OB Exam 3: Labor
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
What is
fetal presentation
fetal attitude/flexion
fetal station
fetal presentation:
part of baby that enters pelvis first
Cephalic, Breech, or shoulder
fetal attitude/flexion:
how baby holds body
chin tucked to chest, arms/legs flexed
fetal station:
how far baby’s moved down in pelvis (-5 to +5
0 station= head @ ischial spines
positive numbers= baby moving toward birth
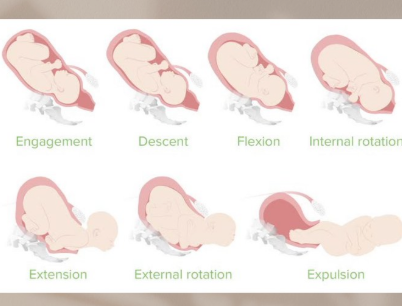
Whats the 7 mechanisms of labor:
engagement
head enters pelvis
descent
head through pelvis
flexion
infant chin to chest
internal rotation
head turns to fit pelvis
extension
infant chin up
external rotation (restitution)
realignment and shoulders
expulsion
baby delivered
*EDFIREEE
Stage 1 of Labor
2 stages
Early stage: onset of regular contractions till cervix is @ 4 cm
Active stage: cervix 5-10 cm
Stage 2 of Labor:
2 phases
Latent: delayed pushing, laboring down, passive descent till full dilation with urge to push (Fergusons Reflex)
Active: pushing (descent) till baby BORN
Stage 3 and Stage 4 of labor:
Stage 3: Placenta delivered
Stage 4: begins w/ placental delivery and includes @ least first 2hrs after birth
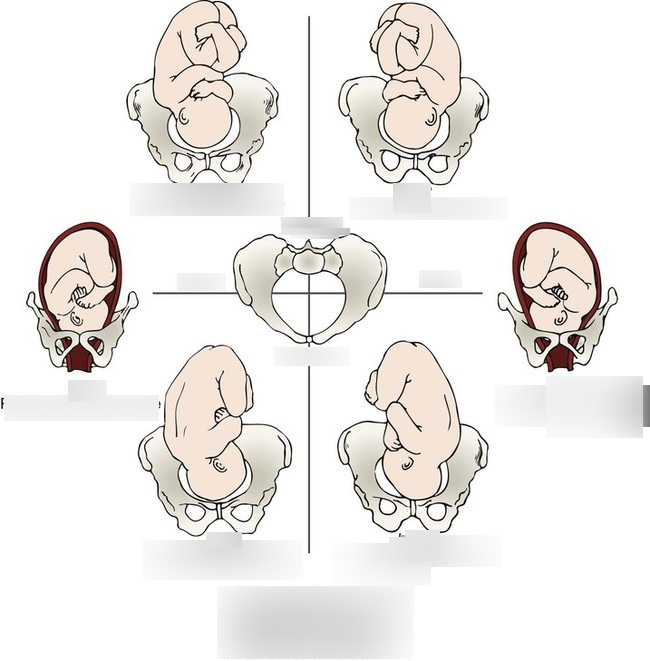
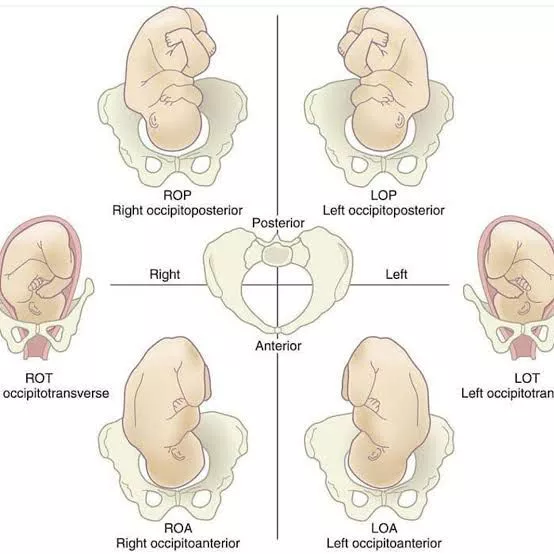
Determine the fetal positions:
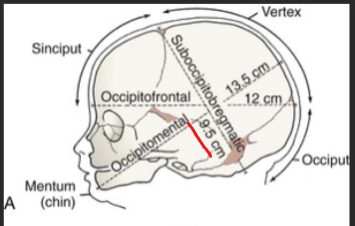
Whats the desired diameter of the fetal head through pelvis?
