Headache, Fever, & Musculoskeletal Injuries
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
Abbreviation for HCP,PCP,PMH
HCP→ Health care provider
PCP→ Primary care provider
PMH→ Past medical history
Tension-Type Headache
Location→ Bilateral, over top of the head extending to base of skull
Nature→ Varies: diffuse ache to tight pressing, constructing pain
Onset→Gradual
Duration→ Minutes to days
Non-headache symptoms→ Scalp tenderness, neck or muscle pain
Migraine headache
Location→ Usually unilateral “one side.”
Nature→ Throbbing sometimes preceded by aura
Onset→ Sudden
Duration→ Hours to days
Non-headache symptoms→ Nausea
Sinus Headache
Location→ Face, forehead, periorbital area
Nature→ Pressure behind eyes or face, dull, bilateral, worse in morning
Onset→Simultaneous with sinus symptoms
Duration→ Days
Non-headache symptoms→ Nasal congestion
Exclusions To Self Care
Severe head pain
rapid onset of maximum pain
Concerning change in headache pattern (first or worst, gradual escalation over months)
Persisting for 10 days ± treatment
Occur> 15 days per months for 6 months
Third trimester of pregnancy
New headache during pregnancy
Age< 8 years
HIgh fever or signs of serious infection
Neck stiffness
History of liver disease or >- 3 alcoholic drinks/day
Association with underlying pathology
Migraine symptoms with no previous migraine diagnosis
Neurologic changes (seizures, vision changes, altered mental status )
High risk comorbid conditions (cancer, HIV)
Non-pharmacologic therapies for Tension
Relaxation exercise
Physical therapy-stretching and strengthening head and neck muscles
Chronic headaches- headache log to document triggers, frequency, intensity, duration, response to treatment
Headache diary :> 8 weeks, frequency, duration, related symptoms, precipitating factors, medications used for relief, menstruation scedule
Non-pharmacologic therapies for Migraine
Maintaining regular schedule: sleeping, eating, exercise
stress management
Ice or cold packs applied with pressure to forehead or temple areas
Avoiding triggers foods, hunger/low blood sugar
Avoiding light, noise and other triggers
see headache diary above
Treatment goals headache
Alleviate acute pain
restore normal functioning
prevent relapse
minimize side effects
General treatment approach headaches
Limit OTC analgesic use to < 3 days per week OR < 14days per month (prevent medication overuse headache)
For migraines, medications work best when taken during aura (as applicable) or at the onset of symptoms
Sinus headaches respond well also to decongestants
Concomitant use of a decongestant + nonprescription analgesic helps relieve sinus headache pain.
When to follow up:
Headache persists>10 days
Headache worsens despite self-treatment
After HCP (health care provider) diagnosis/follow-up:
Chronic headaches- after 4-6 weeks of management
Episodic headaches- after 6-12 weeks of management
Fever Pathophysiology
Average body temperature
97.5-98.9 F (36.4-37.2 C)
Common core body temp= 98.6F (37)
Body temperature is regulated by the hypothalamus and neurons in skin and CNS
