7243 - Exam 2 w/ Kim (radio rebel)
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
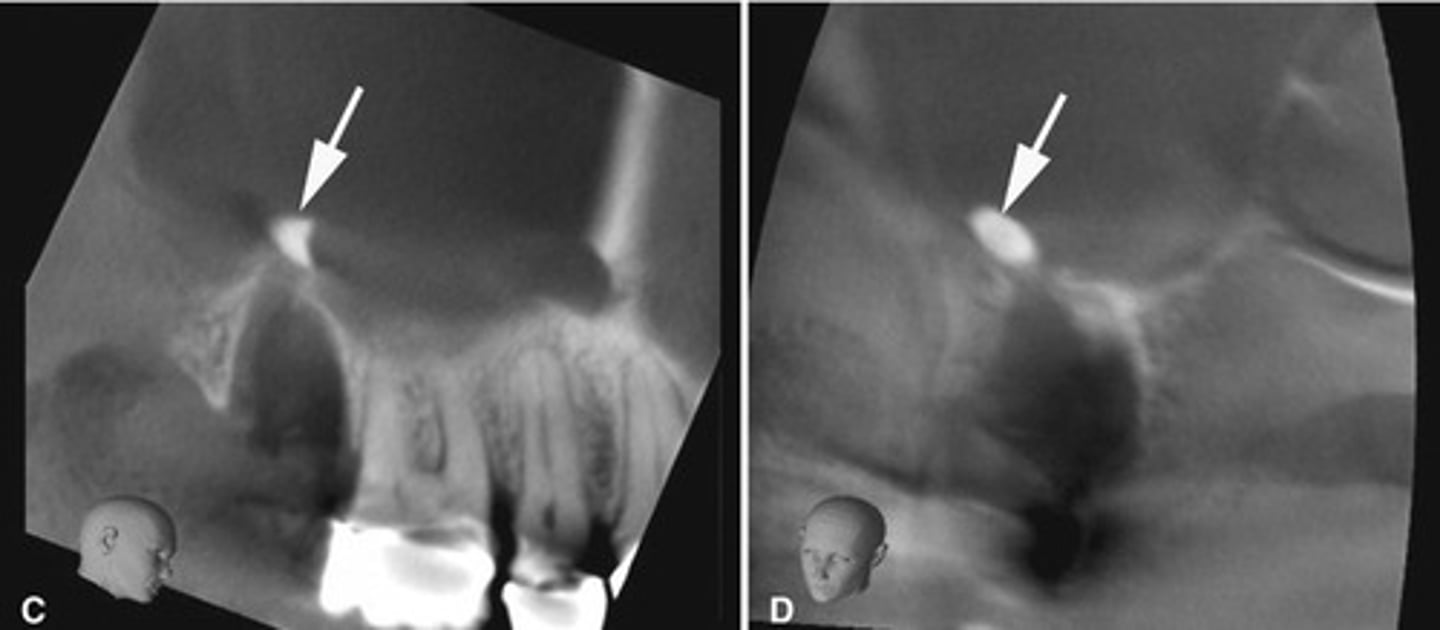
Root tip dislodged into the maxillary sinus.
You can see the PDL
How can you differentiate this from an antroliths in the maxillary sinus?
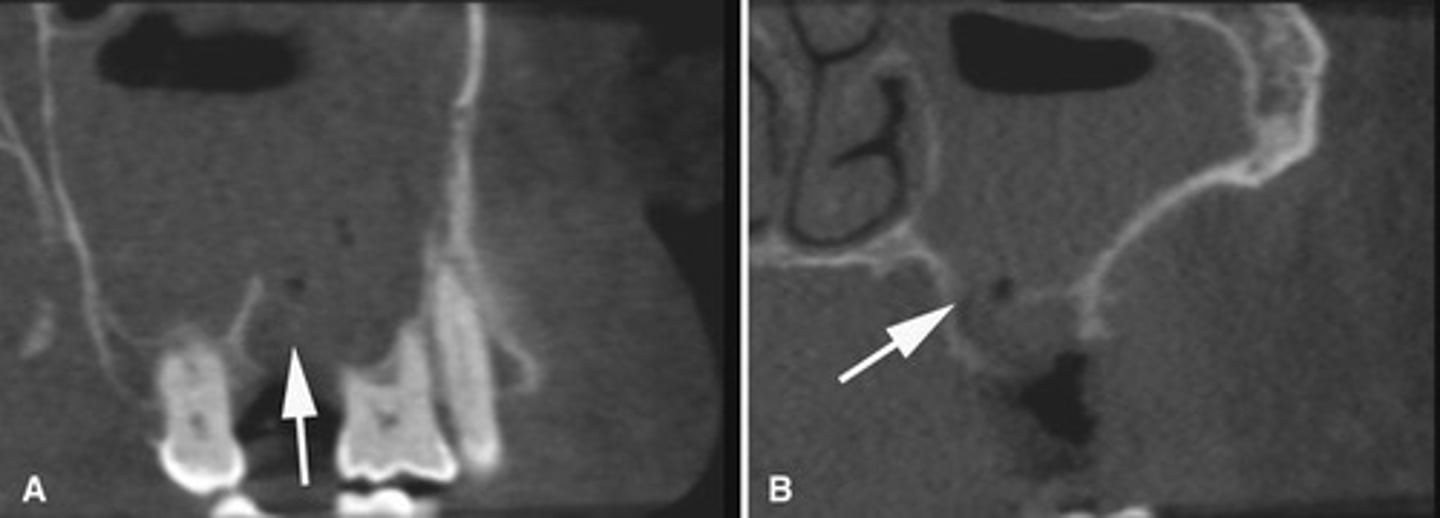
The radiograph depicts a sinus graft with irregular radiodensity, the discontinuity of the bone integration might impact implant treatment.
What does the radiograph show and how might it impact dental treatment?
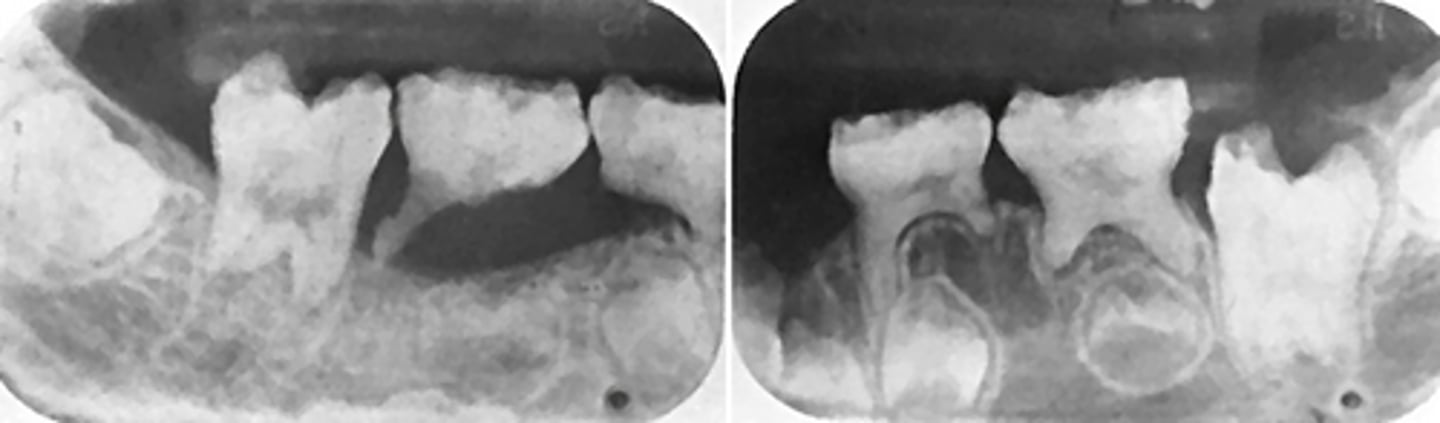
Root fragment dislodged into the maxillary sinus, this has implications for maxillary posterior extractions.
What does the image show?
Maxillary sinus perforation causing mucosal thickening.
What does this image show?
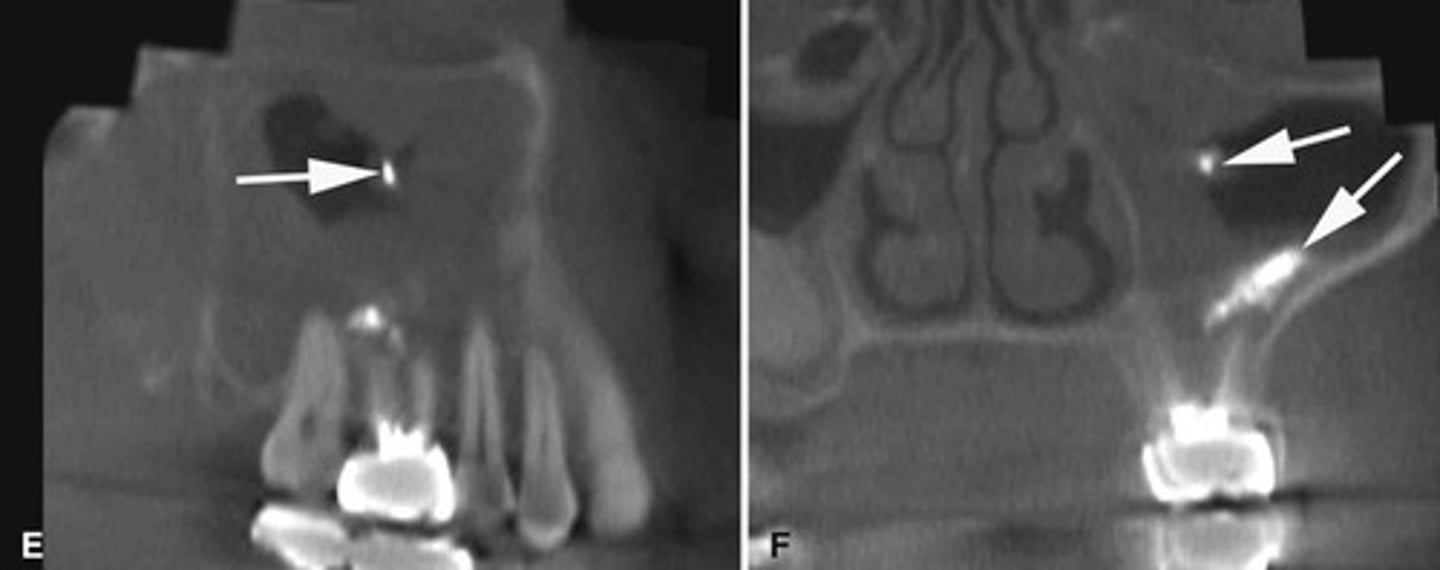
Endodontic materials into the maxillary sinus causing mucosal thickening.
What does the image show?
Completed around 20years; discontinuity of cortication for adults would indicate pathology (arthritic changes) , but in kids thin or no cortical border would be normal.