9.5 cm: when baby tucks head→ suboccipitobregmatic
if not tucked = 13.5 cm (baaad)
4 Categories of FHR variability:
variability= how much beat to beat fluctuation is there
absent 0
minimal 1-5 bpm
moderate 6-25bpm (normal!!)
marked >26 bpm
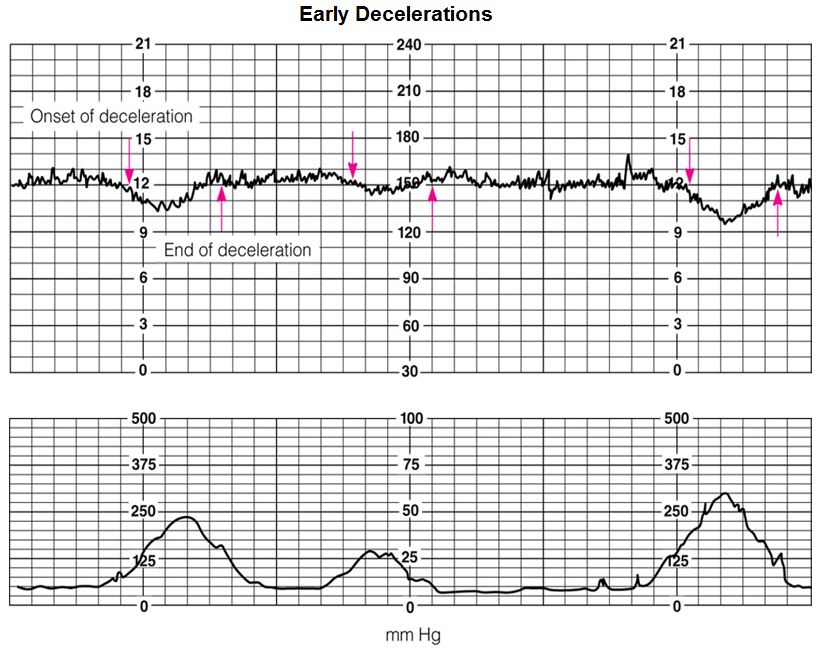
What are Early Decelerations?
cause?
gradual drop in FHR during contractions (GOOD)
mirrors contractions—goes down after peak and recovers before contractions end
cause: head compression (NORMAL)
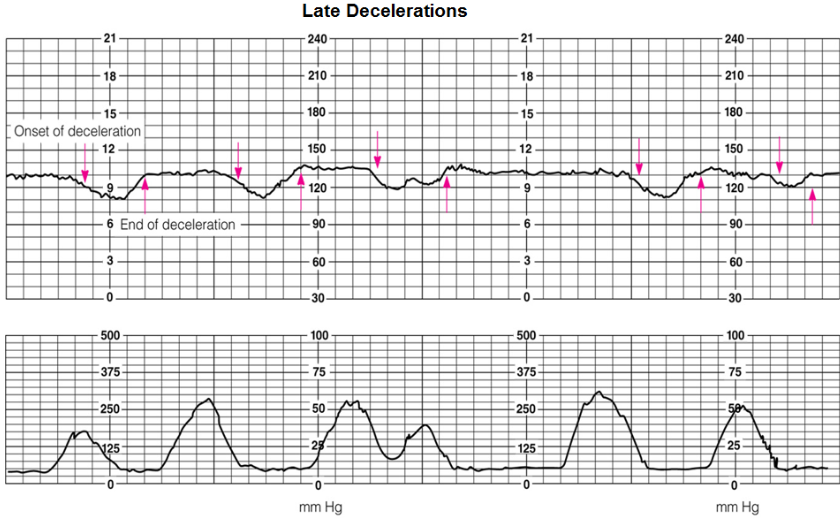
What are Late Decelerations?
cause?