Pyrogens- fever producing substances
exogenous: toxins, microbes
endogenous: immune cytokines
Prostaglandins- produced and released in response to pyrogens and elevate body temperature set in the hypothalamus
Oral
Mouth
wait 20-30 min to use after eating/drinking
Rectal the gold standard
rectum
preferred in children most reliable
Axillary
armpit
least reliable
Tympanic
ear
ensure proper technique for best measurement
Temporal
forehead “No touch”
convenient
Exclusions To Self Care
Patients >3 months old with rectal temp>- 104 F
Patients < 3 months old with rectal temp >- 100.1F
children with a history of febrile seizures or seizures
serve symptoms of infection
risk of hyperthermia
Impaired oxygen utilization(cardiovascular or pulmonary disease)
impaired immune function (cancer, HIV)
CNS damage (head trauma, stroke)
Patients > 2 years old with fevers that last 3 days without treatment
patients < 2 years old with fevers that last > 24 hours
Nonpharmacologic therapies for fever
Fluid replacement
children - increase by 20-60 ml (1-2 oz) per hour
Adults- increase by 60-120 ml (2-4 oz) per hour
Wearing lightweight clothing, removing blankets
Maintain a comfortable room temperature
Body sponging/bathing- limited effectiveness
Do not recommend ice baths or alcohol solutions
Approach to Treatment Fever
Ensure accurate measurement of the body temperature
Product specific
Use the same thermometer at the same site for duration of illness
If non-excluded, treatment may include OTC antipyretics (APAP or Ibuprofen) and non-pharm measures
Counseling
Do not use pharmacologic therapy (antipyretics) for more than 3 days without direction or further evaluation of a healthcare provider
Pediatrics &liquid preparations- measure the dose to avoid medications errors
Do not alternate between APA and ibuprofen- this may increase the risk of med errors and side effects
Follow-up see a healthcare provider if:
Fever persists > 72 hours
Additional symptoms develop (stiff neck, serve headache, sore throat, serve ear pain, unexplained rash, repeated vomiting/diarrhea)
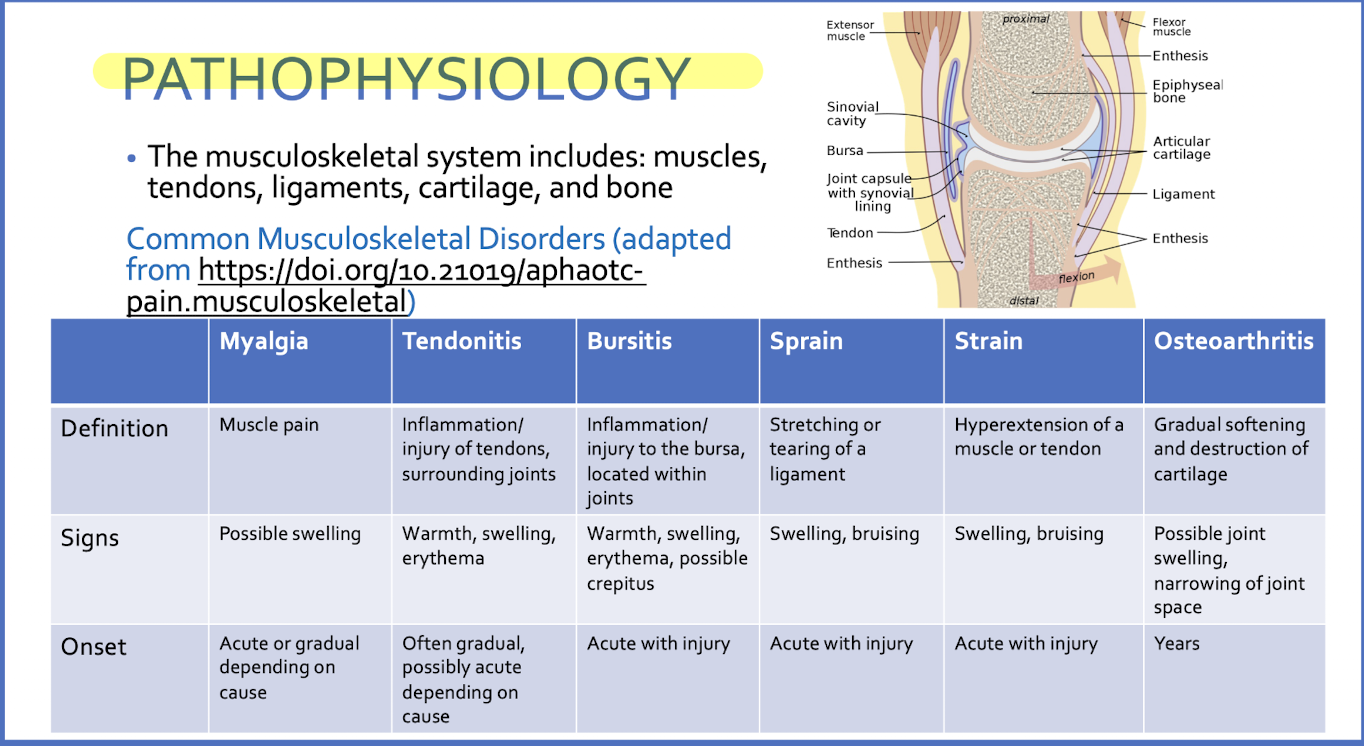
Pathophysiology Musculoskeletal Pain
Exclusions to self care
Serve pain (pain score>6)
Pain lasting > 10 days
Pain persisting > 7 days after treatment with a topical analgesic
increase in intensity or change in character of pain
Pelvic or abdominal pain (excluding menstrual pain)
Accompanying signs of infection, nausea , or vomiting
Visually deformed joint, abnormal movement, weakness/ numbness in limbs suspected fracture
pregnancy
< 2 years of age
back pain pain associated with loss of bowel and bladder control
Non-pharmacologic therapies RICE for muscle
Rest
Rest injured area until pain is reduced, generally 1-2 days
Use slings, splints, crutches as necessary
Ice
Apply ice as soon as possible after injury
15-20 min increments
At least 3-4 times daily
Continue until swelling subsides (usually 1-3 days)
Compression
Apply compression to the injured area with elastic support bandage
Elevation
