5012 Theory 2: Post midterm
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
Describe anatomy of aortic valve (4 components)
Annulus: provides structural support to cusps
Cusps: 3 half-moon (semilunar) in shape; right, left, non-coronary
Commissures: where the cusps come together
Interleaflet triangles: extensions of the ventricular outflow tract
Describe anatomy of aortic root/ Sinuses of Valsalva, includes 4 components
section between the LVOT and Asc. Ao
specifically the inferior attachment of the aortic cusps to the ST junction
Includes:
aortic cusps
Sinuses of Valsalva
Comissures
Interleaflet triangles
Differentiate aortic valve stenosis from sclerosis
Aortic Stenosis: reduced (restricted) opening of the aortic valve in systole via calcium build up over time
valve appears brighter than normal, does not open well, has velocity over 2.5 m/s
Aortic Sclerosis: thickening of the valve leaflets with no restriction of blood flow
valve appears brighter than normal, still opens well, has velocity less than 2.5 m/s
Describe pathology causes of aortic stenosis (3) and how common
1) Congenital: roughly 30-40% of cases
2) Acquired: Calcific: > 50% of cases
3) Acquired: Rheumatic: <10% of cases
What are some specific details of congenital AS?
bicuspid aortic valve is most common causes of AS in <50 yros, not all bicuspids will be stenotic
unicuspid (discovered at birth) or quadricuspid aortic valve
subvalvular or supravalvular stenosis is most rare
What are some specific details of calcific AS?
acquired, most common cause of AS in elderly
calcium deposits build up on the valve over time preventing normal opening in systole
“chunks” of brightness (calcium) seen, uneven brightness
commissural fusion common absent
MAC and CAD commonly associated
What are some specific details of rheumatic AS?
complication of strep throat → occurs years after acute rheumatic fever
often co-exist with mitral stenosis
scar tissue forms on the valve, which narrows opening
scar tissue creates rough surface where calcium deposits can collect
chronic inflammation → thickening & calcification/ stiffness
commissural fusion → triangular systolic orifice
slightly brighter than normal, uniformly thickened leaflets
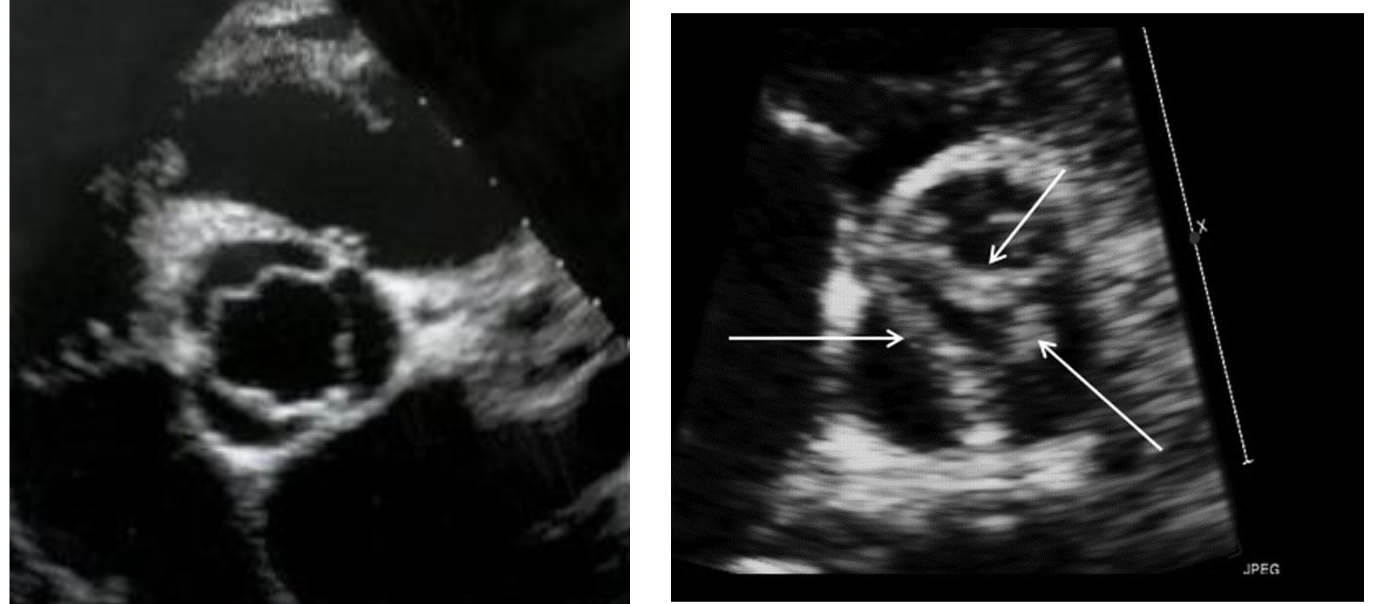
What are the 2 types of congenital bicuspid aortic valves
Without a raphe
rare
cusps usually equal in size
With a raphe (seam/union)
common
most common location of raphe is between the RCC and LCC
cusps unequal in size
What part of cardiac cycle do you assess aortic valves?
