SOC363 Quiz Flashcards
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
Sociology orientation of mental heath
Focused on how society shapes the thoughts, feelings, and actions of it’s members in ways that are considered to be mental illness (and mental health) and with the consequences of having or being thought to have a mental illness.
Not focused on the individual but on the macro and societal level of distress and mental illness.
Earliest example of sociology studies of mental illness
1920s study with Chicago and which sections had more or less cases of schizophrenia. Found that schizophrenia was more common in low SES regions.
Very segregated and each region has been separated by gerrymandering and redlining which is focused on SES and politics. Also could be because of less repairs, more far from the rest of towns, harder to stay in high SES areas, deviance and criminalization, lack of resources, stigmatization, job discrimination, more prone to illness which could lead to schizophrenia from prenatal disease.
Social causation
Environment causes a higher risk to risk factors.
Being laid off leads to distress and mental illness as a direct result.
Social selection
People that are at higher risk are pushed out and drift into certain circumstances
Ex. Being laid off leads people to drift into low income situations and as a result distress and mental illness.
Social constructionist perspective of mental illness
Mental health is relative and subjective. A way of controlling deviant behavior but can lead to ignoring suffering and inequality.
Ex. homosexuality was considered a mental illness in the past due to the subjective and relative idea at the time and became a way of controlling subjectively deviant behavior. This lead to suffering and inequality through discrimination against LGBTQ members which was ignored.
Biomedical perspective
Derived from understanding of physical health
Classify signs and symptoms into discrete categories.
More emphasis on individual causation and treatment but still no clear biological cause identities.
Why is the study of stress sociological according to Len Pearlin?
Stressful experiences don’t occur in a vacuum and typically can be traced back to surrounding social structures and people’s location within them.
These structures as most encompassing people, like stratification that cuts through societies, socioeconomic status, gender, and age.
To the extent these systems embody the unequal distribution of resources, opportunities and self regard, a low status within all of them may be stressful in life.
Disorder defintion
A diagnosed condition (based on criteria in DSM) existing in the individual.
A sign of dysfunction in some respect, like a cognitive, motivational, behavioral, emotional, or other psychological mechanisms.
Causing real harm to self or others, like distress, disability, impairment of function, and not due to social disapproval.
Horowitz characterization of disorders
A disproportionate response to external stress, though many in medical community also argue disorder is caused by internal dysfunction (ex. Due to genetics, brain damage, neurotransmitter issues, etc)
Horowitz definition of distress
“Normal” expectable and sanctioned responses to environmental challenges and threats.
Naturally self limiting (like a natural timeline of response to distress)
Sociological studies usually deal with exact kids of ‘expectable and sanctioned responses’ that the DSM excludes from its definition of mental disorder because they arise in response to social stressors and only persists as long as these stressful social conditions endure.
Wheatons definition of distress
Related to certain kids of disorders, but not all. On a continuum (scale), stable differences, and not “normal” or necessarily moderate
“Distress can be interpreted to refer to the extent of anxiety and depression symptomatology … indicating an affectively based impairment in … social functioning capacities. The range of impairment is probably from none through lower levels of severity; that range is sufficient to make the Langner Index useful as a proxy indicator of variation in the probability of … a diagnosis in the realm of anxiety and depression disorders.”
Historical approaches to measuring mental health
Revision to the DSM APA in 1970s and the first attempt to standardize the DSM.
The DSM III allowed for new population research on the prevalence of disorders because it provided specific criteria for assessing a disorder. The criteria could be coded into a question on a survey which could be administered by non-clinicians.
ECA and NCS / NCS-R followed
Epidemiological Catchment Area (ECA) Project
Robins and Regier 1991
Surveyed samples of the general population in 5 sites (New Haven, St. Louis, Baltimore, Los Angeles, rural North Carolina)
First time a standardized diagnostic instrument was used.