FHR drops after contractions end
cause: placental insufficiency!! (BAD: baby not getting enough O2)
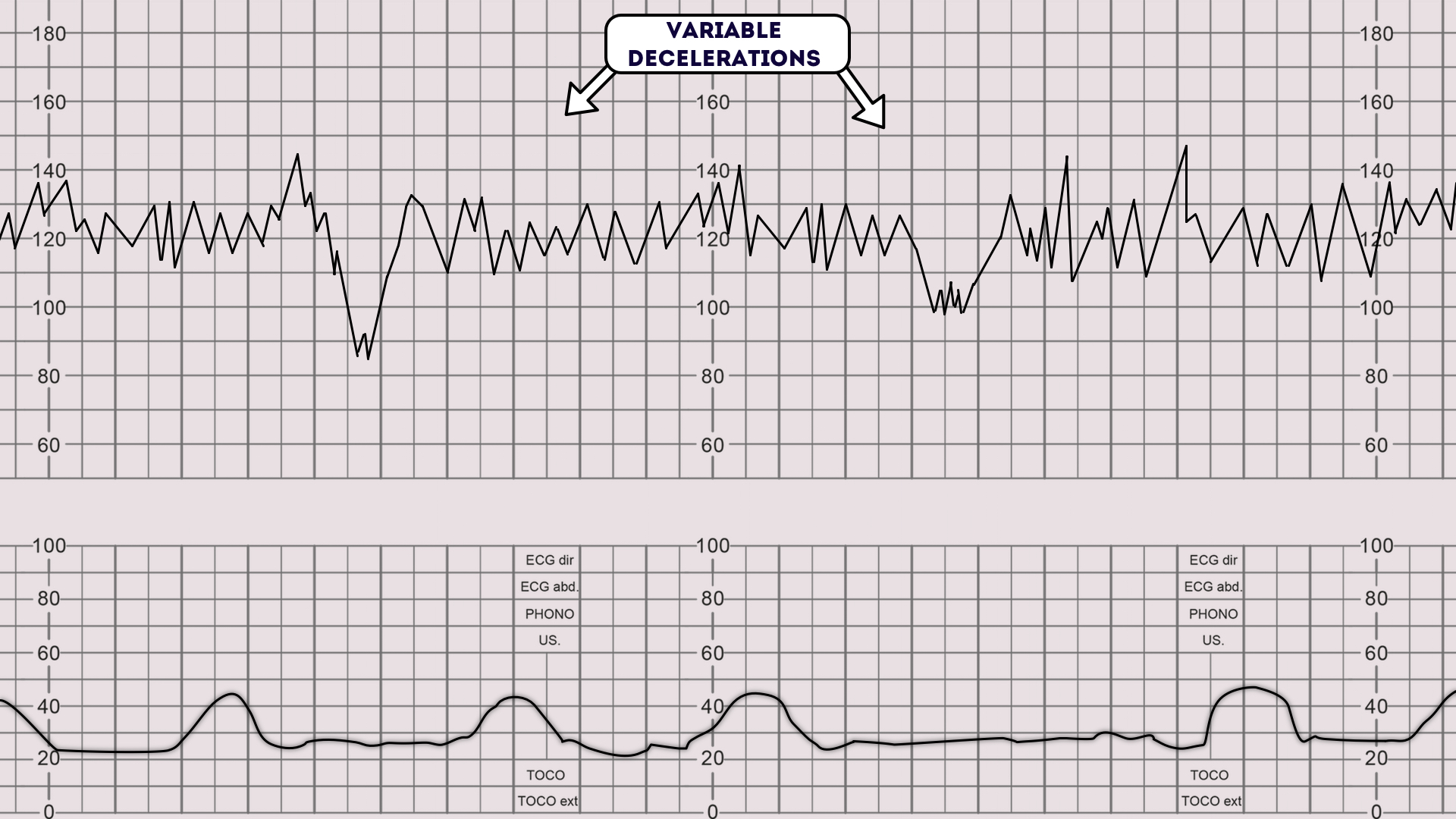
What are Variable decelerations?