Systole
What are the consequences of congenital bicuspid AoV? (4)
1) Aortic root dilation: higher risk for aortic aneurysm or dissections
2) Coarctation of aorta: narrowing in desc. ao
3) Supravalvular aortic stenosis
4) Ventricular septal defects
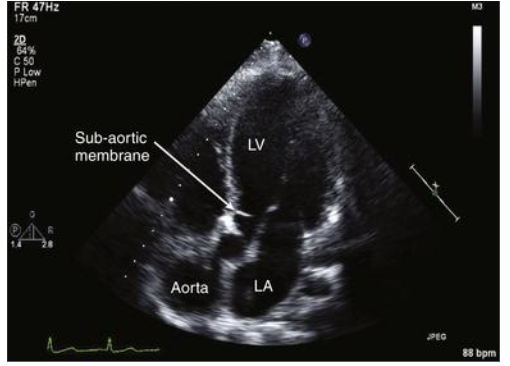
Describe congenital subvalvular stenosis
fibrous membrane or muscular ring in LVOT → obstruction in the outflow
Leads to: narrow LVOT → septal hypertrophy = thicker IVS → dynamic obstruction → mitral valve may get “sucked up”
dynamic because degree of stenosis varies depending on loading conditions
What is dynamic obstruction?
degree of stenosis varies depending on loading conditions, or variable blockage of blood flow instead of fixed narrowing
severity changes based on: cardiac cycle, HR, volume, movement of leaflets
Describe congenital supravalvular stenosis
uncommon
dysplasia of the aortic wall (hour glass type)
membrane with central orifice
hypoplasia of ascending aorta
Describe hemodynamic consequences of aortic stenosis (2)
Concentric LVH
narrowed AoV → increased pressure load → LV wall thickens to compensate (concentric LVH) → LV stiff + lower compliance
lead to diastolic dysfunction → LV does not relax well → poor filling
increased LAP → back into lungs → increase pulmonary pressures → SOB
Usually, normal EF, but will drop in severe cases
Ischemia
increased muscle mass due to LVH → increase oxygen demand
compressed coronary vessels due to LVH → decrease oxygen supply
angina: decrease oxygen → decrease LV contractility → systolic dysfunction
Big picture of the hemodynamics summary:
Pressure overload → LVH (thick)
Stiff ventricle → diastolic dysfunction → pulmonary congestion
Oxygen mismatch → ischemia (starved)→ possible systolic failure in late stages (weak, low EF)
List signs and symptoms of aortic stenosis (4)
Systolic Ejection Murmur (SEM)
can be diastolic, systolic, or both
most common, based on symptoms, timings of the murmurs
Angina- patient may have coexistent CAD
may be worsen by LVH
increased myocardial oxygen demand of LVH
decreased coronary artery perfusion pressure/perfusion time
