1.2 - acute post-op management and pre-prosthetic training
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
pre-amputation
_______________ phase of amputation/prosthesis:
patients who are preparing for an amputation
pre-amputation
_______________ phase of amputation/prosthesis:
patients in the hospital outpatient clinic (ex. amputation, wound, diabetic)
pre-amputation
_______________ phase of amputation/prosthesis:
objectives - explain sequence of upcoming events, discuss expectations of provider and patient, pt ed, answer any questions
acute post-operative
_______________ phase of amputation/prosthesis:
patients in the immediate recovery from the amputation surgery
acute post-operative
_______________ phase of amputation/prosthesis:
patients in the acute care hospital
acute post-operative
_______________ phase of amputation/prosthesis:
objectives - prevent post-op medical complications, manage residual limb health, prevent loss of motion and physical deconditioning, promote basic mobility and self-care, promote sound limb care, assist with limb loss adjustment
prevent post-op medical complications
manage residual limb health (promote wound healing)
prevent contractures
what are the main objectives during the acute postoperative phase
pre-prosthetic training
_______________ phase of amputation/prosthesis:
patients whose residual limb is NOT ready to be fit with a prosthetic limb
pre-prosthetic training
_______________ phase of amputation/prosthesis:
patients who are in IPR, SNF, outpatient rehab, or home
pre-prosthetic training
_______________ phase of amputation/prosthesis:
objectives - manage residual limb health, address any ROM deficits, increase UE and LE strength, progress mobility and self-care, reinforce sound limb care, assist with limb loss adjustment
manage residual limb health (add scar management and limb shaping)
prevent contractures
LE strength
what are the main objectives during the pre-prosthetic training phase
prosthetic training
_______________ phase of amputation/prosthesis:
patients whose limb has healed enough to tolerate using a prosthesis
prosthetic training
_______________ phase of amputation/prosthesis:
patients in IPR, SNF, outpatient rehab, home, prosthetist clinic
prosthetic training
_______________ phase of amputation/prosthesis:
objectives - same as pre-prosthetic objectives, incorporate prosthesis use into activities, address community reintegration
lifetime care
_______________ phase of amputation/prosthesis:
any post-acute person with amputation
lifetime care
_______________ phase of amputation/prosthesis:
patients in an outpatient clinic or prosthetist clinic
lifetime care
_______________ phase of amputation/prosthesis:
objectives - maintain function and quality of life, promptly address any medical or prosthetic concerns

rigid
a _____________ dressing is a cylindrical plaster or fiberglass cast applied to residual limb immediately after surgery (in operating room)

5-7 days (or sooner: severe pain/pressure, significant loosening, or fever and oder present)
rigid dressing should be changed after _________

rigid
the advantages of ____________ dressing:
Best for limiting the formation of post-op edema (and pain)
Limits contracture formation
Protects residual limb (including incision)
Assists with desensitization, adjustment to socket weight.
Can allow early ambulation with the attachment of a pylon and foot (described with IPOP)
May allow earlier fitting of the definitive prosthesis

rigid
the disadvantages of _____________ dressing:
Requires careful application by a professional
NOT removable
Does NOT allow daily inspection

F (i made that up… the rigid dressing does NOT allow for daily inspection period)
T/F: the rigid dressing is made to check for pressure wounds daily

removable rigid
_______________ dressing is plaster cast or prefabricated shell worn over a soft dressing and held in place by a suspension belt or cuff

limb protectors
removable rigid dressing is also called ______________

soft
a removable rigid dressing uses ____________ dressings to fill volume as residual limb shrinks

removable rigid
______________ dressing is recommended as the first treatment of choice for a transtibial amputation

removable rigid
advantages of _____________ dressing:
Limits the formation of post-op edema
Provides residual limb protection
Can help prevent contracture formation
Promotes using socks regulate fit
Assists with desensitization, adjustment to socket weight
Allows daily inspection and dressing

removable rigid
disadvantages of _____________ dressing:
Require careful application by a skilled professional
Almost exclusively used with transtibial amputation
Requires an external suspension system

immediate post-operative (IPOP)
the __________________ prosthesis has a rigid or removable rigid dressings designed to allow attachment of temporary components

immediate post-operative (IPOP)
the intent of the ________________ prosthesis is to facilitate ambulating with both limbs as soon as possible

T (leads to functional gains and earlier discharge)
T/F: you can mobilize with the immediate post-operative prothesis (IPOP) within the first 3 days

immediate post-operative (IPOP)
advantages of the _______________ prosthesis:
Reduced extrinsic risks (i.e., falls etc.)
Facilitates healing
Promotes early fitting and training
Reduced inpatient length of stay and cost

immediate post-operative (IPOP)
disadvantages of the _______________ prosthesis:
hard to control WB

