NR-507 Alterations in Neurobiological Functions latest exam ( 112 questions and answers )
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
112 Terms
Bipolar Disorder
Anticonvulsants
combined with other medications to treat Bipolar disorder; may improve both mania and depression symptoms
Dysthymia is a persistent depressive disorder used to describe milder symptoms of depression that happen over longer periods of time.
True
False
This statement is true. Dysthymia is a persistent depressive disorder used to describe milder symptoms of depression that happen over longer periods of time.
Despite the different classifications, all antidepressant medications are equally effective in reducing the major symptoms of major depressive disorder.
True
False
This statement is true. Despite the different classifications, all antidepressant medications are equally effective in reducing the major symptoms of major depressive disorder.
Selective Serotonin Reuptake Inhibitors are the most common antidepressants prescribed.
True
False
This statement is true. Selective Serotonin Reuptake Inhibitors are the most common antidepressants prescribed.
The Monoamine Deficiency Theory states that the underlying basis of depression is low levels of serotonin, norepinephrine and dopamine.
This statement is true. The Monoamine Deficiency Theory states that the underlying basis of depression is low levels of serotonin, norepinephrine and dopamine.
Electroconvulsive Therapy (ECT) is no longer used as a treatment of major depressive disorder (MDD).
True
False
This statement is false. Electroconvulsive Therapy (ECT) is still used as a treatment of major depressive disorder (MDD).
Depression
Major Depressive Disorder (MDD) is known as clinical depression where approximately 20% of females are clinically depressed compared to males at 12%. To be clinically depressed means that the symptoms experienced interfere with the individual's daily life. It leads to an overall feeling that life is not an enjoyable experience. The exact cause of MDD is unknown, but most likely due to a combination of genetic, biologic and environmental factors.
MDD-Genetic Factors
Family members who have depression are three times more likely to have it themselves. This link tends to increase with how close the members are related.
MDD- Biological
From a biological perspective, most medications used to treat depression focus on the neurotransmitters of the brain. Neurotransmitters are signaling molecules that are released by one neuron and received by receptors of another neuron. A message is relayed from one neuron to the next. Regulation of how many neurotransmitters are being sent at any given time plays a significant role in the development of the symptoms of depression since they are involved in the regulation of many brain functions like mood, attention, sleep, appetite and cognition
MDD-Neurotransmitters
The three major neurotransmitters that are involved in the development of depression are serotonin, norepinephrine and dopamine. These are significant because medications that cause there to be more of these neurotransmitters in the synaptic cleft (the space between the neurons) are shown to be effective antidepressants.
Monoamine Deficiency Theory
the underlying basis of depression is low levels of serotonin, norepinephrine and dopamine. These are known as monoamines because they have one amine group. In addition, it is thought that each of these may have an impact on certain sets of symptoms of depression
Serotonin
Obsessions and compulsions
Some theories believe it also regulates the other neurotransmitters.
Norepinephrine
Anxiety and attention
Dopamine
Attention, motivation, and pleasure
Tryptophan Depletion
This is the amino acid that the body uses to make serotonin. If there is a decrease in tryptophan, there will be a decrease in the production of serotonin. Without a normal level of serotonin, individuals begin showing symptoms of depression.
Post Partum Depression
Post-partum depression occurs following childbirth. Although studies have shown that it can occur prior to childbirth as well. The actual diagnosis is Depressive Disorder with Peripartum Onset because the onset occurs during pregnancy or four weeks following delivery. The cause is generally unknown but is suspected that hormonal factors play a role in its development, especially estrogen and progesterone. The impact of childbirth on lifestyle may also play a role in its development because it can happen in men as well as in women.
Atypical Depression
Atypical depression is characterized by an improved mood when exposed to pleasurable or positive events. This is known as mood reactivity in contrast from other subtypes like melancholy even during what used to be pleasurable events. Atypical depression also includes the symptoms of weight gain, increased appetite, oversleeping, heavy feeling limbs (leaden paralysis) and rejection sensitivity where the individual feels anxiety at thoughts of rejection.