Syncope (fainting)/ presyncope (feeling light-headed)
on exertion
caused by decreased cerebral perfusion
Shortness of breath and fatigue
insufficient oxygen supply
Describe treatment options for aortic stenosis
medical → alleviate symptoms
surgical/percutaneous → only definitive therapy
surgical: bioprosthetic /mechanical valve replacement
percutaneous: Trans Aortic Valve Implantation (TAVI)
Role of sonography in aortic stenosis (6)
determine presence of AS
differentiate between sclerosis vs stenosis
determine etiology
congenital or acquired (via age→ calcific or rheumatic)
assess LV wall thickness
wall thickness/LVH and AS= afterload problems
can lead to diastolic dysfunction, but patients have normal systolic function
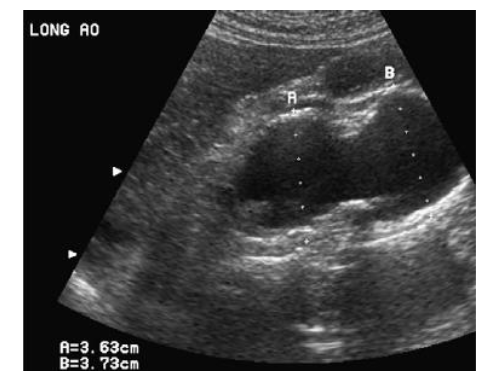
measure aorta
post-stenotic dilation, measure @ ED
be wary in biscuspid bc they have higher dilation and aneurysm risk
estimate severity of aortic stenosis
gradients, continuity equation, velocity ratio
identify associated lesions (regurgitation)
What are the 3 extra steps to assess AS (summary)
1) Use PEDOF probe in multiple windows to try to find the highest V through the valve
2) Mean Gradient and Peak V via CW trace of highest AoV velocity
3) Continuity equation (add on to step 2: PW LVOT trace, LVOT diameter) for machine to calculate AVA
How do we quantify the severity of disease in aortic valve stenosis?
Mean average gradients: different in pressure between LV and Ao in systole
Continuity equation: valve area
Velocity ratio: AS jet
What is the continuity principle? How is it related in normal vs stenotic valve?
states what flows in, must flow out
in normal valves: the velocity should be the same before and after the valve
in stenotic valves: blood will have to speed up to get through the valve due to narrowing
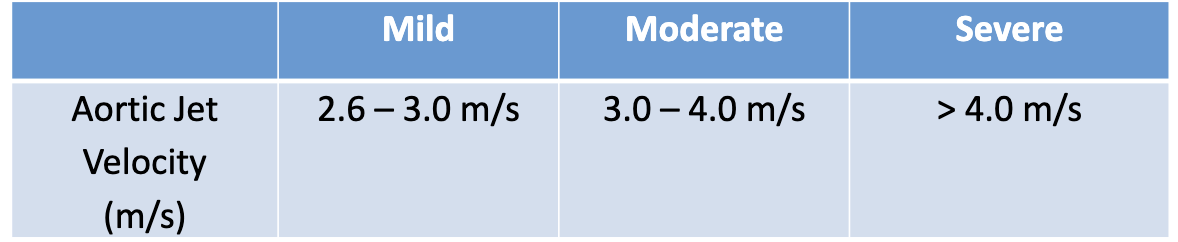
How to assess AS Jet velocity, what are normal values?
CW Doppler through maximum flow through AoV
Assess multiple windows, but only use highest velocity
PEDOF probe: when jet is > 3 m/s
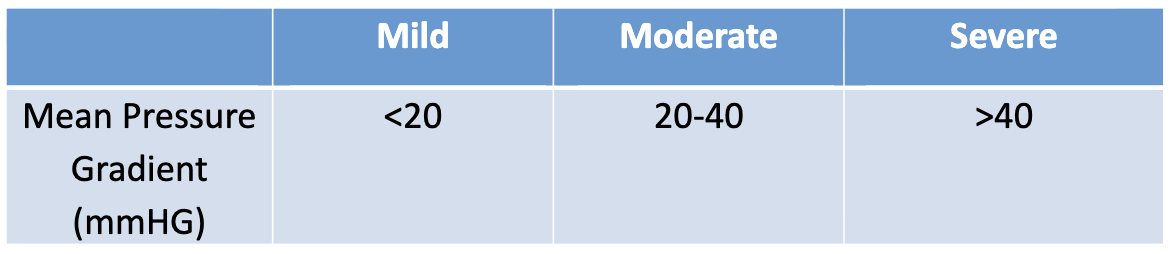
How to assess pressure mean gradient, what are normal values?
