SAM Exam 4 - EEC
1/114
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
115 Terms
Triage Categories
Category 1: Emergency: needs to be seen NOW
toxins, GDV, male cat no peeing, trauma, resp issues, diabetes, heart disease, 2+ seizures in 24hrs, paralysis, anaphylaxis, heat stroke
Catagory 2: ASAP: needs to be seen today
toxins, pain, anorexia >24hrs, rapid decline, lethargy, bldy diharreah, swollen eyes
Catagory 3: Routine: should be seen in 24-48h
chronic lameness, allergy’s, infections, non bleeding wounds, GIT upset
Fundamental history questions to ask the owner
Topics: SAMPLE
Signs, Allergies, Medications, Past history, Last knowns, Events
Phone: breathing? Conscious? Bleeding? Mobile? Open wounds/fractures? When did it happen? How far away? Do you know where clinic is? Transport? Explain triage process and emerg fee.
Arrival: Contact? Pet info? Records? Authorization? What happened? When did it happen? Progression? Any care given prior? STAT consent? Last meal/BM?
Crash cart
Contents:
Drugs: CPR medications and dosing charts
Airway: ET tubes, laryngoscope, ties, Ambu bag, stylets
IV supplies: syringes, needles, large flushes, clippers
Packs: thoracocentesis, pericardiocentesis, urinary catheter kits, laceration repair, tracheostomy
Audit:
Restock every shift and check for functionality
Label and keep organized
CPR guidelines
Training: CPR drills every 6 month, recover training
CPR Stats: <6% of dogs and <20% of cat survive
Timing is critical: 0.5 minutes = ROSC vs 1 minute
Catheter: improves ROSC
Recognize: absence of breathing, agonal breaths, no pulse
Personnel: switch q2min to avoid fatigue
1: lead
2: airway/breathing, intubate
3: compressions (30 bpm)
4. Vascular access
5. Drugs
6. Monitor, pulses/rhythm checks
Primary and secondary survey and Minimum emergency database
Primary Survey: ASAP
Airway: Patency?
Breathing: RR/effort, localize obstruction
Circulation: MM color, CRT, pulse, HR
Disability (brief neuro exam) & pain
Secondary Survey: once stable
Minimum database: PCV/TS, Bld Glucose, Lactate, Acid base, Bld gas, Electrolytes, iCa
From catheter hub blood
Full PE, Neuro exam, BP, SPO₂, temp
SIRS criteria
Use: triage alert system evaluating vitals
Limitations: Non-specific
Criteria:
Dogs: ≥2 abnormal vitals
Cats: ≥3 abnormal vitals
Scoring systems in veterinary medicine
Modified Glasgow Coma Scale (MGCS): Neurological scoring
Animal Trauma Triage (ATT):
6 categories (perfusion, cardiac, respiratory, neuro, skeletal, integument)
Higher score = worse prognosis
SOFA: systemic organ failure assessment
Localization of respiratory
Upper airway obstruction
Inspiratory dyspnea
Externally audible noise: stertor/stridor
Lower airway obstruction
Expiratory dyspnea
Audible wheeze on auscultation not externally audible
Pulmonary parenchymal disease
Inspiratory and expiratory efforts may both be increased
Increased or wet lung sounds, crackles, harsh lung sounds
Pleural space disease
Paradoxical chest wall movement
+/- Fast and shallow breathing
Quiet or decreased lung sounds

