Static lung volumes
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
10 Terms
What determines FRC and how does that change w/ age?
FRC:
Determined by interaction between ribcage flexibility and lung elasticity
Ribcage always want to EXPAND (due to tension in costal cartilage)
Lungs always want to COLLAPSE (b/c they are elastic and stretched in the thorax)
FRC is determined by the balance of these two forces
As We Age:
lung elastic recoil lessens → FRC rises
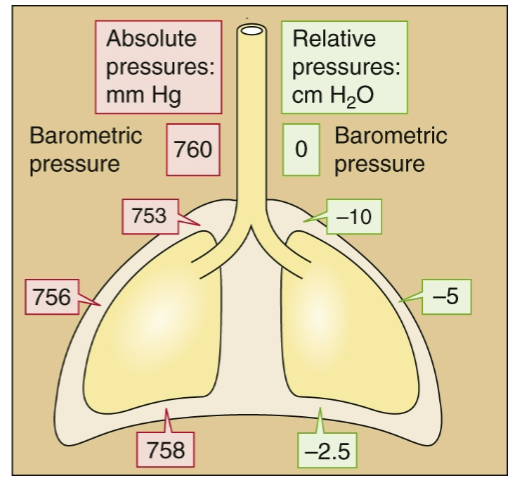
Desribe the absolute and relative pressures present in the thoracic cavity
Describe the muscles of:
Inspiration
Expiration
Inspiration:
Diaphragm
Scalenes
Lifts R1,R2
Sternocleidomastoid
Lift sternum upward and outward
External Intercostals
Fiber direction: Down and forward (hands in pockets)
Elevate ribs
Neck and back musculature
Posture allows better lung inflation
Bronchial smooth muscle
Bronchodilation reduces airway resistance
Expiration:
Abdominal muscles: increase abdominal cavity pressure
Internal/external obliques
Rectus abdominus
Transverse abdominus
Internal intercostals
Fiber direction: Down and back
Depress ribs
Neck and back musculature
Postural Changes
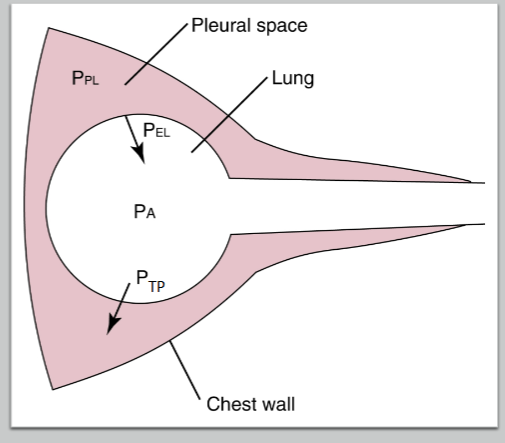
Describe the importance of PTP in lung-chest wall interactions
What happens in Pneumothorax?
What happens as lung volume rises?
A positive Transpulmonary Pressure (PTP) is necessary to maintain lung volume:
PTP = PA – PPL
Alveoli naturally wants to collapse due to Elastic Forces (PEL)
Alveoli stays open b/c lung is adhered to chest wall via the negative pressure in Pleural Space
As long as PTP is positive, lung stays open
Pneumothorax:
air enters the pleural space → pressure becomes equal to atmospheric and the lung → PTP = 0 → Lungs collapse
Lung Volume:
When Lung volumes rise, PTP must rise as PEL increases as the lung is stretched further
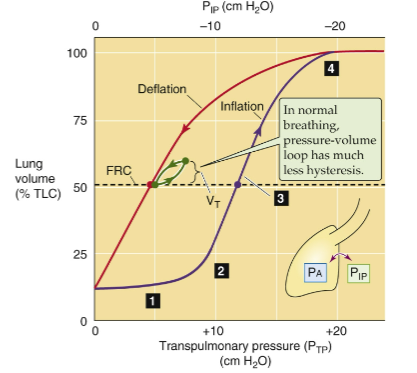
Draw out the PV graph depicting Transpulmonary Pressure, Intrapleural Pressure, and Lung Volume (TLC)
Why do we breath from FRC?
FRC:
We breath from here b/c this makes expiration at rest is passive
Due to elastic recoil
Minimizes the work of breathing
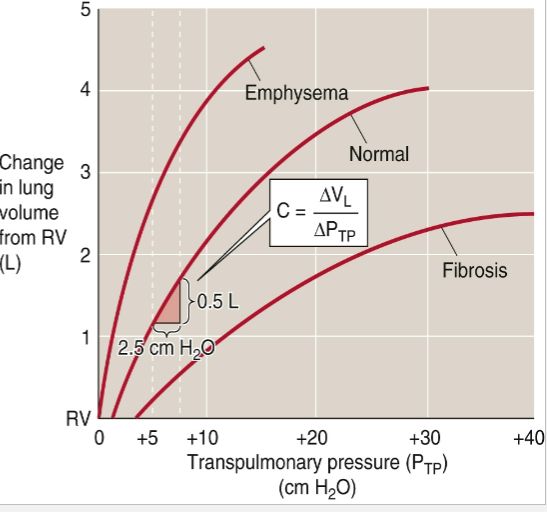
Draw out the graph depicting compliance of Normal, Emphysema, and Fibrosis. Describe why the lines are shaped that way
Emphysema:
Increased compliance
Destruction of elastic tissue
Fibrosis:
Reduced compliance
Increased deposition of fibrous tissue
What is Hysteresis?