CW Doppler through maximum flow through AoV
trace around the CW Doppler spectral trace
machine automatically calculates mean pressure gradient between LV and Asc. Ao
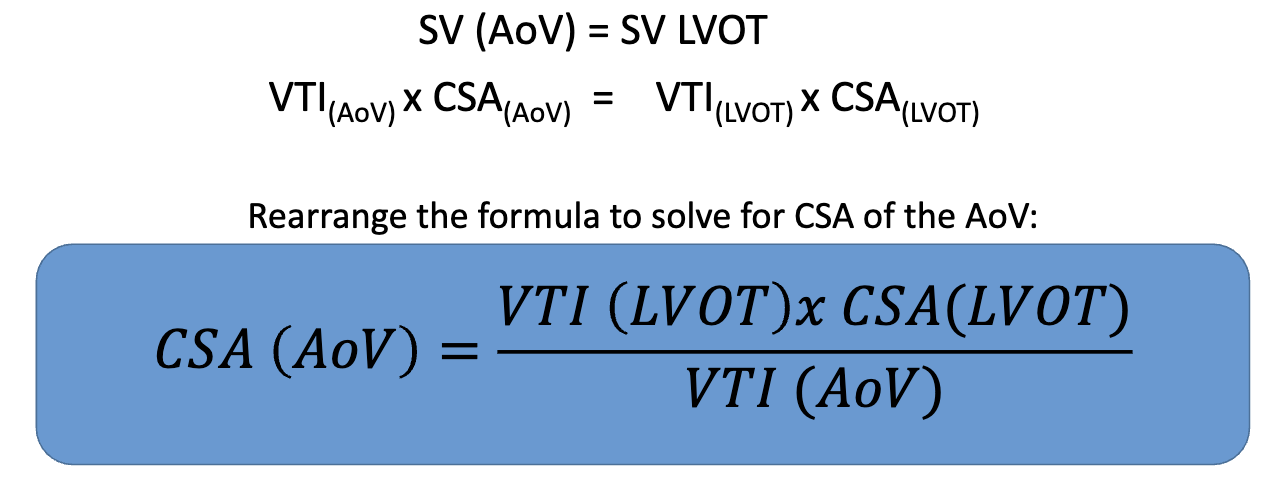
How to assess aortic valve area (AVA), what are normal values?
utilizes the continuity equation/principle
stroke volume of blood in LVOT must be the same as the stroke volume of blood in the AoV
Three measurements needed (any order, will auto calculate after all measurements)
AoV VTI: trace area under CW Doppler of AoV
through AoV, at max aliasing
LVOT VTI: trace area under PW Doppler of LVOT
0.5 cm proximal to AoV
CSA of LVOT: 2D of the LVOT diameter
zoom, inner-inner, MS, 0.3-1 cm inferior to AV cusp → CSA = πr²

What is VTI and why do we use it?
What: area under Doppler curve
Unit is cm because VTI = velocity/time
Why: In human body, velocity is not constant at any given time and varies at different parts of the vessel
VTI sums up all the individual velocities over time to find a representative overall velocity
Continuity Equation formula for AoV
Can you use continuity equation of AoV when there is LVOT obstruction?
no, bc equation compares normal flow to stenotic flow
with LVOT obstruction → velocity is already high in LVOT and the velocity in AoV will still be high since there was no time to slow down
Have to assess visually or perform a valve planimetry in SAX
What is 2D Planimetry of AVA
@ PSAX
trace opening in mid systole
not routinely performed due to many pitfalls
could be used to double check the AVA if clearly seen
What is dimensionless velocity ratio (DVI)?
removes error associated with LVOT diameter by removing CSA from the continuity equation
velocity ratio = VLVOT/ VAoV
smaller #s= severe, closer to 1= normal

What is the velocity profile and acceleration time (AT) in severe stenosis?
