
What is criterion B for anorexia nervosa (AN)?
Intense fear of gaining weight (doesn't go away even after losing weight) or becoming fat OR persistent behavior that interferes with weight gain, even though at a significantly low weight
True/False: a lot of people won't acknowledge they fear weight gain
True
What is criterion C for anorexia nervosa (AN)?
Disturbance in way in which one's body weight/shape is experienced (distribution of weight), OR undue influence of body weight or shape on self-evaluation (effect on self-esteem), OR persistent lack of recognition of seriousness of low weight
What are the subtypes of anorexia nervosa (AN)?
Resitrictive type and Binge-eating/purging type
What would be some examples of purging?
misuse of laxatives
self induced vomitting
restricting insulin from self
What is the prevalence rate of Anorexia Nervosa?
less than 1% lifetime prevalence
True/False: Anorexia Nervosa is not egosyntonic (acceptable to the individual)
False
For Anorexia Nervosa, how are patients often brought into treatment?
By family members or legal guardians
What are the psychological features of one with Anorexia Nervosa?
obsessive-compulsive (could be related to food): hoarding cookbooks, increased perfectionism, black/white thinking.
Depressive symptoms
True/False: There are high rates of suicide among individuals with Anorexia Nervosa (AN)
True
What did the Minnesota Starvation Study (1944-5) look at?
What is the impact of low body weight on physiological processes and psychology? + how to properly gain weight back
How did the Minnesota Starvation Study (1944-5) get participants? How many people were in the sample?
Offered participation as an alternative to military combat services for conscientious objectors
Sample included 36 males of good physical and mental health
What was the protocol for the Minnesota Starvation Study (1944-5)
- 3 months (baseline): observations of daily life
- 3200 kcal/day
- 6 months (semi-starvation)
- 1570 kcal/day
- Goal was to lose ~25% of body weight-> most if not all attained
- walk 22 miles/day
this
- 3-5 months nutritional rehabilitation
- 3 months: 2000-3200 kcal/day
- 8 weeks: Subgroup remained under study without calorie requirements-- ate 7000-10,000 kcal/day in first 2 weeks
What symptoms were seen during the study?
Eating Behavior Changes
- Increase in food preoccupation
- Toying with food, eating slowly
- During rehabilitation phase, many engaged in BE
Depressive symptoms
- Fatigue
- Irritability
- Low mood & apathy
- Social isolation
- Reduced sex drive
- Increased anxiety
Cognitive changes
- Self-reported decreases in mental ability
- No impact on cognitive testing
What is the Family-Based Therapy (FBT)/Maudsley Method?
Phase 1: Weight restoration
- family controls meals
Phase 2: Progressively returning control of eating over to the patient
- Only once back to "normal weight"
Phase 3: Establishing identity
- return to balanced life
True/False: Medication is helpful in treating Anorexia Nervosa (AN)
False
What does full remission vs. partial remission look like for someone experiencing anorexia nervosa?
full: no longer experiecing symptoms
partial: criterion A not met for sustained period
What does the cycle of bulimia look like?
A. Recurrent episodes of BE
B. Recurrent compensatory behaviors
C. Frequency (i.e., 1x/week over 3 months)
D. Self-evaluation based on body shape/weight
What does binge eating (BE) look like?
I. Eating, in a discrete period of time, an amount of food that is definitely larger than what most individuals would eat in a similar period of time under similar circumstances
II. Lack of control over eating during the episode
What is the prevalence rate of bulimia nervosa?
below 2%; mostly women
True/False: Bulimia Nervosa (BN) is egosyntonic
False, BN is egodysyntonic (they want to receive treatment)
What is the largest difference between anorexia and bulimia?
A. Patients with AN are underweight, patients with BN are not
B. Patients with BN binge eat, patients with AN do not
C. Patients with AN compensate, patients with BN do not
A
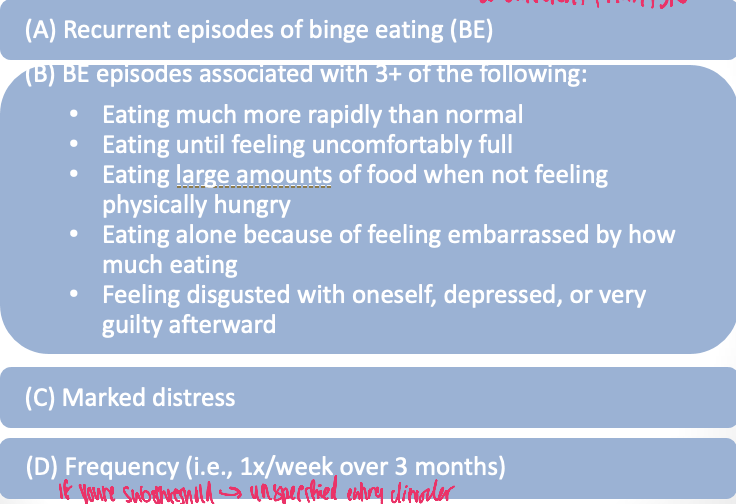
What are the diagnostic criteria for Binge-Eating Disorder (BED)?
How is BED different than other ED’s
More common
More equitable across genders
No compensatory behaviors
Linked with obesity
What does treatment for BN and BED look like?
Psychotherapies
Enhanced Cognitive Behavioral Therapy (CBT-E)
Interpersonal Psychotherapy (IPT)
Family-Based Therapy (FBT)
Dialectical Behavior Therapy (DBT)
Medications
Prozac is the only SSRI FDA approved for BN
Vyvanse is the first medication FDA approved to treat BED
Behavioral weight loss
Is AN, BN, or BED heritable?
AN heritability estimates as high as 74%
BN heritability estimates ranging from 54 and 83%
BED heritability estimates ranging from 41% to 57%
How does brain function differ in Anorexia Nervosa (AN) vs Bulimia Nervosa (BN) and Binge Eating Disorder (BED)?
AN (Anorexia Nervosa):
↓ Reward response to food → food less motivating
↑ Emotional response to body image
↑ Inhibitory control → strong self-control
↑ Rigidity & habit learning → strict routines
👉 Leads to restriction
BN & BED:
↑ Reward response to food → food highly motivating
↓ Inhibitory control → difficulty stopping
↑ Emotional response to body image (especially BN)
👉 Leads to binge eating (and purging in BN)
AN = “Less reward, more control”
BN/BED = “More reward, less control”
What makes a substance addictive?
Processing naturally occurring substances potency and quick absorption
UPFs trigger fast, large spikes in blood sugar.
There is heterogeneity in “addictive” substances:
Some are intoxicating
Some have potentially fatal withdrawal symptoms
Some are consumed in discrete binges
Some are legal
What impact has the global pandemic had on EDs
Increase in reported cases and healthcare utilization
Stressors → heighten risk
Social isolation
Routine disruption
Access to services
Loss of control