When is complete calcification of the cortical boarders of the condyle completed? What would be indicated by lack of cortication after that time?
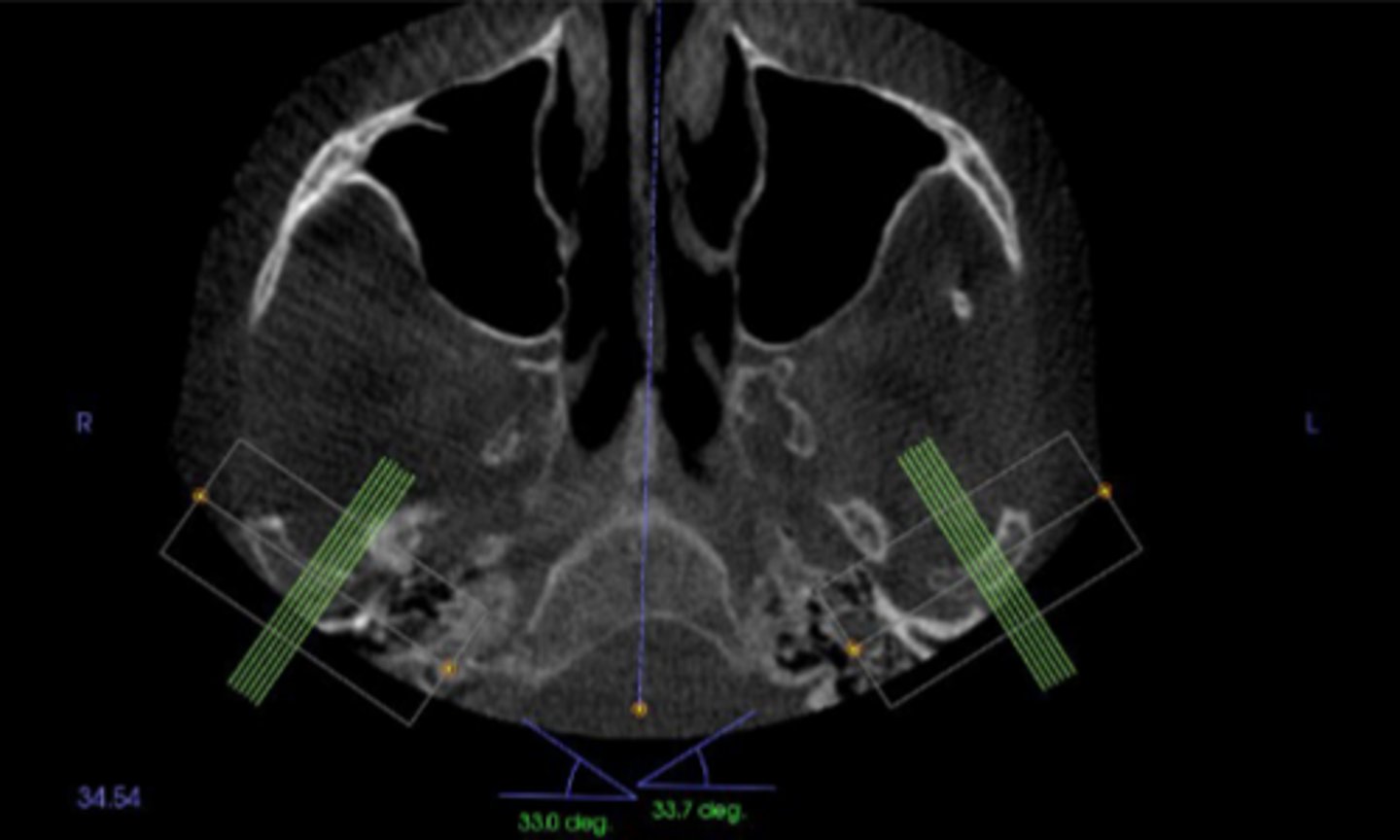
Posteriorly
The condylar neck is angled about 15-33° with a sagittal view so that the medial pole of the condyle is located ____________ to the lateral pole.
Age 4
The glenoid fossa and articular eminence mature by age___, but the cortices my still remain indistinct until adulthood.
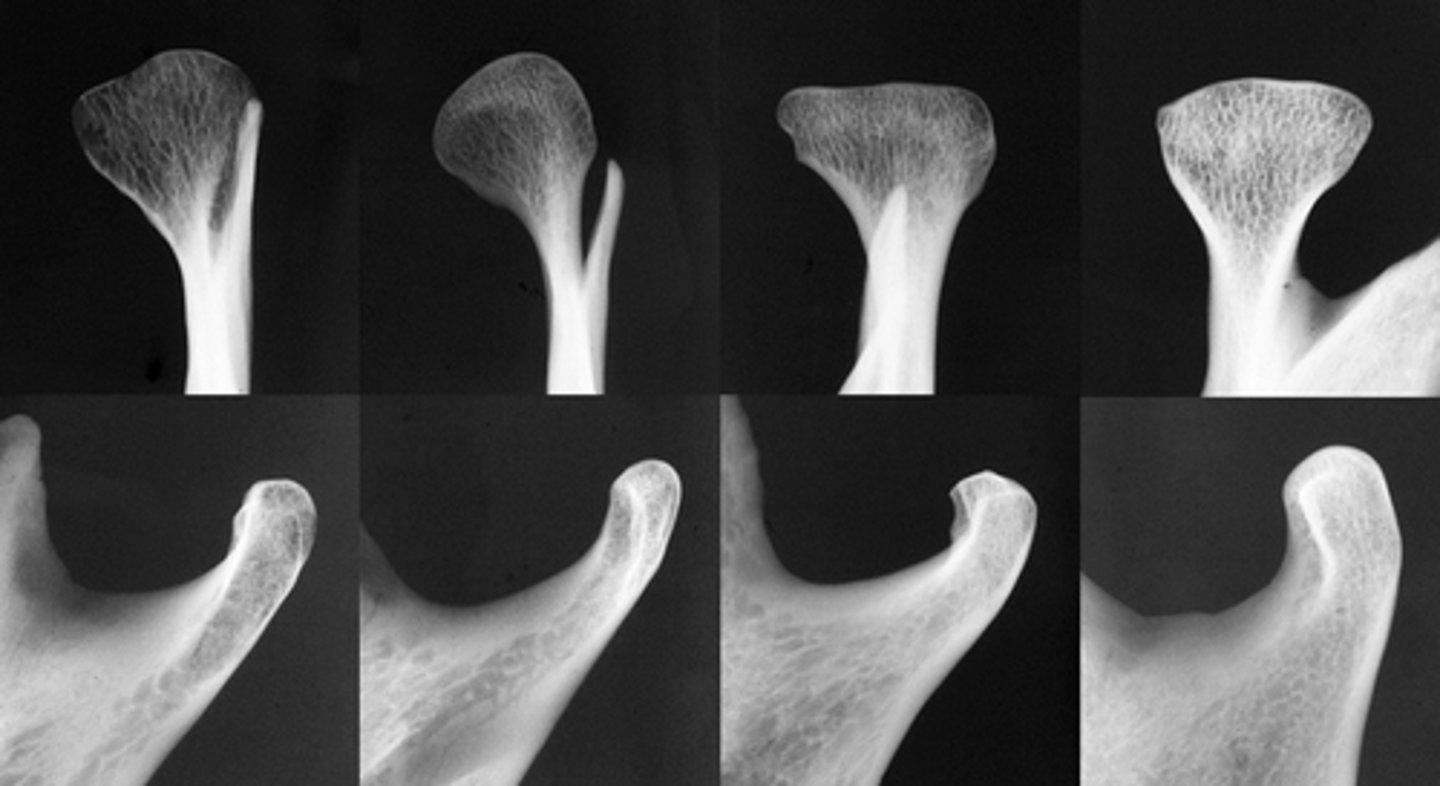
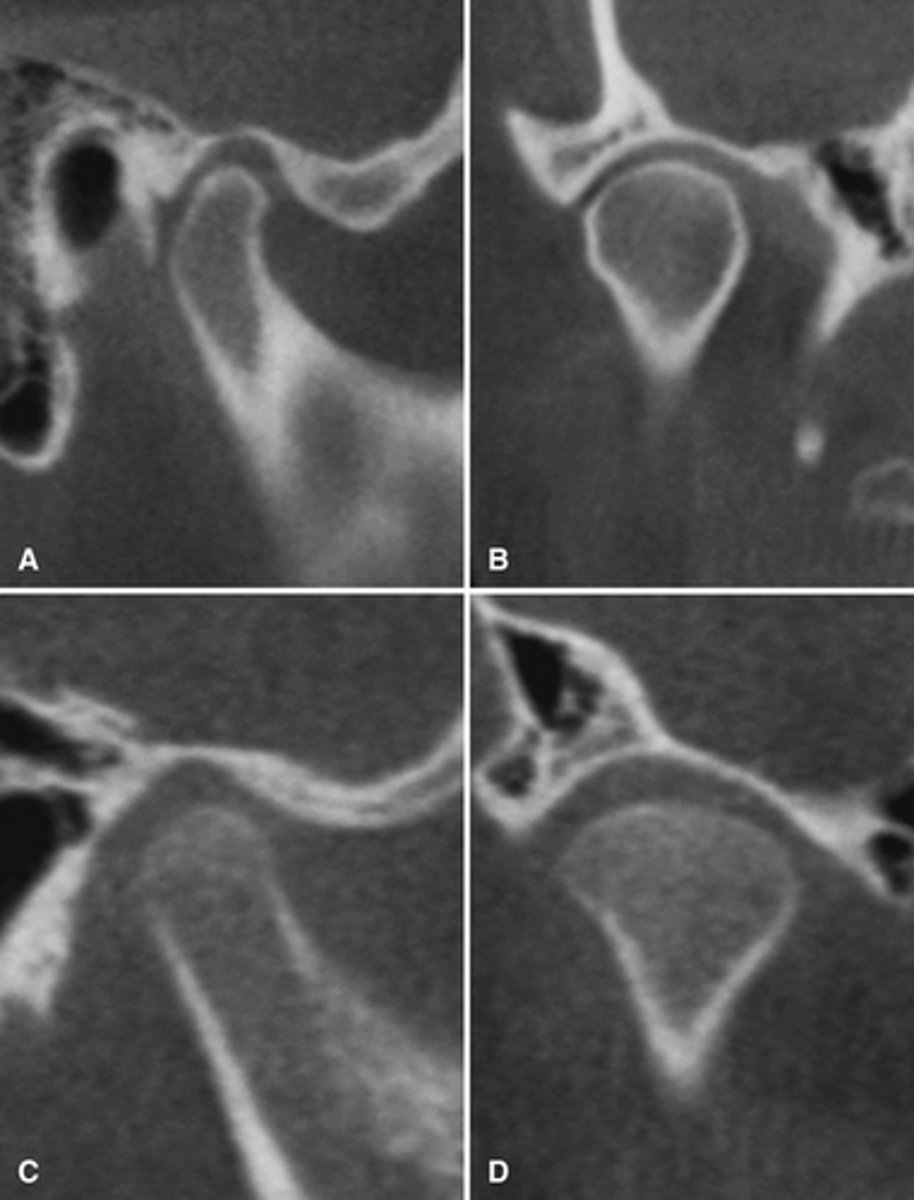
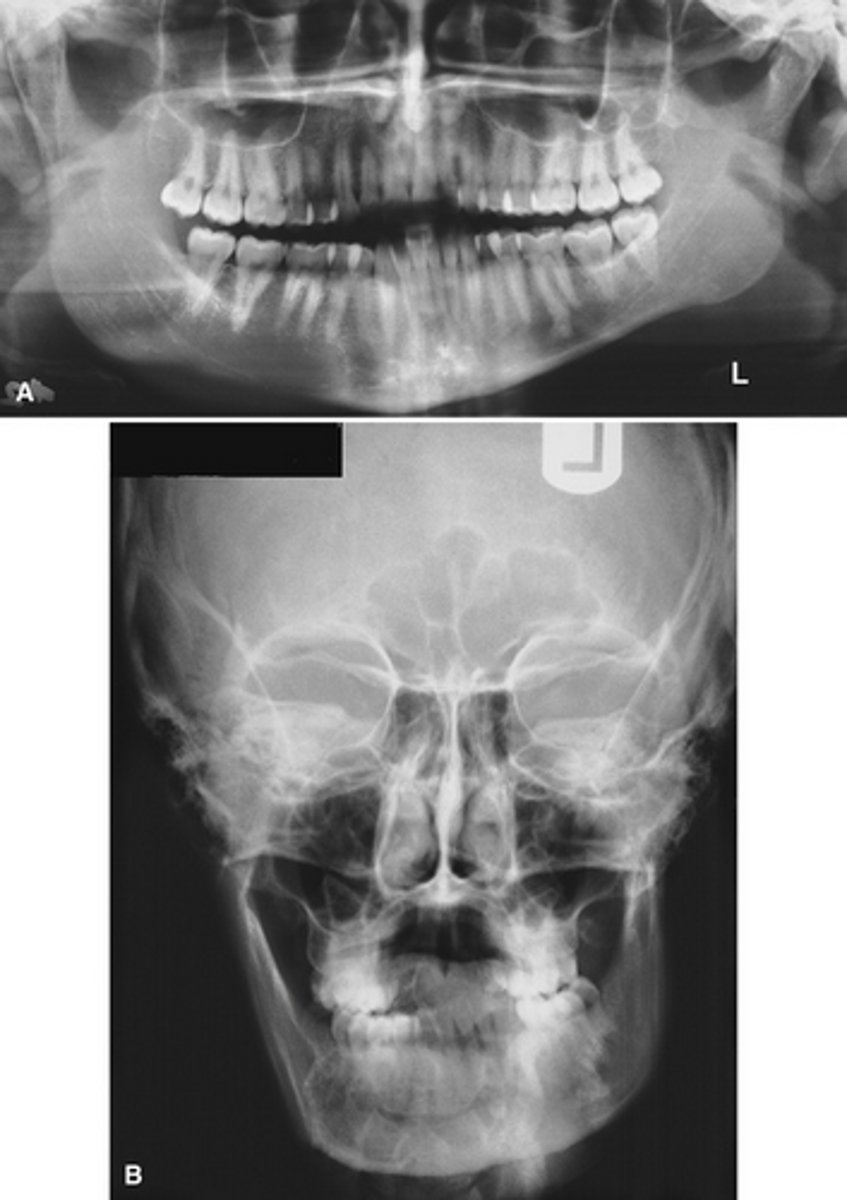
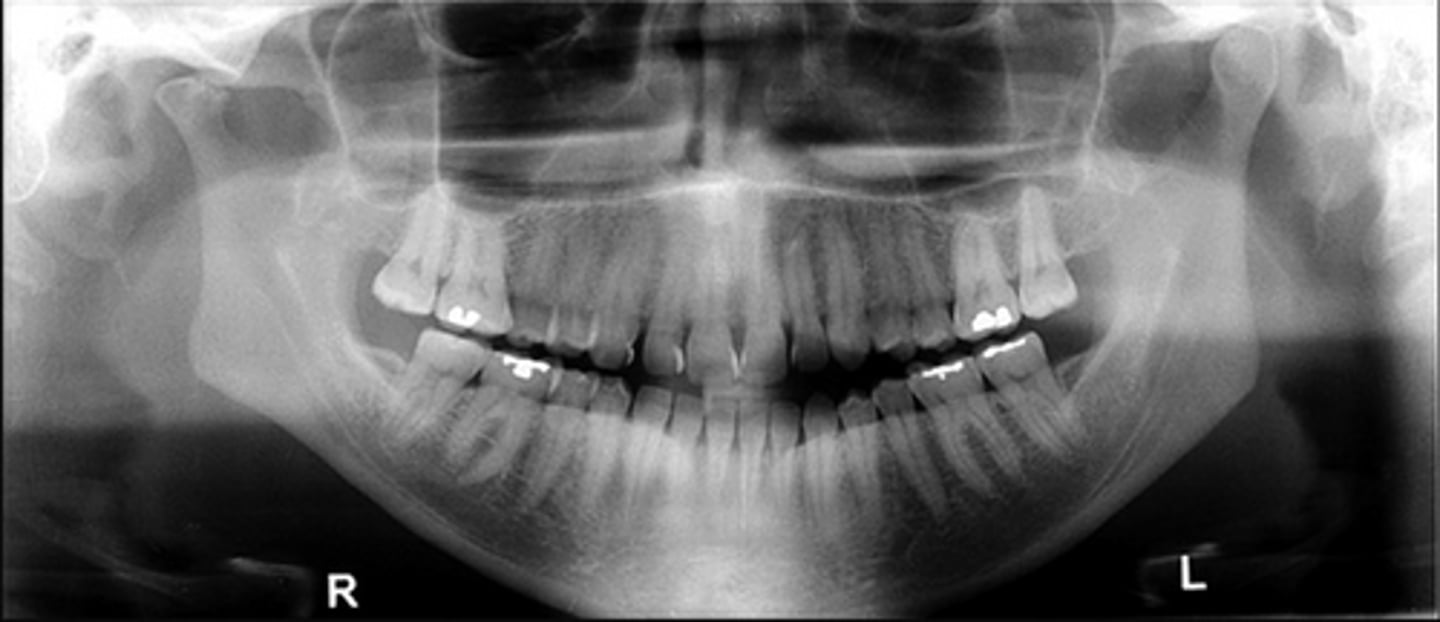
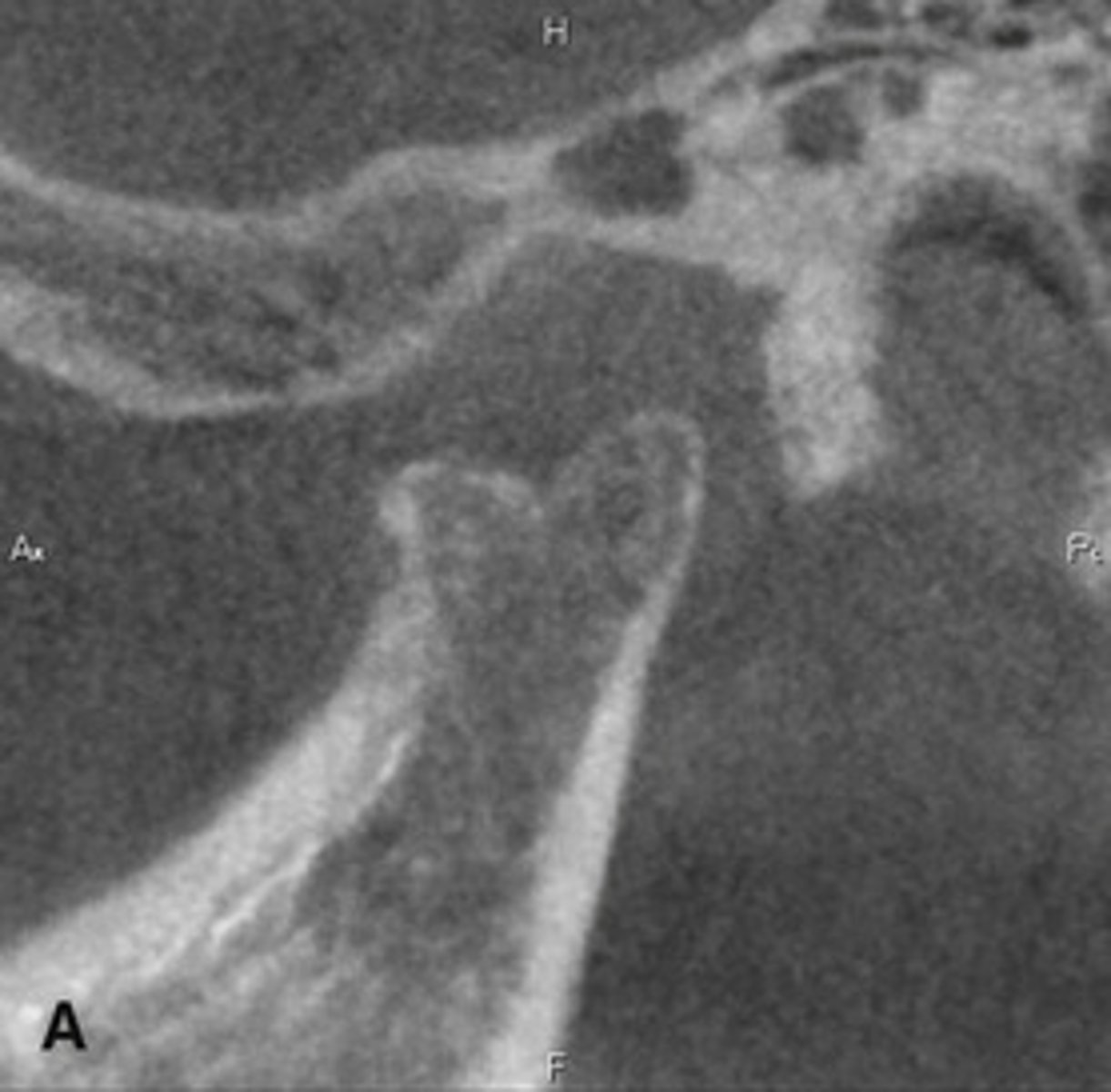
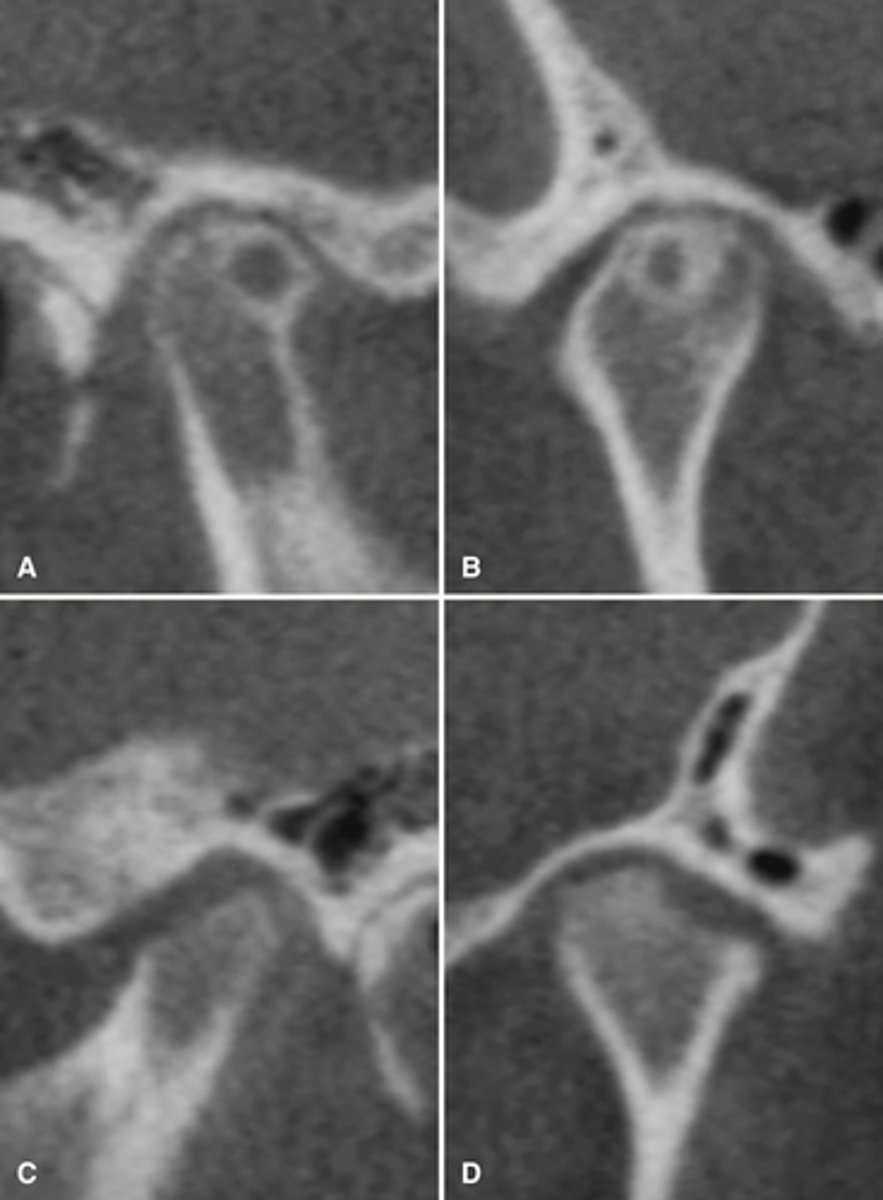
The bottom radiographs depict a developing 7year-old child.
1. The cortication of all the articulating surfaces are thin.
2. The mandibular fossa is shallow
3. The articular eminence is short
The top images are being compared to the bottom images, which patient is younger and what are all the ways to know this.
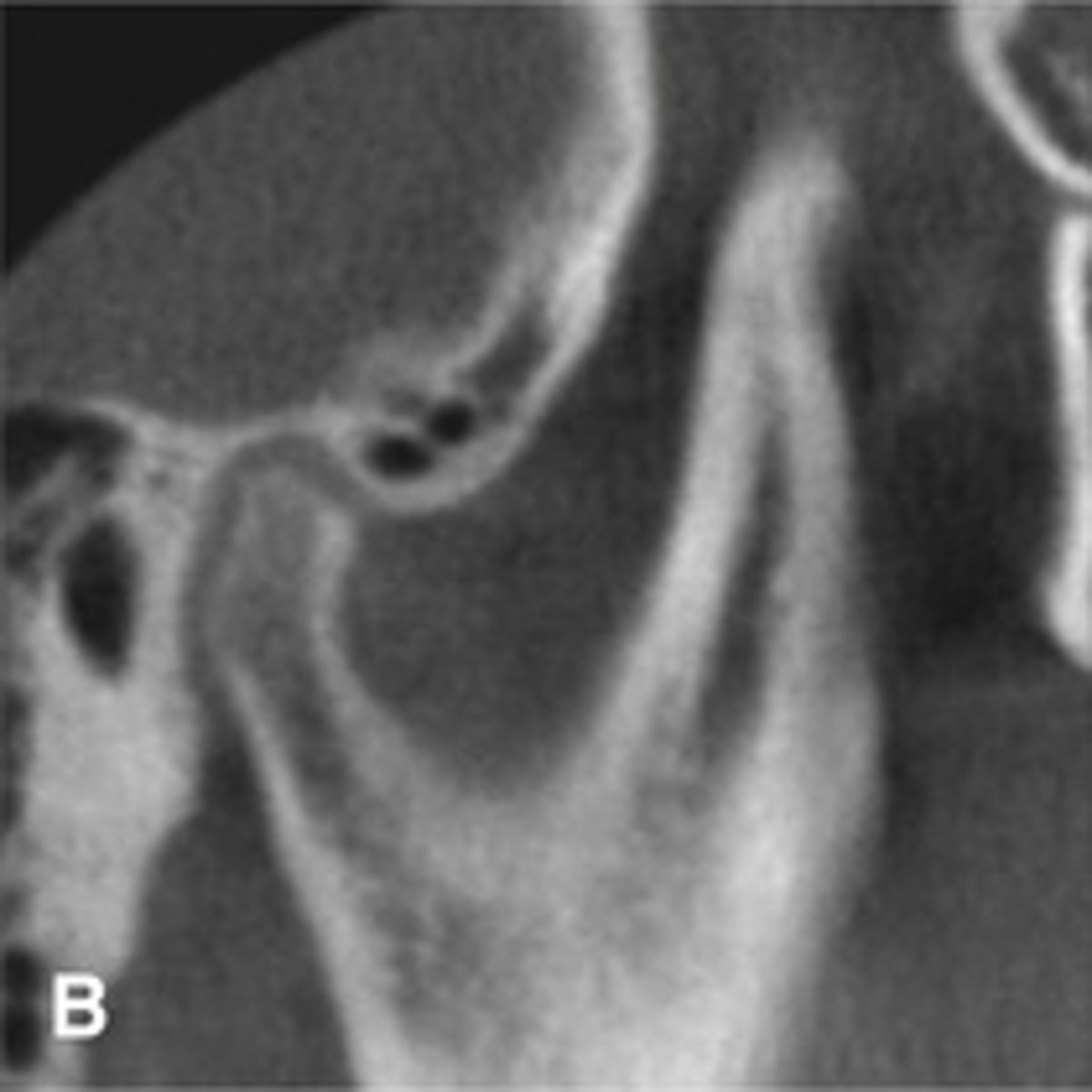
No, this is a normal variation of pneumatization of the mastoid air cells of the temporal bone into the articular eminence.
Is this pathological?