Shock
MOA: inadequate cellular energy production
Hypovolemic: Loss of volume circulating
CS: tachycardia (not cats), pale, CRT >2, poor pulse, MAP <60mmHg(severe)- unable to palpate pulse
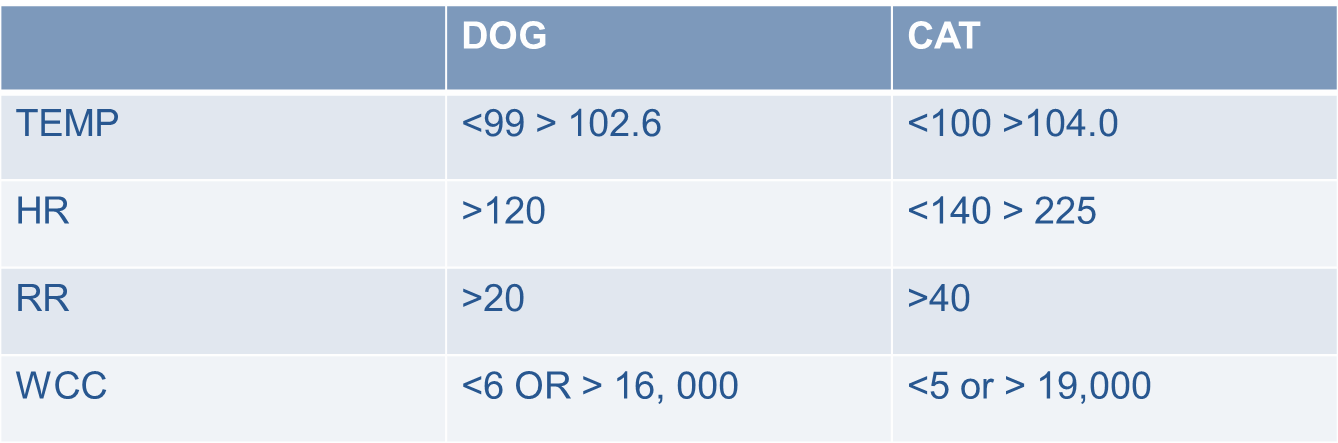
Hypothermic: <98F, Hyperthermic: >102.5 F
TX: Buffered isotonic fluids
Cardiogenic: decreased forward flow from the heart
Distributive: decrease in or increase in SVR or maldistribution of blood
Metabolic: deranged cellular metabolism
Hypoxemic: decreased 02 content
Septic: subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality
Blood pressure
Doppler
Gives only systolic pressure
Oscillometric
Gives systolic, diastolic and mean pressure
Invasive
Catheterization of dorsal pedal or femoral artery
Normal:
Systolic: > 90-140 mmHg
Diastolic: 50-80 mmHg
Mean: 70-100 mmHg
Vascular access options
Peripheral IV
Jugular IV
Intraosseous (IO)
Minimum database
PCV/TS – must interpret PCV with TS!
both decreased: hemorrhage
Decreased PCV w/ normal TS: RBC issue
Blood glucose
Lactate
Blood gas/acid-base
Electrolytes
iCa
ALL this can be obtained from Catheter hub!
Fluid resuscitation
Isotonic crystalloids for resuscitation
Avoid colloids and hypotonic fluids in early phase
Fluids: Buffered isotonic IV fluid bolus
5–10 mL/kg (cats), 15–20 mL/kg (dogs) over 15-30 mins
Colloids and hypotonic fluids contraindicated
Monitor fluid responsiveness
Lactate/lactate clearance
by-product of anaerobic glycolysis
Normal: < 2.5 mmol/L
High: inadequate perfusion (Type A) or cellular metabolism dysfunction (Type B)
Persistent elevation = worse prognosis
Use: Serial measurements can guide fluid therapy
Blood glucose
Hypoglycemia:
MOA: Collapsed/mentally altered patients, Neonates, Diabetics
TX: 2.5% Dextrose bolus
Easy to test and fix!
SPO2
Cyanosis late indicator for hypoxemia
SPO2 < 95 % = PaO2 < 80 mmHg
SpO2 90% = PaO2 60 mm Hg
Point of care ultrasound
Done Before x-rays
Done in lateral or standing
Use: Detect fluid, pneumothorax, effusion before rads
Not for resp distress patients
Take DV views not VD
NOT in a patient in respiratory distress
AFAST: 4 quadrants (liver, bladder, spleen, kidneys)
REPEAT once fluid resuscitated
TFAST: Pericardial, pleural, diaphragmatic views
The role of low stress and fear free handling in the ECC patient
Reduces worsening of respiratory distress and shock
Oxygen in carrier
Gentle restraint
Sedation if needed
Pain relief
Give 1st!!
Key part of stabilization
Opiates are first line
no NSAIDS
Lidocaine: good for motility, adjunctive analgesia, VPCs
Ketamine: good for wind up and visceral pain relief
pancreatitis
Kirbys rule of 20
Critical parameters that should be evaluated at least daily in all critically ill animals
Fluid Balance, Electrolytes
Oncotic Pull/Albumin
Glucose
Acid-Base Balance
Oxygenation and Ventilation
Neurologic Status, Renal Function, immune status
Blood Pressure, Heart Rate, Rhythm, and Contractility
Temperature
Coagulation, RBC/Hemoglobin Concentration|
GI Motility, Mucosal Integrity, Nutrition
Drug Dosages and Metabolism
Pain Control
Wound Care and Bandages
Loving Care
Timing for emergency surgery
When: stabilized for 24–48h first
Exceptions: Hemorrhage, GDV, septic peritonitis, perforation
Client Comm: Discuss timing with owners in context of stability and urgency
Body water distribution
60% of BW is water
ICF: 40% BW, 2/3 TBW
ECF: 20% BW, 1/3 TBW
Electroneutrality: ∑ cations = ∑ anions
Na+ + K+ + UC = Cl- + HCO3- + UA
UA – UC = Anion Gap
Regulators of water balance
Kidneys: Na and volume
Volume Receptors: Cardiopulmonary circulation, carotid sinus, aortic arch, kidneys
Effectors of Circulating Volume: sympathetic nervous system, renin/angiotensin, renal Na excretion
Body’s response to Blood Loss
Phase I: within 1 hr of hemorrhage, movement of fluid from interstitium into intravascular space
Phase II: Activation of R-A-A-S system: Na retention
Phase III: Bone marrow begins to increase production of RBC’s
occurs within a few hours of blood loss, takes 7 days
2024 AAHA Fluid therapy guidelines
Takaways: Compartmentalize your thinking, one fluid rate does not fit all, don’t overload
Actions: Don’t set it and leave it, choose a fluid administration route
Remember: Fluids are drugs
Individualized and goal directed fluid therapy
1 Recognize which fluid compartment deficit(s) exists
Intravascular, intracellular, interstitial
2 Understand which fluid type and administration route will best replace each deficit
Kidney issues, toxins
IV, SC, IP, IO Enteral
3 Calculate the fluid dose and administration rate
Resuscitation, Rehydration, Maintenance
4 Monitor patients for response to therapy and signs of complication
BW, Temp, PR, MM, CRT, RR, Skin turgor, Auscultation, Mental status, Urine output, PCV/TS, Serum lactate, USG, BUN, Cr, BP, Bld gas, O2
Assessment of interstitial space
MOA: assessed as dehydration
excessive panting, vomiting, diarrhea, diabetes
CS: skin tent, MM, retracted globes, dull corneas
Physical findings in dehydration
<5%: none
5-6%: decreased skin turgor
6-8%: decreased skin turgor, dry MM
9-10%: decreased skin turgor, dry MM, retracted globes
10-12%: persistent skin tent, dry MM, retracted globes, dull corneas
>12%: death, shock
Assessment of intravascular space
History
Hypovolemia: excessive bleeding, severe burns, severe diarrhea or vomiting, kidney disease, or inadequate fluid intake
Hypervolemia: fluid overload, PD, salt intoxication, osmotic agent admin
Cardiovascular: HR, CRT, pulse quality, BP, ECG
Hypovolemia: MAP: >80 = mild, >60 moderate, <60 severe; arrhythmias
Hypervolemia: hemodilution, arrhythmias
Imaging: POCUS
Hypovolemia: Collapsibility index >27%, microcardia, small vasculature
Hypervolemia: ascites, effusion, Collapsibility index <27%
Addressing hypotension
Situational fluid therapy
Resuscitation
Rx: Buffered isotonic IV fluid bolus
Dose: 5–10 mL/kg (cats) or 15–20 mL/kg (dogs) over 15–30 min
Replacement
Dose: L = BW (kg) x %D
12–24 hr SQ
Maintenance
Dose: 30 x BW (kg) + 70 = mL/kg/day
Crystalloids
Isotonic: hypovolemia, anaphylaxis, dehydration, always good 1st step
0.9% NaCl: No added K, Mg, Ca, dextrose, buffers
Plasma-lyte: added K, Mg, acetate, gluconate
No added Ca, dextrose
Normosol R: added K, Mg, acetate, gluconate
No added Ca, dextrose
Hypertonic:
5.0, 7.5, 23.4% NaCl: No added K, Mg, Ca, dextrose, buffers
Hypotonic:
Plasmalyte 56% w/ dextrose: added K, Mg, acetate, dextrose
No added Ca
0.45% NaCl: No added K, Mg, Ca, dextrose, buffers
0.45% NaCl w/ dextrose: added dextrose
No added K, Mg, Ca, buffers
Dextrose in water: added dextrose
No added Na, Cl, K, Mg, Ca, buffers
Normosol M w/ dextrose: added K, Mg, acetate, dextrose
No added Ca, buffers
Colloids
Natural: blood, albumin, fresh frozen plasma
Artificial: hetastarch, vetstarch, dextrans
Risks: AKI, coagulopathy, delayed platelet closure time in dogs.
Banned by FDA in people
Contradictions: bleeding, inflammatory states, anaphylaxis
Replacing interstitial and intravascular volume
Hypovolemia: 5-10mL/kg (cats) or 12-20mL/kg (dogs) over 30 min of buffered isotonic fluid IV
IV moves from vascular to interstitial
Dehydration: buffered isotonic fluid over 24hrs IV, oral, SQ
IV moves from vascular to interstitial to intracellular
Determines patient “fluid responsiveness”
Infusion of a rapid bolus of small volume
10 – 20 ml/kg
Anesthesia fluid guidelines
Indications: renal disease, recovery optimization in heathy patients
IVFT rates = 5ml/kg/hr (dogs) or 3ml/kg/hr (cats)
Recognize signs of fluid overload
MOA: Aggressive fluid therapy
CS: hypervolemia, edema, cavitary effusions, BW increase >10%, discharge, murmurs, distention, low SPO2, loss of serosal detail, enlarged veins/arteries, decreased collapsibility index
Appropriate management of an IV catheter
Use: Lg bore and short cannula
Steps: aseptically prep, secure
Maintenance: check 2x per day, clean when disconnecting
Acid/base Definitions
Acid: molecule that donates a H+
Base: molecule that accepts a H+
Buffer: weak acid/base that protects against pH changes
EC: bicarbonate
IC: PO4, proteins, hemoglobin