Elevation the injured area at or above level of heart 2-3 hours a day (if possible)
Non-pharmacologic therapies- Heat
For non-inflammatory case only - do not administer to injured or inflamed areas
Do not use with topical agents ( analgesic or other)
Do not use on broken skin
Do not use on areas of skin with decrease
Recommended as adjunct non-pahrm therapy of osteoarthritis
Increase blood flow, reduce muscle spasm alleviate stiffness
Apply in 15-20 min increments 3-4 times daily
Non-Pharmacologic Therapies OTHER
Stretching, massaging and adequate hydration
TENS ( transcutaneous electrical nerve stimulation)
Chiropractor
Physical therapy
Acupuncture
Magnesium sulfate baths ( Epsom salt)
Treatment Goals
Decrease intensity of pain
Decrease duration of pain
Restore function of the affected area
Prevent re-injury and disability
Prevent acute pain from becoming chronic persistent pain
Approach To Treatment Musculoskeletal Pain
Non-drug therapy: RICE or heat
OTC oral analgesics-Limit to 10 days of self-care use
APAP- can be used for inflammatory pain, including osteoarthritis
NSAIDs-better for inflammatory pain
Topical analgesics
Do not concurrently with heat
Monitor for changes in skin condition
Do not apply to wounded, broken, or irrated skin
Avoid eyes, inside of nose, mouth or genitals.
Follow-up
Pain persists >10 days (excluding osetoarthritis
Symptoms do not improve for >- 7 days
Acetaminophen (APAP)
MAO
central inhibition of prostaglandin synthesis
BLACK BOX WARNING
hepatotoxicity
Counsel patients
Adhere to MDD recommendations
CHeck other RXs and OTCs that may contain APAP
Acetaminophen Dosing
Adults (>12 years)
IR products: 325mg-1000mg every 4-6 hours as needed
ER PRODUCTS: 600-1300MG EVERY 8 hours as needed
Children (<12 years)
10-15 mg/kg every 4-6 hours as needed
maximum of 480mg per dose *5 doses (2,400 mg) OR 75mg/kg/day
Acetaminophen Considerations
Maximum daily dose of APAP from all non prescription and prescription products (single ingredient or combination)
< 4,000mg daily → Appropriate for acute (short term) use or those under HCP supervision
< 3,000 mg daily→ Appropriate for those using chronically, or without HCP supervision
< 2000 mg daily→Consider for in those with liver disease, use of other hepatotoxic drugs, poor nutritional intake, warfarin or > 3 alcoholic beverages daily
Children→Do not exceed 75mg/kg/day or 2,400 daily
Stop taking APAP and seek medical attention if you develop nausea, vomiting drowsiness, confusion, or abdominal pain
NSAIDs -MOA
Reversibility inhibit COX-1 and COX-2 enzymes
Decreased prostaglandin formation (both centrally and peripherally)
Decreased pain, fever, inflammation
OTC NSAIDS are non-selective
risks
Cox-1 inhibition→increased risk of bleeding
COx-2 inhibition → increased of clotting
Cox1 and 2 inhibition→ increased risk of GI events (ulcers, bleed)
NSAIDs warning
BLACK BOX WARNINGS (CLASS WIDE)
Stomach bleeding and other GI events
Serious CV events, including myocardial infarction (MI), stroke
Adverse effects:
Edema, heartburn, dyspepsia, GI bleeds, CV events