Pneumatization of the mastoid air cells of the temporal bone into the articular eminence.
Radiograph shows?

The correct ones are
B and D only.
A. Composed of AVASCULAR fibrous CT
C. Divides the joint cavity into SUPERIOR and INFERIOR joint spaces
E. The POSTERIOR band attaches to the retrodiscal tissue
F. The anterior band attaches to the SUPERIOR head of the lateral pterygoid muscle.
Which of these is correct? (select all that apply) The interarticular disc is:
A. Composed of vascular fibrous CT
B. Thicker medially than laterally
C. Divides the joint cavity into medial and lateral joint spaces
D. Demonstrates a biconcave shape
E. The anterior band attaches to the retrodiscal tissue
F. The anterior band attaches to the inferior head of the lateral pterygoid muscle.
c. Both statements are true
Although it is abnormal for the condyle to be uncentered about 1/3-1/2 of patients are asymptomatic. However, a markedly eccentric condylar position usually represents abnormality and should be noted.
a. The first statement is true and the second is false.
b. The first statement is false and the second is true.
c. Both statements are true
d. Both statements are false
1. b
2. a
3. d
4. c
(1)Posterior condylar positions may suggest anterior disc displacement.(2)Anterior condylar position may suggest destruction of the articular eminence, such as juvenile idiopathic arthritis. (3) Inferior condylar position may suggest fluid accumulation within the joint. (4) Superior condylar position may suggest loss, displacement, or perforation of the disc or attachments.
Match the abnormal eccentric position with the suggested pathology.
1. Posterior condylar positions may suggest
2. Anterior condylar position may suggest
3. Inferior condylar position may suggest
4. Superior condylar position may suggest
a. Destruction of the articular eminence, such as juvenile idiopathic arthritis
b. Anterior disc displacement
c. loss, displacement, or perforation of the disc or attachments.
d. Fluid or blood accumulation within the joint
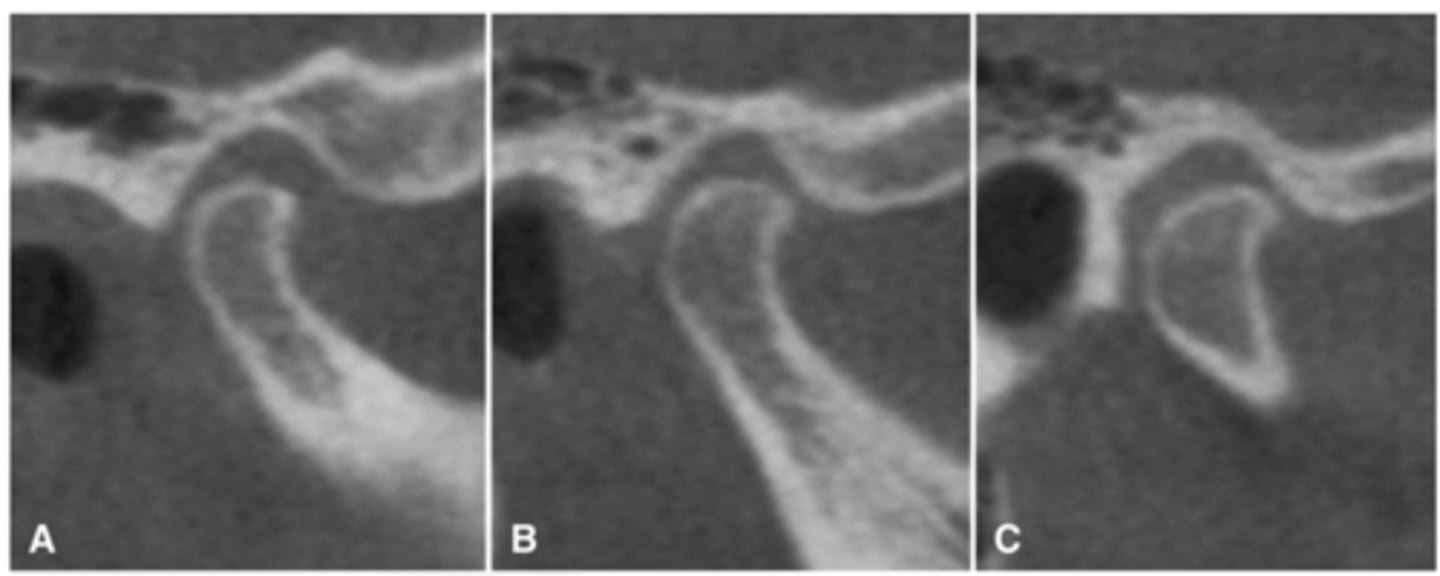
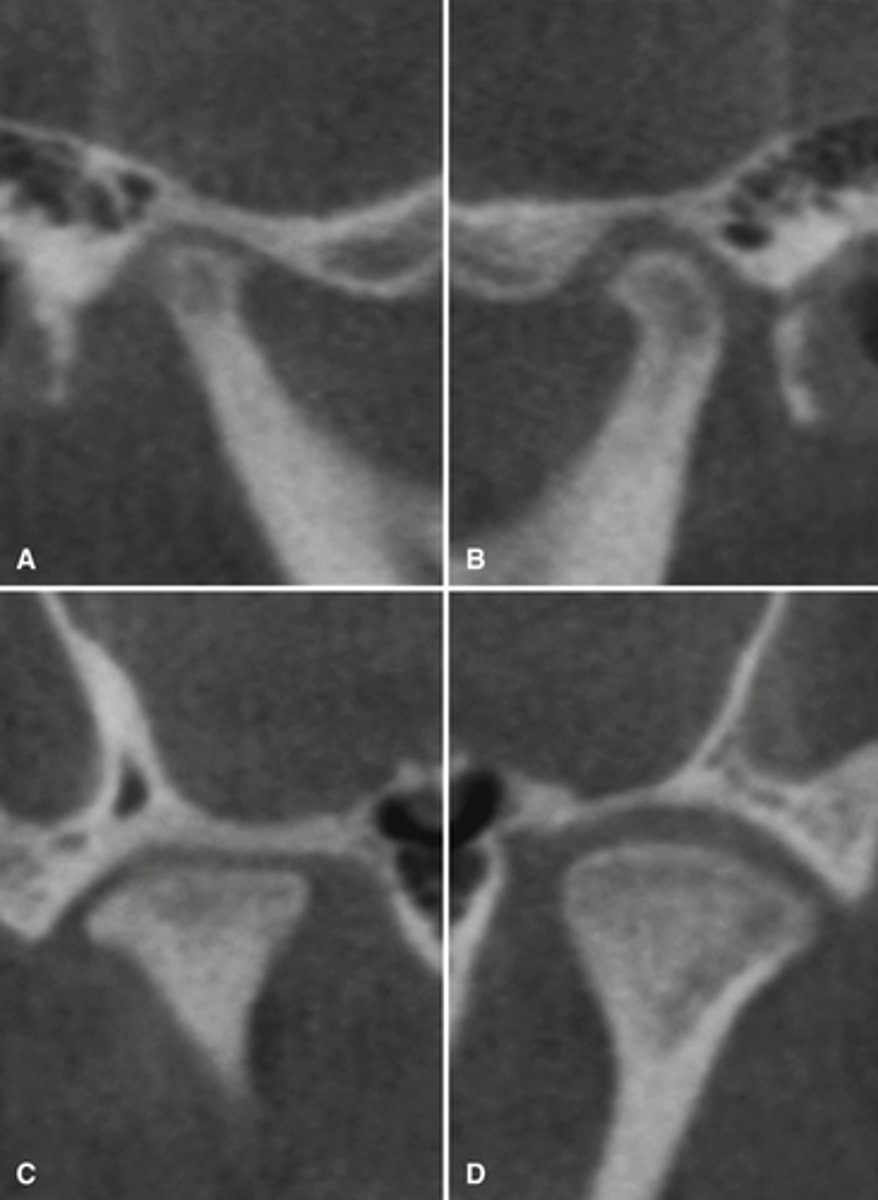
The images are showing the condyle from lateral to medial, and although A looks to be posteriorly positioned both B and C look centered, so it is likely centered.
Joint positions can vary from lateral to medial pole as seen in the radiograph so to determine if the condyle is eccentrically located or centered just see where the condyle is sitting most of the time. Would the example be eccentrically located or centered?
The condyle at the crest of the articular eminence with a normal degree of translation in maximum opening. (Max opening = condyle at the crest or just anterior)
What does the radiograph depict?
Hypermobility
A patient is at maximum opening and the condyle is 6mm anterior to the crest of the articular eminence; what is indicated?
Limited degree of opening
A patient is at maximum opening and the condyle is posterior to the crest of the articular eminence; what is indicated?
hypermobility and anterior locking or dislocation
A patient is at maximum opening and the condyle is anterior and slightly superior to the crest of the articular eminence; what is indicated?
Right condylar hyperplasia
Right condyle shows?
Destruction of condyle by malignant tumor
Images shows?
Soft tissue structures and discs.
Pano is okay for detecting general and extensive TMJ abnormalities. CBCT allow us to view more subtle TMJ features except for what?
MRI would be the choice because it is the only one that allows for visualizing the disc, however osseous changes are not as well detailed, and some dental materials create artifacts.
If you wanted to view the soft tissues and disc of the TMJ what imaging modality is the choice?
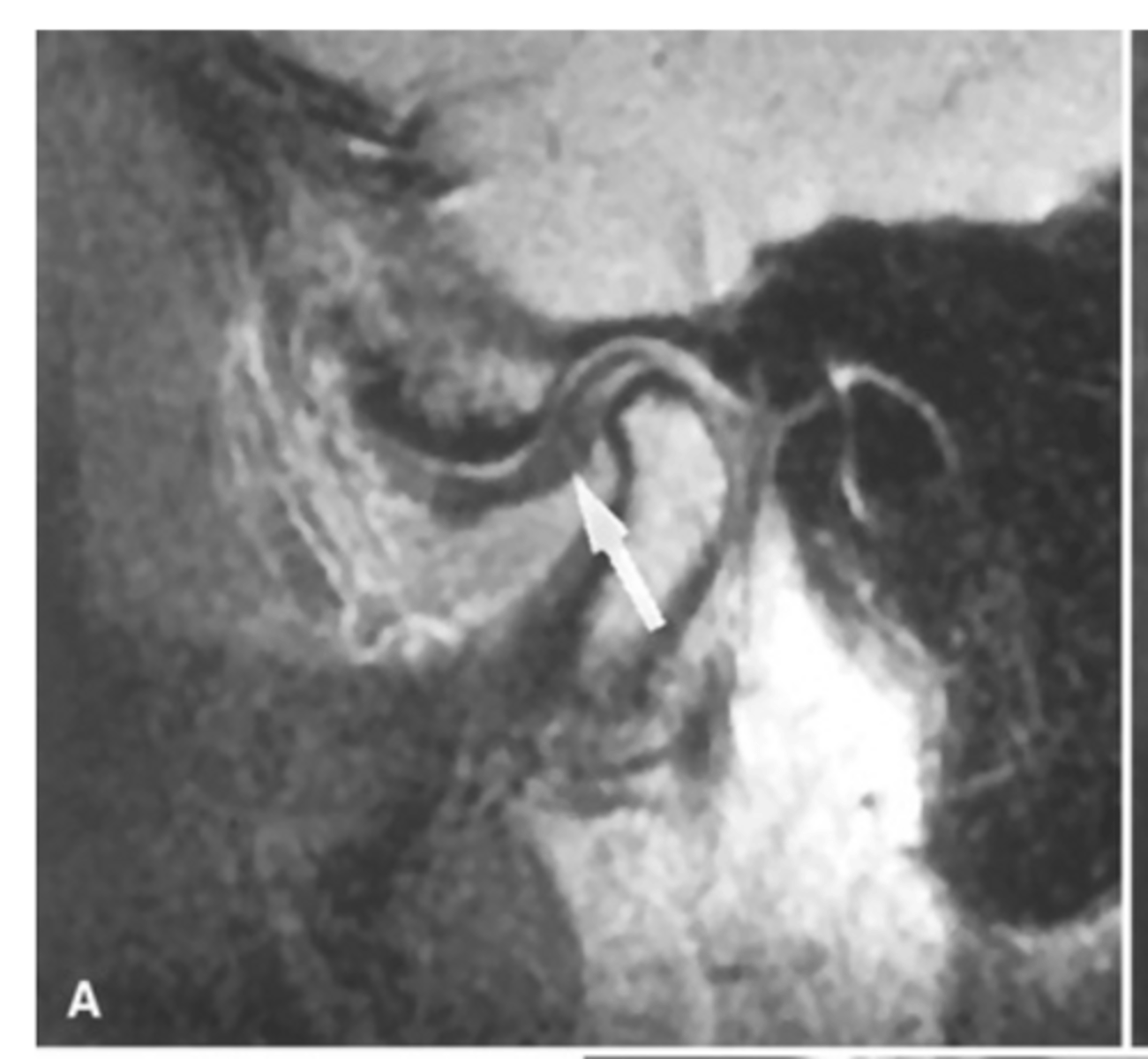
MRI image of the TMJ allowing for visualization of the condylar disc.
What is the image showing?
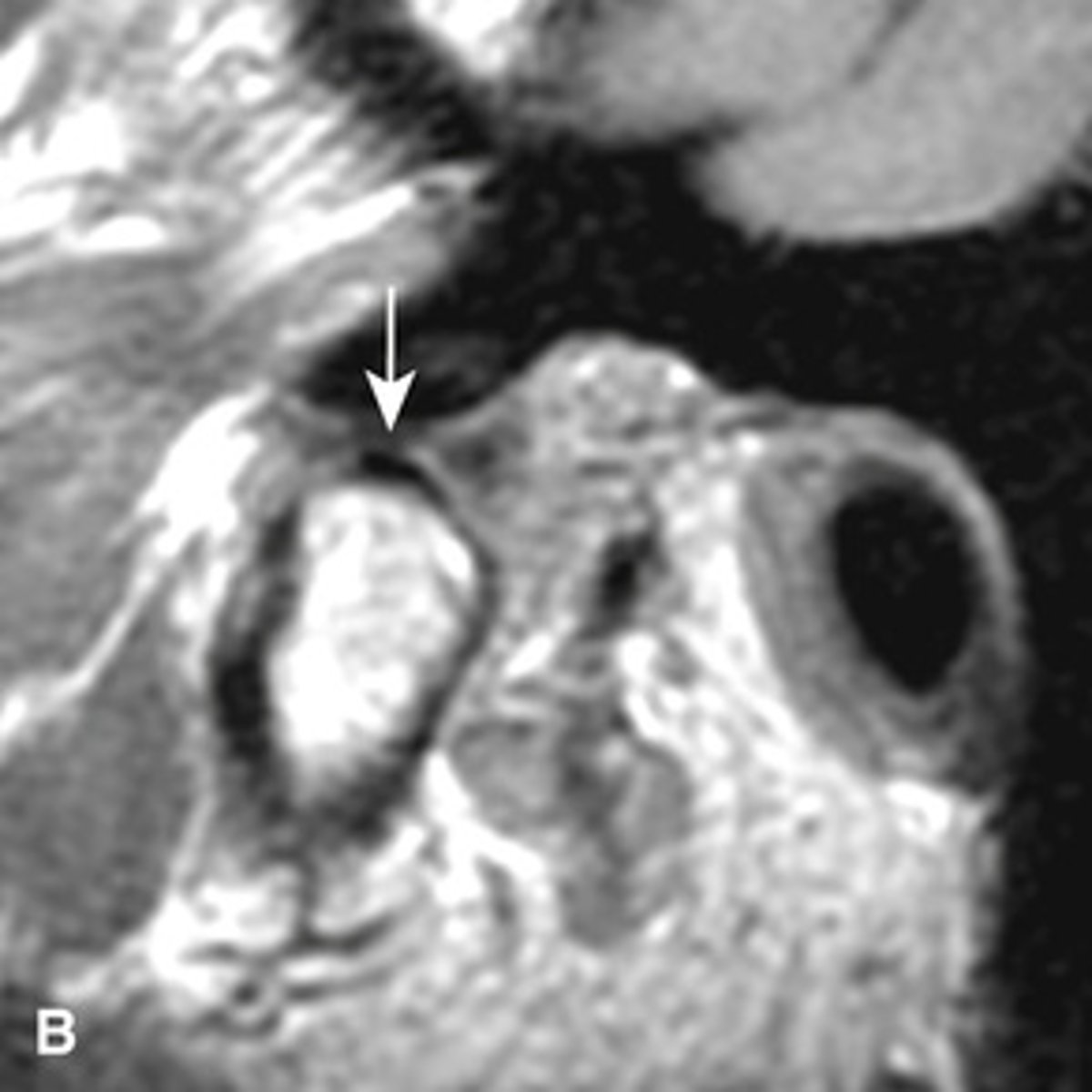
anteriorly displaced (the posterior band is anterior to the condyle)
The MRI is showing the disc ________ ______
laterally displaced (the joint capsule is bulging out laterally)
The MRI is showing the disc ________ ______