cause?
sudden DROP in FHR (looks like U,V,W)
caused by umbilical cord compression→ change position!!
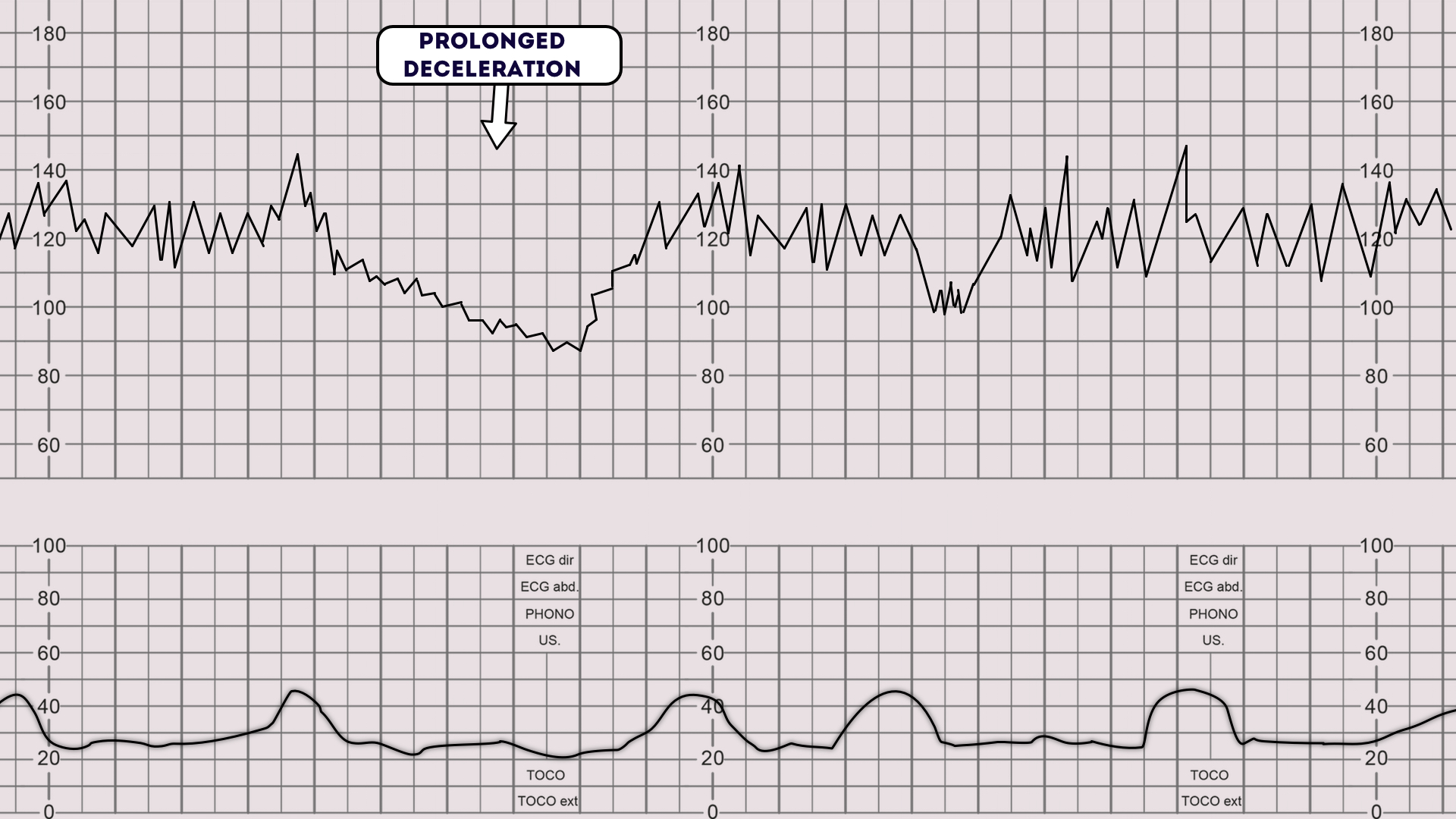
Prolonged decelerations
causes (5)
Drop in FHR > 15 bpm below baseline
Duration: 2-10 mins
maternal HTN
rapid cervical dilation
anesthesia
uterine tachysystole (too many contractions)
mom position compressing blood vessels
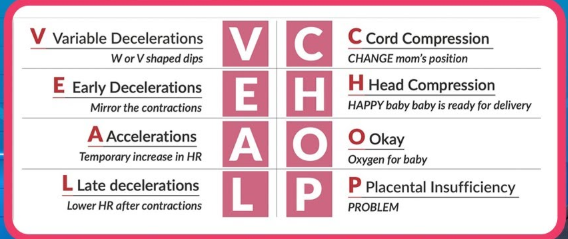
acronym for decelerations:
veal chop mine
Variable deceleration = Cord compression → Move pt (left side; hands and knees)