Normal valve:
short ejection time and acceleration time
blood flows easily into the ascending ao, hitting peak V quickly
looks like a shark tooth?
Aortic stenosis
longer ejection time and acceleration time
more rounded, symmetrical shape
hard to push blood into aorta, so everything takes longer
What are some specifications of PEDOF Probe
Known as: Pulsed Echo Doppler Flow aka pencil probe
non-imaging CW probe, only shown is Doppler trace
small footprint allows this probe to easily fit between small rib spaces
may be used for AS protocol, can be used anywhere but common in the right parasternal window (usually higher velocity)
Quantify severity of disease in the setting of supravalvular AS
extremely rare
not stenotic: attempt continuity equation with PW only (using multiple PW gates sampling until high velocity to prove the location)
AoV PW in sinuses of valsalva, prior to the supravalvular stenotic area
use values for max V, mean gradient, and continuity equation
then:
place CW through stenosis area
document mean, max gradient, and max velocity in asc, ao
indicate valve itself is normal
show stenosis in 2D and explain why there is an increase in velocity
Quantify severity of disease in the setting of dynamic subvalvular obstruction
continuity equation and peak/mean gradients will not work (bc high velocity in LVOT)
assess 2D AoV, esp PSAX
grade based on 2D images
some sits may as for planimetry
record mean and peak gradients through LVOT
use PW if possible, but may be forced to use CW
clearly indicate on report that high gradients are from the LVOT and not AoV
assess health on 2D images
Quantify severity of disease in the setting of low output AS
defined as valve area < 1.0 cm² with an aortic velocity < 4.0 m/s or pressure gradient < 40 mmHg, and a poor EF
stenotic AoV, but normalish velocity through valve
significantly reduced EF → little blood pushed through valve → low velocities and pressure gradients through valve
What is aortic insufficiency (AI) / aortic regurgitation (AR) ?
inability of the aortic valve leaflets to remain closed during diastole
results in portion of the left ventricular stroke volume leaking back from the aorta into the left ventricle
added volume of regurgitant blood produces an increase in left ventricular end-diastolic volume
aortic regurgitation occurs in diastole and includes both isovolumetric periods
List the common etiologies of AI/AR (4)
aortic annulus/ aortic root dilation
cusp abnormalities
loss of aortic cusp (commissural) support
What is aortic annulus/ aortic root dilations? What are the main causes (5+3 sub)
aortic root dilatations prevent normal leaflet coaptation → unable to close normally in diastole
causes include:
congenital conditions:
bicuspid AoV
Marfan synfrom
Ehlers-Danlos/ Loeys-Dietz syndromes
aortic stenosis (turbulent flow in Asc. ao)
atherosclerosis
untreated infection
trauma → dissections cause leakage
What is Marfan syndrome (congenital, aortic root dilation)? Characteristics (5)?
most common systemic connective tissue disease (genetic) → leaky connective tissue
fault connective tissue weakens blood vessels
characteristics of Marfan syndrome are:
tall/scoliosis/hypermobility of joints
high palate/poor vision/long limbs
mitral valve prolapse (60% of cases)
dilatation of Asc Ao/ dissection
AR due to dilation of aortic root
What is bicuspid AoV related to congenital, aortic root dilation?
just more susceptible to dilation and aneurysm
inherently different→ need to assess well in Asc Ao
Difference between dilation and aneurysm
Aortic aneurysm:
dilatation involving all layers of the aorta 1.5x greater than normal diameter
Aortic dilatation:
diltation involving all layers of the aorta, larger than accepted normal values, but not large enough to be considered an aneurysm
Operation on an aneurysm @ the following levels:
normal patient: 55 mm
bicuspid AoV: 50 mm
Marfan syndrome: 45 mm
OR if growth of aorta is >0.5 cm per year
What are reasons for cusp abnormalities (4)
rheumatic fever
calcific changes
calcium can block complete closure of the valve
infective endocarditis
bacteria on valve
bicuspid/quadricuspid
quad more associated with AI than AS
What are reasons for loss of aortic cusp (commissural) support? (3)
ventricular septal defects (holes/shunts)
aortic dissection
trauma
Whats are some causes of acute vs chronic AI?
