Respiratory: Common Cold
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
Common Cold
Self-Limiting Viral Infection of Upper Respiratory Tract
Typical Season: August to April
Pathophysiology
Increased Susceptibility
Crowded classrooms/daycare, weakened immune system, smoking, allergies, chronic stress, sleep deprivation
Viral Transmission
self-inoculation (hands) and/or inanimate objects (ex: door knobs)
Mechanism of Infection
Peak ~2 to 4 days
Present in Nasopharynx
~16 to 18 days
Pathophysiology of Mechanism of Infection
Virus binds to intercellular respiratory epithelium
Replication
Virus Spreads (peak ~2 to 4 days after inoculation)
Anti-Viral Treatment
none for common cold
Clinical Presentation
Rhinoviruses (most common cause in adults and children)
Start 1-3 days after infection
Symptoms
Nasal congestion, rhinorrhea, sneezing, low-grade fever, headaches, malaise
Nasal Symptoms
1. Clear, thin/watery secretions
2. Thick, yellow/green secretion
3. Clear, thin/watery secretions again
Predictable Sequence
Sore Throat - Nasal Symptoms (Day 2-3) - Cough (Day 4-5)
Complications (Uncommon)
Sinusitis
Middle ear infection
Bronchitis
Pneumonia
Asthma/COPD exacerbations
Treatment Goals
Reduce symptoms
Rest and adequate fluid intake
Prevent transmission
Stay home
Wash hands
Treatment Approach
No cure
No antibiotic use
Ineffective against viruses
Non-pharmacologic
Mainstay
Symptom specific treatment
Use of single ingredient products preferred
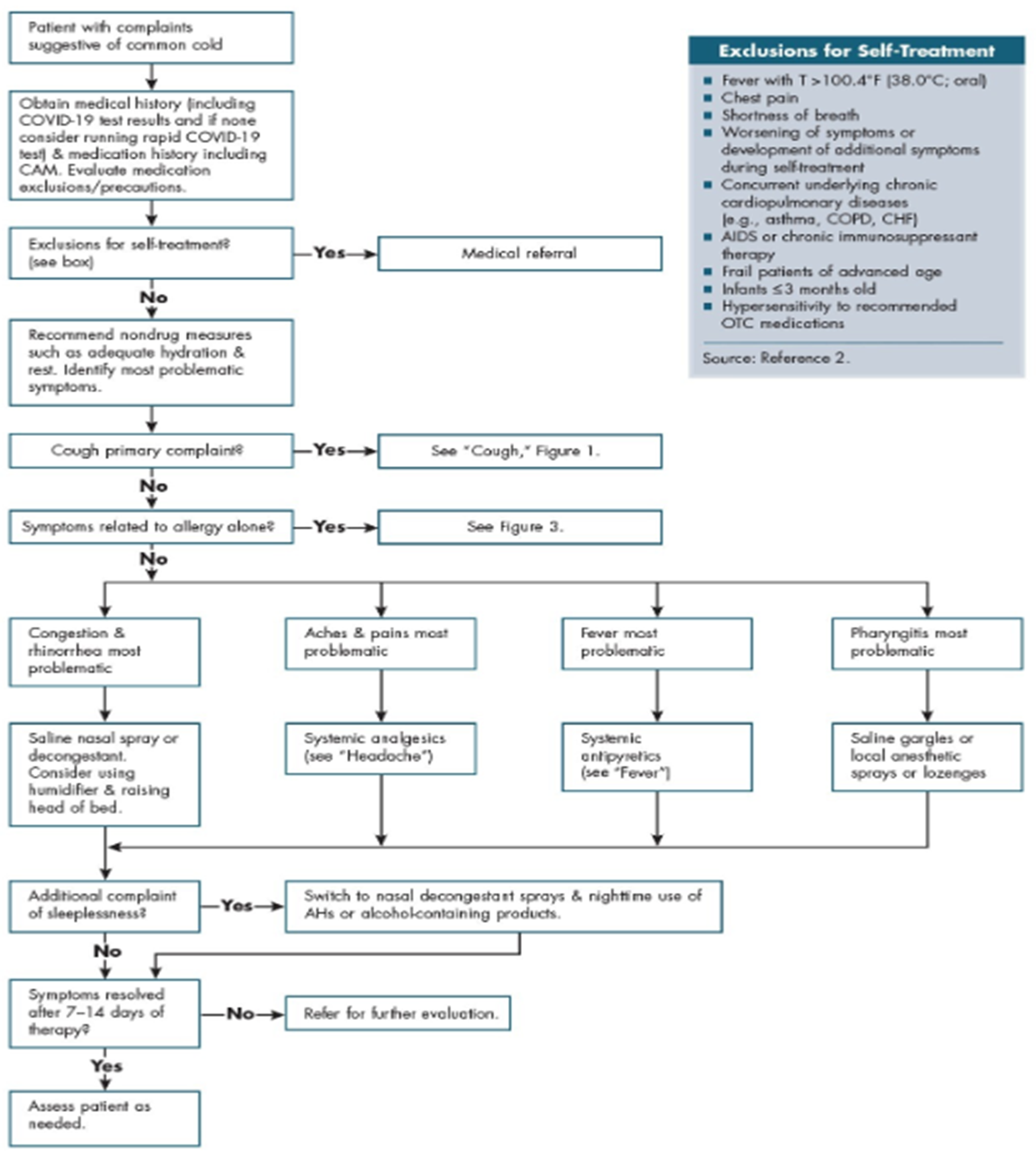
Exclusions for Self-Treatment
Fever (Temperature >100.4)
Chest Pain
Shortness of Breath
Worsening of Symptoms or Developmental of Additional Symptoms During Self-Treatment
Concurrent Underlying Chronic Cardiopulmonary Disease
AIDS or Chronic Immunosuppressant Therapy
Frail Patients of Advanced Age
Infants < 3 months old
Hypersensitivity to Recommended OTC Medications
Always Recommend
Non-Drug Measures (such as adequate hydration and rest)
Table Path and Exclusions
Non-Pharmacologic Therapy (Mainstay of Treatment)
Increased fluid intake
Adequate rest
Nutritious diet
Chicken soup
Lemon with honey
Increased humidification or vaporization
Proper hand hygiene
Saline gargle
Nasal irrigation
NETI Pot
Helps w/ congestion
Caution When Making
Use Boiled Water (get rid of brain-eating amoebas) and Allow to Cool
Tonicity: Want Isotonic (0.9% Saline or NS)
Pharmacologic Therapy
Decongestants (nasal/eustachian tube congestion)
Antihistamines (rhinorrhea/sneezing, allergic rhinitis)
Local anesthetics (pharyngitis)
Systemic analgesics (fever, pain)
Antitussives and protussives (cough)
Combination products
Systemic Decongestants
Pseudoephedrine (best)
Phenylephrine
Pseudoephedrine
Behind the counter, works much better than phenylephrine
Schedule C-V in some states (purchaser must show valid ID)
Limit 3.6 g per day and 9 g per month
Largely being replaced by phenylephrine
Main Ingredient of Methamphetamine (potential to make meth)
Phenylephrine
Does not work very well, may be removed from market (FDA in the process of proposing removal from the market due to studies showing ineffectiveness)
Direct Action
Phenylephrine, Oxymetazoline, and Tetrahyrdozoline