National Comorbidity Survey (NCS & NCS-R)
Kessler et al. 1994-2005
Focused on the degree to which different disorders appeared in the same individual
Applied a new instrument : CIDI (composite international diagnostic interview) for comorbidities.
ECA and NCS findings controversy
Across both surveys the rates seem too high
People didn’t want to believe that many people had mental disorders, so they questioned the legitimacy.
Despite the instruments being similar, the findings were significantly different… but there are reasons for this.
Prevalence defintion
The percentage of the population with a given disorder in given time period.
True prevalence of mental health over the year as an explanation to ECA and NCS findings
Before 1980s, studies were only based on data from clinical settings and, as such, did not measure true prevalence.
Clinical prevalence is based on counts of patients in treatment or in touch with health authorities, which introduces bias.
True prevalence is a measure of how many people have mental disorders, whether or not they seek/receive treatment.
Estimated 3:1 ratio of untreated cases to treated cases. Before 1980s we know very little about actual social patterns of mental health.
Why are prevalence rates different and difficult to compare across surveys?
They used different diagnostic systems : ECA and NCS
Employed different sampling strategies : ECA based on 5 sites, NCS and NCS-R based on national samples.
Changes in instrumentation and protocol : In the CIDI (used in the NCS and NCS-R) screening questions were at the beginning of the survey when there’s lower risk of denial. Computer assisted interviewing reduced error.
Validity
How well does a measurement tool, like a test, accurately measure what it intends to measure.
In this case, the ability to successfully distinguish between people who have mental disorders and those that do not.
Sensitivity detection cases
Ability to detect true cases, but could be under-diagnosiing.
Should not indicate that someone is mentally healthy when, in fact, they have a disorder (false negative)
Specificity detection case
Ability to exclude “true non-cases” while potentially over-diagnosing.
Should not indicate that someone has a disorder when they are mentally healthy (false positive).
Diagnostic interviews
Screen questions for a disorder and a unique set of defining symptoms for each disorder.
Exclusion criteria to Diagnostic Interviews
1) If you have this, you can’t have this
2) “Understandable” or “normal” explanation of responses, such as grief after a death, or physical illness, or a reaction to drugs.
Fundamental differences between disorder and distress
Disorder : after all the questions asked, criteria met are tallied to decide whether the person qualifies for a diagnosis or not - two categories, yes or no.
Distress : A total score on a scale is derived, varying from 0 to all symptoms asked, it’s a count of symptoms.
Disorder is categorical, distress in a continuum.
Overlap between distress and disorder
Disorder is presumed for measure of serious problems, distress more moderate problems… is that the case?
Wheaton’s perspective on the overlap between distress and disorder
Within both some psychological and sociological research, there’s a tendency to treat distress as transient, not impairing / a moderate problem, prevalent therefore not important, qualitatively distinct from disorder, and normal.
Argues that a person’s classification within a diagnostic model must first start by scoring the type, frequency, and severity of their symptoms.
Taxometrics
The study of whether the underlying phenomenon measured is continuous or categorical. Usually studies find that underlying mental health phenomenon are continuous in nature.
Is distress stable or transient?
Estimates of stability need to find correlation with itself over time
Most between .5 to .75 correlation over a 1-10 year period which means the level of stability is high enough to suggest that distress describes persistent and fundamental differences in mental health of the population.
Is distress accompanied by impairment of functioning?
Predicts loss in income/ social status
Shows effect on educational performance, associated with 28% lower household income by age 50 when bigger physical health problems occur, distress in childhood is associated with 35% reduction in adult family incomes.
Significant effect on marital stability, with 30% higher risk of ins-ability each standard deviation increase in distress.
Problem with “normal” and “expectable” for disorders and distress
Historical, cultural, socially patterned variation due to social location. Varies with situational demands, threats, and complexity.
What do we expect after divorce? Anger, joy, or fear? It depends.
Measurement of a “Human Science” goal
Creating knowledge that helps everyday people understand and control their own life, avoid suffering, achieve well-being and create knowledge that people can use for temselves.