Condylar hyperplasia;
- condylar head is shaped normal just enlarged
- usually unilateral and maybe accompanied by hyperplasia of the ipsilateral mandible
- more common in females
- self-limiting
- increased vertical dimension
- deviated or limited opening
- posterior open bite or crossbite.
What is this developmental abnormality, and what is the etiology for it?
Condylar Hypoplasia
- Condylar head is normal shaped just undersized with proportional glenoid fossa
- condylar neck is thinner and may look short or long
- Decreased vertical diminution
- Usually unilateral and maybe hypoplasia of the mandible
- Deviated midline
- Might have TMJ dysfunction
What is this developmental abnormality, and what is the etiology for it?
Condylar Hypoplasia
What is this developmental abnormality?
Coronoid hyperplasia
- Elongation of the coronoid process where the tip extends 1cm above the inferior rim of the zygomatic arch
- Usually bilateral
- The condyle can hit the posterior of the maxilla or the zygomatic bone during opening and restrict condylar translation.
What is this developmental abnormality, and what is the etiology for it?

Coronoid hyperplasia
What is this developmental abnormality?
Bifid condyle
- Vertical depression in the condylar head
- often unilateral but may be bilateral
- may be a result of trauma
- some patients may have TMJ dysfunction
- Treatment isn't indicated unless pain or fxn impairment.
What is this developmental abnormality, and what is the etiology for it?
Remodeling; is considered normal unless accompanied by signs or symptoms of dysfunction.
The adaptive response to cartilage and bone loading forces that causes flattening, thickening, and subchondral sclerosis is __________. Is it pathological or normal?
DJD ( degenerative joint disease) aka osteoarthritis
________ occurs when the ability of the joint to adapt to excessive loading via remodeling is exceeded.
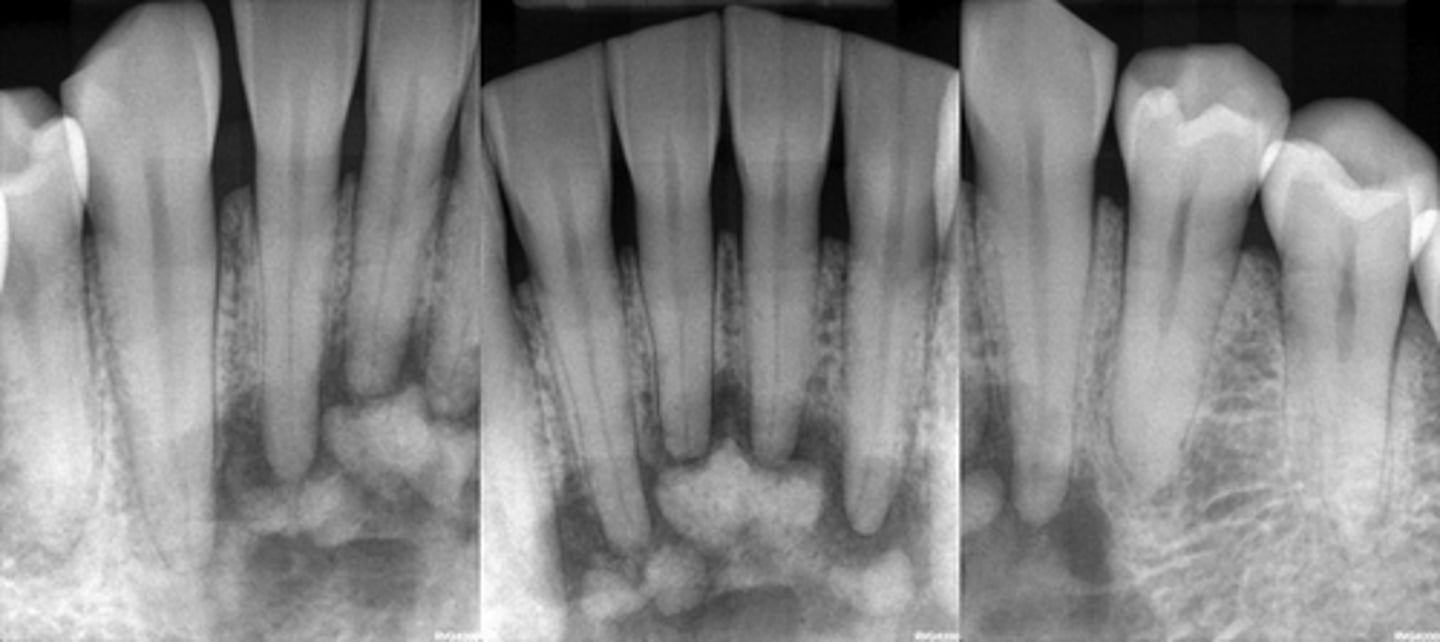
Patient has DJD.
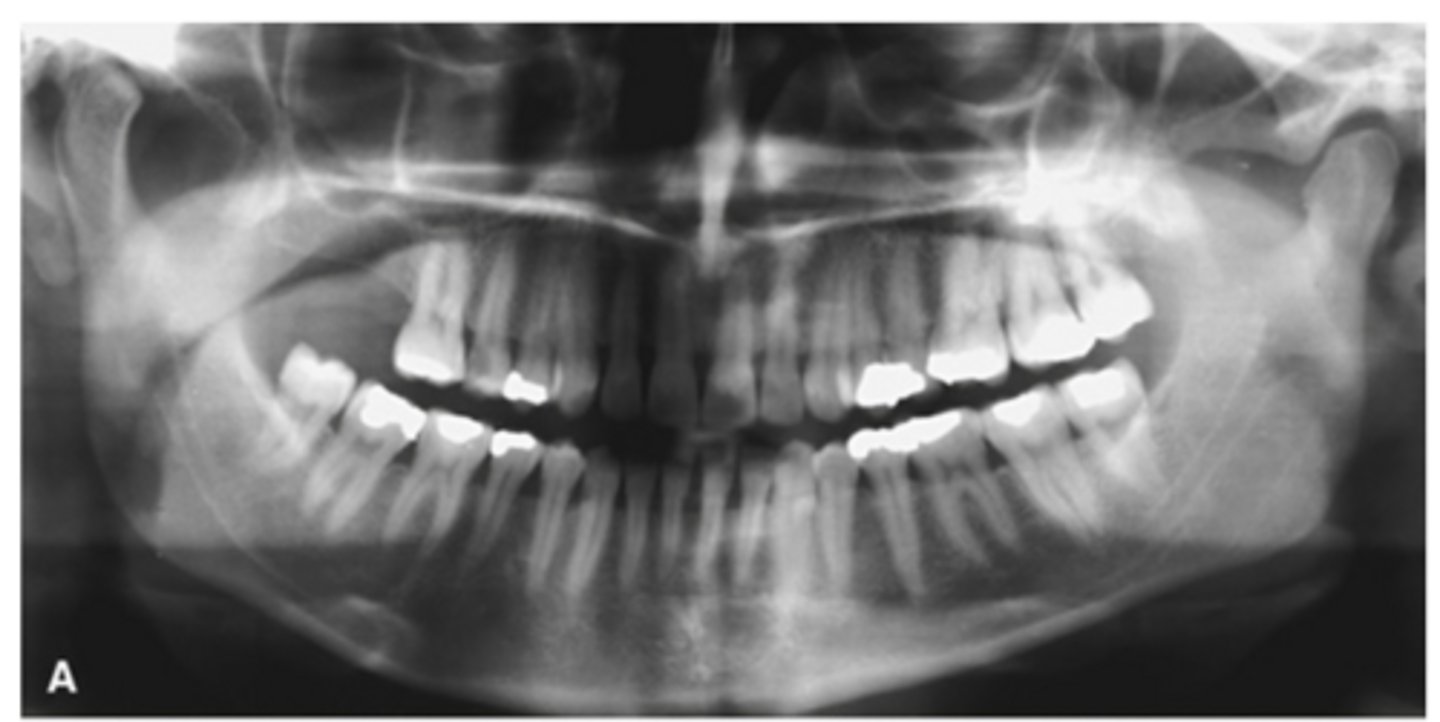
The top images show the subchondral/ Ely cyst, a pseudocyst of connective tissue, granular tissue and osteoid, the bottom images show the same patients left side with broad erosion, a lack of cortication, loss of joint space.
What is the diagnosis of the patient based off these radiographs and what are the features? (Top images = patients right condyle) (bottom images= same patients left condyle)
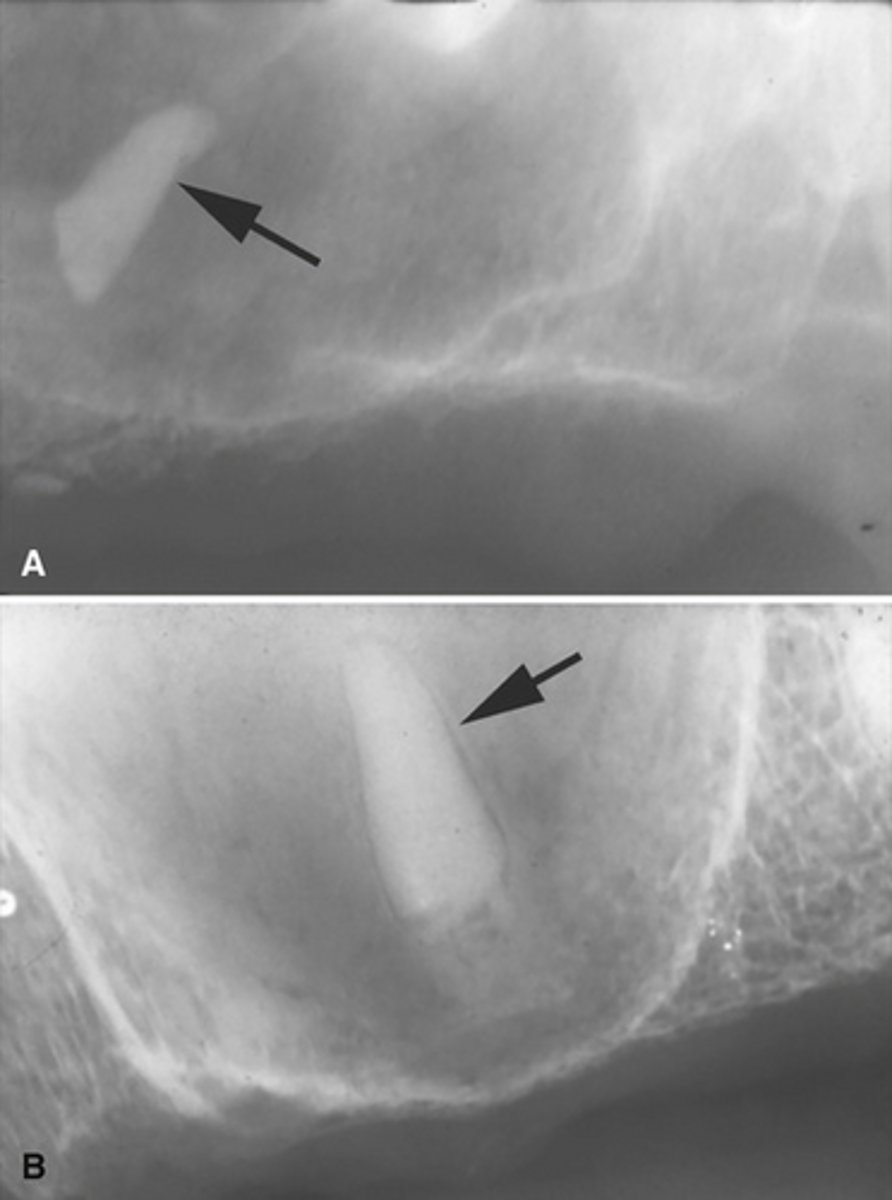
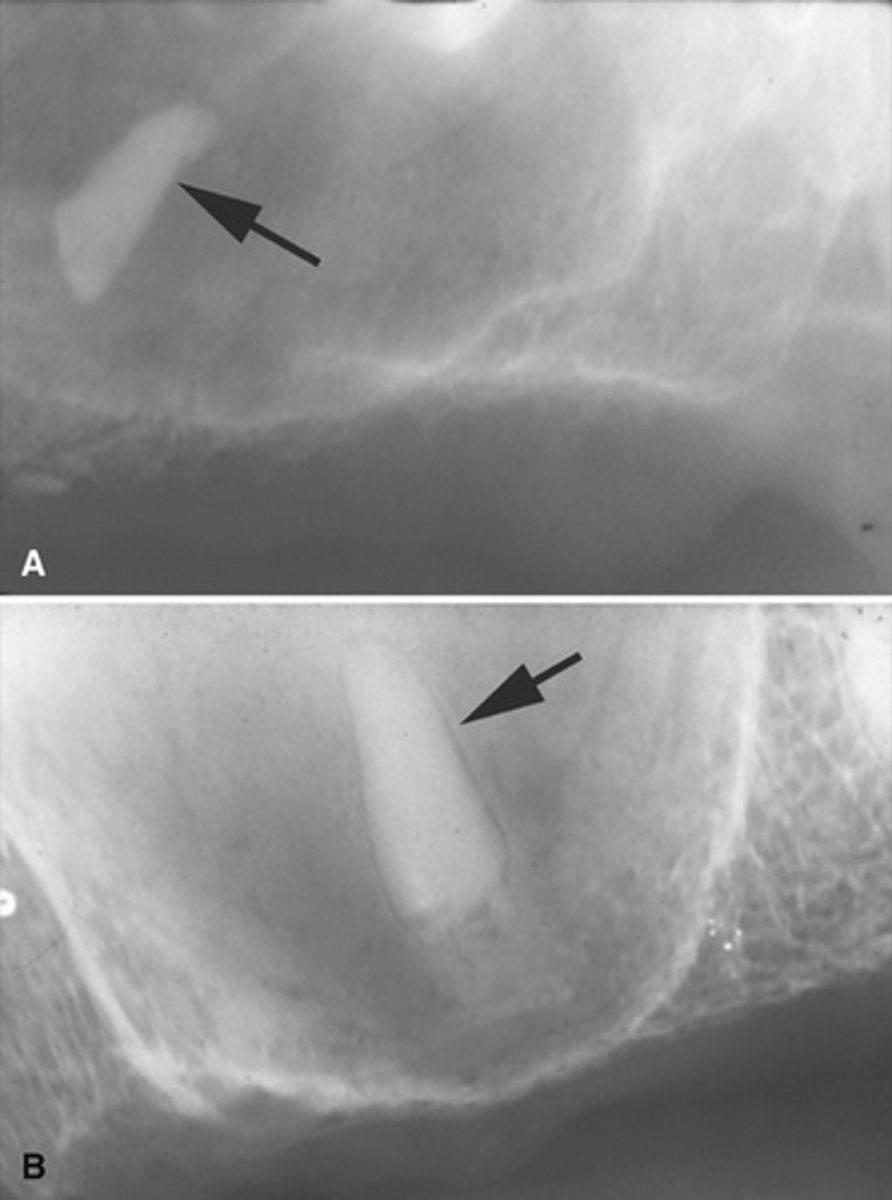
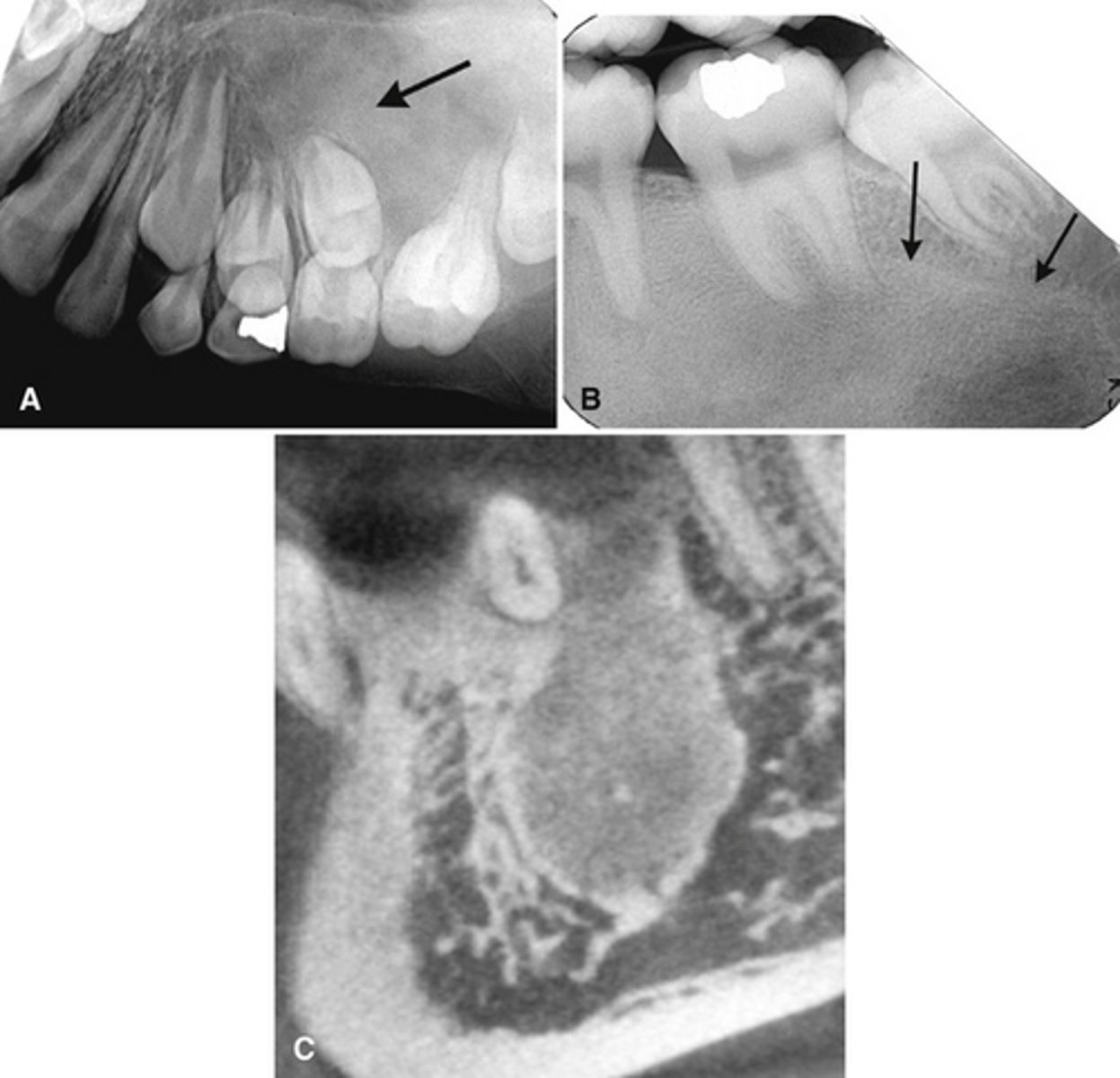
Osteophytes- joint mice associated with DJD
What are the arrows showing?