F (but we aren’t necessarily worried about it right now because we aren’t focused on gait)
T/F: the immediate post-operative prosthesis allows from knee flexion

soft
____________ dressing is the use of elasticized materials to provide an evenly distributed pressure gradient

soft
______________ dressing is the most used post-op dressing method
F (suture line needs to be healed)
T/F: the advantage of using a shrinker dressing is the ability to use it before the suture line heals

shrinker
____________ is used for shaping the residual limb and is the most commonly used soft dressing

soft
disadvantages of _____________ dressing:
Poor control of edema
Provides little protection
Requires careful application (ace-wrap) and some manual strength/dexterity
Can form a tourniquet
Requires frequent reapplication throughout day because of loosening and shifting (shrinkers < ace-wrap)

soft
advantages of _____________ dressing:
Inexpensive and can be laundered
Lightweight and readily available
Easily removable for limb inspection
A variety of pressure gradients are available
Can help with limb shaping
vascularity; sensation
the examination of acute post-op care for a prosthesis includes checking both limbs _____________ and the contralateral limb ____________
ischial tuberosity or greater trochanter → end of bone
when measuring bone length for a transfemoral amputation, measure from ______________ to _____________
medial tibial plateau → end of bone of redundant tissue
when measuring bone length for a transtibial amputation, measure from ______________ to _____________
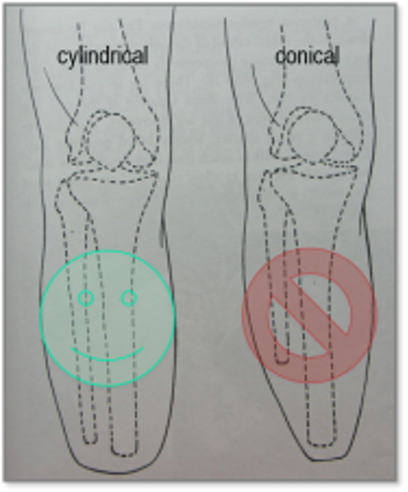
cylindrical; better pressure distribution, conical is too pointy
what’s better, a cylindrical or conical shape of the residual limb? WHY?
8-10cm
when examining the residual limb, measure the soft tissue circumference by every __________
phantom limb
________________ sensation is perceived as originating from the amputated limb
F (can occur immediately after the amputation)
T/F: phantom limb sensation occurs 24hrs after surgery
F
T/F: phantom limb sensation can be painful
phantom pain
_______________ is a painful sensation perceived as originating from the amputated limb
sensation
which is more common:
phantom sensation or pain
1-2 years
phantom pain usually decreases within __________

T
T/F: residual limb pain is NOT phantom

nerve
bone
vascular
wound
intrinsic factors that lead to residual limb pain (4)

cast pressure
socket fit
extrinsic factors that lead to residual limb pain (2)
reduce edema
**also for a candidate NOT using a prosthesis
control pain
**also for a candidate NOT using a prosthesis
wound (incision) healing
**also for a candidate NOT using a prosthesis
protect incision during functional activity
**also for a candidate NOT using a prosthesis
prevent contracture
**also for a candidate NOT using a prosthesis
facilitate preparation for prosthetic placement by shaping and desensitizing limb
what are the 6 post-op residual limb management goals?
Out of the 6 goals, which are also goals for a candidate is not going to use a prosthesis?
0-5 days
what is the timeline for the inflammatory healing phase?
5-21 days
what is the timeline for the fibroblastic (proliferative) healing phase?
begins at 21 days
when does the remodeling healing phase begin?
T (report any red or darker blood or thickened discolored drainage with odor)
T/F: clear drainage is normal for the first couple of days post amputation
tension
the ____________ theory of wound healing is that external stress can effect the strength of a wound and improve collagen organization
2 weeks; 3 weeks; 6 weeks
scar tissue mobility should begin above/below the scar for the first ________
after about __________ and once the wound is closed and there is no steri-strips you can mobilize directly over the scare after
continue scar tissue mobilization for about ___________ or until the epithelial line (lump under the skin) is gone
T (include in pt ed)
T/F: a patient can perform their own scar tissue mobilization
T (whenever they aren’t using their prosthesis)
T/F: a shrinker is often used for the rest of a person’s life
because it will put tension on the skin and the incision
why should a patient not pull the shrinker off like a sock???
24hrs a day for the rest of life
how often should a shrinker be worn
23 hours/day (removed for hygiene only)
how often should an ace wrap be worn
distal; proximal
when using ace wrap, the (proximal or distal) pressure should exceed the (proximal or distal)
4 hours
ace wrapping should be reapplied at least every ___________
F (use tape)
T/F: ace wrapping should be secured via metal clips
residual limb
________________ sensation is where the skin becomes hypersensitive to touch and pressure inhibiting dressing and prosthetic use
light touch or tapping
exposure to different textures
massage
wear prosthesis/compression bandages
what are 4 early and continual methods of desensitizing the stump
conservative and complementary
examples of a _______________ treatment approach for phantom and residual limb pain:
Compression, use of prosthesis, desensitization techniques
Ultrasound (heat), ice
Massage, Vibration Therapy
Electric Stimulation (TENS)
Acupuncture
Mirror Therapy
Note: May help prevent/lessen phantom pain (Purushothaman 2023 J Anesthesia)
Biofeedback to reduce muscle tension
Psychological Interventions (motor imagery and relaxation)
Stretching, strengthening, low-impact aerobic training
medical and invasive
examples of a _______________ treatment approach for phantom and residual limb pain:
Medication and Injections (muscle relaxers and pain meds)
Neurostimulation (spinal cord stim, transcranial stim, deep brain)
Surgery- Remove neuroma or structure impinging a nerve
contractures
range of motion and strength prevents _____________
gait
there is a focus on certain muscle groups within general strengthening, muscles are selected based on their impact on ___________