causes of acute AI:
trauma
dissection
infective endocarditis
causes of chronic AI:
bicuspid AoV
rheumatic AoV
calcific AoV
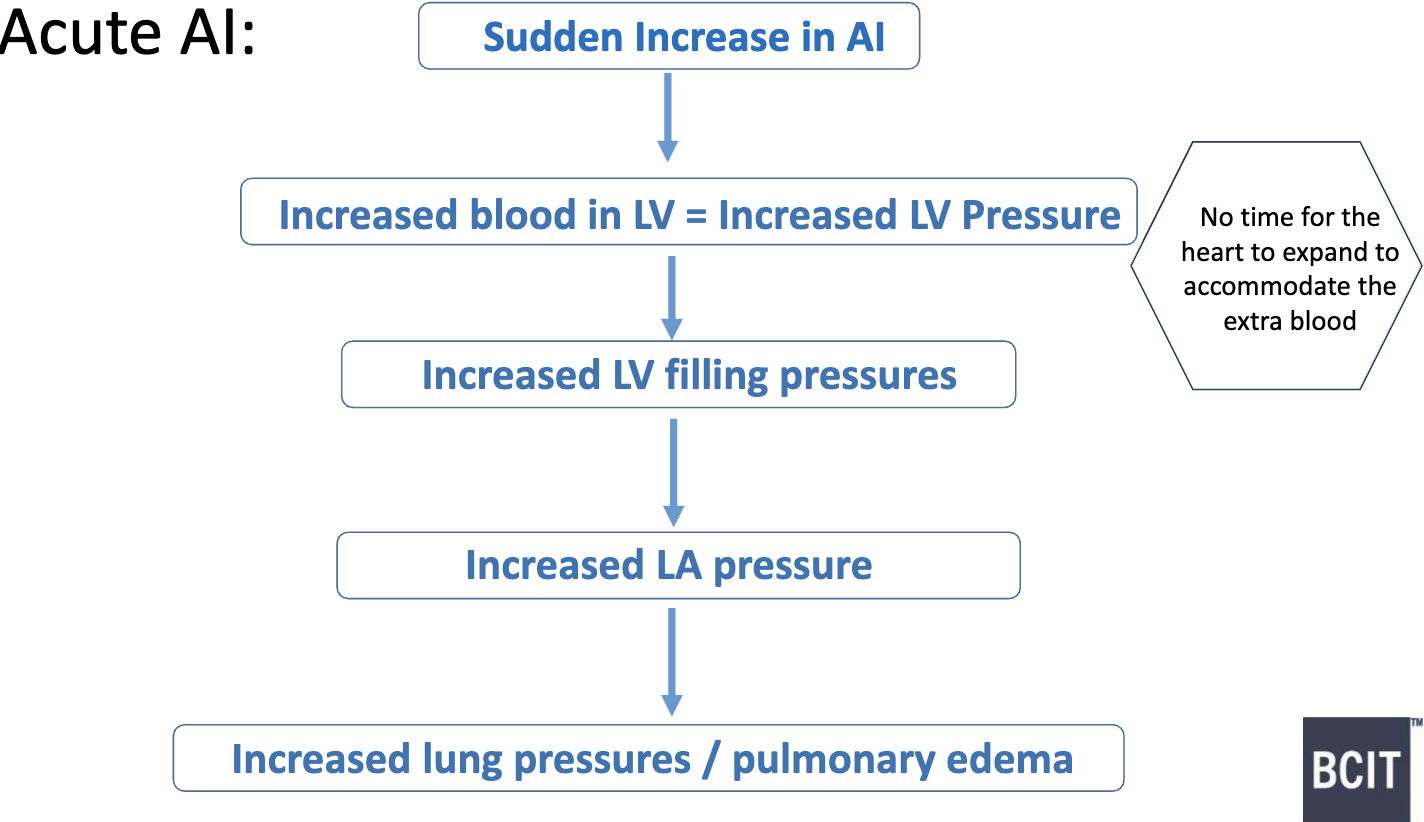
What are some hemodynamic consequences for Acute AI?