Describe the mechanism that causes hysteresis
Hysteresis: difference between the inspiratory pressure-volume curve and the expiratory due to inspiration being “harder” to do then expiration
Mechanism:
Inspiration:
changes in surface tension*
overcoming the elastic recoil
Expiration:
Elastic nature of the lung → work done on the lung during inspiration is partially “given back” during expiration
*= the attraction of water molecules to one another
What does Surfactant do?
How?
Importance?
How is it produced?
What is the effect of lung volume on surface tension?
Surfactant reduces surface tension:
By replacing water molecules at the air-liquid interface
Mechanism:
surfactant molecules have hydrophobic tails → Pulls it towards surface → Reduces attraction of water molecules from one another @ surface
Importance:
allows work of breathing to be minimized
Production:
produced in type II pneumocytes in ER
Stored in lamellar bodies
Exocytose and “spread” into alveolar surface
Tubular myelin = reservoir for surfactant and helps to spread surfactant rapidly
Lung Volume on Surface Tension:
Inspiration → Alveoli Inflates → increases distance between surfactant molecules → Surface Tension Rises → puts a brake on inspiration (as well as elastic recoil)
Expiration → Vice Versa
Thus: surfactant also helps the alveoli maintain a uniform size
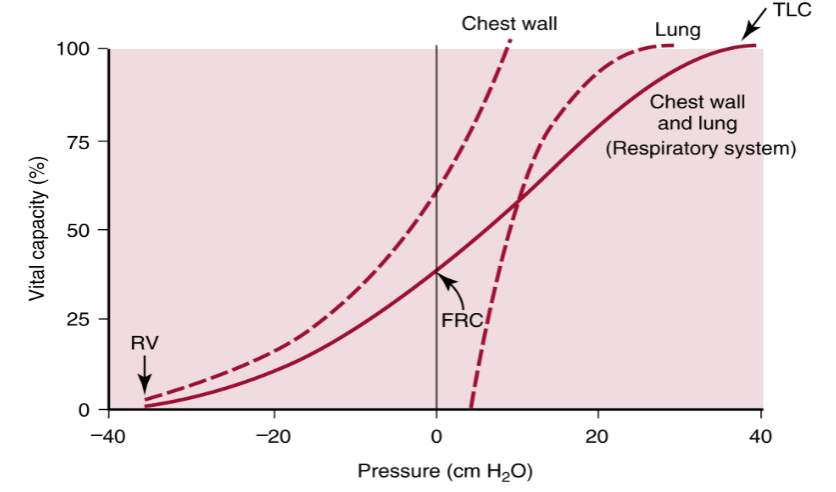
Draw out the graph depicting Compliance of Chest Wall and Lung as a function of Pressure Vs Volume (Vital Capacity)
Describe the three curves
Where is FRC on this graph?
What must happen if we go above/below FRC
Chest Wall:
Wants to expand (aids inspiration); after a certain point, it wants to recoil inwards (aids expiration)
Lung:
always want to collapse to it’s minimal volume
will never get there as that point is w/in residual volume
Tendency of elastic recoil aids expiration
Solid Line = Combined chest wall and lung pressure volume curve
FRC:
volume at a Pressure of zero
balancing point between the tendency for the lung to collapse inward and the ribcage to expand outward
To go above FRC
We need to expand chest wall and lung, so PTP becomes more positive
To go below FRC
PTP becomes less positive
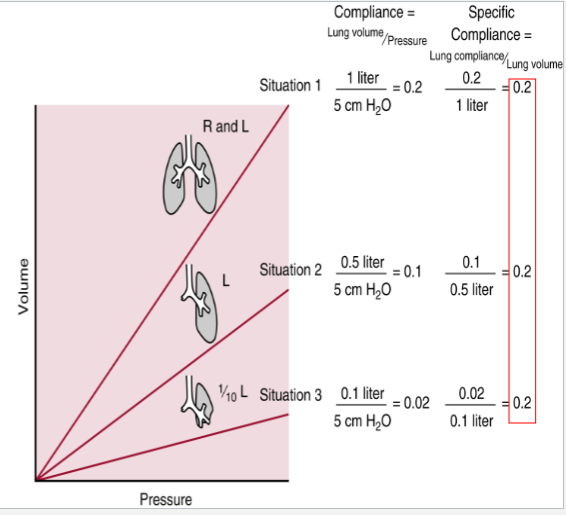
What is specific Compliance?
Why is this important
Compliance = Lung Volume/Pressure
Specific Compliance = Lung Compliance/Lung volume
Why is this important:
For people w/ less lung volume (due to disease, surgery, etc), it appears that compliance decreases as lung volume decreases; This shouldn’t happen as compliance is an intrinsic property of the lung’s tissue, not dependent on size
The fall in “regular” compliance is due to the fact that the smaller lungs are always closer to TLC as they have to use a lot more of their available volume to perform the duties of the lung
Specific Compliance fixes this; Once we apply the appropiate volume, it turns out that everybody has the same value of Specific Compliance.