Forms of measurement and the person or object
Placing people into diagnostic categories is viewed by Mirowsky and Ross as treating them as objects and ignoring the person with thoughts, feelings and actions of their own.
Assert that continuous forms of measurement are better at represented the reality of people’s lives, emotions, and thoughts, as perceived and reported by the people themselves (both in terms of types & severity of the problem)
Aneshensal et al. sociological models
Focus on the mental health consequences of patterns of social organization
Aneshensal et al. socio-medical models
That emphasize the social antecedents of mental disorders.
Argue that socio-medical models ignore the full effects of social conditions, look for causation in “unusual elements” in individuals, rather than normative social arrangements. Ignore how exposure to stress may cause other symptoms that don’t correspond to diagnostic criteria.
Important question raised in Aneshensel et al.’s research
Are you interested in investigating causal factors associated with individual mental health problems, so as to be able to improve outcomes for individual patients, or are you interested in investigating how we as a society might make larger scale changes to our social organization, so as to reduce the disproportionate mental health burden experienced by marginalized populations?
Latter approach may ultimately be more effective and benefit a larger segment of the population.
The particular approach adopted by a group or society has significant policy level implications
You don’t need to diagnose people to treat them
Adopting continuous rather than categorical approach would allow for a more tailored treatment, recognizing the suffering of those short of the diagnostic cut off
If social status and the social environment have a causal role in mental health problems, is focusing resources on more proximal causes cost-effective for reducing population level suffering?
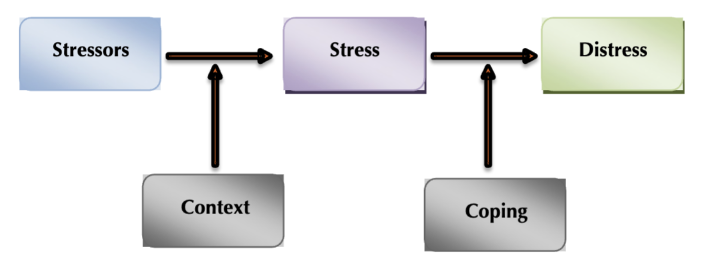
Stressor, stress, distress process model
Stressor —> (context) —> stress —> (coping) —> distress
Stressors defintion
Conditions of threats, demands of structural constraints, by their very existence, calls into the question the operating integrity of the organism
Stress defintion
A feeling of emotional strain or pressure, often as the result of a internal or external stimuli.
Distress definition
A state of persistent anxiety and/or depression.
Threats as a stressor
Expectation or possibility of harm
Demands as a stressor
THe feeling of pressure/ being pushed
Constraints as a stressor
When our choices are restricted/ have limited opportunities.
Context in regards to stressors
The circumstances which the stressor occurs in.
This could include 1) the history of experience of similar or contrasting stressors, 2) the knowledge and skill resulting from coping with previous stressors, 3) the social context which determines the meaning of the stressor, 4) social comparison with other lives, and 5) operative norms (ex. the cultural norm that university is stressful)
The Biological Model of Stress
Stressors —> Alarm response —> resistance.
Issues with the Biological Model
Stressors are presumed to be a problem, but whether it is perceived as a threat is in fact determined by context.
Biological response are not a necessary condition of mental health responses to stressors.
Stressors have broader sociological consequences, spreading into many areas of life.
Translated to human research, stressors were though to involve change by definition. Only acute forms of stress evolved as the focus.
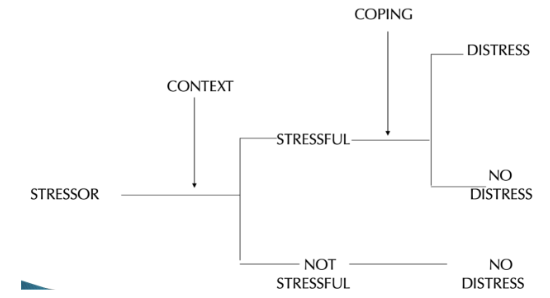
Multi-stage model of stress
Stressor → (context) → Stressful or not stressful
Stressful → Coping → Distress if not coped well or No distress is coped well
Not stressful → no distress
The engineering model of stress
Stress is an external force acting against a resisting body
Stress becomes a stressor when it exceeds the limits of structural integrity, the elastic limit of the material.
