independent subjective refraction
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
give 2 scenarios when we have to refine BVS without a retinoscopy starting point/why would we not be able to do retinoscopy?
- Dense cataract – media opacified – difficult to do ret
- Keratoconus – change in shape of cornea – reflexes are hard to determine – scissor reflexes – difficult to do retinoscopy
if we have a px who we cannot do ret on - what can we do instead (2)
- Can use their old glasses and previous history
- However some patients will not have their previous glasses/any previous history (new customer)
explain how we first get an idea of the px’s rx in refining BVS without a ret starting point (4)
•Occlude the left eye.
•Measure the unaided vision (V) – if myopic test their near vision with a reading vision
•If possible, estimate the ametropia.
•This is particularly helpful in the case of uncorrected myopia. Also in myopia, the position of the true far point can be used to estimate the refractive error e.g. a person with −8.00 D myopia sees clearly if a target is placed at approximately 12.5 cm from the eye.
explain the use of a pinhole in refining BVS without a ret starting point (4)
Pinholes: occluder with a small hole in it – this reduces the blur circle/abberrations – generally improves vision with the pinhole – use if the patient has uncorrected refractive error
If vision is around 6/24 – first thing to do is add the pinhole to see if this will improve their vision
If it does – probably uncorrected cylindrical error – around 2D
If pinhole makes no difference or makes vision worse/causes blur – likely to be pathology (at the back of the eye) that is causing problems with vision
once we have an idea of px’s rx - explain the steps in refining BVS without a ret starting point (7)
•Add a +1.00 D sphere - if emmetropic/myopic = should blur them // If it doesn’t they are either hypermetropic or have uncorrected error
•Is the vision worse?:
•No: add more plus spherical power until the vision blurs. From the blur point, reduce by +0.25 DS. The BVS should be the maximum plus that the eye can tolerate without causing blur on a letter chart.
•Yes: add minus spherical power until the best line can be resolved. Make sure that each addition actually increases VA and does not just make the letters smaller.