Dysthymia
Dysthymia is a persistent depressive disorder used to describe milder symptoms of depression that happen over longer periods of time, specifically over two or more years with at least two of the following symptoms:
Change in appetite
Change in sleep
Fatigue or low energy
Decreased self-esteem
Decreased concentration
Feelings of hopelessness or pessimism
MDD-Physical Activity
Physical activity is thought to be related to the release of neurotransmitters, endorphins, and endocannabinoids as well as raising the body temperature to cause muscle relaxation. Regardless of the exact mechanisms, data suggests that exercising for 20 minutes for three times per week can help alleviate symptoms of depression.
MDD-Diet
Diet may also impact symptoms of depression. Some research suggests that healthy eating habits with increased consumption of fruits and vegetables may play a role in reducing depressive symptoms.
MDD-Psychotherapy
Psychotherapy is "talk therapy" that is preferred for younger individuals and those who have mild symptoms. Techniques include cognitive behavioral therapy and interpersonal therapy. The most important point is that success of these techniques depends significantly on the individual's relationship with the therapist as well as the clinical skills of the therapist. In more severe depression or for long-term symptoms of depression, pharmacologic intervention is indicated. Motivational interviewing is an encouraged communication technique that helps to influence change in the individual's behavior through exploring and resolving ambivalence to the change and then helping the individual facilitate the change. It is a collaborative process that involves the use of open-ended questions, affirmations, reflections and summarizations.
MDD-Electroconvulsive Therapy (ECT)
Electroconvulsive Therapy (ECT) is usually tried when all other treatments have failed. A small electrical current is passed through the brain while patients are under general anesthesia. It induces a brief seizure. Although ECT has been used for many years and seems to be effective for at least some patients.
Antidepressant-SSRI MOA
Selective Serotonin Reuptake Inhibitors (SSRIs): these are the most common antidepressants prescribed. In the synaptic cleft, after neurotransmitters get released, they are normally reabsorbed. Selective Serotonin Reuptake Inhibitors (SSRIs) block the reabsorption or inhibits the reuptake of serotonin that allows for more of it in the synaptic cleft.
SSRI Side Effects
nausea, headaches, restlessness and insomnia.
Antidepressant-SNRI MOA
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): these drugs increase levels of serotonin and norepinephrine in the brain by blocking or delaying their reuptake by nerves. Norepinephrine is another neurotransmitter that regulates emotions and thought processes. They are also weak inhibitors of dopamine reuptake
SNRI Side Effects
insomnia, dizziness, weakness, hypotension, tachycardia and diaphoresis.
Antidepressant-Mirtazapine
Who should NP avoid prescribing this to?
the obese patient with diabetes as it increases appetite and weight, thus leading to poor glycemic control in the patient.
Depressive Symptoms
Symptoms consistent with depression include:
Depressed mood
Fatigue/loss of energy
Loss of interest/Anhedonia
Feeling worthless or having excessive guilt
Insomnia or hypersomnia
Poor concentration
Recurrent thoughts of death, suicide, a suicide plan or attempt
Psychomotor agitation or retardation
Which of the following symptoms would prompt the NP to refer the patient to a psychiatrist?
Psychotic symptoms.
Suicide ideation.
Patient's request.
All of the above.
All conditions would prompt the NP to refer the patient to a psychiatrist.
Amitriptyline (Elavil) is an alpha-agonist that increases synaptic concentration of serotonin and/or norepinephrine.
Amitriptyline is a tricyclic antidepressant, not an alpha-agonist.
A mood disorder is a mental illness that causes the individual to have dramatic shifts in emotions, mood and energy levels.
True
False
This statement is true. A mood disorder is a mental illness that causes the individual to have dramatic shifts in emotions, mood and energy levels.
Which of the following can trigger a bipolar mood disorder?
Selective Serotonin Reuptake Inhibitors. (SSRIs)
Stimulant drugs.
Changes in circadian rhythm.
Life stressors.
All of the above.
All of these factors can trigger a bipolar mood disorder.
During a manic phase, the individual will experience a low self-esteem.
True
False
The individual will experience a high self-esteem.
Unipolar depression is characterized by extreme anxiety and hallucinations.
True
False
Unipolar depression is characterized by the same symptoms as MDD.
Individuals with family members who have bipolar disorder are ten times more likely to also have it.
True
False
This statement is true. Individuals with family members who have bipolar disorder are ten times more likely to also have it.