if severe enough → medical emergency & immediate valve replacement needed
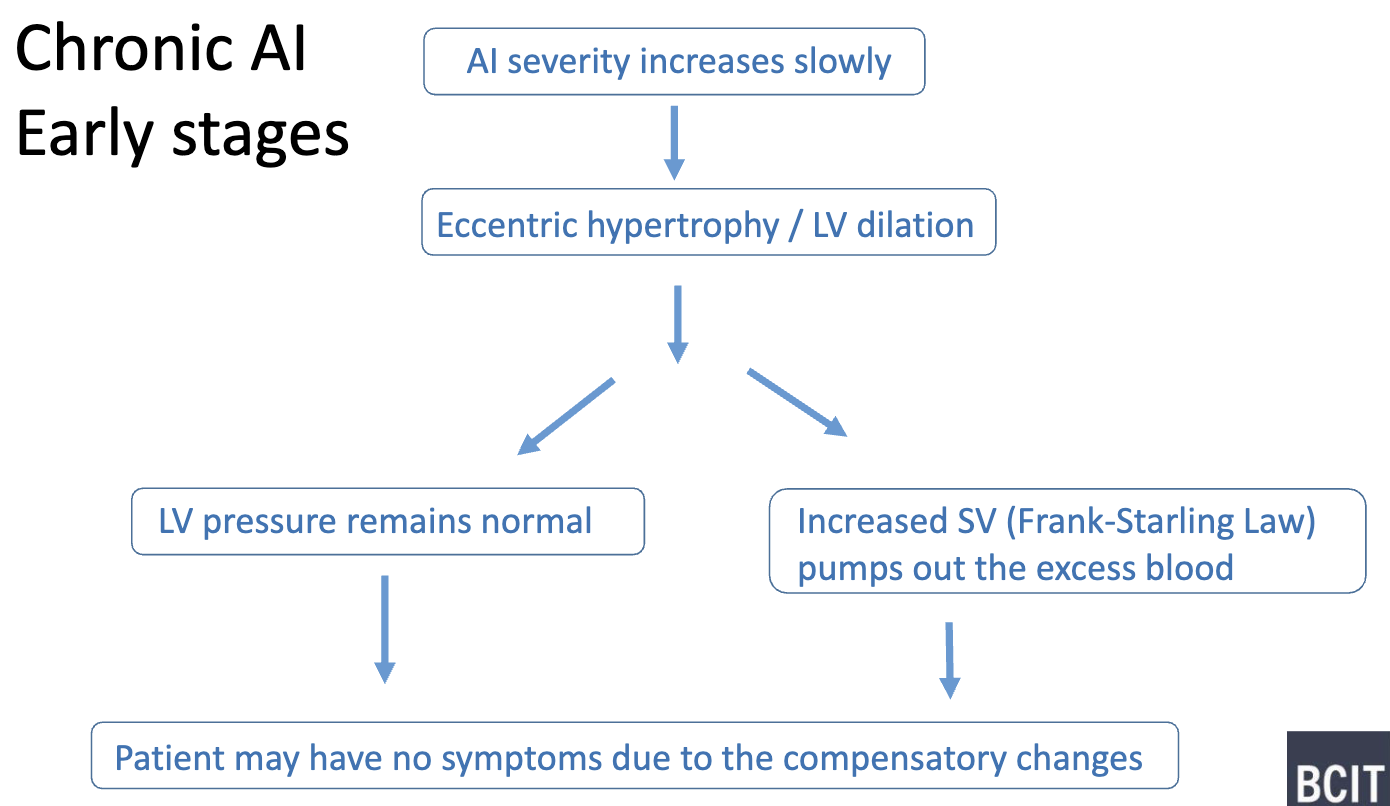
What are some hemodynamic consequences for Chronic AI- early stages?