Blood gas analysis
Respiratory
Arterial blood gas: O2(paO2)
Venous blood gas: CO2
Metabolic: HCO3
Anion Gap
Increase in serum lactate, ketoacids, uremia
Alkalemia
(Na+ + K+ + UC) - (Cl- + HCO3- + UA) = 10-20AG
High: low UC, high UA
Low: high UC, low UA
Acidosis

Metabolic acid/base disturbances
Acidosis: Low pH, Low HCO3
Myocardial contractility decreases if pH < 7.2
Venous vasoconstriction, Arterial vasodilation
↑ AG: EG toxicity, Salicylate toxicity, DKA, Uremia, Lactic acidosis
Normal AG: Diarrhea, Carbonic anhydrase inhibitors, Dilutional acidosis, Addison’s, Posthypocapnic metabolic acidosis
Hyperchloremic
Compensation: hyperventilation, ↓ PCO2
Alkalosis: High pH, High HCO3
Arteriolar vasoconstriction, Decreases stroke volume, less oxygen delivery to the tissues
MOA: Vomiting, diretics, heart failure, renal dx, crons dx, Alkali administration, cushings
Cl resistant: addisons, cushings
Compensation: low RR to increase CO2, urine is alkaline

Respiratory acid/base disturbances
Acidosis: Low pH, High PCO2
MOA: asthma, COPD, opiates, heat stroke, high ICP, MG, paralysis
Compensation: renal retention for ↑ of HCO3
Alkalosis: High pH, Low PCO2
MOA: hypoxia, fever, anxiety, Pulmonary dx, anemia, pain
Compensation: renal excretion for ↓ of HCO3