The material can then adjust by elongation or compression (coping), producing a greater elastic limit until an ultimate elastic limit is reached and then a “breakdown”
Stressors and stress are not distinct phases in the engineering model; both refer to external force or threat. Accounts for stress that is a continuous force (chronic) rather than an event.
Life event stressor
Acute and self-limiting, have a natural course and point of resolution, a clear onset and offset
Chronic stressors
Develop insidiously, are stable or continuous in nature, are more open ended
Under-reward Chronic stressor
The stress of not experiencing reciprocity and someone taking more than replenishing.
Ex. Reduced output from a relationship relative to input, as in being paid less for a job than others with the same qualifications (due to discrimination)
Complexity chronic stressor
As in the number of sources of demands, or direct conflict of responsibilities across roles, or constant contingency and instability in life arrangements, or complex content in role responsibilities.
Uncertainty chronic stressor
A problem only when one desires or needs resolution of an ongoing issue, in effect, unwanted waiting for an outcome.
Conflict chronic stressor
When regularly reenacted and thus institutionalized in relationships without apparent resolution, as embodied by differences over goals or values.
Daily hassle stressors
The “irritating, frustrating demands that characterize everyday transactions with the environment”
Such as : traffic jams, grocery shopping, waiting in lines, losing things, house maintenance, the weather.
Non-events stressors
“An event that is desired or anticipated but does not occur”. The unwanted waiting for a desired outcome
Such as : Not getting promoted, not getting married, when you want to, not getting into a school.
Traumatic stressors
Overwhelming, extreme, experience, violent encounters with nature, technology, or other persons, more severe than life events
Such as : experience in combat, sexual assault, physical abuse, partner unfaithful, death of a child, natural disaster.
Contextual Stressors
Any form of stress that occurs at a level of social reality beyond the individual, such as in neighborhoods, communities, work places, whole nations
Such as: recession, 9/11, Katrina, crime, state violence, COVID-19, climate change
Two way Classification of Stressors
Two axes :
1) Discrete (like a sudden event with clear onset) or continuous stress (a long term stressor with prolonged and unclear onset and offset)
2) Levels of Social Context which include Micro (individual to interpersonal level level), Meso (small community to town/city level), and Macro (national, global, societal level)
Stressors fall on a continuum of both these axes.
Ex. COVID-19 is a macro chronic traumatic condition while divorce is a micro level life changing event.
What stressors have a bigger impact on mental health
Before the field was focused on acute measures, but actual research finds that chronic stressors are more correlated with mental health issues and disorders.
The other highly correlated is childhood trauma.
Still some results of impact on mental health for daily hassles.
Trait hypothesis
Believed that stressors differ in their inherent characteristics, need to specify further (uncontrollable, negative, unscheduled)
Differential vulnerability
Believe that differential access to coping resources results in differential sensitivity to stressors, so some are affected by a lot, some not at all.
Context hypothesis
Belief that effect depends on context which determines threat value.
Stress domain hypothesis
Life events only a part of the stress-universe, need to specify all varieties of stress.
The Stress Process Model is a multi-stage process including
1) Socio-environmental sources of stress exposure , 2) Sequence of stress trajectories through life, 3) The intervention of coping resources and behavior, 4) The Myriad of life consequences that follow.
Pearlin et al. (1981) proposed a multi-stage process relating different types of stress to each other, and specifying how coping both explains and can shape the impact of stress.