Bipolar Disorder
Bipolar disorder, formerly known as manic depression, is a mental illness that causes the individual to have dramatic shifts in emotions, mood and energy levels. It encompasses a wide range of symptoms and is classified according to the types of mood episodes exhibited. The individual shifts from extreme lows to extreme highs. The shifts do not happen moment to moment. Instead, they happen over several days or weeks. It is known that individuals with family members who have bipolar disorder are ten times more likely to also have it. The cause is unknown.
Bipolar Disorder- Genetic Factors
no single bipolar gene has been identified. But there are some variations of genes that may contribute. The genes are associated with serotonin signaling (SLC6A4, TPH2); dopamine signaling (SLA6A3, DRD4); glutamate transmission (DAOA, DTNBP1) and cell maintenance and growth (NRG1, BDNF, DISC1). Several brain differences have been observed in individuals with bipolar disorder. White matter hyperintensities and reduction in gray matter volume identified on MRI have been described in patients with bipolar disorder as well as increased ventricular size and decreased frontal cortical area volumes.
Manic Episodes
They can be manic or hypomanic, depending on their level of severity. In a manic state, the individual can feel:
Energetic
Overly happy or optimistic
Euphoric
High-self esteem
Dangerous Characteristics of Mania
On the surface, these may seem like positive characteristics. But, when an individual is in a full manic episode, the symptoms can reach dangerous extremes where the individual exhibits:
Poor decision making without any regard to the consequences
Pressured and constant speech
Racing thoughts
Delusions of grandeur
Common Feature Between Bipolar 1 & 2
Unipolar Depression
Symptoms:
Low mood
Feelings of hopelessness and discouragement
Lack of energy and focus
Eating or sleeping too much or too little
Bipolar 1
Bipolar I involves a full manic or mixed episode. Manic episodes include major highs that can last at least a week or major lows that last for at least two weeks. Untreated manic episodes can last 3-6 months.
Bipolar 2
A Bipolar II disorder involves at least one major depressive episode and at least one hypomanic episode, but no full mixed or manic episode. The individual experiences similar lows (depression) as described for the individual with Bipolar I disorder and has additional highs called hypomania. Hypomania involves less severe manic episodes than seen in Bipolar I. To qualify for a diagnosis, the hypomanic states must last for at least 4 days, but generally last from a few days to a few months.
Bipolar Disorder
Mood Swings
The average healthy individual may have normal and healthy ups and downs throughout life, including serious lows as when experiencing a situational event such as a death or loss of a job. An individual with unipolar depression, though, might have normal highs, but are also likely to have significant lows that last for an extended time period without an obvious trigger.
Bipolar 1-Summarized
More severe
One or more manic or mixed episodes leading to:
Serious problems
Hospitalization
Psychotic features
Bipolar 2-Summarized
One or more hypomanic episodes (4 days or more), and no mania
One or more major depressive episodes (2 weeks or more)
Cyclothymia
Alternating between hypomanic symptoms, and mild or moderate depressive moods, like Bipolar II
Less severe, higher functioning
Rapid Cycling
4 or more episodes of acute mania within 1 year
Classic Euphoria Mania
Circumscribed episodes
Low levels of comorbidities
Lithium responsive
Good prognosis
Dysphoria or Mixed Mania
Increased severity of episodes
Rapid cycling
Anxiety/Spectrum Substance use disorders
Increased suicidality
Unresponsive to lithium
Poor psychological functioning
Bipolar Disorder
Lithium salts
Lithium acts as a mood stabilizer. It seems to be more effective at treating mania rather than depression symptoms.
Bipolar Disorder
Antidepressants
these can be problematic since SSRIs can trigger manic episodes in individuals who are predisposed to them.
Bipolar Disorder
Benzodiazepines
Antianxiety medication that slows the activity of the brain resulting in reduction of mania, anxiety and panic disorder
Bipolar Disorder
Antipsychotics
acts on dopamine receptors to reduce levels of excess dopamine. It exhibits high affinity for D2, D3, 5-HT1A, and 5-HT2A receptors
In a mixed episode, the individual experiences symptoms of depression and mania simultaneously.
True
False
This statement is true. In a mixed episode, the individual experiences symptoms of depression and mania simultaneously.