Indirect Action
Ephedrine
Mixed of Direct and Indirect Action
Pseudoephedrine
Decongestant Route of Administration
Systemic
phenylephrine, pseudoephedrine
Ophthalmic:
naphazoline, phenylephrine, oxymetazoline, and tetrahyrdozoline
Intranasal:
Short-acting: ephedrine, epinephrine, naphazoline (Privine), phenylephrine (Vicks Sinex), and tetrahyrdozoline
Long-acting: oxymetazoline (Afrin)
Decongestant Information
Indication: temporary relief of nasal and eustachian tube congestion
MOA: adrenergic agonist
Don’t use late at night (may keep up at night)
Decongestants: Adverse Reactions
Cardiovascular stimulation
Increased blood pressure, tachycardia, palpitations, arrhythmias
CNS stimulation
Restlessness, insomnia, anxiety, tremors, fear, hallucination
Rebound congestion
Rhinitis medicamentosa: if use longer than 3-5 days, can make congestion worse once medication is withdrawn
Limit: 3-5 day supply of intranasal decongestant
Decongestants: Systemic Overdose
Excess CNS stimulation
Cardiovascular Collapse
Shock
Coma
Decongestants: Warnings
May exacerbate disease sensitive to adrenergic stimulation (HTN, heart disease, diabetes, hyperthyroidism, etc.)
Patients with HTN should use decongestants only with medical advice
Antihistamines First-Generation
Are Sedating
Not Effective Alone Against Common Cold
Antihistamines Second Generation
Non-Sedating
Some find sedating
Not Effective Against Common Col
Sedating Antihistamine + Decongestant
Indicated for common cold
May decrease rhinorrhea and sneezing due to cold
sneezing and cough, and anticholinergic effect (runny nose)
Topical Local Anesthetics
Benzocaine & Glycerin: Throat Spray
Phenol: Throat spray
Benzocaine: Lozenges
Topical Local Anesthetics Information
Indication: temporary relief of sore throat
Dosage forms available: lozenges, sprays, or mouthwashes
Step above lozenges, contain active ingredient (API is to help numb the throat)
Aspirin-Containing Products Warning
Should Not Be Used in Children with Viral Illness - Reye’s Syndrome
Rate Limiting/Max Doses: Acetaminophen
3,000 to 3,250 mg Daily
Rate Limiting/Max Doses: Ibuprofen
1,200 mg
Antitussives for Colds Associated w/ Non-Productive Cough
Codeine and Dextromethorphan = Not Recommended (Questionable Efficacy in Cold)
Protussive = Not Proven Efficacious in Colds
Complimentary Products
Zinc
Vitamin C (Ascorbc Acid)
Oscillococcinum
Zinc
Theoretical MOA: blocks adhesion of rhinovirus to nasal epithelium and inhibits viral replication
Side effects: nausea, upset stomach, and bitter taste
Vitamin C (Ascorbc Acid)
Reduces duration of cold by 8% in adults and 14% in children
Ineffective for preventing colds in most people
Airborne
Oscillococcinum
Like treats like
Patient Encounter Questions
Detailed description of symptoms
Medical history and medication use
Current or previous self-treatment
Patient Encounter Counseling
Nondrug measures may be effective in relieving discomfort of cold symptoms
Products should be selected based on specific symptom(s)
Advise about proper use of medications
Duration of treatment
Adverse effects
Drug interactions
Cost
Explain signs and symptoms requiring further evaluation by PCP