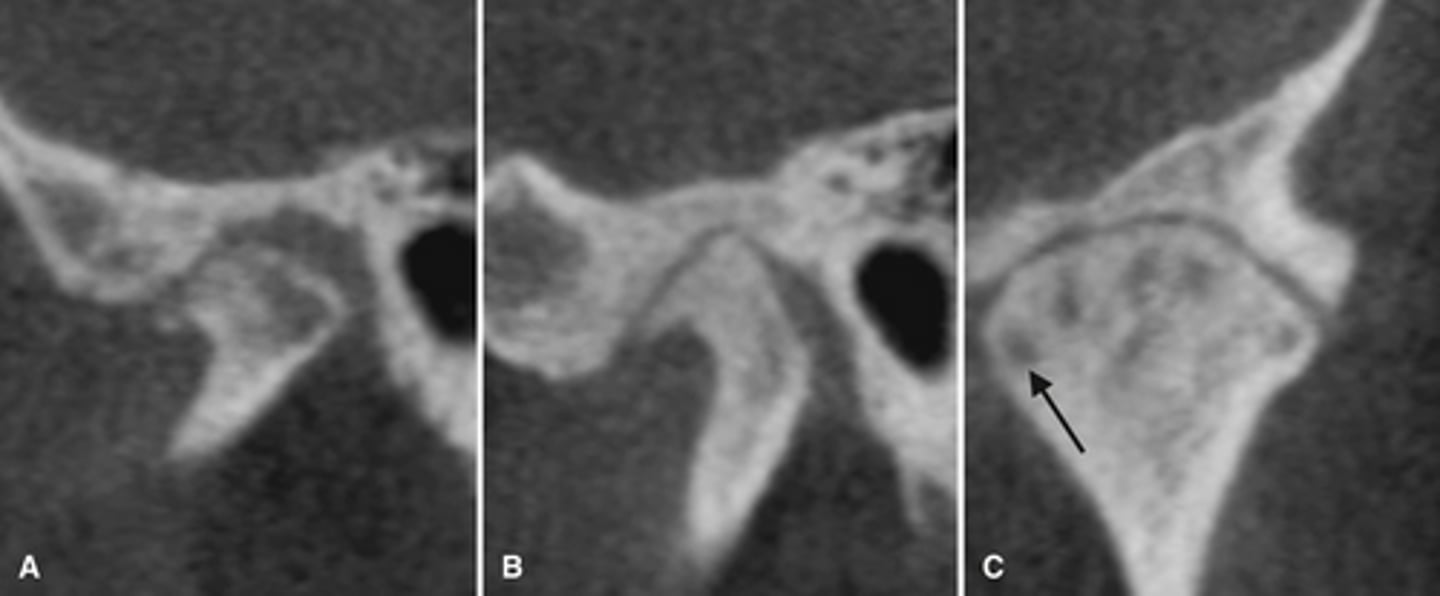
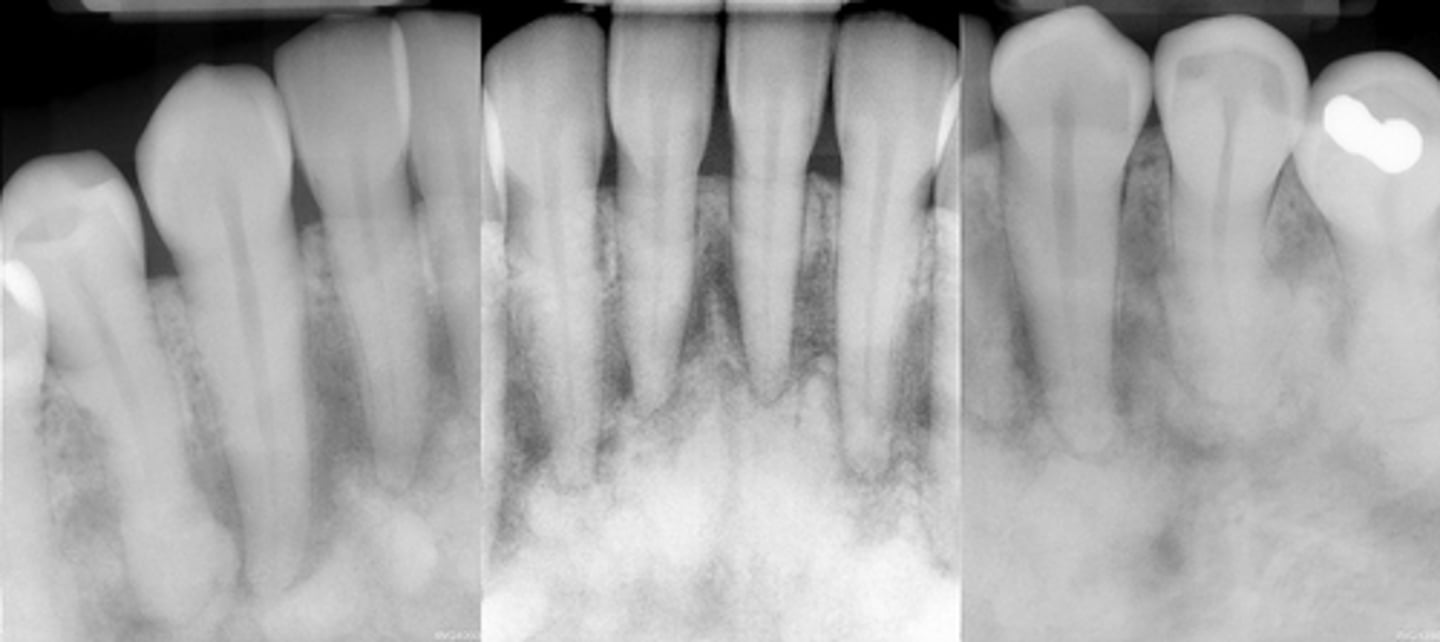
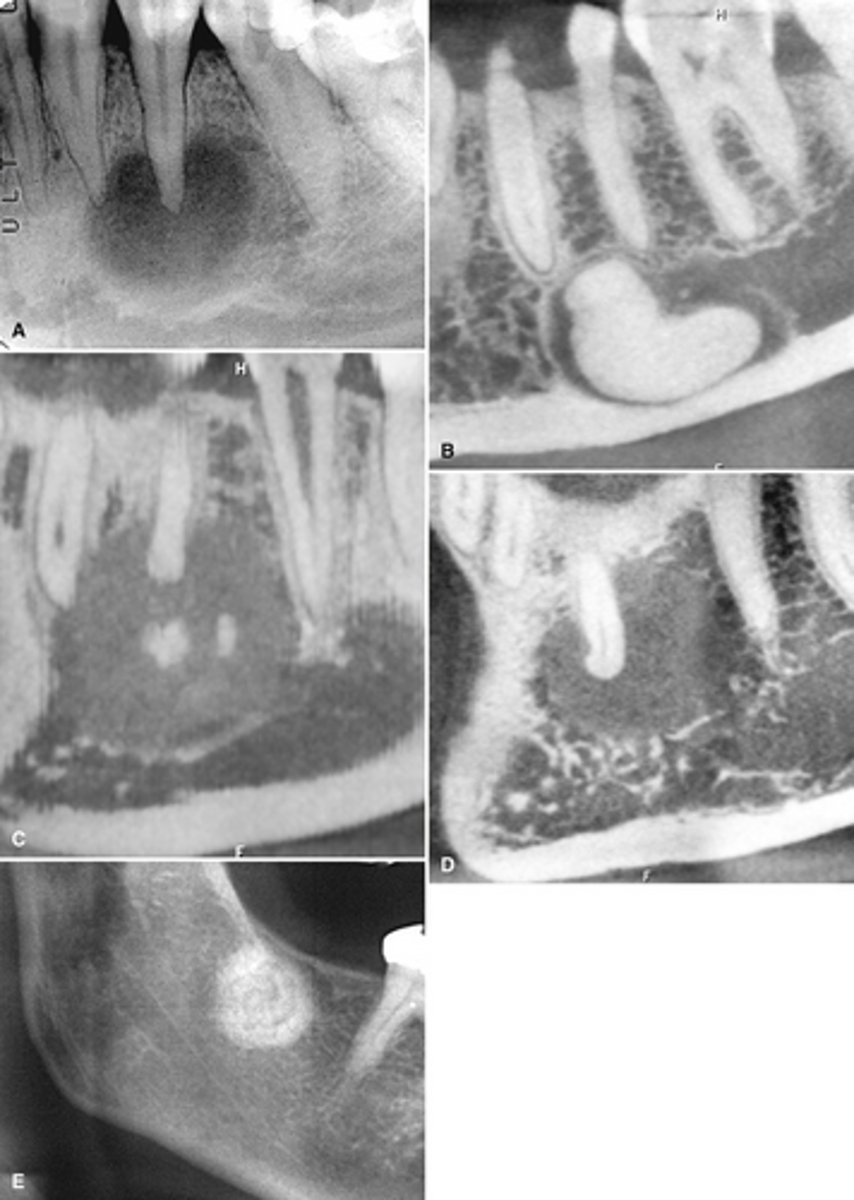
Patient has DJD, there is significant erosion and loss of joint space.
A and B show prominent osteophyte formation at the anterior aspect
C shows multiple subchondral erosions
What is the diagnosis of the patient based off these radiographs and what are the features?
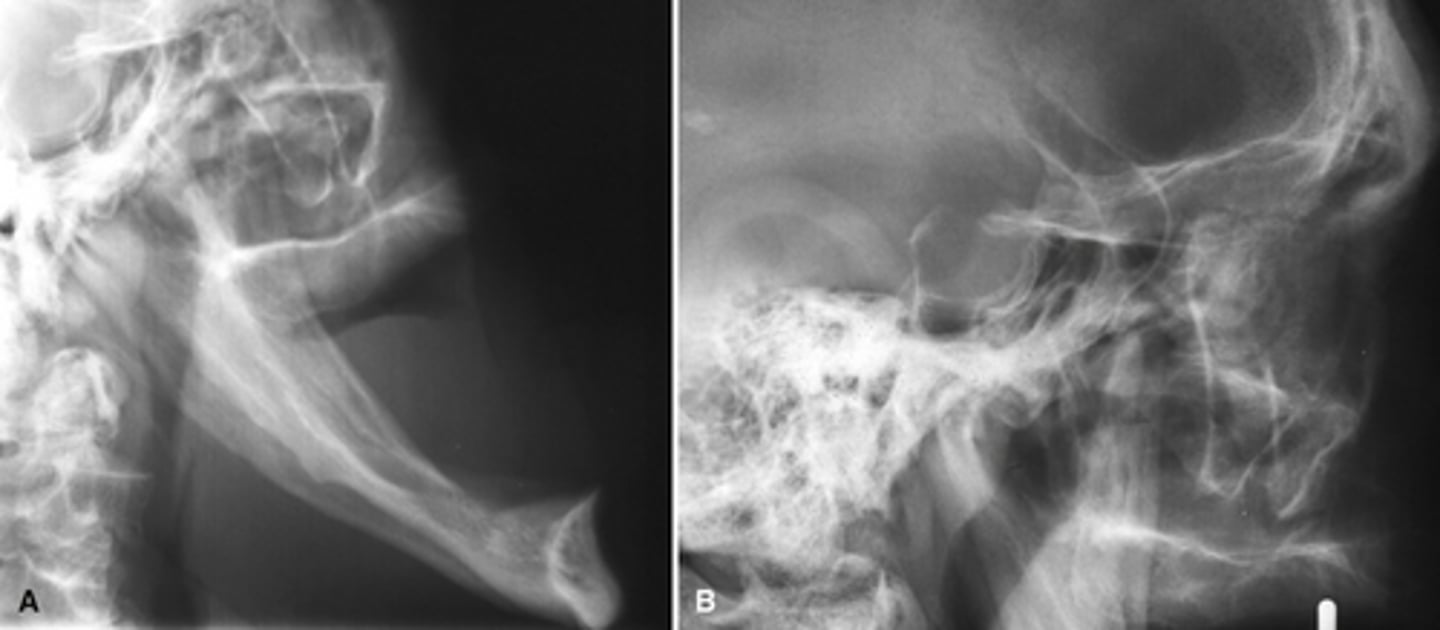
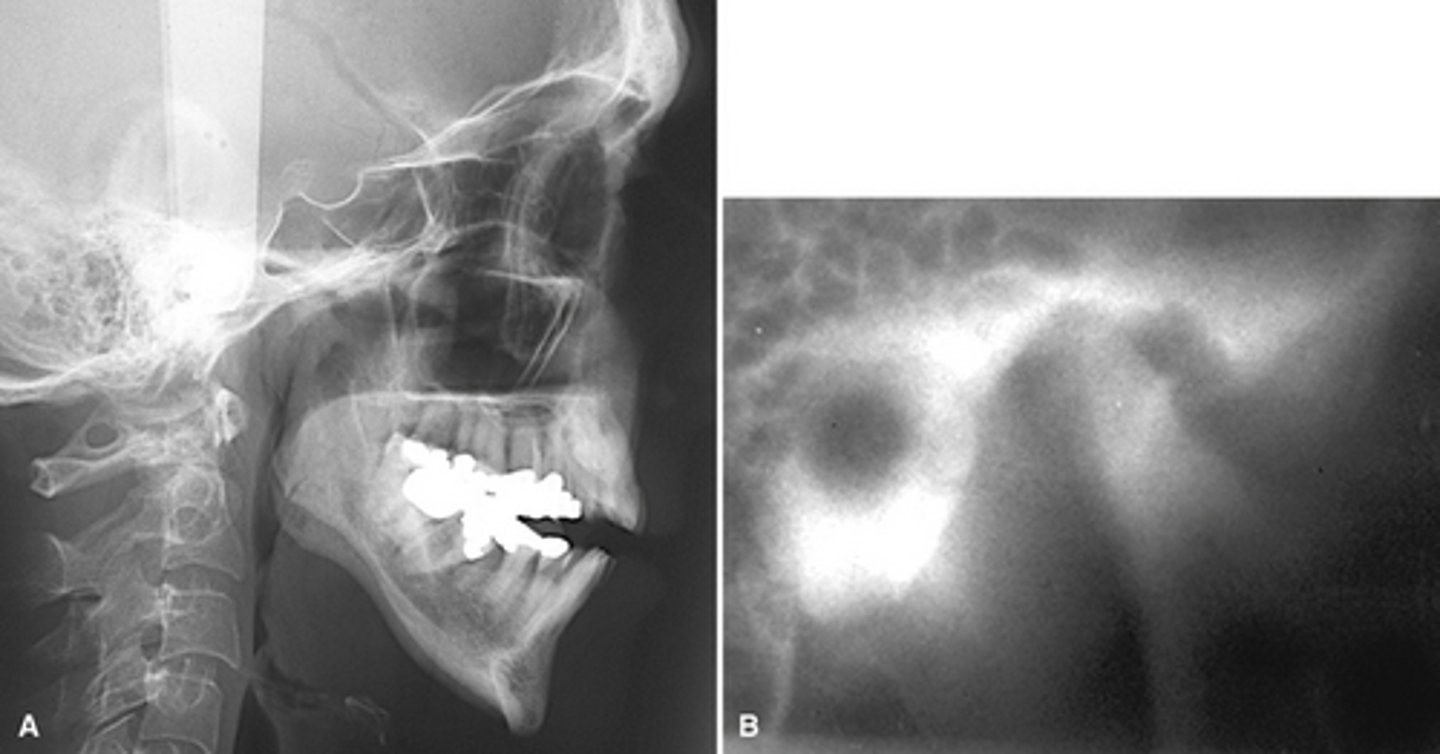
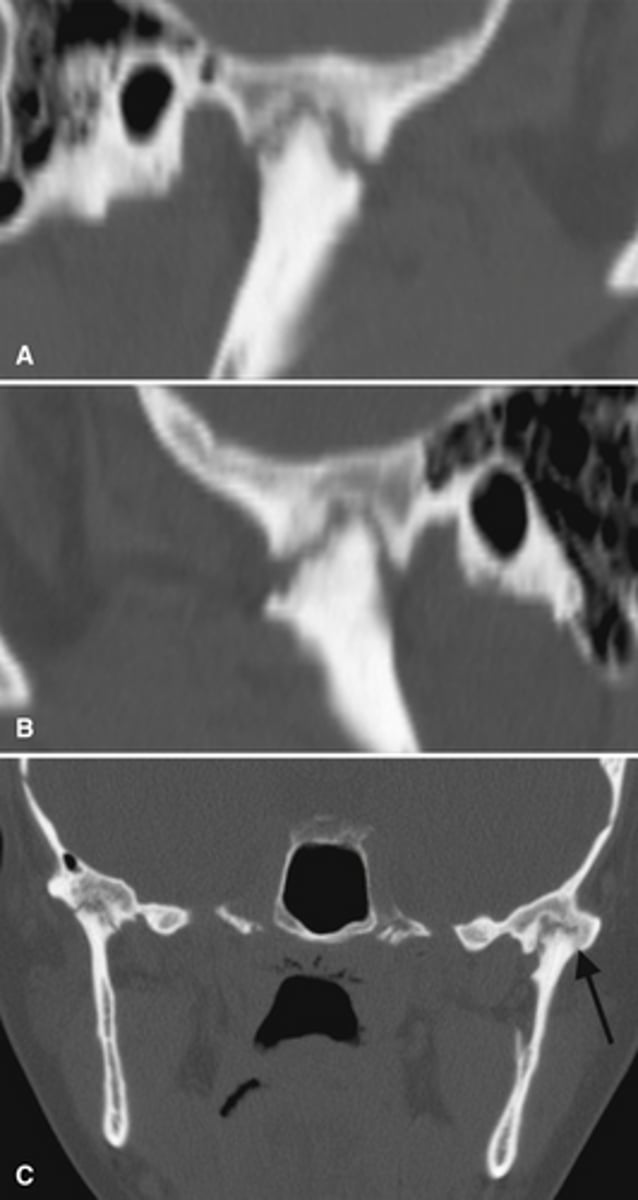
RA (rheumatoid arthritis)
Image A shows a lateral ceph where the patient has a steep mandibular plane and anterior open bite.
Image B shows erosion of the temporal component of the TMJ
What is the diagnosis of the patient based off these radiographs and what are the features?
I didn't wanna type the RA stuff.
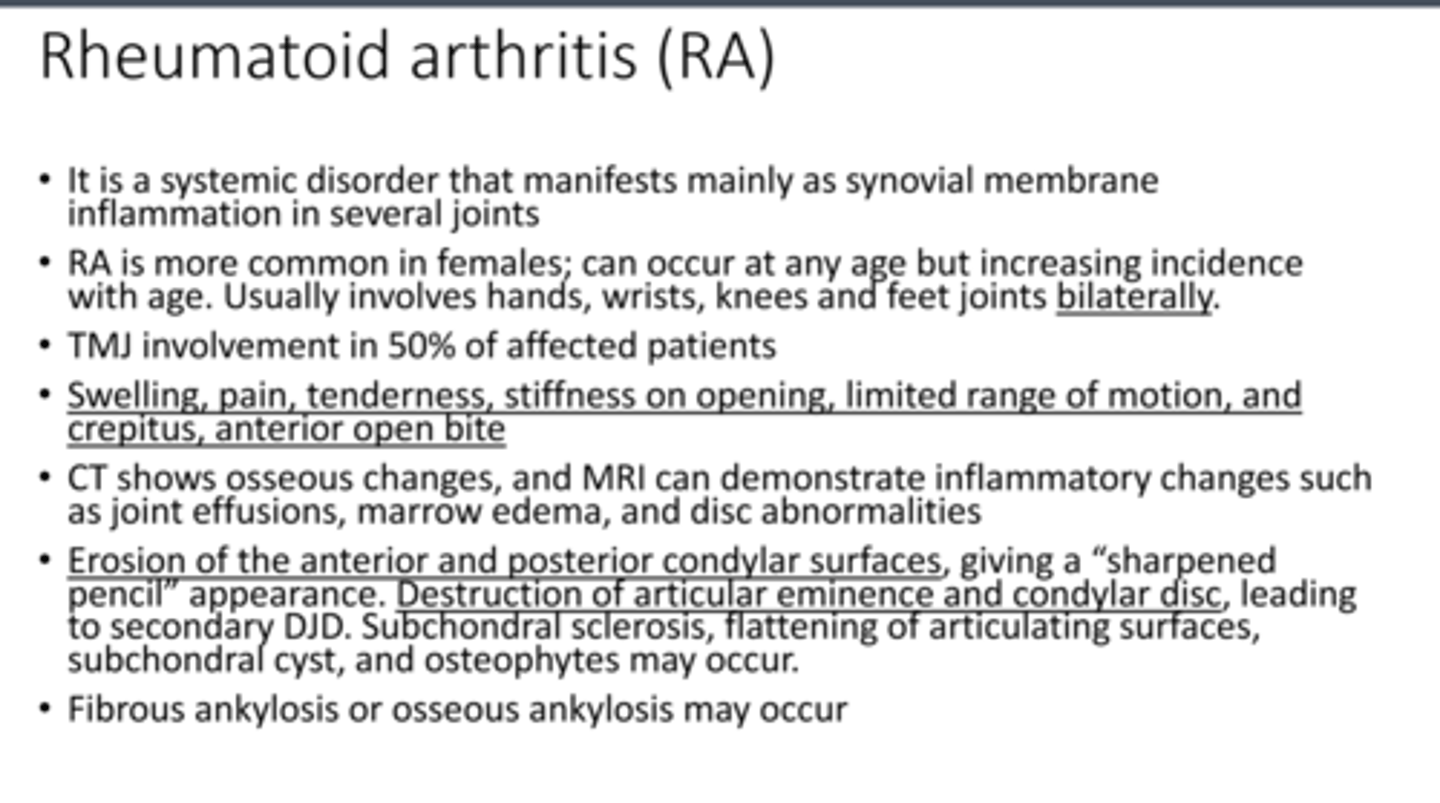
RA (rheumatoid arthritis) - Images shows the erosion of the anterior and posterior condylar surfaces, giving a "sharpened pencil" appearance. Causing secondary DJD.
Adolescence (teens), mainly females; present with asymptomatic or symptomatic TMJ dysfunction and mandibular asymmetry or anterior open bite
Who does progressive condylar resorption impact, and what is the major clinical presentation
progressive condylar resorption

