Module 10 - Transposition of the Great Arteries
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
__-TGA means the ventricles are in the normal position and __-TGA means the ventricles are switched in position.
D-TGA - normal position
L-TGA - switched in position
Describe D-TGA with complete transposition of the great arteries.
Concordant AV connections
RA→RV
LA→LV
Discordant VA connections
RV→Ao
LV→MPA
In d-TGA with complete transposition of the great arteries, there are two completely separate circuits. How is oxygenated blood brought to systemic circulation?
ASD has L→R flow.
Oxygenated blood to the right heart.
A patient with d-TGA and complete transposition of the great arteries has a VSD. Is this patient cyanotic?
RV>LV pressure → deoxygenated blood to lungs
Patient is cyanotic.
A patient with d-TGA and complete transposition of the great arteries has a PDA. Is this patient cyanotic?
Ao>PA pressure → deoxygenated blood to left heart and lungs
Patient is cyanotic.
A patient with d-TGA and complete transposition of the great arteries has an ASD. Is this patient cyanotic?
LA>RA pressure → oxygenated blood to right heart and systemic circulation.
Patient is less cyanotic.
Your patient has d-TGA with complete transposition of the great arteries. Describe the appearance of PSSAX.
Aortic valve is anterior and rightward of the PV because the Ao comes off the RV.
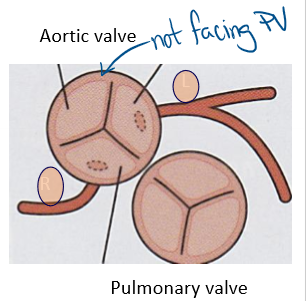

Describe the findings of this image.
PSSAX with the aorta anterior and rightward of the PV.
Indicates complete transposition of the great arteries.
Don’t know if d-TGA or l-TGA.
Describe how the RV and LV can be differentiated on echo.
TV more apically displaced (A4C)
LV has papillary muscles (PSSAX)
RV has prominent trabeculations and moderator band
Describe the treatment for d-TGA.
Prostaglandins to keep the PDA open
Rashkind procedure
Jatene, Mustard-Stennings, or Rastelli repair
When would a Rashkind procedure be used? Describe the process.
Used on d-TGA with small or no ASD.
catheter inserted through PFO
balloon dilated in LA
balloon pulled into RA to create ASD
Describe the Jatene procedure.
Arterial switch the great arteries to their correct ventricle.
MPA → AV root
Ao → PV root
Slice of Ao at the CAs is removed and stitched onto the neo-aorta
Branch PAs are brought anterior to the ascending aorta.
What are some complications from the Jatene repair that should be recorded on post-op echo?
Supravalvular AS and PS from suture lines
Branch PA stenosis
AI/PI
Coronary artery flow
Associated defects repaired (ASD, VSD, PDA)
Describe the LeCompte maneuver.
LPA and RPA both anterior to the ascending aorta.
Describe the Mustard-Stennings repair.
Atrial switch.
IAS removed
Interatrial baffle to redirect systemic VR to the left heart (which is connected to the MPA)
Redirect pulmonary VR to the right heart
List some common complications for a Mustard-Stennings repair.
RV dysfunction from RVPO
Systemic TR
Obstruction or leak in baffle
Sinus node dysfunction (RA dilation)
How is SPAP assessed in a patient with a Jatene repair?
RVSP = RAP + 4(TR)2
Lungs connected to right heart.
How is SPAP assessed in a patient with a Mustard-Stennings repair?
RVSP = LAP + 4(MR)2
Lungs connected to left heart.
A patient with d-TGA has PS. What repair would be recommended?
Don’t want to do an arterial or atrial switch because one valve will be stenotic→ use Rastelli repair
VSD patch to redirect LVOT to Ao
Remove PV and insert RV-PA conduit
Describe the anatomy of L-TGA.
AV and VA discordance but hemodynamically correct.
RA→ LV → PA
LA → RV → Ao
Great arteries do not cross.
Ao is anterior and left of PA.
Ventricles are side by side (not anterior/posterior).
Coronary arteries are commonly inverted.
List some common associated findings with L-TGA.
Ebsteinoid TV
VSD, PS
Conduction disturbances
Right ventricle failure
In PSSAX, the ventricles are side by side. This is diagnostic of…
L-TGA

Describe the findings of this image.
Aorta anterior and leftward of the PA.
L-TGA
Describe the treatment for l-TGA.
None required until the RV starts to fail.
When RV starts to fail:
Replace TV
Pacemaker for heart block
Heart transplant when severe RV dysfunction
OR double switch surgery.
Describe the double switch procedure.
Arterial and atrial switch.
Narrow MPA to prepare LV for high pressures
After a few years, Jatene and Mustard-Stenning repair done
A 5 year old patient with l-TGA, mild TR (4m/s), mild MR (2m/s), and BP 100/60mmHg. Calculate SPAP.
LV is connected to MPA → use MR
LVSP = SPAP if no LVOTO
LSVP = 4v2 + RAP
LVSP = 4(2)2 + 5mmHg
LVSP = 21mmHg