Do not use IBU with ASA- will prevent anti-platelet effects of
Via competitive inhibition of COX-1 binding site
Not true with naproxen
NSAID + Salicylate considerations
Contraindications
Chronic/recurrent GI ulcers
coagulation/bleeding disorders
concurrent anticoagulants/ antiplatelets
Heart failure
Kidney disease
Aspirin allergy, aspirin sensitive asthma, nasal polyps, rhinitis
High risk for heart disease or stroke (unless supervised by healthcare provider)
Last trimester of pregnancy (unless surprised by healthcare provider)
Avoid salicylates in history of gout or hyperuricemia
Ibuprofen Dosing
Adults
200-400 mg every 4-6 hours as needed
maximum of 1,200 mg daily
Children (>6 months and <12 years )
5-10 mg/ kg 6-8 hours as needed
Maximum of 300 mg per dose *4 doses (1,200 mg daily) or 40mg/kg/day
Naproxen Dosing
Adults (>12 years )
220mg every 8-12 hours as needed
may take 440mg (2 tablets) within the first hour for initial dose
Maximum of 660 mg daily
Children DO NOT USE
Salicylates MOA
MOA - inhibition of COX-1 and COX-2
Antiplatelet effects with inhibition of TXA2 (thromboxane) (eg baby aspirin)
Compared to NSAIDs, platelet inhibition is irreversible (NSAIDs are reversible)
Dosage forms -ASA
Regular IR: absorbed in stomach and small intestine, may irritate stomach
Enetric- coated: delay absorption until small intestine, avoid stomach irritation, ulcer risk
PPIs other antacids may negate this effect
Buffered: co-formulated with an antacid to reduce stomach upset symptoms
ASA intolerance
Cutaneous or respiratory
Not an immunologically mediated allergy
Increased risk in those with chronic urticaria, nasal polyps
Aspirin Dosing
Adults(>18 years)
325-1000 mg every 4-6 hours as needed
Maximum of 4000mg daily
Children (< 18 years) DO NOT USE
Magnesium Salicylate Dosing
Adults ( >18 years)
1160mg every 6 hours as needed
Maximum of 4640 mg daily
Children (<18 years) DO NOT USE
Salicylate Considerations
REYE’s Syndrome
Do not give aspirin or products containing aspirin to children and teenagers who have or are recovering from chicken pox or influenza-like symptoms.
Recommend avoiding use in children and teenagers (<18 years old)
Signs/symptoms: lethargy, nausea, vomiting, changes in behavior
can lead to neurologic damage, fatty liver, hypoglycemia
AVOID ASA CONTAINING PRODUCTS IN CHILDREN!!
NSAID + APA
product containing both IBU +APAP
considerations + contraindications apply from BOTH products
Side effects and possible toxicity from BOTH products
Caffeine
Indicated only for treatment of headaches
Found in several combination product such as Excedrin
MOA (in headache)- vasoconstriction through adenosine receptor antagonism
May cause withdrawal headaches when chronic consumption is stopped
Caffeine itself may be a trigger for migraines
When will my medication work
Acetaminophen
onset: 30-60 minutes
duration: 4-6 hours
Ibuprofen
onset:15-30 minutes
duration: 6-8 hours
Naproxen
onset: 30 -60 minutes
duration: up to 12 hours
Aspirin
onset: <60 minutes
duration: 4-6 hours
Special populations
Pediatric
6 months- 2 years (you dose!)