eccentric hypertrophy/ LA dilation also help reduce wall stress (LaPlace’s Law)
note: LV pressure may remain normal without changing SV too → patient asymptomatic
EF remain normal
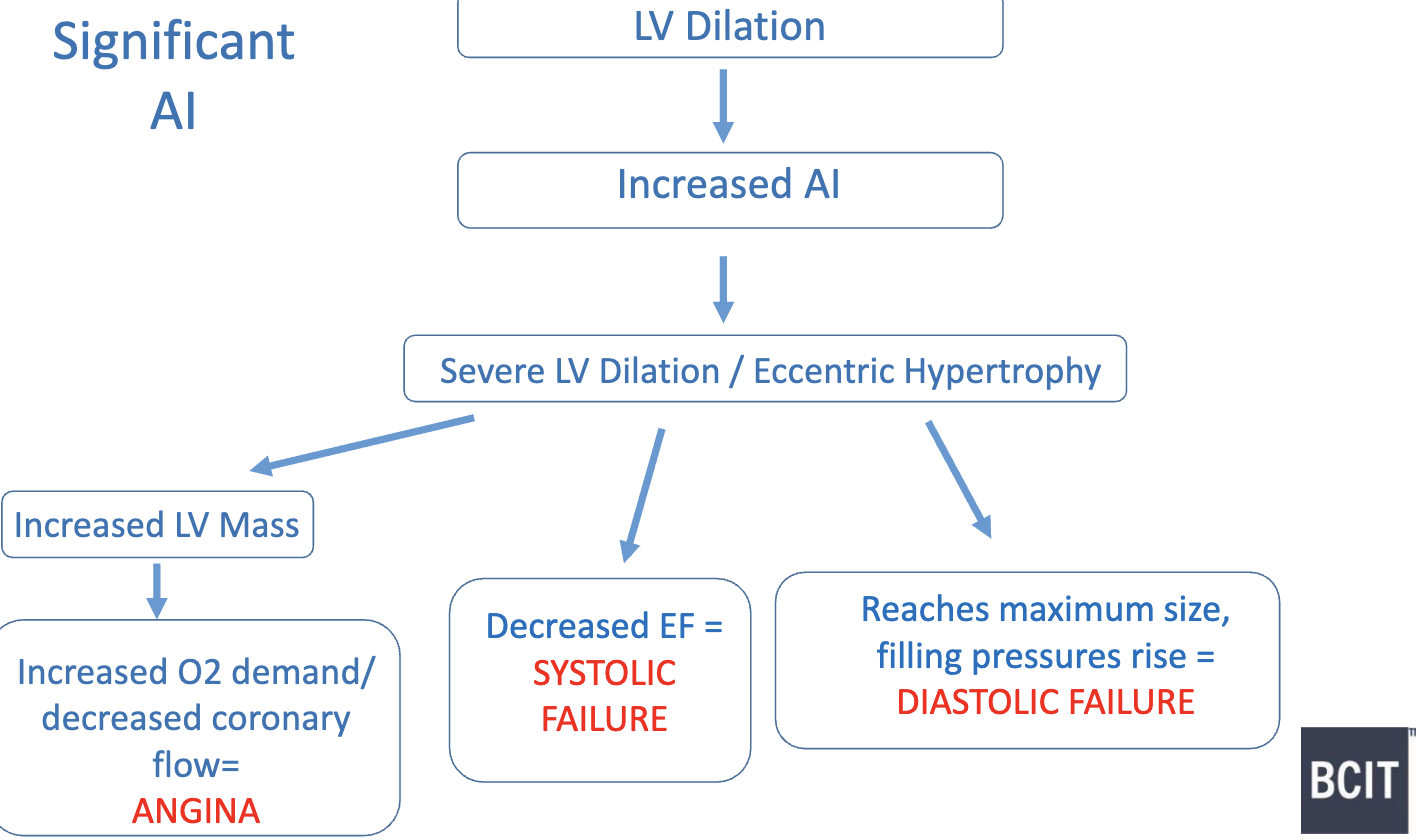
What are some hemodynamic consequences for Chronic AI- long standing?
as LV dilates more:
myofibrils pass their optimal length and contractility decreases → EF decreases and eventually patient goes into systolic heart failure
pericardium reaches max size, cannot accommodate excess blood → LV filling pressure increase → diastolic heart failure