Simple vs. mixed acid/base disturbances
Simple: There is a primary disorder and there is an adequate compensatory response
Lungs: Excretion of CO2
Rapid compensation
Kidney: Reclaim filtered bicarb, excrete acid
Slow compensation
Mixed: Two separate primary disorders are occurring and compensation is inadequate or there is “overcompensation”
Osmoles
Ineffective: does not generate osmotic pressure or an influx/efflux of water
Effective: does exert osmotic pressure
does not freely cross membranes
Effective ECF osmolality (mOsm/kg) = 2 x Na+ + [glucose]/18 + [BUN]/2.8
Hyponatremia
Dog: <140, Cat: <147
Hypervolemic: increase in TBW, CHF, liver dx, nephrotic syndrome, renal failure
Normovolemic: PD, myxedema coma, hypotonic fluids, SIADH
Hypovolemic: addisons, GI loss, third-spacing effusion, renal dz
CS: Abnormal mentation, ataxia, seizures, CNS deficits, edema
TX: 1mmol per hour
≤10 mmol/L over 24 hours
Watch for Osmotic demyelination with chronic (>48hr) correction: CS takes days to occur
Hypernatremia
Dog: >155, Cat: >162
Hypervolemic: prolonged replacement fluids, salt toxicity 4g/kg.
CS: Tachycardia, weak pulse, prolonged CRT, anorexia, Lethargy, Vomiting/diarrhea, Behavior change, Ataxia, Seizures , Coma, renal
Normovolemic: hypodipsia, diabetes insipidus
CS: PU/PD, norexia, Lethargy, Vomiting, Behavior change, Ataxia, Seizures , Coma
Hypovolemic: Vomiting, diarrhea, third spacing, burns, CKD, post obstructive diuresis, excessive water loss
CS: Tachypnea, respiratory distress, pulmonary edema, norexia, Lethargy, Vomiting, Behavior change, Ataxia, Seizures , Coma
Pheudo: hyperglycemia
TX: Up to 1 mmol/L/hr if acute (<24hrs), <12 mEq/L per day if chronic (>24hrs), LR, plasmalyte A, Normosol R, 0.9% NaCl
No 0.45% NaCl
Shock: Expected change in [Na] with 1 liter of fluids = (Fluid [Na + K] – Patient [Na])/(TBW + 1)
TBW = BW× 0.6
Stable:
FWD (in liters) = {(Patient [Na] – Target [Na])/Target [Na]} × TBW
Target [Na] = Midrange of the reference interval
FWD acute = Patient [Na] – Target [Na]
FWD chronic = 2(Patient [Na] – Target [Na] )
Potassium
Normal: 3.5-5.5 mEq/L
Hypokalemia
MOA: diet, NaCL/D5W fluid therapy, AlkalemiaInsulin, insulin/glucose, hypothermia, albuterol toxicity, Hypokalemic myopathy of Burmese kittens, vomiting, diarrhea, CKD, Post-obstructive diuresis, Hyperadrenocorticism, Hyperaldosteronism, diuretics, penicillin, rattlesnake antivenom
CS: Ventral neck flexion, arrhythmias, PU/PD, poor urine concentration
TX: <0.5 mEq/kg/hr K MAX !! & label IV bags
Hyperkalemia
MOA: CKD, urinary obstruction, addisons, puedo from translocation, whipworms
CS: slow HR, prolonged QRS, atrial stand still, high T aves, short Q-T interval
Do not rely on ECG or bradycardia to tx, not reliable
TX: LRS, Normosol R, insulin @ 0.25-0.5 u/kg, Calcium gluconate 10% @ 0.5-1 ml/kg if bradycardic, albuterol
Chloride
Most abundant anion in ECF, produced in GIT, reabsorbed in the renal tubules
Normal Dog: 110, Cat: 120
Hypochloremia
MOA: pseudo w/ lipemic samples, diuretics, vomiting, GI dx, thiazine/diuretic therapy, chronic resp acidosis, hyperadrenocorticism
TX: 0.9 % NaCl + buffered isotonic crystalloid
Hypercholermia
MOA: KBr, diarrhea, diet, salt poisoning, renal failure, diabetes mellitus, chronic resp alkalosis, hypoadrenocorticism, fluid therapy
TX: avoid NaCl, oral bicarb, discontinue iatrogenic fluids
HCO3− deficit = Weight (kg) × {Desired [HCO3] – Patient [HCO3]} × 0.3
![<ul><li><p>Most abundant anion in ECF, produced in GIT, reabsorbed in the renal tubules </p></li><li><p>Normal Dog: 110, Cat: 120</p></li></ul><p><strong>Hypochloremia</strong></p><ul><li><p><strong>MOA</strong>: pseudo w/ lipemic samples, diuretics,<strong> <u>vomiting</u></strong>, GI dx,<strong><u> thiazine/diuretic therapy</u>,</strong> chronic resp acidosis, hyperadrenocorticism </p></li><li><p><strong>TX: </strong>0.9 % NaCl + buffered isotonic crystalloid</p></li></ul><p><strong>Hypercholermia </strong></p><ul><li><p><strong>MOA:</strong> KBr,<u> diarrhea</u>, diet, salt poisoning, renal failure, diabetes mellitus, chronic resp alkalosis, hypoadrenocorticism, <u>fluid therapy </u></p></li><li><p><strong>TX: avoid NaCl, </strong><u>oral bicarb</u>, discontinue iatrogenic fluids</p><ul><li><p><strong><u>HCO<sub>3</sub><sup>−</sup> deficit = Weight (kg) × {Desired [HCO<sub>3</sub>] – Patient [HCO<sub>3</sub>]} × 0.3</u></strong></p></li></ul></li></ul><p></p>](https://knowt-user-attachments.s3.amazonaws.com/0707a2ae-4b48-49de-b1a9-420c691cdb4d.png)
Phosphate
Most important intracellular anion
maintaining calcium balance
Hypophosphatemia
MOA: DKA tx, insulin, resp alkalosis, TPN, PPN, refeeding, hyperparathyroid, rena; tubu;ar dysfunction. Eclampsia, vomiting, malabsorption
CS: erythrocytes fragility, hemolysis, poor WBC function, muscle weakness, poor platelet aggregation, pain due to rhabdomyolysis, seizures, coma, vomiting, ileus, diarrhea
TX: 0.01-0.06 mmol/kg/hr for 12hrs perenteral, prevention is best!
Hyperphosphatemia
MOA: tumor cell lysis, tissue trauma, rhabdomyolysis, hemolysis, metabolic acidosis, PO4 enemas, Vit D toxicity, Kphos administration, renal failure, hypoparathyroidism, hyperthyroidism
CS: Tremors, hyperthermia, seizures, tetany
TX: Balanced isotonic IVFT, dietary restriction, phosphate binders
Calcium
99% of Ca stored in bone
Regulation via kidneys and GIT
Regulates: Parathyroid gland, Kidney, thyroid C cells
Hypocalcemia
MOA: CKD, pancreatitis, ↓ albumin, hypoparathyroid, ethylene glycol toxicity, artifact, eclampsia
CS: anorexia, facial rubbing, growling, nervousness, twitching, stiff gait, tetany, seizures
TX: 10% calcium gluconate @1–1.5 mL/kg over 10/30min slowly, monitor on ECG
Hypercalcemia
MOA: malignancy, idiopathic, hyperparathyroid, kidney dx, addisons, granulomatous inflam, toxins
CS: PU/PD, uroliths, incontinence, prerenal azotemia, dehydration, anorexia, vomiting dihharea, depression, weakness, twitching, muscle wasting, bradycardia, arrhythmias
TX: 0.9% saline, LR, Plasmalyte, normosol R, furosemide, calcitonin, dex, pred, bisphosphonates
Hypomagnesemia
Kidneys control and regulate Mg balance
Majority of absorption is in the loop of Henle
maintaining resting cell membrane potential
MOA: ↓ protein, ↓ intake, ↓ absorption, colitis, short bowel, diuretics, aminoglycosides, kidney dx, insulin, hypoparathyroid, refeeding syndrome
CS: ventricular arrythmias, ↓BP, neuronal excitability, can see refractory ↓ Ca and K
ECC TX: 0.15-0.3mEq/kg for 1 hr
Important electrolytes
Magnesium
ID: ICF cation
Role: enzymatic rxn, muscle contractions, PTH production
Physio: kidneys reg, ileum absorbs
Potassium
ID: ICF cation
Role: maintaining resting cell membrane potential
Low increases potential (more -/polarized) and vise versa
Sodium
ID: ECF cation
Role: determines ECF volume
Physio: glomeruli filtered, absorbed in tubules
Chloride
ID: ECF anion
Physio: produced in gastric acid, absorbed in intestines, filtered by kidneys
Role: determines metabolic acidosis
hyperchloremic = normal AG
Normochloremic = high AG
Phosphate
ID: ICF anion
Role: cell structure/function, O2 delivery, ATP, cAMP
Physio: GIT absorbs, kidney regulates, opp relationship w/ Ca
high Ca = low Phos
Calcium
Role: Enzymatic rxn, transport, stability, Coagulation, Neuro, Vascular tone, Muscle contraction, Bone formation, metabolism
Total Ca: 9-11.5mg/dl (dogs) or 8-10.5 mg/dl (cats)
Ionized Ca: 56% of plasma, bio active