> 2 years can use APAP or IBU per label
<12 avoid naproxen
<18 avoid ASA
Pregnancy
APAP is recommended
NSAIDs- do not use in 3rd trimester ( okay in 1st 2nd is the safest)
Avoid ASA
Lactation
IBU demonstrated best safety
APAP and NSAIDs are compatible
Avoid ASA
Elderly
NSAIDs not recommended
Kidney dysfunction
Avoid NSAIDs and salicylates
Liver dysfunction
Avoid APAP
Diclofenac (Voltaren )
February 2020-FDA reclassified diclofenac 1% topical gel as a nonprescription drug
approved for the treatment of osteoarthritis in the hand, wrist, elbow, foot, ankle, and knee in patients> 18 years of age
Topical NSAID- similar riks as oral?
Amount absorbed systemically is 6% or 17* less than oral diclofenac (an Rx NSAID)
Indicated for osteoarthritis
If no pain relief within 7 days- conatct HCp
DO not use use longer than 21 days ( unless directed by HCP)
Diclofenac- Dosing
use the dosing card included in every box
total MDD (including all joints)= 32 g daily
upper body
apply 2 grams up to 4x daily
MDD=8g per joint
lower body
apply 4 grams to 4 x daily
MDD= 16g per joint
Lidocaine
MOA
Inhibition of nerve impulse conduction via sodium channel blockade
Dosing
Vary by formulation
Patches: up to 3 applications at once up to 12 hours in 24 h
Caution
Avoid in patients sensitive/ allergic to other amide anesthetics (‘caine’s-benzocaine prilocaine, procaine/novocaine, etc)
Do not exceed MDD, do not apply to open wounds
Capsaicin
MOA
Triggers the release and eventual depletion of substance P from sensory neurons at site of application
Elicts a transient feeling of warmth or burning stimulation of TRPV1 receptor
Repeated applications decrease burning sensation
Dosing
Initiate at once every 4-6 hours, once pain relief is noticed, may decrease to 3-4x daily
Counseling
Use gloves during AND wash hands thoroughly after applying
AVOID touching mucous membranes
Pain relief may take anywhere from 14 days to up to 6 weeks in cases of chronic pain
Methyl Salicylate
• MoA
Counterirritant – production of a less severe pain to counter a more intense one via nerve stimulation (i.e., a distraction)
Rubefacient – vasodilation of cutaneous blood vessels, leading to a sensation of heat that may exert a counterirritant effect (the “hot” in IcyHot)
Inhibition of central and peripheral prostaglandin synthesis
• Adverse reactions
Local – irritation, rash, blistering
Systemic – salicylate toxicity (increased risk with heat exposure and exercise after applying)
Some systemic salicylate absorption – use with caution in populations sensitive to salicylate effects (e.g. patients at a higher risk for bleeds)
• Avoid in:
Children
Those sensitive to aspirin, severe asthma, nasal polyps
Trolamine salicylate
MOA-salicyate
not a counterirritant
Absorbed through skin and produces synovial salicylate concentrations similar to ASA
Adverse effects
Same as salicylates
Utilization
Efficacy date is lacking
Use if other counterirritants are bothersome (irritation, scent)
Camphor
MOA
counterirritant at concentration> 3 %
Rubefacient when applied vigorously
ingestion may lead to serious adverse reaction: seizures, delirum, coma, dealth
Avoid use in children
Menthol
MOA
• Counterirritant at concentrations > 1.25%
• Activates TRPM8 receptor to trigger a cold sensation, followed by warmth
• Acts as a permeability enhancer when administered with other topical agents
• Caution – menthol hypersensitivity
• Discontinue if irritation, rash, burning, stinging, swelling, or infection occurs
Topical products general counseling
• Immediately discontinue and seek medical attention if pain, swelling, blistering of the skin occurs after application
• Do not bandage the area tightly where the product has been applied
• Do not use heat where the product has been applied
• Do not apply to wounded, damaged, broken, or irritated skin
• Do not allow these medications to come in contact with eyes, inside the nose or mouth, or with genitals