Talk therapy and cognitive behavioral therapy are not helpful in treating the manic episodes of bipolar disorder.
True
False
This statement is true. Talk therapy and cognitive behavioral therapy are not helpful in treating the manic episodes of bipolar disorder.
In rapid cycling, the individual has 4 or more episodes of depression and mania within one year.
True
False
This statement is true. In rapid cycling, the individual has 4 or more episodes of depression and mania within one year.
Lithium is best at treating both manic and depressive episodes.
True
False
Lithium is best at treating manic episodes.
Major depression is required to be present in order to diagnose Bipolar 1 and Bipolar 2 disorder.
True
False
Major depression may be present in both but are not required for the diagnosis.
Physical manifestations can also be associated with Generalized Anxiety Disorder
True
False
True
Cognitive behavioral therapy has major advantages over medications in the long-term treatment of anxiety
True
False
True
Generalized Anxiety Disorder (GAD) is episodic in nature that is brought on by stressful situation
True
False
False
GAD is characterized by excessive, persistent, unreasonable anxiety about everyday situations
Benzodiazepines are drugs that reduce depression associated with the individual's anxiety.
True
False
False
Benzodiazepines are psychoactive drugs that reduce anxiety by providing a calming effect on the individual.
Psychotherapy helps the individual to think and act in different ways to deal with stressful situation
True
False
True
Generalized Anxiety Disorder
Anxiety is associated within areas of the brain such as the amygdala that is associated with the limbic system. It is responsible for processing memory and emotions related to the fight or flight response. This is regulated by different neurotransmitters.
GAD-Neurotransmitter
Norepinephrine
this neurotransmitter is involved in the fight or flight response. The feeling of anxiety triggers norepinephrine release that leads to the physical manifestations associated with anxiety. These include tachycardia, increased blood pressure, tremors, and diaphoresis.
GAD-Neurotransmitter
Serotonin
Serotonin is a modulator of a several factors that are associated with anxiety, including modulating the release of norepinephrine and corticotropin-releasing factor.
serotonin acts as an inhibitory neurotransmitter (found in the raphe nuclei). Alterations in serotonin here will affect the serotonin-reuptake transporter and the post-synaptic serotonin receptors to cause more sensitivity to anxiety
GAD-Neurotransmitter
Corticotropin-releasing hormone system
Through the mechanism of the hypothalamic-pituitary-adrenal axis, it causes hormones to become released that contributes to the feeling of anxiety. There are also primary excitatory and inhibitory neurotransmitters (y-aminobutyric acid (GABA) and glutamate that when imbalanced, will contribute to anxiety.
GAD
Noradrenergic Factors
Individuals who are prone to anxiety will have hypersensitivity to stimuli. When the individual experiences fear, it activates the locus ceruleus to stimulate the release of norepinephrine. Once norepinephrine is released, the sympathetic and parasympathetic nervous system is activated. Corticotropin-releasing factor will stimulate the release of cortisol (stress hormone) to cause a stress response. Over time, the stress response becomes hypersensitive and dysregulated which can lead to chronic anxiety.
GAD-GABA
GABA is the major inhibitory neurotransmitter that helps to regulate serotonin, norepinephrine, and dopamine systems. When GABA is enhanced or the increased utilization of GABA in the brain, it causes anxiolysis, which is the release of anxiety.
GAD-Prevelance
It can be prevalent in individuals who have family members with GAD. It is also twice as prevalent in females than in males.
GAD-Symptoms
Worry and anxiety
Edginess and restlessness
Difficulty concentrating, and irritability
Overeating or undereating
Muscle aches due to tension soreness and difficulty sleeping. Lack of sleep can lead to issues of chronic fatigue.
GAD-Diagnosis
DSM-5
Excessive anxiety present for more days than not for over six months (90 or more days out of 180 days). It is difficult, though for individuals to quantify or track their feelings in this way. Therefore, this is just a general guideline on how to identify GAD.
Inability to control anxiety that indicates they are unable to calm themselves or regain control over their feelings.
Adults must have three of more of the symptoms listed above. In children (6-18-years of age), though, only one symptom is needed for the diagnosis.
The anxiety causes impairment in daily life activities. This is evident when the individual is unable to meet deadlines or go to work because of their symptoms.