Blood pressure Monitoring
Direct: Gold standard
Indications: hypovolemic/septic shock, CHF, vasopressors, mechanical ventilation, severe hypertension, high anesthetic risk
NOT indicated in healthy, ambulatory patients
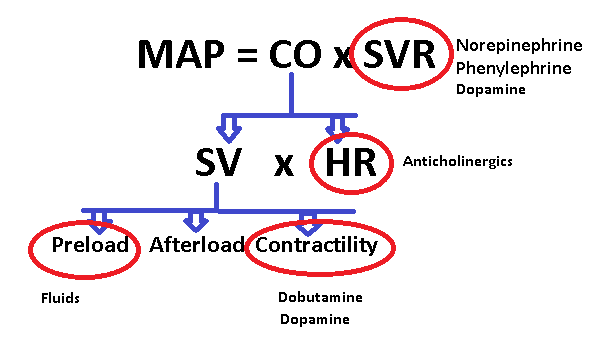
BP = (HR x SV) x SVR
MAP = (SBP-DBP)/3+DBP
Indirect:
Doppler: Systolic BP
Oscillometric: Use: Systolic, Diastolic, Mean BP
Cuff: 40% of the limb circumference
Too sm elevates, too Lg decreases

Pulse oximetry
MOA: Non-invasive measuring the oxygen saturation of Hb in arterial blood
Normal: SPO2 98-100%,
>95% = <80 mmHg moderate hypoxemia
90% = 60 mmHg severe hypoxemia
Cyanosis late indicator for hypoxemia
Limits: pigmented MM, stress, movement, poor perfusion, thin tissue, anemia, lighting
Benefits of pre-oxygenation
Causes of hypoxemia
Oxygen toxicity
Cuve

Capnography
Tells us: ventilation & cardiac output
MOA: Continuous, noninvasive assessment of partial pressure of arterial CO2
USE: ET tube placement, ventilation assessment, dead space estimate, CPR
For CPR: ETCO2 > 10 to 15 mm Hg = ROSC
<10mmHg = poor outcom
TYPES:
Diverting (side-stream): from breathing system and measures CO2 in main unit
Non-diverting (mainstream): directly in breathing system
Troubleshooting:
Cuff leak: narrow plateaus
Cardiac Oscillation: movement w/ HR seen in phase IV, no significance
Zero: cardiac arrest, disconnection, obstruction, apnea test in brain death dead patient
CO2 dysregulation
Hypercapnia
MOA: hypoventilation, fever, shivering, malignant hyperthermia, seizures
pCO2 > 50 mmHg = respiratory acidosis = cerebral vasodilation
ID: capnography
TX: Increase RR , Increase Tidal Volume
Hypocapnia
MOA: hyperventilation, hypothermia
ID: capnography
TX: analgesia, deepen anastesia plane
Rule out cardiovascular/pulmonary cause FIRST
ECG
How: flat clips and pads
Reading: heart beat
P: atrial contraction (depolarization)
Tall P wave: RAE
Wide P wave: LAE
QRS: ventricular contraction (depolarization)
Tall R wave: LVE
Deep S wave: RVE
T: ventricular repolarization
P-R interval: delay in AV node
Arrhythmias
MOA: Abnormal impulse generation or propagation of sinus, atrial, or ventricular orgin
ID: ECG + BP!!(#1)
CS: Syncope, weakness, decompensation of CHF, poor BF
TX:
Class I: Sodium channel blockers
A: quinidine, procainamide
B: lidocaine, mexilitine
C: flecanide
Class II: Beta blockers
propranolol, esmolol, atenolol
Class III: Potassium channel blockers
sotolol, amiodarone
Class IV: Calcium channel blockers
diltiazem, verapamil

Sinus rhythms
Tachycardia: pain, fear, stress
Bradycardia
Respiratory: HR low normal w/ irregular rhythm, high vagal tone, wandering pacemaker
Pause/arrest: fail to depolarize, cardiac dx, irregular rhythm, not a P for every QRS
TX: atropine, pacemaker
Sick sinus syndrome: tachy/brady periods, cardiac dx
TX:Tachycardia w/ beta blockers, Bradycardia w/ pacemaker