Early deceleration = Head compression→ Identify labor progression
Acceleration = OKAY!!→ Nothing
Late deceleration = Placental insufficiency→ Emergent delivery!
How do nurses assess uterine contractions (5) and rupture of membrane (4)?
uterine contractions
frequency: how often
duration: how long
intensity: strength
TOCOdynamometer
palpitation
rupture of membrane (aka water breaks)
color of fluid
odor
amount
time of rupture

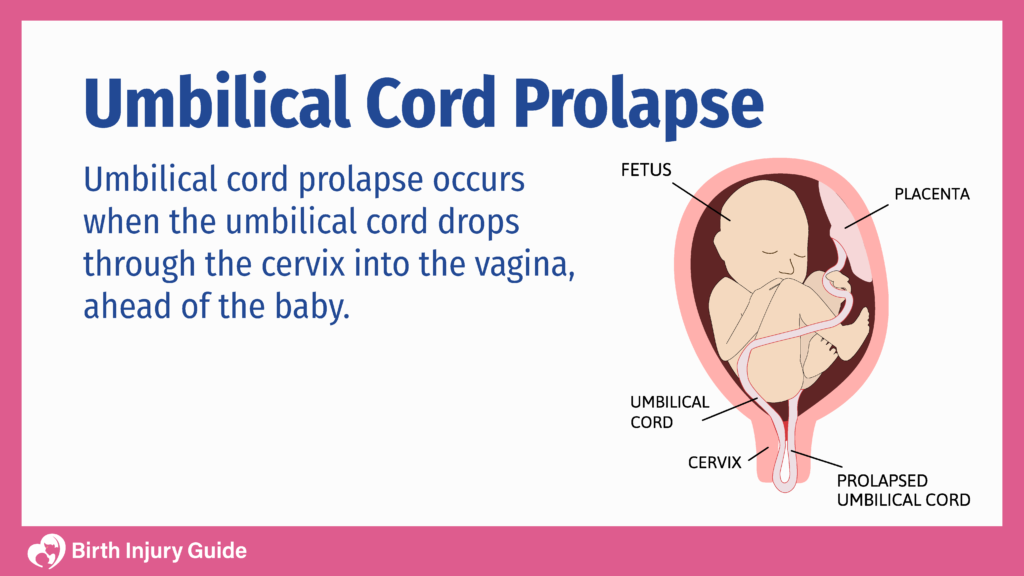
Whats priority after membrane ruptures??