Females, unilateral
synovial chondromatosis affects __________ (males; females)
and is usually ___________ (unilateral; bilateral)
Synovial chondromatosis- multiple ossified bodies surrounding the condyle and within the joint capsule
[periapical] Cemento-osseus dysplasia (PCOD)-
Fibrous dysplasia
Both cause abnormal bone metabolism where cancellous bone is replaced with fibrous tissue containing abnormal bone.
What are the 2 types of bone dysplasia's and the major disease mechanism?
Females
4-5 decade
African Americans
Non-invasive but can cause expansion of the jaw and thinning of adjacent cortices the Involved teeth are vital
Who gets PCOD? Is it invasive?
People with the GNAS1 mutation on chromosome 20
Monostotic: 2-3 decade
Polyostotic (many bones involved) : Before 10yo - some associated with McCune- Albright syndrome with almost exclusively females
Who gets fibrous dysplasia?
PCOD- Most common location anterior mandible
PCOD - Developing- Mature stage
PCOD- Mature stage
PCOD through its stages from Early ---> developing ---> Mature
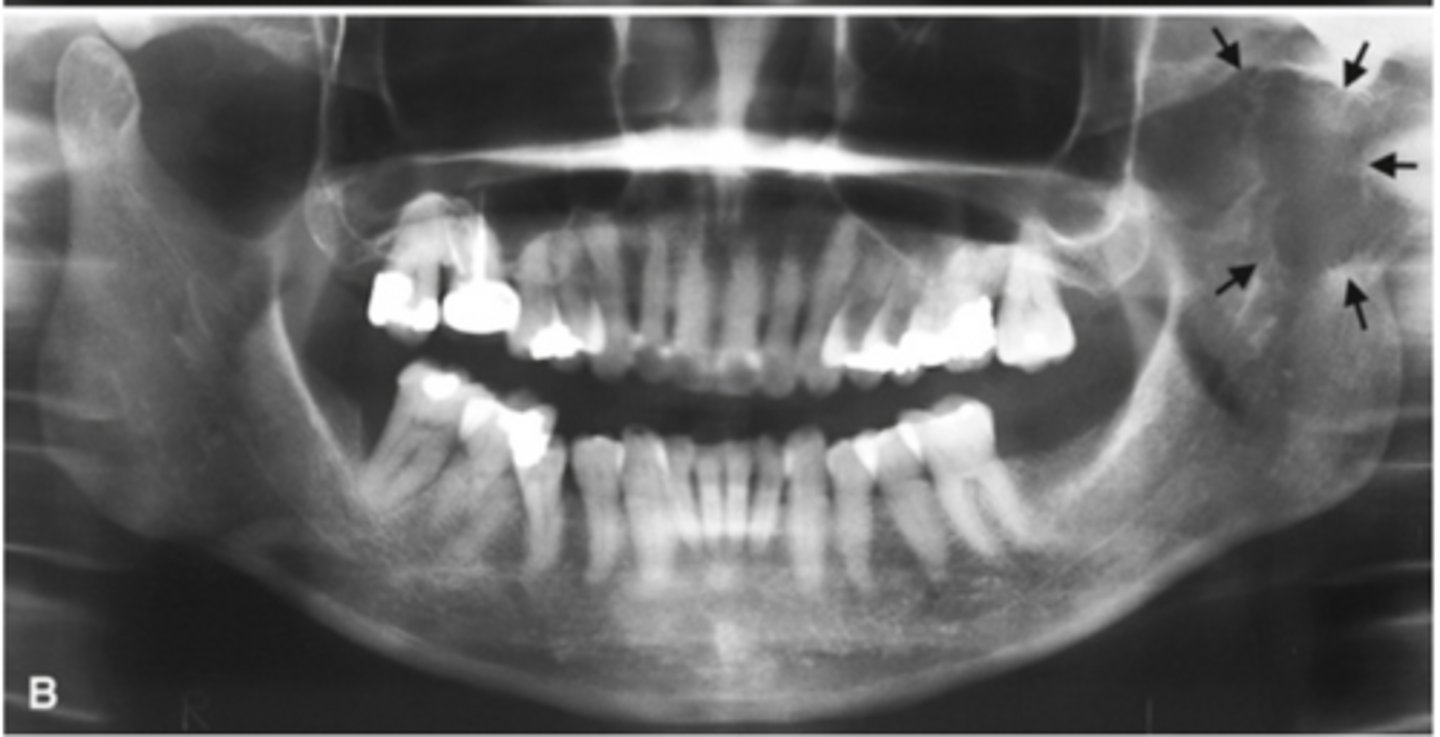
Florid Cemento-Osseous Dysplasia (FCOD)
(florid= widespread) Affects the same demography as PCOD
What dysplasia is pictured and who gets it?