Factors involved in the Stress Process Model
Sources Context : Statuses, roles, structures that generate inequality and thus are likely to map to the experience of stress
Stressors : Primary and secondary — the concept of proliferation through life and Different types — event chronic, one breeds the other
Coping : Both social and personal coping resources intervene as mediators and moderators
Outcomes : Mental health, physical health, achievements in social roles, instability in roles, losses of status.
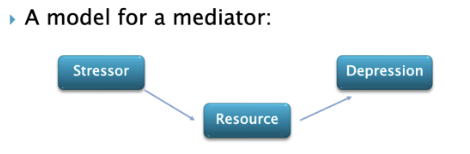
Mediators
Variables that are affected by an earlier variable in a process and, explain part or all of it’s effect
Answers the question : How does X affect Y? It is part of the effect on X on Y.
The task of explanation and theorizing a relationship involves specifying mediators.
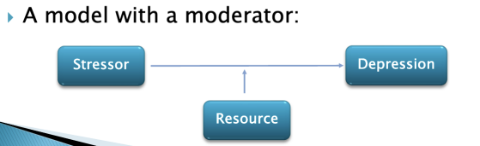
Moderators
Variable that actually changes the size or direction of the effect on X on Y.
Coping resources can play both roles.
Stress proliferation
Chain of stress set off by an initial (primary) stressor.
Spillover of stress across roles, lives, and levels of social reality: Work family conflict, Cost of Caring (Kessler and Mcleod, 1984), Effect of macro-level stress on micro-level (ex. recession -> job loss -> financial strain)
Not automatic : There are contingencies at each stage determining whether the next stressor occurs.
Pearlin two proposed approaches to medical sociology
Structure seekers and meaning makers.
Two different approaches which should be complementary and together offer fuller insight into how mental health operates.
Structure seekers
One approach to medical sociology : Seek to reveal structure in everyday life & its consequence for health
Focused on the hierarchical systems, social experience & conditions that people regularly encounter in their participation in institutional systems & social relationships. Concerned with similarities among people similarly located within structures systems and differences among those with different positions.
Typically engage in large scale quantitative research.
Critiques by meaning makers as too removed from the people they study, their research as mechanical, passionless, insensitive to individual respondents.
Meaning makers
Second approach to medical sociology : Endeavor to get into the heads and hearts of society’s participants as they interact and encounter different situations.
Realign theory with lived experience & come to understand social life as it is seen, interpreted, acted upon & shaped by people we are studying.
Most qualitative data from smaller samples, interpreted not only by researchers but also based on subject’s own interpretations & perceived relevance of life circumstances to the person’s life.
Critiqued by Structure Seekers for small samples, lack of strategic comparisons, and because studies aren’t generally replicable.
McLeod position on approaches to medical sociology
Most sociology applications have focused on it’s objective characteristics narrowly. These applications emphasize a structure over a idea of social arrangements and cultural conceptualization.
Both approached neglect equally important questions about the social origins and meaning of stressful events and mental health, and how stressful experiences are constructed over time in response to structural and cultural constraints and in interpersonal interactions.
McLeod applies this critique to Stress Process Research
There is recognition of stressors on outcomes depending on the person and that resources and actions that modify stressors’ effect (ex. social support and coping) do so in part by altering meanings.
Further suggests that we cannot understand how stress process operates without taking meaning into account and that social arrangements may produce distress not only by influences objective life circumstances but also by influencing how those circumstances are interpreted.
Coping
Any response that prevents reduces, controls, or make tolerable emotional distress
Social variation in the occurrence of mental disorders and distress is linked to…
Status-based differences in access to the resources available to help people cope with difficult life circumstances.
Active coping
When we’re actively attempting to resolve the problem
Emotion-focused Coping
When we attempt to manage how we feel about the problem, we’re not taking steps to change the stressor, we just change out emotions about that stressor to cope.
Avoidance Oriented Coping
When you ignored a problem or delay confronting a problem
Psychosocial resoruces
The skills, beliefs, talents, and individual personality factors that influence how people manage stressful events.