The symptoms cannot be attributed to the effects of drug abuse or medications or due to a medical condition as in the case of hyperthyroidism.
The symptoms are not better explained by another medical disorder, including social phobia or panic disorder.
GAD-Psychotherapy
This involves cognitive behavioral therapy. It can help the individual to think and act in different ways to react to stressful situations.
Better long term effects due to unwanted side effects of medications such as tolerance, dependance, and withdrawal
GAD-Medication
Benzodiazepines which are psychoactive drugs that provide a calming effect on the individual.
Antidepressants which include Selective Serotonin Reuptake Inhibitors (SSRIs). These regulate the serotonin levels in the brain to help elevate mood.
Social Anxiety Disorder
fear of being judged negatively by others to the point that it affects their ability for the individual to perform daily activities. In fact, the idea of having to attend an event where the individual perceives that there will be negative judgements may invoke feelings of not wanting to go or complete, for example, a work-related activity
Social Anxiety Disorder-DSM-5
The DSM-5 defines social anxiety disorder as the individual's fear of acting in a certain way that might cause judgement by others. It also interferes in the individual's normal routine and relationships with others. The anxiety is also persistent, lasting greater than six months.
Performance Anxiety
Performing in front of others. This is called performance anxiety. which can impair the individual from giving a presentation.
Social Anxiety Disorder-Explained
Social anxiety is an ego-dystonic condition where the individual who has the disorder usually understand that their anxiety is unwarranted. This can cause even more anxiety because of fear that others can perceive the anxiety felt by the individual. Sometimes the individual may worry about the presence of physical symptoms such as trembling or blushing that other mays notice. Sometimes the anxiety can become so severe that derealization occurs. This is where the individual can feel "spaced-out" and unable to recognize their surroundings. In order to reduce social inhibitions, the individual may resort to drugs and alcohol that can lead to dependency and addiction.
Social Anxiety Disorder
Psychotherapy
Psychotherapy
Cognitive behavioral therapy is the technique most often recommended. It helps the individual to acquire new ways of thinking and behaving when around others.
Social Anxiety Disorder
Medications