Atrial rhythms
Premature complex: normal QRS, abnormal P wave, no TX
Tachycardia: Run of APC’s, atrial enlargement, disease, self limiting
TX: short acting beta blockers (esmolol)
Flutter: fast HR, irregular, sawtooth p waves
TX: slow HR if increased
Fibrillation: fast HR, no p waves, heart dx, DCM
TX: Ca channel blockers, beta blockers, digoxin
Standstill: slow HR, no p waves, hyperkalemia
TX: atropine, glycopyrolate, pacemaker
Systole: no conductivity, cardiac arrest, flat line
TX: CPR

Ventricular rhythms
Premature complex: abnormal QRS, no TX
Tachycardia: high HR, irregular, no P for every QRS
TX: Lidocaine (AVOID WITH CATS)
Most concerning
Fibrillation: no PQRS, Non-perfusing rhythm
TX: defilation


Rhythms involving the AV node/junctional arrhythmia
Supraventricular Tachycardia: normal QRS, p wave present, fast HR
AV block: bradycardia
1d: Prolonged PR interval > 0.2 sec, all P waves get through
CS: asymptomatic, no TX
2d: some p waves get through
Mobitz type I: Increasing prolongation of PR interval
Mobitz type II: PR interval consistent
3s: No P waves, complete dissociation, symptomatic
TX: pacemaker

Basic Life Support
Ventilation
Rate: 1 breath per 6sec
Single rescuer: 30 bpm/2 breaths
Tidal volume: 10ml/kg
Chest compressions
Hand placement
Round chest: Lateral recumbency, thorax pump
widest pt of chest
Keel chest: lateral recumbency, cardiac pump
between rib space 3-5
Small animal: cardiac pump
Wide chest: dorsal recumbency
Depth: 1/3-1/2 in lateral and ¼ in dorsal
Switch out every 2 minutes to avoid rescuer fatigue
Rate: 100-120bpm
Monitor: Use of ETCO2 as an early indicator of ROSC
>12mmHg= ETT is properly positioned
18 mmHg: compression target

Advanced life support drugs
Vasopressin/Epinephrine: standard low dose,
Epi: can repeat Cycle q 3-5 minutes(0.01 mg/kg)
Atropine: give early, dont repeat, non shockable rhythms
Only give ONCE
Lidocaine: ventricular antiarrhythmics, NOT cats
Amiodarone: arrhythmias in cats/dogs
Method: IV preferred
Reverse other drugs: naloxone (opitates), flymazel (benzo), Atipamazole (dex)
Fluids: isotonic crystalloids in hypovolemic NOT euvolemic
Advanced life support tasks
Defibulation
Biphasic NOT monophasic
Start @ 2J/kg then double if no rxn
Before drugs if shockable rhythm
Resume compressions
Open chest CPR: Lg round chest dogs, pleural dx, pericardial dx, unsuccessful CPR, sx patients
Contradicted in sm pets
Monitor: Use of ETCO2 as an early indicator of ROSC
>12mmHg= ETT is properly positioned
18 mmHg: compression target
Post cardiac arrest care
Post cardiac arrest syndrome: anoxic brain, cardiac dysfunction, ischemia, reperfusion injury
Hemodynamic optimization:
Therapeutic hypothermia
Titrate O2 to achive normal SPO2
Manage seizures
Maintain normal glucose, CO2, lactate
Pericardial effusion
Causes: neoplasia (#1), idiopathic (goldens), bleeding disorders, CHF (cats), rupture
CS: diarrhea, weakness, episodic collapse, staring
ID: US heart (TFAST/POCUS)
TX: if tamponade, pericardiocentesis immediately, limit stress, NO restraint
Do not Xray until AFTER pericardiocentesis
Right lateral w/ 6G 2’-4G 5’ needle into thorax
Apply suction and bld should come back
Monitor + recheck >6hrs, rescan w/ US

Acute abdomen
CS: vomiting, regurgitation, doharrhea
CBC: stress leukogram
BioChem:
Hypoalbuminemia, hypocholesterolemia, ionized hypocalcemia
AKI: high BUN/Crea
Sepsis, Addisons: Hypoglycemia
Rads: VD orthogonal views
GVD, FB, pneumoperitoneum, pneumonia, megaesophagus
US: POCUS before rads of diaphragmatic hepatic, splenorenal, cystocolic, pleno-umbilical, hepatorenal views
Peritoneal effusion, FB, Pancreatitis, Pyometra, Masses
Abdominocentesis
How: US guided or 4quad method
Cytology: Degenerate neutrophils, neoplastic cells, intracellular bacteria
TP: Transudate, modified transudate, or exudate
Refractometer
Results:
Transudate: TP<2.5, NCC <100
Hypoproteinemia, low COP, high hydrostatic pressure
Modified: 2.5-5TP, NCC 500-10,000
Increased vascular permeability
Exudate: >3TP, >5000
Sterile vs non-sterile, FIP, chyle, neoplasia, pancreatitis
Drugs for GIT disorders
Antiemetics/Gastroprotectants: Maropitant (#1), H2 blockers (famotidine, pepsid), PPI (omeprazol), carafate (req ulcers to work)
Prokinetics: movement, Metoclopromide, Cisapride, Ranitidine, Erythromycin, Lidocaine
For ileus, not for obstruction
Surgical GI conditions
GDV
Small intestinal FB
Intussusception
Septic peritonitis
Hemoabdomen
Mesenteric torsion
Pyometra
Dystocia (medical and surgical treatment)
Esophageal FB
Medical (non surgical) GI conditions
Hypoadrenocorticism
Pancreatitis
Diabetic ketoacidosis
Hemorrhagic gastroenteritis

Gastric dilation and volvulus (GDV)
MOA: Lg, deep chested dogs
CS: Unproductive retching/gagging, shock, dehydrated, distended, tympanic abdomen, abdominal pain
ID: double bubble’ pylorus on rads, hypovolemia, high lactate
TX: SX to flip stomach(gastropexy), gas decompression, antibiotics, aggressive fluid resuscitation