Includes things like sense of control/mastery and social support.
Sense of control/ mastery
A learned generalized expectation that events and circumstances in one’s life are contingent on personal choices and actions. Understood as existing in opposition to powerlessness.
Powerlessness typically tends to be negative for mental health.
Distress tends to be higher for those who believe…
They have little influence over what happens to them,
what is going to happen will happen,
we might as well decide what to do by flipping a coin,
and success is mostly a matter of good breaks.
Distress tends to be lower among those who believe :
When they make plans, they can make them work
Misfortunes result from the mistake they make
There is really no such thing as luck
What happens to them is their own doing.
Effect of low sense of control/mastery
Has a direct effect, demoralizing impact,
Undermines confidence and hope
Diminish the will and motivation to actively solve problems
Make active attempts to solve problems seem pointless : “What’s the use?”
Types of external attributions
Luck, chance, family background, other people, god, etc.
Benefits of a high sense of control/mastery
A greater sense of control implies greater motivation
An excessive sense of control implies a unrealistic self-appraisal.
Structural amplification of mastery
Neighborhood disorder destroys the sense of control that other insulates residents from the consequences of disorder for mistrust.
The very thing needs to protect disadvantaged residents from further negative effects of their environment — a sense of personal control is eroded by that environment.
Structural factors
SES : level of prestige, education, income
Gender: male, female, non-binary, other
Age: place along the life course
Race: exposure to discrimination, segregation, violence
Employment: full-time, part-time, unemployed, retired
Work Structure: level of complexity, routine, supervision
Culture: e.g. collectivist vs. individualist cultural values
"The Sociology of Mental Health: Surveying the Field" by Aneshensel, Phelan, and Bierman
In this foundational text, the authors introduce several critical concepts in the sociology of mental health.
medicalization of mental health issues
cultural competence in mental healthcare and cultural and social factors is vital for effective treatment
The role of structural strain in mental health outcomes
Minority stress is a central concept, revealing the chronic stressors faced by stigmatized minority groups. Racial and ethnic disparities in mental health are examined, showing the connection to systemic inequalities.
Social Integration (Aneshensel, Phelan, and Bierman)
The level of connection and participation individuals have in social networks, communities, and institutions, which can influence their mental health.
Social Determinants of Mental Health (Aneshensel, Phelan, and Bierman)
The societal factors, including socioeconomic status, education, and social support, that significantly affect mental health and well-being.
Stigmatization (Aneshensel, Phelan, and Bierman)
The labeling, stereotyping, and social exclusion of individuals with mental health issues, often leading to negative mental health outcomes.
Social Support (Aneshensel, Phelan, and Bierman)
Emotional, instrumental, and informational assistance provided by social networks and relationships that can positively impact mental health.
Mental Health Disparities (Aneshensel, Phelan, and Bierman)
Differences in mental health outcomes experienced by various social groups, often linked to social inequalities and access to mental health care.
Gender and Mental Health (Aneshensel, Phelan, and Bierman)
The influence of gender roles and expectations on mental health, with attention to gender-based disparities.
Life Course Perspective (Aneshensel, Phelan, and Bierman)
An approach that examines how mental health experiences and outcomes evolve over an individual's lifetime, considering social and environmental factors.
Social Epidemiology (Aneshensel, Phelan, and Bierman)
The study of how social factors, including social determinants and stressors, impact the distribution of mental health outcomes in populations.
Socialization (Aneshensel, Phelan, and Bierman)
The process through which individuals learn and internalize cultural norms, values, and behaviors, influencing their mental health.
Policy Implications (Aneshensel, Phelan, and Bierman)
The practical applications of research findings to shape policies and interventions aimed at promoting better mental health outcomes in society.
Medicalization (Aneshensel, Phelan, and Bierman)
The process by which behaviors or conditions are defined and treated as medical issues, potentially leading to over-reliance on medical solutions for mental health problems.