Antidepressants are the most common medications used to treat social anxiety disorder, specifically Serotonin Selective Reuptake Inhibitors (SSRIs) that regulates serotonin levels in the brain and Serotonin Norepinephrine Reuptake Inhibitors (SNRIs) that help regulate serotonin, norepinephrine and dopamine.
Benzodiazepines: are psychoactive drugs that have a relaxing effect.
Beta-blockers: can help ease the physical symptoms of performance anxiety.
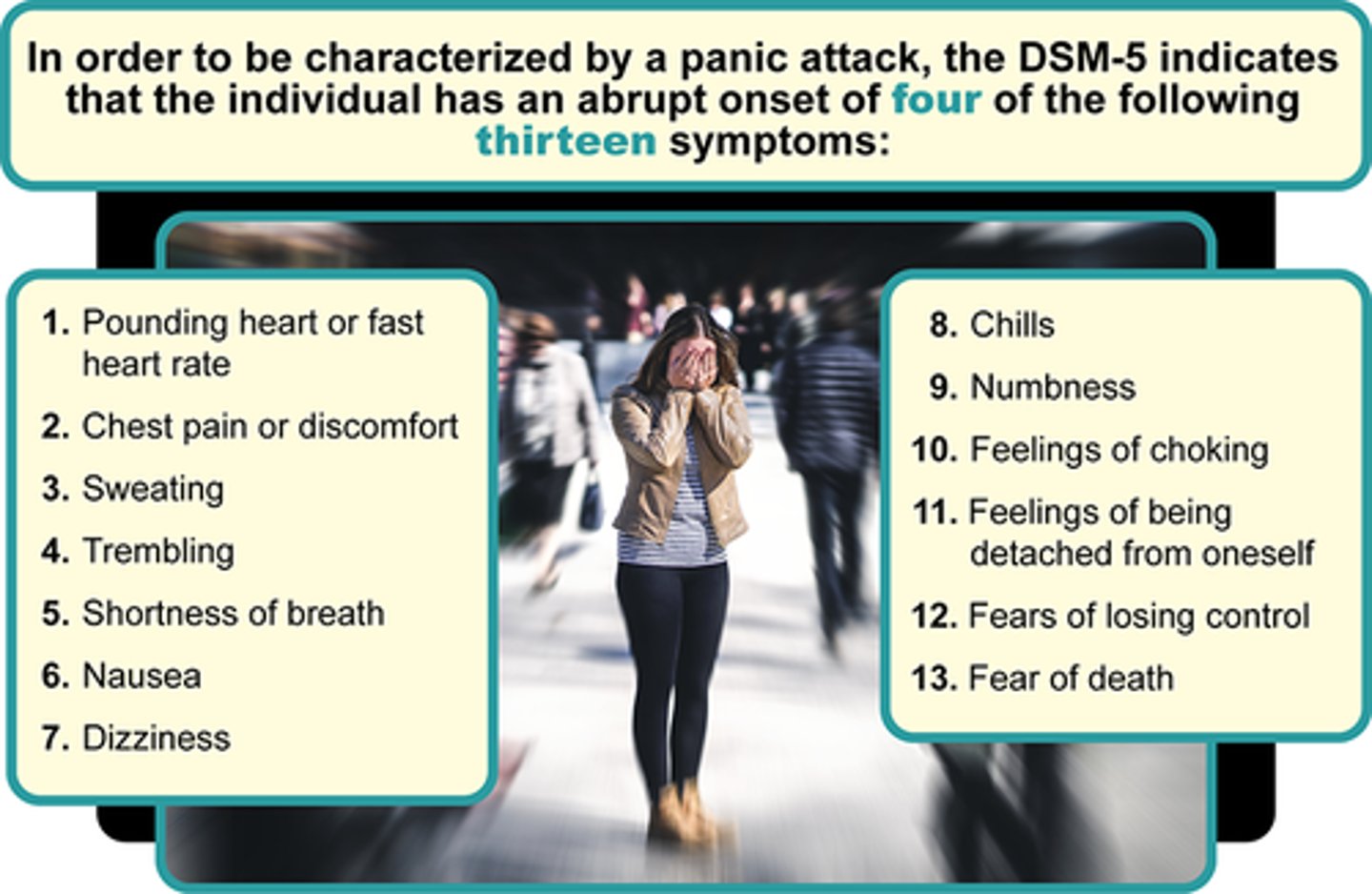
Panic Disorder
A panic attack involves a very stressful situation where the individual develops an intense fear that something bad will happen. An imminent threat or danger is also perceived. These feelings are often so intense that they can be accompanied by physiological symptoms such as heart palpitations, dizziness or shortness of breath. The symptoms typically peak within the first ten to twenty-minutes, but some may last for hours. The individual will sometimes describe the feeling of having a heart attack or some other life-threatening illness. A panic attack can be unpredictable because they can happen even in familiar places where there are no real threats. This can further increase anxiety, as the individual begins to anticipate when the next panic attack might happen.
Panic Attack Characteristics
...
Panic Attack Occurrences
Panic attacks can also happen in the presence of other mental disorders that include depressive disorders, post-traumatic-stress syndrome (PTSD), and substance abuse disorder. It can also happen in the context of a panic disorder which is defined by the panic attack being:
Recurrent (two or more) and unexpected
Persistent worry, change in behavior because of the panic attacks
Not due to the effect of a substance including medication and illegal substance
Not explained by some other anxiety disorder such as social anxiety disorder and agoraphobia
Panic Attack-Psychotherapy
Cognitive behavioral therapy is an effective intervention that relies on five steps:
Learning about the panic disorder and how to identify certain symptoms
Monitoring the panic attacks using a diary
Using breathing and relaxation techniques
Changing beliefs about the severity of the panic attack to achieve a realistic level of thought
Exposure to situations that evoke fear and anxiety
Panic Attack-Medications
Antidepressants: Serotonin Selective Reuptake Inhibitors (SSRIs) are commonly prescribed to create a relaxing effect
Benzodiazepines: can decrease anxiety and have a relaxing effect
Antiseizure medication: will be used if the panic attacks are severe
Overall, with the combination of the above strategies, many patients can be effectively treated for panic attacks.
Serotonin Selective Reuptake Inhibitors (SSRIs) are commonly prescribed to create a relaxing effect in the anxious individual.