Small intestinal FB
MOA: younger, perforated or obstructive mass
CS: Vomiting, possible lack of bowel movement, dehydrated, hypovolemic, abd pain, may palpate the FB
ID: abdominal rads/US (bowel dilation x2 portions)
TX: SX to remove, antibiotics, GI meds, fluids

Intussusception
MOA: parasites, viral, bacti, FB, prior sx w/ addhesions
CS: vomiting, diarrhea, abdominal mass, dehydrated, hypovolemic, abd pain, GI parasites known, mass palpable
ID: SNAP for parvo, rads, abdominal US (double wall telescoping intestine), low albumin
TX: SX repositioning, antibiotics, anthelmintics, GI drugs, fluids

Pyometra
MOA: female intact dogs w/ prior heat > 6 months ago or unknown
CS: Dehydrated, hypovolemic, discharge, sepsis, abd pain, febrile
ID: rads/US caudal abdomen mass cranial to bladder, PROFOUND leucocytosis
TX: antibiotics, spay
Septic peritonitis
MOA: Perforated foreign body, ruptured mass, ruptured gastric ulcer
CS: Dehydrated, hypovolemic, abd pain, mentally altered
ID: loss of serosal detail w/ rads, abdominal US, Hypotensive, Hypoglycemic, Hypoalbuminemic, high BUN/Crea
TX: SX to reduce, fluids, GI drugs, antibiotics

Hemoabdomen
MOA: traumatic, neoplasia, Rodenticide, anaphylaxis
CS: Pale mm, anemic pulses, hypovolemic, distended abdomen, labored breathing, may palpate mass
ID: mass effect + loss of serosal detail on rads, abdominal US, Low TS, PT/PTT is prolonged
TX: Sx remove spleen, fluids, GI drugs, blood

Mesenteric torsion
MOA: GSD, Lg dogs
CS: Vomiting, lg volumes bloody stool, severe shock, severe pain
ID: gas dilation on rads and abdominal US
TX: Aggressive supportive care + surgery, fluids, analgesia, GI drugs, antibiotics, Ischemia/reperfusion
Dystocia
MOA: Difficult birth, common in toy breeds, bulldogs, mastiffs, etc.
Maternal: Anatomic abnormalities
Fetal: fetal oversize, fetal malposition, fetal death
CS: no birth 36hrs of temp drop, >30min intervals w/ myometrial contractions or >2hrs w/o, labour lasting >24hrs, active labor >4hrs no fetus produces, contractions >60min w/ no fetus produced
TX: oxytocin, Ca gluconate, Dextrose, manual manipulation, C-section if ill or not progressing

Esophageal FB
CS: Pain with a change in posture or head carriage, drooling, regurgitation, excessive swallowing, anorexia, aspiration pneumonia
Chest x-rays
TX: blind removal, endoscope, surgery, thoracotomy is indicated if perforation occurs.
Hypoadrenocorticism / Addisons
MOA: poodles
CS: Dehydrated, hypovolemic, abd pain, mentally altered
ID: High k, Low Na, Low Glucose, high Ca, lack of stress leukogram, Baseline cortisol, ACTH stim
TX: fluid, steroids ASAP (pull bld and give), Mineralcorticoids
Pancreatitis
MOA: high fat food
CS: Vomiting, diarrhea, decreased appetite, Dehydrated, hypovolemic, abd pain
ID: abdominal US w/ sterile exudate, TFAST w/ pleural effusion, Hyper or hypoglycemic, Hypoalbuminemic, high BUN/Crea, may have DM
TX: fluids, analgesia, GI meds, Prokinetics Corticosteroids, NE tube, bland diet
Avoid NSAIDs because of high risk for AKI !!
Diabetic ketoacidosis
CS: Vomiting, decreased appetite, diarrhea, dehydrated, hypovolemic, can be mentally altered, kussmal breathing
ID: Hyperglycemia (point of care), ketones, UA, UCS, AUS and CXR
TX: Fluids, insulin, electrolyte support, GI meds, Antibiotics NE tube
Hemorrhagic gastroenteritis HGE
MOA: sm dogs
CS: dietary indiscretion, vomiting, hemorrhagic diarrhea, dehydrated, hypovolemic, abd pain, mentally altered
ID: abdominal US, Hypotensive, Hypoalbuminemic, high BUN/Crea, Hemoconcentration w/ low TS(PCV >55), Parvo snap
TX: fluids, analgesia, NG tube, GI meds, antibiotics, anthelmintics
Heat Related Illness
Presentation: Hypovolemic, distributive shock
Heat exhaustion: Dizziness, headache, nausea, weakness, unsteady gait, muscle cramps fatigue
Heat stroke: Change in mental status, loss of consciousness, and a core body temp >104 F
Multiple organ failure occurs 107°-109°F
ID: Shock, high PCV, high PLT, increased LES, AKI, electrolyte derangements, hypoglycemia, Rhabdomyolysis, DIC
owners may have cooled, temp may not reflect
TX: cold water immersion, evaporative cooling, crystalloids fluids, O2 for all dogs, FF plasma if coagulation issues, fans, ice packs
Dogs: crystalloid boluses of 10–20 ml/kg
Cats: crystalloid boluses of 5–10 ml/kg
Cool first transport second
Goal = 103F, stop cooling down
Avoid ice water: causes vasoconstriction
Add antibiotics if hypoglycemic, GI distress, sepsis, low WBC, aspirated pneumonia
Time-dependent: 10-20 days, 2 months for complete
acclimatization
Effects: CNS, Renal, GIT, Cardio, Respiratory
Anaphylaxis
Path:
IgE (type 1): no initial rxn, immediate rxn w/ repeat exposure
IgG (type II-IV): no prior exposure needed for rxn
Mediated: mast cells/basophils w/ histamine, Liver/GIT in dogs, resp in cats
CS: acute low BP, resp distress, multi system involvement
Cutaneous only is NOT anaphylaxis
Crazy high ALT
TX: Fluids, Epi, O2 in cats, antihistamine, Glucocorticoids(dex), bronchodilators
Epi: Vasoconstriction, bronchodilation, increase cardiac output, do not give subQ
H1+2: (1) diphenhydramine, chlorpheniramine, cyproheptadine,(2) famotidine, ranitidine, and cimetidine
Bronchodilators: albuterol, Aminophylline