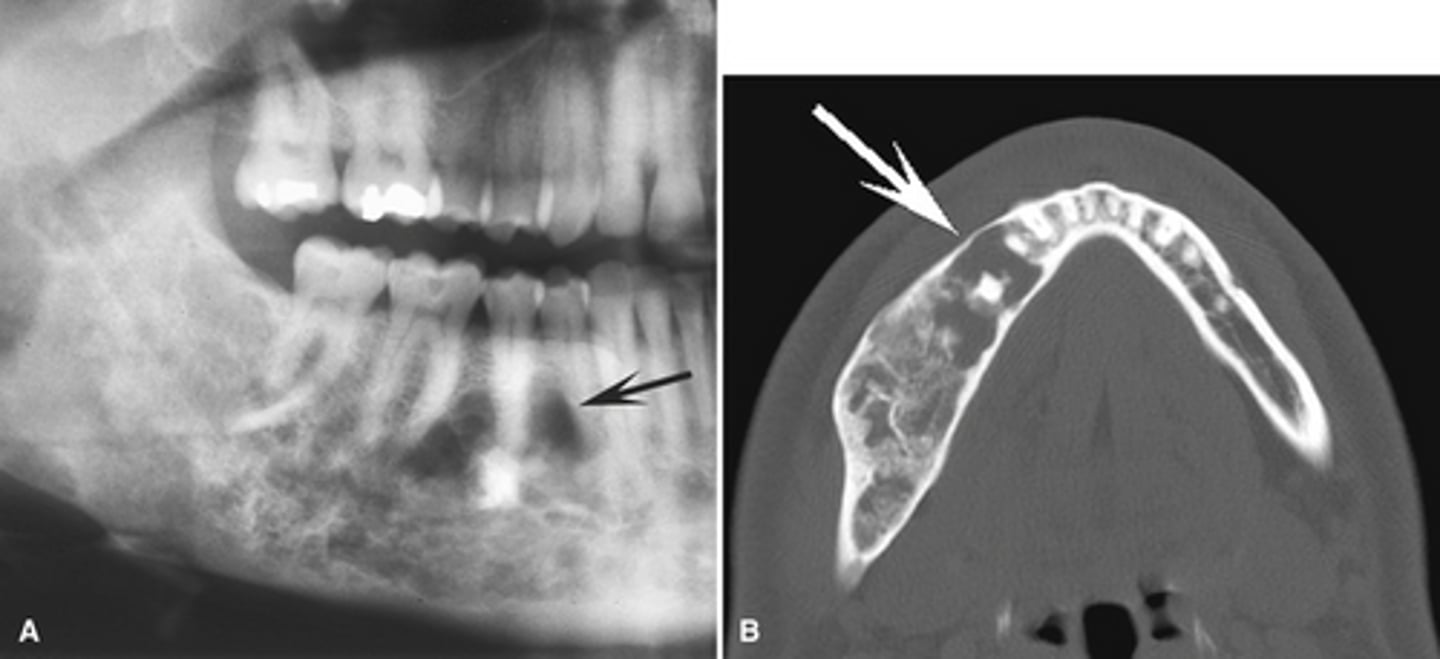
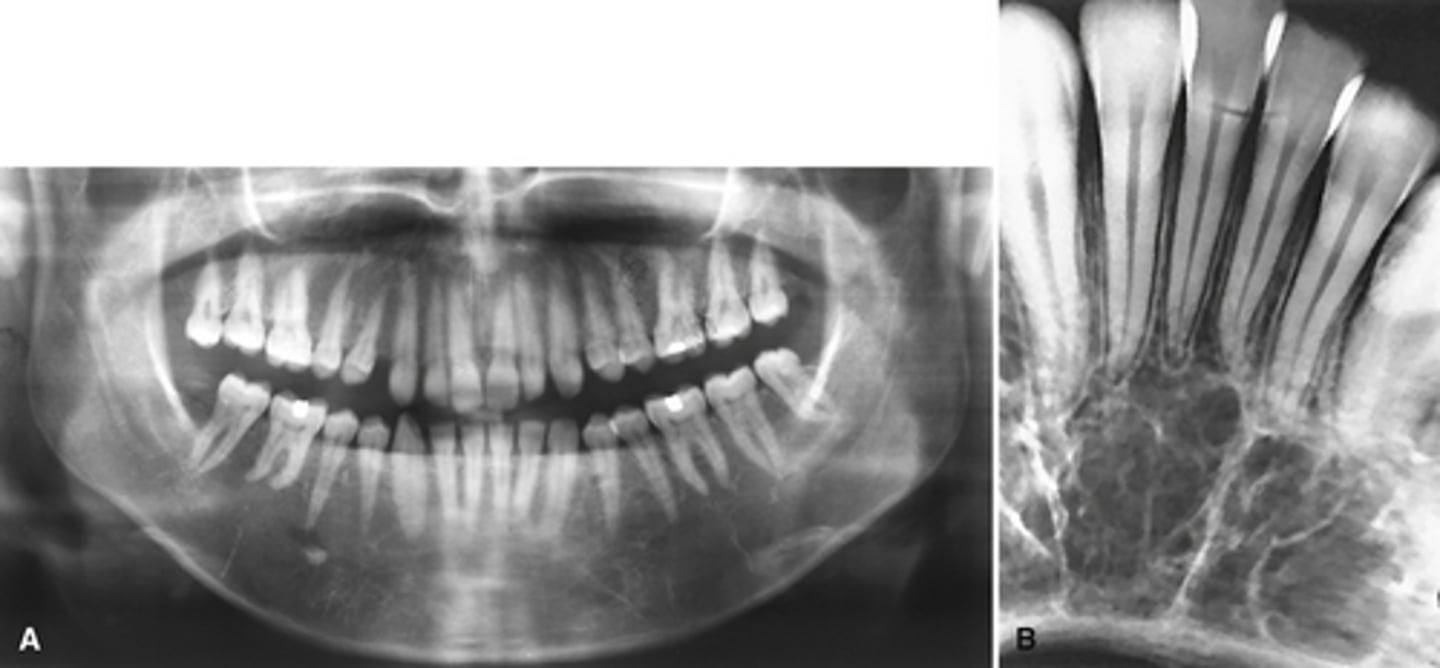
Simple bone cyst; Image caption: simple bone cysts developing with florid cemento-osseous dysplasia. The scalloping feature around the roots of the molar teeth in the right mandible is very characteristic of simple bone cyst
________ is commonly associated with this dysplasia pictured.

Vitality testing- PCOD will still have vital teeth
How do you test if a periapical radiolucent lesion is early stage PCOD or Rarefying osteitis (apical periodontitis).
PCOD will have a radiolucent rim and will also have loss of the lamina dura around the teeth involved
How can you differentiate the mature stage PCOD from dense bone island?
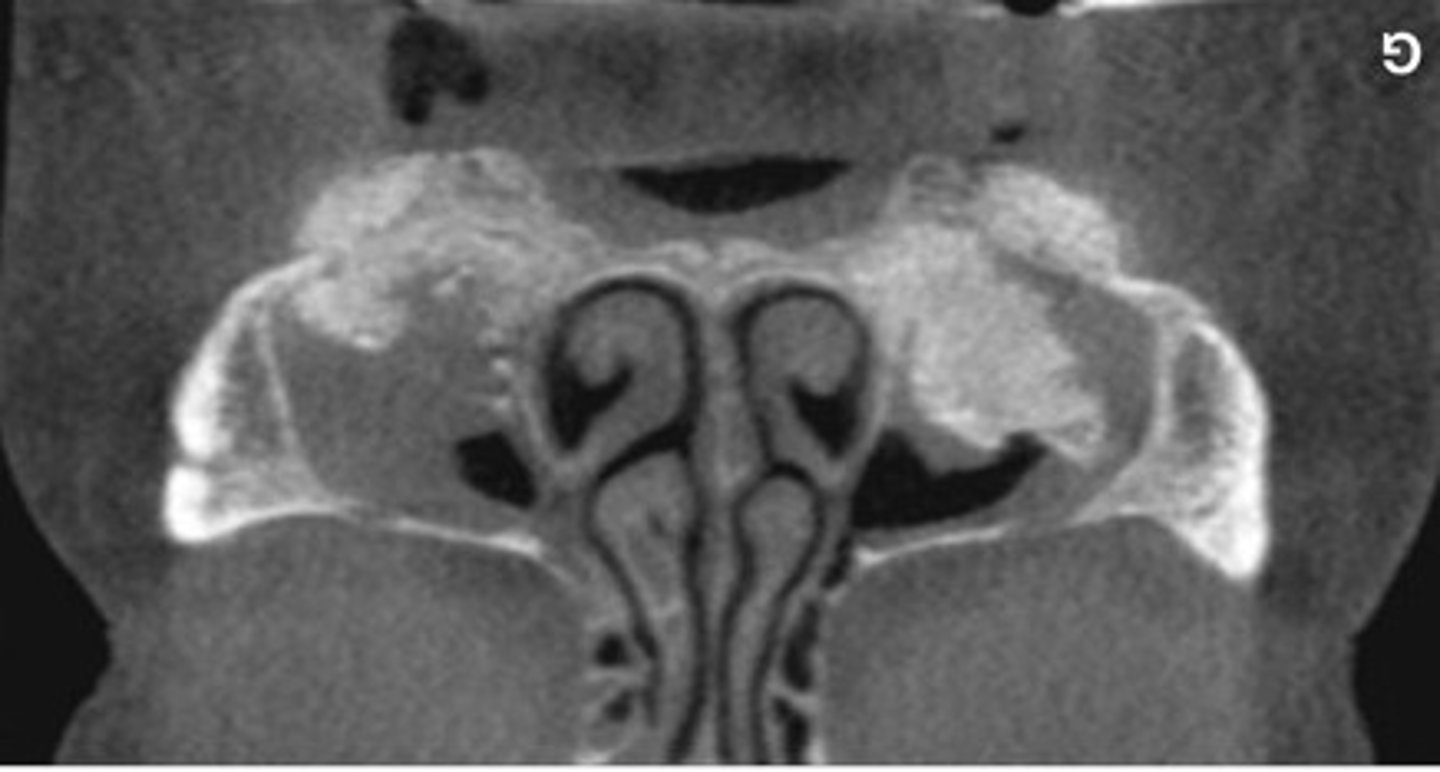
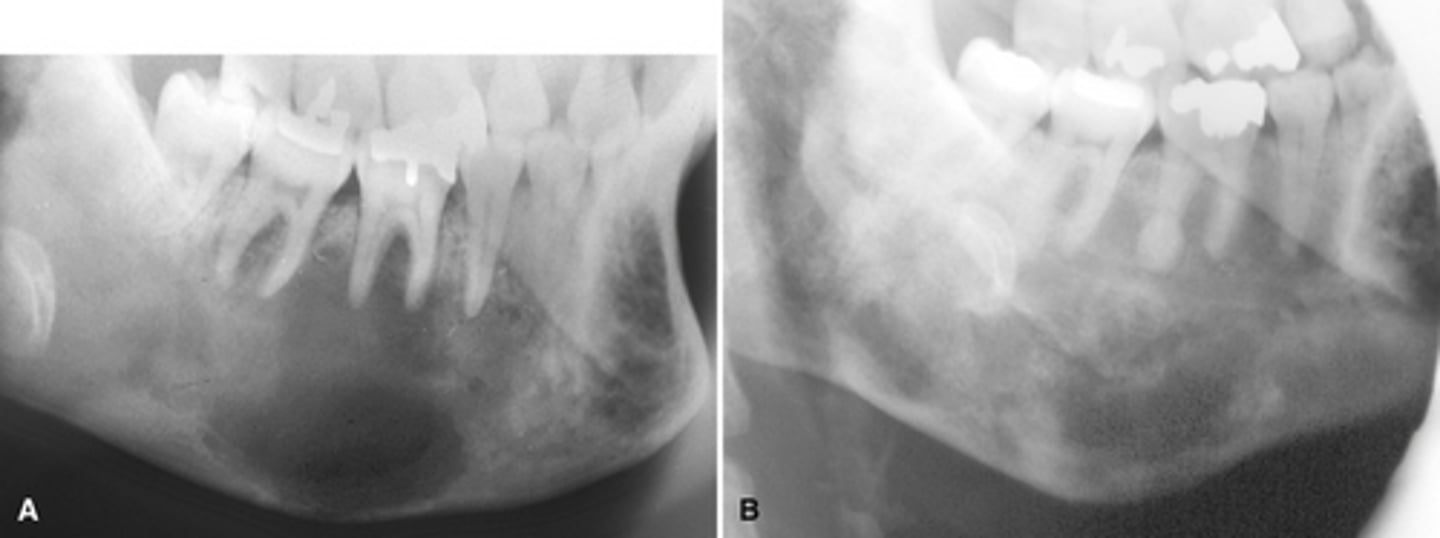
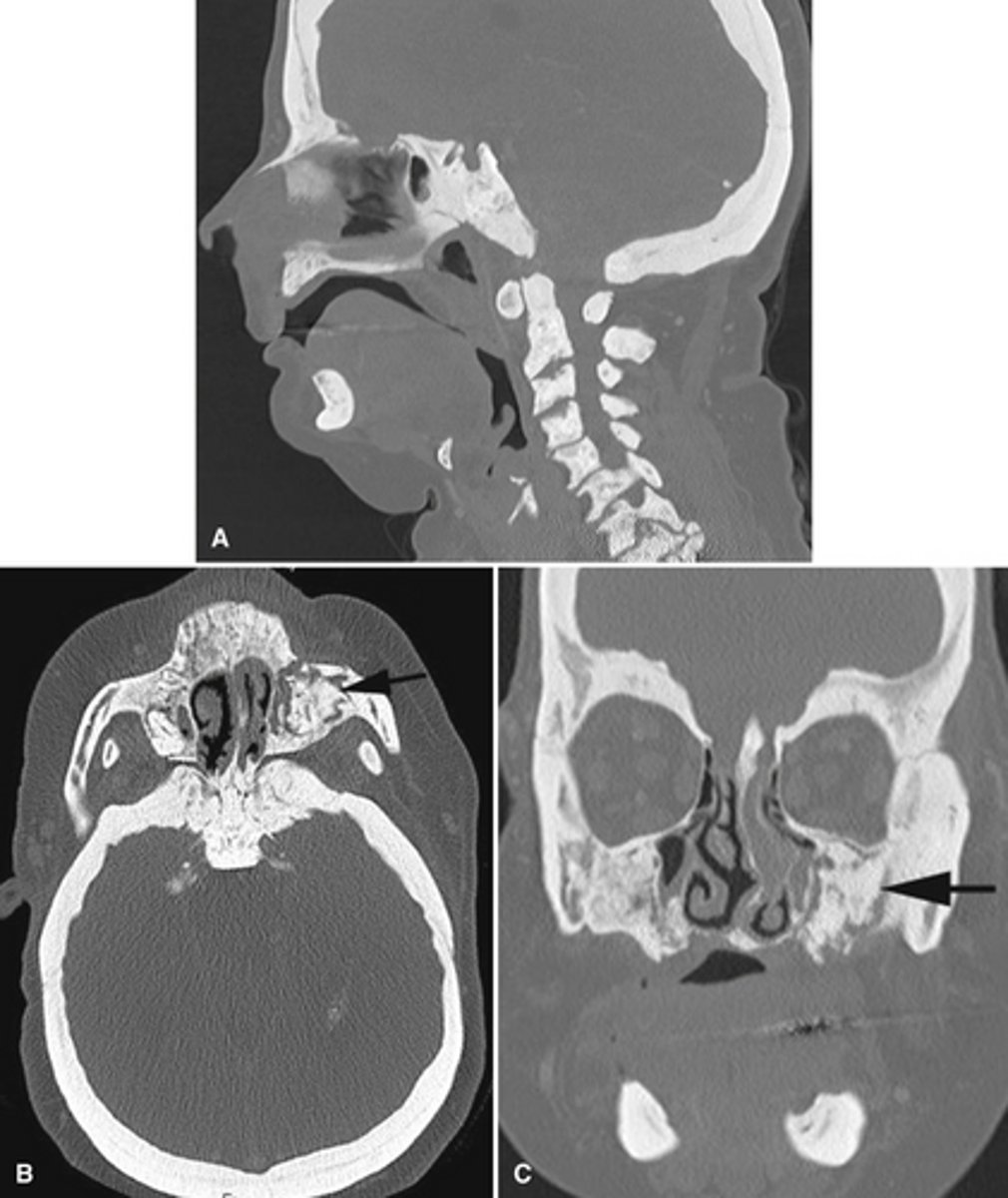
Fibrous dysplasia- ground glass appearance and poorly defined border
(look at the more radiopaque area in the upper right (patients left maxillary tuberosity))