True
False
This statement is true. Serotonin Selective Reuptake Inhibitors (SSRIs) are commonly prescribed to create a relaxing effect in the anxious individual.
Monitoring the panic attacks using a diary can be an effective component of psychotherapy.
True
False
This statement is true. Monitoring the panic attacks using a diary can be an effective component of psychotherapy.
Which of the following is a situation where the individual may experience social anxiety?
Making small talk.
Sending out invitations to a party.
Setting the table for dinner guests.
All of the above.
Making small talk is the only choice that denotes actual interaction with others.
A panic attack involves a very stressful situation where the individual develops an intense fear that something bad will happen.
True
False
This statement is true. A panic attack involves a very stressful situation where the individual develops an intense fear that something bad will happen.
Antiseizure medication can be used in severe panic attacks.
True
False
This statement is true. Antiseizure medication can be used in severe panic attacks.
The cognitive symptoms of schizophrenia are subtle and may only be detected when specific tests are performed.
True
False
This statement is true. The cognitive symptoms of schizophrenia are subtle and may only be detected when specific tests are performed.
Which of the following would be considered a negative symptom of schizophrenia?
Flat affect.
Hallucinations.
Disorganized speech.
Delusions.
Flat affect is the only negative symptom listed. The other choices are positive signs of schizophrenia.
In the prodromal phase of schizophrenia, Individuals become hyperactive and outgoing.
True
False
Individuals become withdrawn.
More men than women seem to be affected by schizophrenia with onset in the mid-twenties.
True
False
This statement is true. More men than women seem to be affected by schizophrenia with onset in the mid-twenties.
Catatonic behavior involves bizarre movements, posture, and responsiveness.
True
False
This statement is true. Catatonic behavior involves bizarre movements, posture, and responsiveness.
Schizophrenia
The term "schizo" refers to split while "phrenia" refers to mind. Even though schizophrenia can be thought of a splitting of the mind, it does not refer to a split personality. Instead, schizophrenia is a scattered fragmented pattern of thinking. It is a syndrome that includes symptoms that are associated with it and different patients might experience different symptoms.
Schizophrenia Causes
The cause of schizophrenia is unknown. One thought is that most antipsychotic medications that improve schizophrenia blocks the dopamine receptor D2, which reduced dopamine levels in neurons. This suggests that one cause of schizophrenia relates to increased dopamine levels. Antipsychotics, though are not either universally or completely effective in its treatment and therefore, do not work for everyone. This implies that there is more to the cause of schizophrenia.
One of the most effective antipsychotic drugs, clozapine, is a weak D2 antagonist, which suggest that other neurotransmitter systems like norepinephrine, serotonin and gamma-Aminobutyric acid (GABA) are probably involved. There is also evidence to support a genetic basis for the development of schizophrenia, although no specific genes have been conclusively linked to schizophrenia. Environmental factors may also contribute to the development of schizophrenia that include early or prenatal exposure to infections and certain autoimmune disorders like Celiac disease.
Schizophrenia Epidemiology
One other factor to consider in the development of schizophrenia involves its epidemiology. More men than women seem to be affected by schizophrenia with onset in the mid-twenties for men and late twenties for women. The clinical signs of schizophrenia are often less severe in women. Some evidence supports the differences in the development of schizophrenia between men and women that estrogen regulation of dopamine may play a role.
Schizophrenia-Positive, Negative, and Cognitive Symptoms
The positive symptoms of schizophrenia are the psychotic symptoms. None of the positive symptoms occur physiologically. Negative symptoms involve the removal or reduction of normal processes. It is characterized by a decrease in emotions or a loss of interest in things that used to be interesting. Cognitive symptoms involve not being able to remember things.
Positive Symptoms
Psychotic symptoms:
Delusions: are thing that the individual feels strong about that they refuse to change their mind even if there is evidence against their stance:
delusion of control-some outside force is controlling their actions
Delusion of reference: insignificant remarks are directed at them
Hallucinations: any type of sensation that is not actually there (visual) of auditory-hearing things that are not there.
Disorganized speech: word salad- a random juggling of words or phrases.
Disorganized behavior: bizarre behavior that is out of context to the situation with no purpose (wearing a heavy coat in the summer).
Catatonic behavior: bizarre movements, posture, and responsiveness; stupor and unresponsive to moving.