•If possible, adjust the final sphere on the letter chart and/or the duochrome (s using a ±0.25 DS
•Record the VA.
•Occlude the right eye and repeat the procedure for the left eye.
what do we do for px’s who have a poor VA (5)
Patients with poor VA - may have difficulty in determining small changes in lens power and clarity
often necessary to make large power changes – BIG STEPS - A bracketing technique can be employed, e.g. use a +2.00 DS trial lens and compare this with a −2.00 DS trial lens
If the patient is able to differentiate between the two, the lens giving the better vision can be added and the technique repeated using, say, a +1.00 DS and a −1.00 DS lens, etc
may be necessary to refract the patient with the chart placed at 3 m or less. If this is done the result is over-plussed (the chart at 3 m acts as a near object and therefore adds a vergence of about −0.30 D in the plane of the trial lens) and a correction should be made
use of a pinhole disc is essential when vision is poor, in order to attempt to differentiate a refractive error from active pathology
when do we use duo-chrome/when do we NOT use it (2)
• Only monocular – cannot do binocularly
• Only use duo chrome if the VA is at least 6/12 or better – no value doing it otherwise
explain how we use duo-chrome for sphere refinement (3)
• +0.25/−0.25 spheres are used, usually mounted on a handle
• If they say the targets are equal: add +0.25 DS – then the targets on red should now be clearer
• If they say targets equal: add −0.25 DS – then the targets on green should now be clearer
what methods can we use to help us identify astigmatism (3)
stenopeic slit - identify astigmatic axis
fan and block
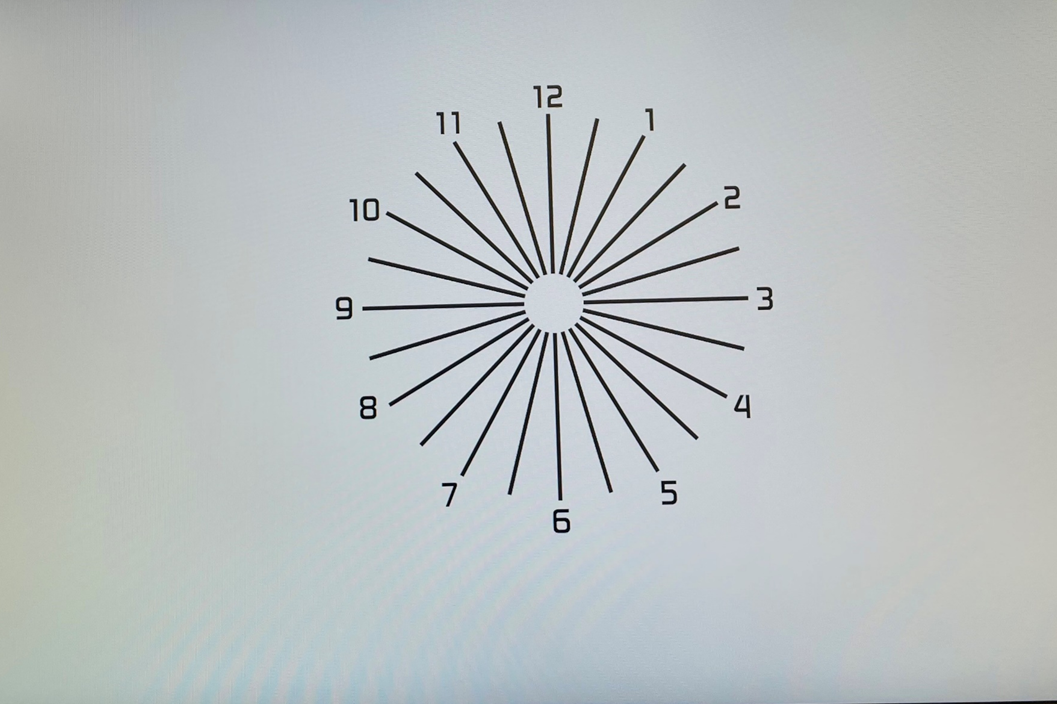
clock technique (elite chart)
explain how the stenopeic slit allows us to identify the astigmatic axis (4)
• Stenopeic slit: A narrow (1–2 mm) slit in an occluder; used in trial frames.
• Functions like an elongated pinhole, allowing only a narrow band of light through.
• Helps identify astigmatic axis by aligning with the meridian of clearest vision.
• Useful for isolating and refining cylindrical correction - helpful to use during JCC when the patient cannot identify between the 2 lenses – when you cannot get the axis in JCC
explain how we actually use the stenopeic slit in practice (5)
• Patient wears trial frames with stenopeic slit over the test eye.