Assess FHR!!!
rules out cord prolapse or abrupt deceleration caused by cord prolapse
What tests are needed if fetal membranes ruptured? (3)
Nitrazine test (pH test)
if paper turns blue= water broke
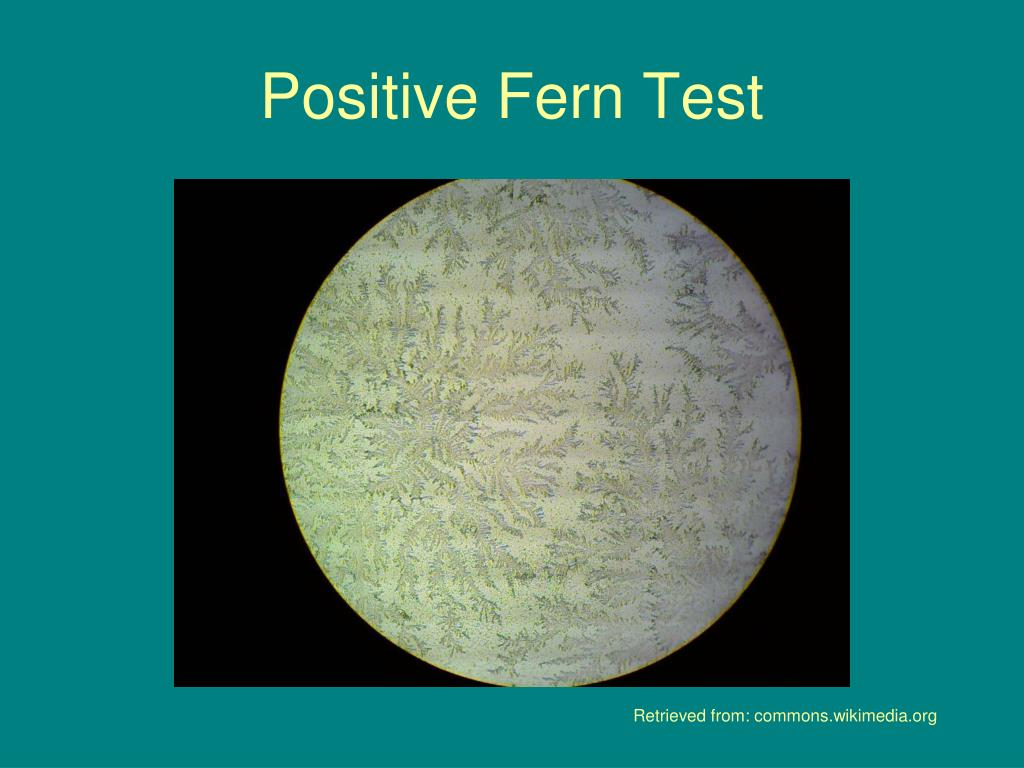
Fern Test
vaginal fluid under microscope
fern pattern/frost = water broke
AmniSure ROM Test (Immunoassay testing)
vaginal swab checks for protein found in amniotic fluid
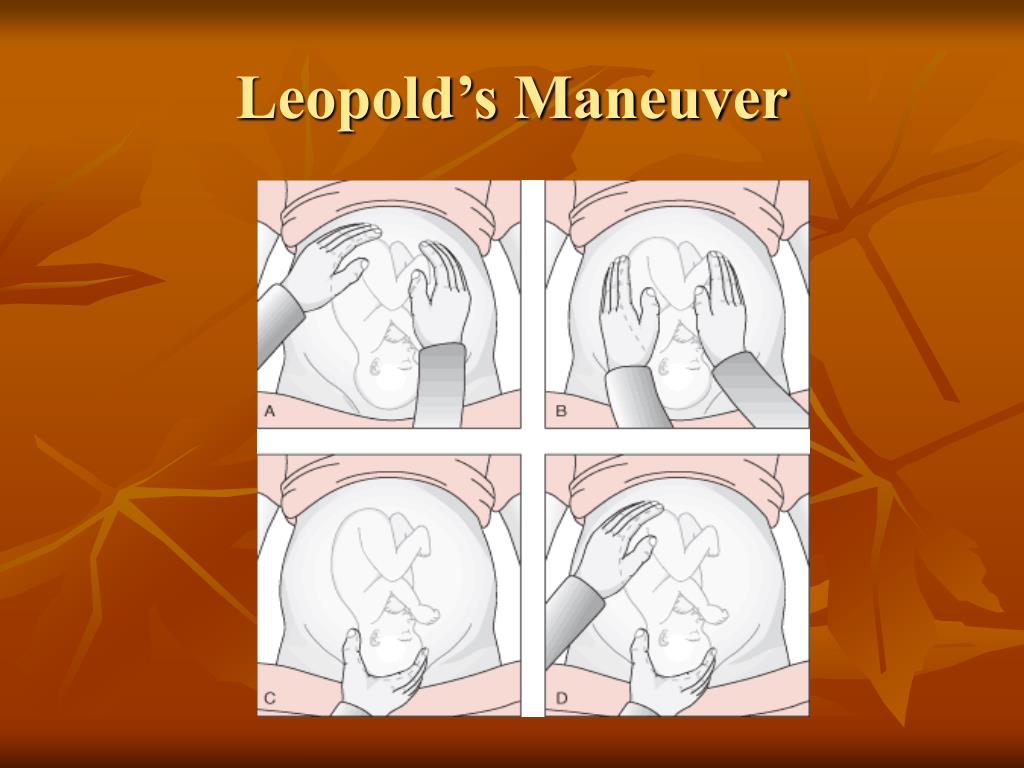
How to perform Leopold Maneuver: (4)
Is fundus hard or soft?
soft=butt (good)
Find fetal back
place monitor here
Squeeze fingers together above pelvis.
if no→ head is engaged or reached mid point of pelvis
Is head flexed?
chin tucked =good
What factors affect the progression of labor? (5 P’s)
Passenger: baby
Passageway: pelvis
Powers: contractions
Position of laboring women
Psyche: moms emotional state
Primary vs secondary powers of labor:
Primary: body doing active labor
Involuntary uterine contractions (laboring down)
effacement/dilation
Ferguson reflex (urge to push)
Secondary: adding to the process