Burns
Superficial Burns (1d): epidermis
Partial-thickness Burns (2d): Epidermis + dermis
CS: blisters, drainage, scaring
Full-thickness Burns (3d): epidermis + dermis + SQ
4d: muscle/tendon involvement
CS: charred, lacks sensation, less painful, scaring, shock, systemic dx
Rule of 9 BSA eval: head+neck (9%), front leg (9%), chest (9%) abdomen (9%), ½ back (9%), ½ back leg (9%)
TX: dressings, pain relief, fluids, oncotic support, nutrition
Sepsis
Path: organ dysfunction from dysregulated host response to infection
Vaso disregulation -> inflam imbalance -> microcercuation dysfunction -> coagulation dx -> immune downreg -> MODS
MOA: bacti, viral, fungi, bugs, GI perforation (dogs)
CS: MM, CRT, HR/RR/temp changes, altered mentation, low BP, hypovolemic/vasodilatory shock, hypoglycemia, peritonitis
ID: Leucocytosis, leukopenia, low PLT, anemia (cats), high bilirubin/BUN/Crea, Low albumin/Ca,
SIRS (TPR), SOFA, qSOFA, BP, MDB: Lactate, PCV/TP, BG
TX: crystalloid fluids, antibiotics (<1h), vasopressors (, norepi <6h), hydrocortisone, gastroprotectants, nutrition, physio, SX (<12h)
Acute kidney injury
Pre-renal: reduced BF, >1.030
hypotension, shock
Intrinsic Renal: kidney injury, 1.005-1.030
Lepto, ethalyne glycol, grapes, lilies, NSAIDs, antibiotics, lyme
Post-renal: increased kidney pressure <1.030
urinary tract obstruction
CS: PU/PD, lethargy, hyporexia, anorexia, vomiting, stranguria, bradycardia, neuro signs
ID: Differentiated with USG, Oliguria < 0.5ml/kg/day
TX: fluids, diretics’, antibiotics
Urethral obstructions
MOA: water intake, stress, diet, infection
CS: Pollakiuria, Dysuria, Stranguria, Hematuria, Pigmenturia, Vomiting, Lethargy, Abnormal posture, Vocalization
ID: palpate (do not try and express), POCUS for rupture, rads for cystoliths, hyperkalemia
TX: buprenorphine (pain), Gaba (stress), fluids, unblock, Ca gluconate/insulin/dextrose/Terbutaline (hyperkalemia)
Unblocking: Male Cats: emergency
Cats: Catheters w/ rads after, freeze red rubber, decompressive cystocentesisclip lg, sterile prep, pull urethra to straighten, lube, flush
Dogs: catheters, Pulling the legs back or forward away, flush vestibule
UTI risk dogs>cats

Ureteral obstruction
CS: Abdominal pain, hydronephrosis, AKI, azotemia, hyperkalemia, metabolic acidosis
ID:US, rads
TX: suburethral bypass device (SUB) placement
Uroabdomen
MOA: Secondary to severe UO or trauma
ID: FF present, azotemia, hyperkalemia, contrast radiographs
Potassium fluid to blood ratio of >1.4:1
Creatinine fluid to blood ratio of >2:1
TX: IVFT, Ca gluconate/insulin/dextrose/Terbutaline (manage hyperkalemia), Urinary divergence
Seizure Definitions
Status epilepticus: seizure > 3-5 minutes
Cluster seizures: > 1-2 within 24 hours
Differential diagnosis for seizures
Degenerative
Intracranial: storage diseases, several months old
Anomalous: Young dogs more likely have infectious diseases, congenital malformations or toxins
Extracranial: insulin overdose, hunting dog exertional hypoglycemia
Intracranial: hydrocephalus (chihuahua)
Metabolic
Extracranial: hypoglycemia, addisons, hypocalcemia, sepsis, hepatic encephalopathy/liver failure, erythrocytosis, severe anemia
Nutritional, neoplastic: Old dog likely have neoplasia, Brachycephalic have gliomas, Dolichocephalics have meningiomas
Extracranial: paraneoplastic
Intracranial: primary neoplasia, secondary neoplasia
Idiopathic (6m-6y), infectious, inflammatory: Toy/small dogs MUE common
Extracranial: sepsis
Intracranial: epilepsy, MUE, Distemper, neospora, Toxo, FIP, rabies, FIV/FeLV, fungal, protozoal
Idiopathic head tremor/bob: English and French Bulldogs as well as Boxers is NOT a seizure
Trauma, toxin: young dogs
Extracranial: Lead, Ethylene glycol, Organophosphates, /Carbamates, Pyrethroids, bromethalin, chocolate, illicit drugs, strychnine, metaldehyde, mycotoxins
Intracranial: penetrating wounds
Vascular: Old dogs
Extracranial: systemic hypertension
Intracranial: systemic hypertension
Treatment recommendations for seizures
Midazolam
5-10min
Levectram, Phenobarb
10-30min
Ketamine, Dex, Phenobarb, Inhalant
30min
Third line: everything and the kitchen sink
When to consider MRIs in seizure cases
Wait: 1st time in dog 1-5y w/ normal neuro exam
Go:
1st time in dog < 1 or > 6 years
Multi seizures over time
Lateralizing neuro deficits
Cats: they are WEIRD
aggression, dilated pupils, hypersalivation, vocalization
Monroe Kellie doctrine
volume of brain parenchyma, blood, and cerebrospinal fluid is constant due to closed calvarium
High ICP squishes brain
Cerebral perfusion pressure equation
CPP = Mean arterial pressure (MAP) – ICP
Cushing reflex
MOA: head injury/bleeding, space occupying lesions
Physio: Increased ICP, high BP, Low HR, Dysregulated RR
CS: Fatal, precedes brain herniation