hip flexion
knee flexion
what range of motion should you focus on to prevent contracture with a transtibial
hip flexion
hip abduction
hip lateral rotation
what range of motion should you focus on to prevent contracture with a transfemoral
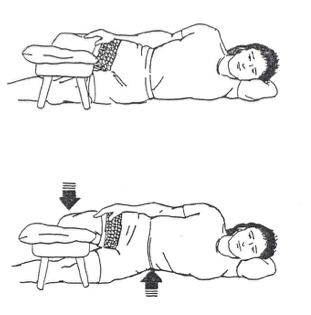
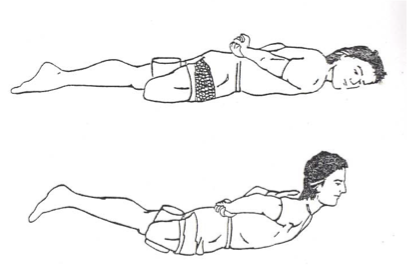
positioning in bed and wheelchair
stretching
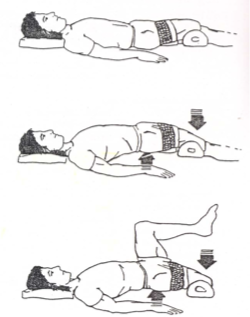
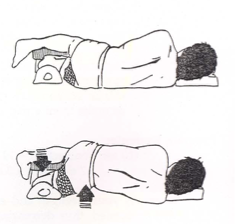
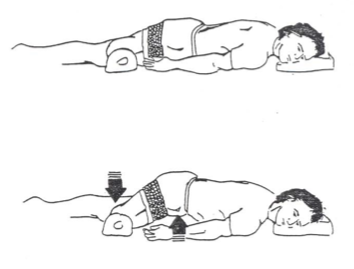
prone lying (as tolerated)
serial casting/bracing (in severe cases)
what are 4 contracture prevention techniques
spinal stabilization
core strength and control
hip strength and control
what are the 3 total body focuses for muscle strength training with an amputee
before the amputation (ideally/if possible)
when should strength training begin for an amputee
isometrics
what kind of strength training should you start with an amputee
6-10; 5-10; 6-10
the isometric strength training recommendations are _______ sec holds followed by ________ rest for ______ reps
muscles
glutes
hamstrings
gait phases
initial contact
loading response
terminal swing
with hip extension…
what muscles are activated?
what phases of gait include it?
an above knee amputation doesn’t have quads to prevent knee buckling
why is hip extension so important for an above knee amputation
muscles
glute med
glute minimus
gait phases
midstance
terminal stance
with hip abduction…
what muscles are activated?
what phases of gait include it?
muscles
iliopsoas
rectus femoris
gait phases
loading response
midstance
initial/mid/terminal swing
with hip flexion…
what muscles are activated?
what phases of gait include it?
muscles
hip ADD
gait phases
initial contact
mid/terminal swing
with hip adduction…
what muscles are activated?
what phases of gait include it?
muscles
lumbar extensors
glute max
hip ADD mm (if using roll)
gait phases
initial contact
loading response
mid/terminal swing
with trunk extension…
what muscles are activated?
what phases of gait include it?