Voluntary pushing efforts by mom (bearing down)
Valsalva maneuver (holds breath and push)

What interventions for Non-Reassuring FHR patterns? (4)
lay on left side 1st
STOP PITOCIN!!! (oxytocin)
IV fluids
amnioinfusion: especially useful if meconium stained/ low fluid
infusing LR or NS into amnio sac through intrauterine catheter
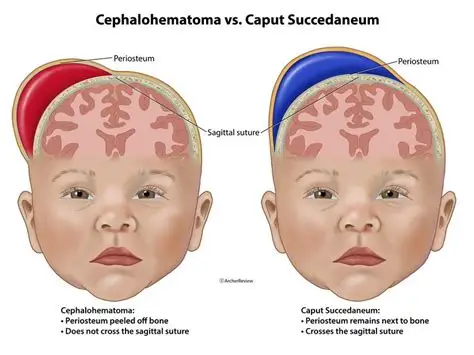
Caput Succedaneum and Cephalohematoma
Caput Succedaneum:
swelling of babys head during birth (normal)
Cephalohematoma:
bleeding bulge on ½ of head
Category I FHR: (4)
Normal w/ early decelerations (baby getting enough O2)
baseline 110-160 bpm
moderate variability (6-25 bpm fluctuations)
no late decelerations
Category II FHR: (4)
Intermediate (not normal but not dangerous yet)
minimal variability
brady/tachy-cardic
variable decelerations
Category III FHR:(4)
abnormal (baby may not be getting enough O2)
recurrent LATE decelerations (placental insufficiency- no O2 to baby)
recurrent Variable decelerations (cord compression)
bradycardia
needs immediate delivery!