• Occlude the other eye !!!
• Display 6/18 or 6/24 Snellen line.
• Patient’s role: Rotate the stenopeic slit using the trial frame knob and stop when image appears sharpest.
• Slit aligns with one principal meridian → Astigmatic axis - the other meridian is at 90° to the first
when would we use the fan and block technique (2)
- Useful when JCC isn’t working (going round in circles)
- Useful when working with LARGE cylindrical powers – high level of astigmatism
explain how we perform the FAN aspect of the fan and block technique (5)
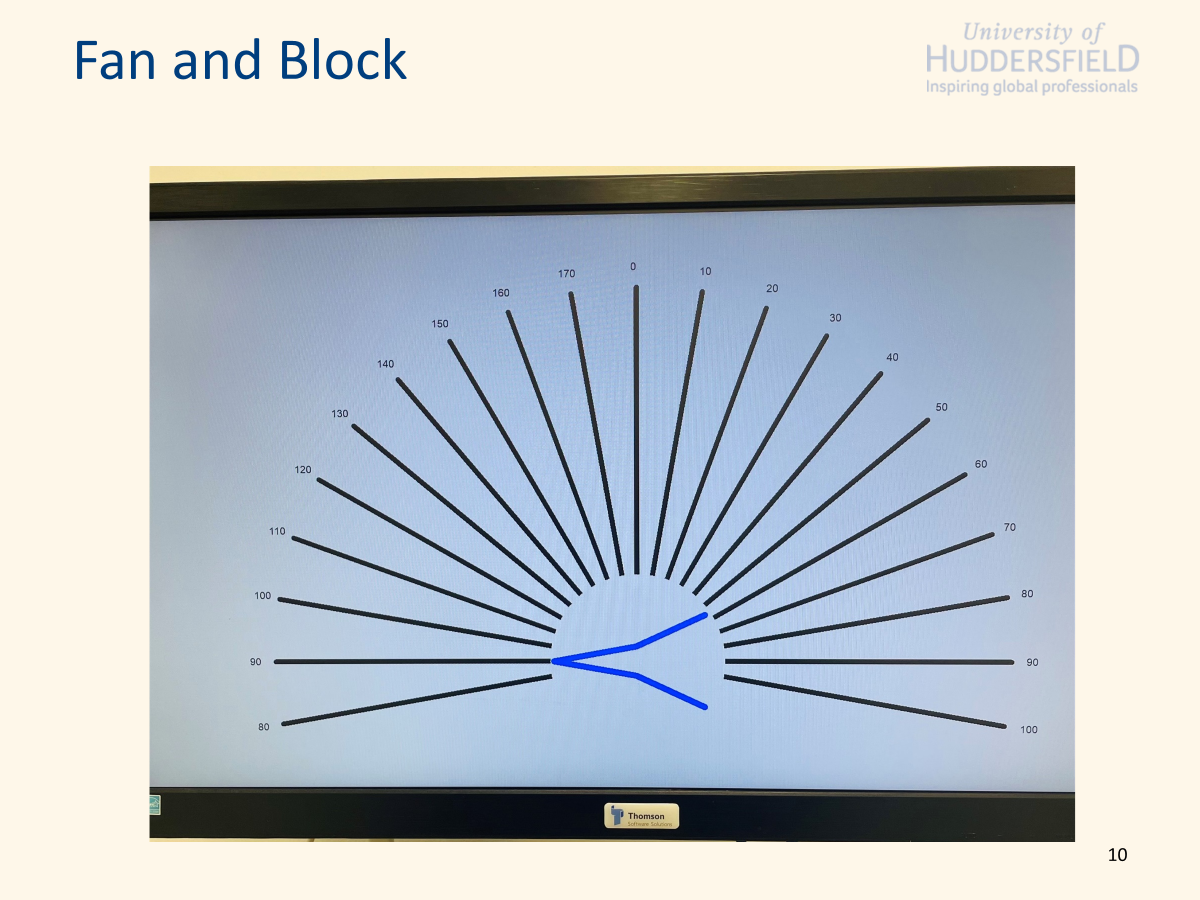
start with BVS in place
add fogging lens to slightly blur the image and prevent an over-minus response (+0.75) - this does depends on the cyl size- so if the patient has estimated 1D of cyl then +0.50DS should suffice
Display the fan dial chart at 6 metres (or appropriate distance).
fan - ask px which line/group of lines is clearest/darkest- add -0.25 DC at that axis
remember - whatever degrees they say that the line is clearer in – it’s actually 180 degrees perpendicular to that !!! – so if they say its clearer at 65 degrees – it is actually 115 degrees then we need to minus 90 degrees – so we will actually place the lens at 25 degrees !!! – confusing but remember – some charts will tell you where to place it in trial frame
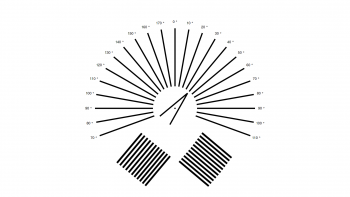
explain how we perform the BLOCK aspect of the fan and block technique (7)
show blocks to px with the trial cyl at the axis you just found
ask the px - do any of these lines look darker/clearer than others
add minus (-0.25) until the blocks are clear
If the lines all look equally blurred or equally clear → power is correct.
If increasing minus makes all lines worse, reduce back (too much cyl)
remember - After each change in cylinder, apply spherical compensation to maintain the circle of least confusion. This is done by adding +0.25 DS for every −0.50 DC added.
then do JCC properly to refine it
explain how we use the clock face method/elite bay chart to refine/detect astigmatism (5)
start with BVS in place and fogging lens (+0.75)
show px the clock chart
ask px which lines clearer
pick the lower number from the line they said and x 30 to determine axis - so 4×30=120 - so we would place the lens at 120
perform JCC as normal - take fogging lens out