Jaffe type = polystotic fibrous dysplasia and cafe au lait spots; 2-3% polyostotic fibrous dysplasia associated with McCune-Albright syndrome
What is the Jaffe type of fibrous dysplasia? And what syndrome might be associated?
True; it may impinge on nerve foramina
True or False. Extensive polyostotic and craniofacial form of fibrous dysplasia can lead to deafness blindness and loss of smell.
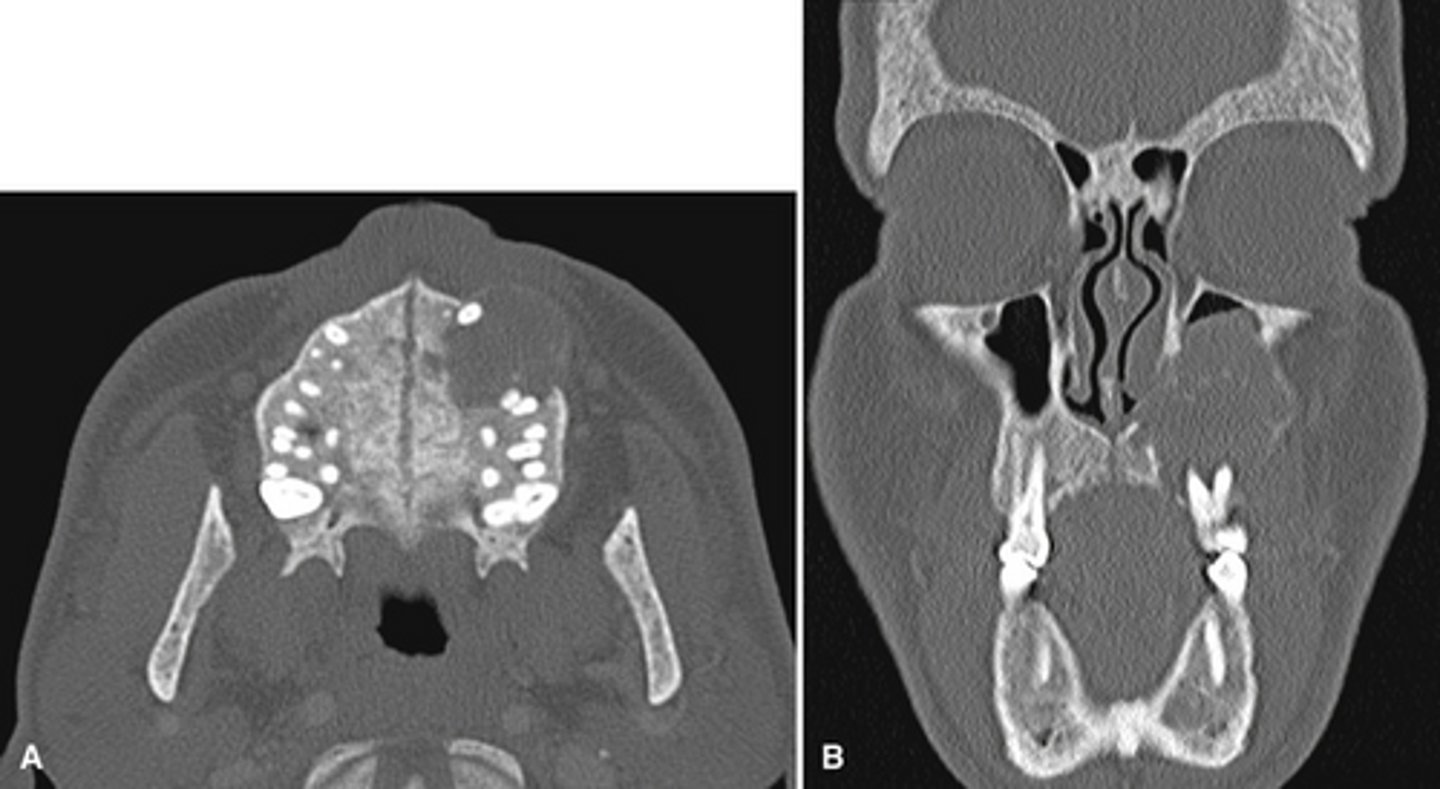
Maxilla; unilaterally
Fibrous dysplasia commonly involves the __________ (mandible, maxilla) and occurs _________ (bilaterally, unilaterally)
False; both are associated with simple bone cyst
True or False. Simple bone cyst is associated with florid cemento-osseous dysplasia but not fibrous dysplasia.
False; it will displace superiorly
True or false.
Fibrous dysplasia in the mandible may displace the IA inferiorly.
True.
True or False. Both types of bone dysplasia will cause the lamina dura outline to disappear and blend into the lesion.
Fibrous dysplasia
Monostotic Fibrous Dysplasia- (a) earlier more radiolucent stage. (b) 18 years later more radiopaque stage
images showing a simple bone cyst developing within a focus of fibrous dysplasia
Paget's disease of bone; Mutations in bone remodeling genes causing abnormal osteoclastic activity followed by vigorous osteoblastic activity leading to enlarged and deformed bone
What is this disease and the mechanism for it?

Paget's disease
What pathology involves enlargement of the jaw which can cause tooth movement, diastema and malocclusion. Bowing of the legs and curvature of the spine?
Paget's disease
Severely elevated serum alkaline phosphatase and elevated urine hydroxyproline are features of what pathology?
Maxilla 2x; Bilateral
Paget's disease commonly involves the __________ (mandible, maxilla) and occurs _________ (bilaterally, unilaterally)
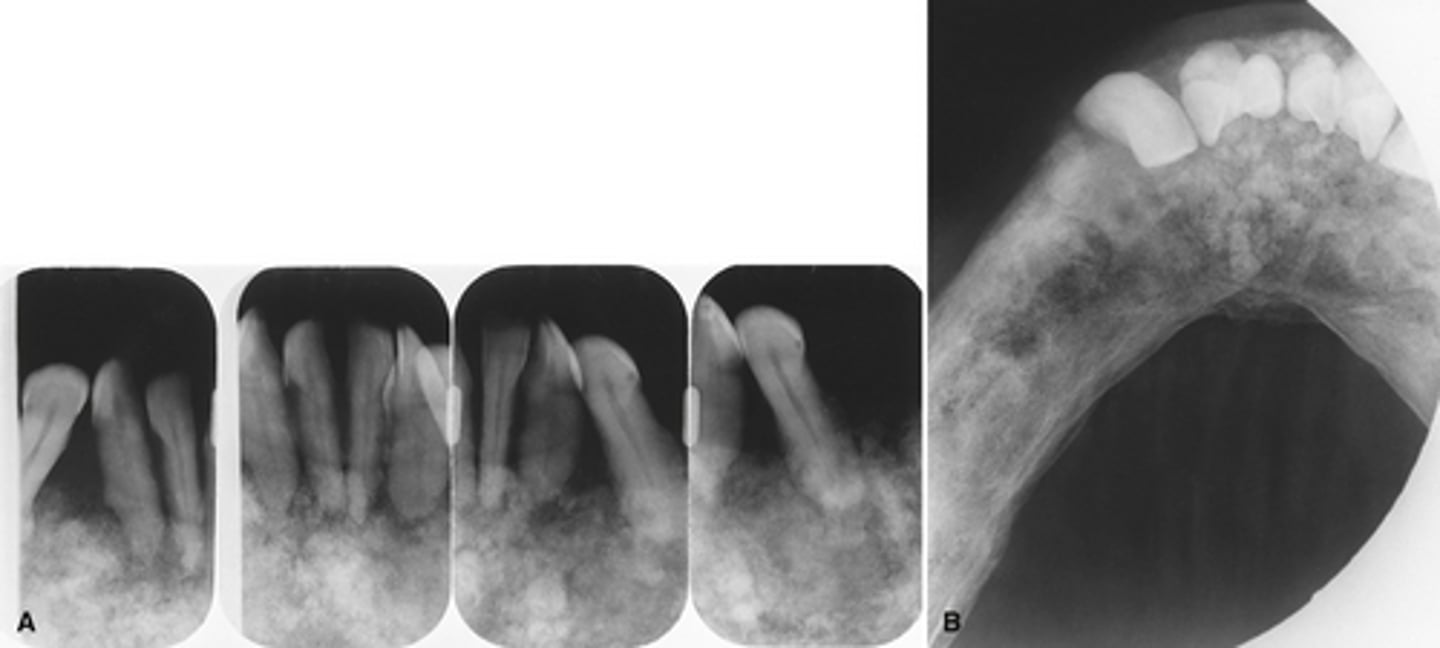
Granular ground glass appearance of the intermediate stage of Pagets with hypercementosis of the teeth.
The images show the intermediated stage of Paget disease accompanied by what additional diagnosis.
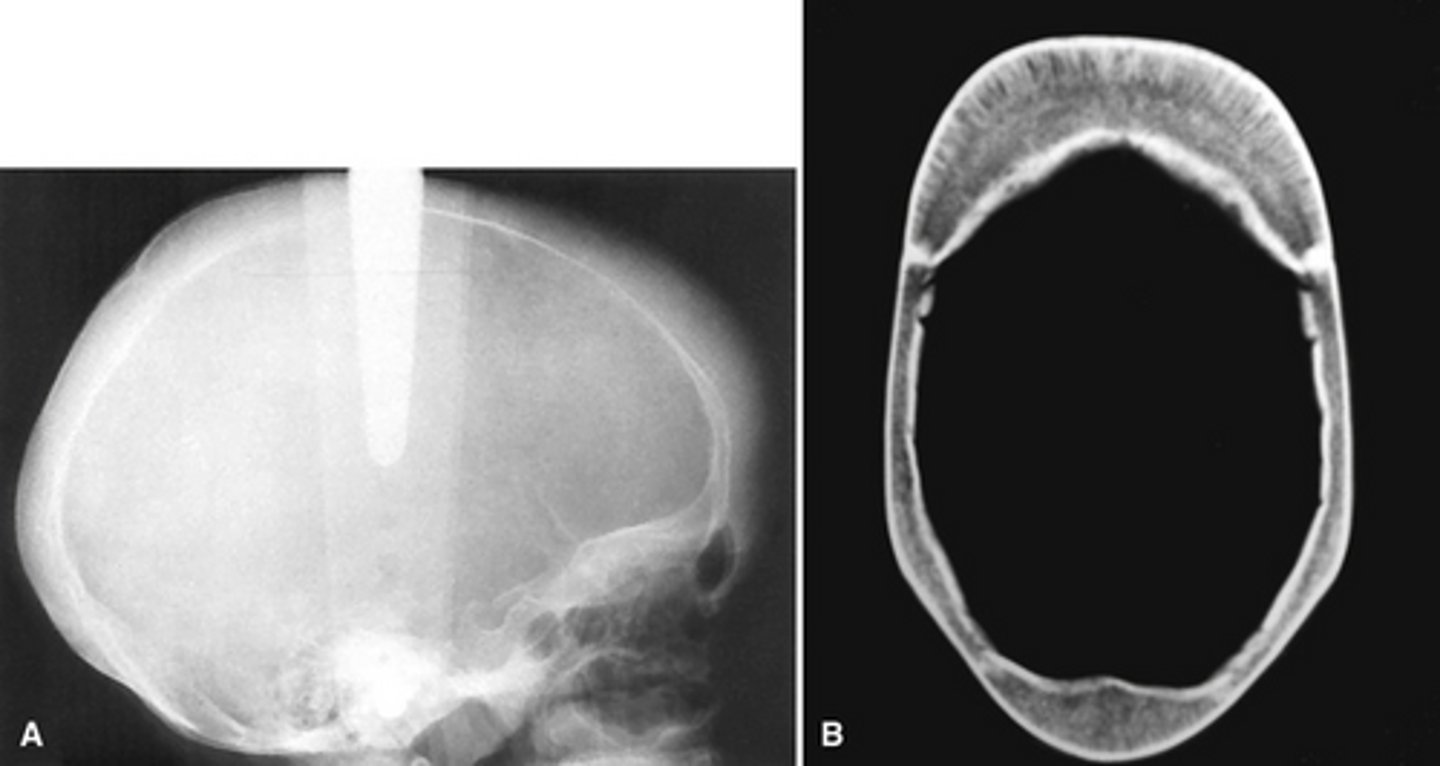
Sickle cell anemia
The radiographs show widening o the diploic space (between the inner and outer cortices) and a "hair-on-end" appearance are features of what pathology?
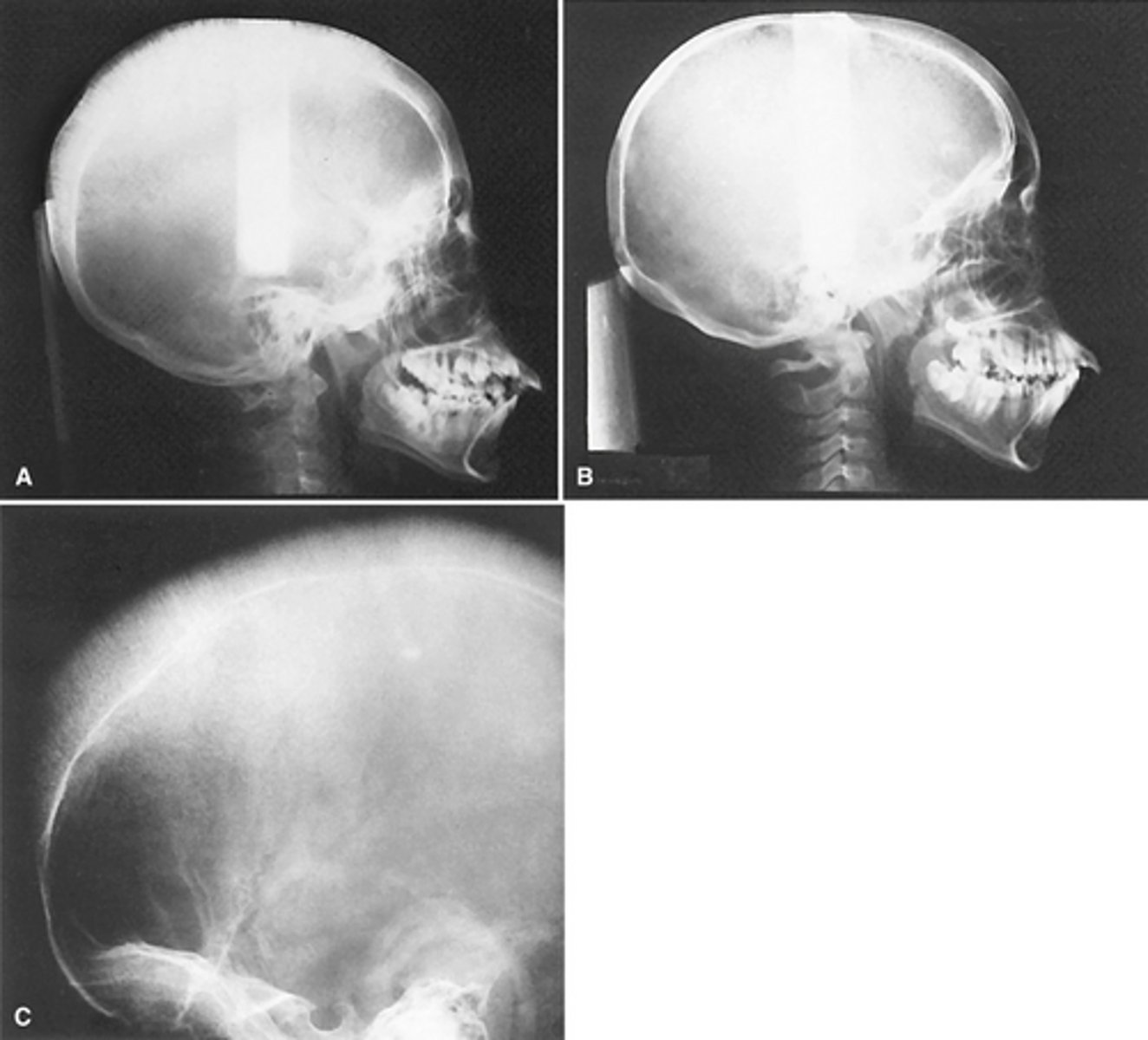
Abnormal blood --> reduced O2 carrying capacity --> spleen destroys the abnormal cells ---> anemia --> bone marrow attempts to compensate --> hyperplasia and large marrow spaces
What is the disease mechanism for sickle cell anemia?
Thalassemia
This pathology is due to a genetic defect that causes RBC's with reduced hemoglobin content.
True
True or False. Thalassemia results in hyperplasia of the bone marrow and will radiographically looks similar to sickle cell anemia.
False: the severe is in infants and the mild in adults.
True or False. Thalassemia Major occurs in adults that will have prominent cheekbones and a protrusive premaxilla and Thalassemia Minor occurs in infants.
Sickle cell anemia or Thalassemia (both with have enlarged marrow spaces)
These enlarged marrow spaces are indicative of
Osteopenia... but it is not a pathology it is a normal aging process
What is the pathology depicted in the image showing a net decrease of bone formation?

Rickets - Growing
Osteomalacia - Mature
Vit D- Resistant Rickets
*(hypophosphatemia = low serum phosphate cause the kidneys can't resorb phosphorus)
This disease results from a lack of vitamin D and calcium in the body and is called _______growing in infants and children and ________ in adults with mature skeleton. Another name is _______ when the hypocalcification is due to hypophosphatemia.
Vit D- Resistant Rickets aka hypophosphatemia rickets
After checking this patients serum levels you see
Low Calcium
Low Vitamin D
Low Alkaline phosphatase
What is the diagnosis?

Osteopetrosis ---> overly dense bones
can cause
- narrowing of bony canals
- loss of marrow space
- poor vascularity
This pathology may cause; hydrocephalus, blindness, deafness, facial nerve paralysis, anemia, leukopenia, thrombocytopenia, and increased risk of osteomyelitis from tooth infection; what is it and how can it cause these other problems?
Osteopetrosis; Bone marrow transplant
What is this and how might you treat it?

Osteopetrosis (marble bone disease) (albers-shonberg disease)
Secondary hyperparathyroidism (compensatory PTH released due to inadequate intestinal vitamin D absorption)
After checking a patients serum levels you see
Elevated PTH
Low Vitamin D
Elevated calcium
What is the diagnosis?
Primary hyperparathyroidism (tumor of the parathyroid gland --> increased PTH)
After checking a serum levels you see
Elevated PTH
Normal Vitamin D
Elevated calcium
What is the diagnosis?

hyperparathyroidism; Brown tumor (aka central giant cell granuloma)
The top images show show loss of lamina dura around the teeth in a patient with _____________. The bottom image shows ________ developing under the molar?

Brown tumor in a patient with hyperparathyroidism
What is the pathology in the radiographs?
hypoparathyroidism - (insufficient secretion of PTH due to damage to or removal of the parathyroid)
After checking a serum levels you see
Low PTH
Normal Vitamin D
Low calcium
What is the diagnosis?
Pseudohypoparathyroidism - (defect in the response to PTH in target tissues)
After checking a serum levels you see
Normal PTH
Normal Vitamin D
Low calcium
What is the diagnosis?
Acromegaly - pituitary gland hyperfunction in adulthood
This patient developed a class III skeletal relationship and enlargement of the sella turcica. What is the diagnosis?