Mesenteric vessels USA and Eval
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
Indications for mesenteric study
Post-prandial pain
Abdominal bruit
Recent weight loss
Fear of food/eating
Diarrhea
N/V
Celiac Axis
Anterior branch of the aorta
Originates from the aorta within the first 2cm below the diaphragm
Normally 1-3cm in lengt
Superior to body of pancreas
Celiac branches
CHA, Left gastric A, Splenic A
In some patients the celiac artery and SMA may share a
Common trunk
Celiac Doppler
Low resistance waveform because it feeds organs requiring constant flow
Pattern does NOT change after eating
Normal PSV → <200cm/s
Abnormal PSV → >200cm/s (70-99% stenosis)
Abnormal EDV → >55cm/s (>50% stenosis)
Celiac occlusion leads to retrograde flow in the ________________ to supply blood to the CHA
Gastroduodenal artery
____ may also demonstrate retrograde flow in a celiac occlusion to send blood back to the spleen
CHA
Left gastric artery
Smallest branch of CA
Travels anterior and cephalad
Supplies the stomach and pylorus
Not usually seen sonographically due to coarse and structures supplies
Anatomy of the CHA
Right branch of the celiac axis
Supplies blood into the liver, GB and stomach
Branches into the proper hepatic artery which enters the liver and the GDA that supplies the pancreas and duodenum
Hepatic artery supplies 20-30% of blood to liver
Indications to scan the common hepatic artery
Chronic liver disease
Liver transplant
Trauma
Anatomic variant of CHA
Hepatic artery originates from SMA
Hepatic artery originates from aorta
CHA is best visualized in what plane
Trans
Doppler of Hepatic artery
Low resistance
Flow velocities increases with cirrhosis, mets, lymphoma
RI >0.78 = Portal HTN
Splenic artery anatomy
Largest branch of celiac
Tortuous course posterior to the body of the pancreas
MOST tortuous artery in body
Supplies blood to the spleen, pancreas, and fundus of stomach
MOST COMMON SITE FOR VISCERAL ANEURYSM
US of splenic artery
Origin and proximal portion best visualized in transverse
Distal segment best evaluated through the splenic hilum from left lateral window
Travels posterior and superior to the pancreas body/tail
Doppler of splenic artery
Low resistance
Tortuous, may normally find areas of high PSV
SMA anatomy
Anterior branch of AO that originates about 1-2cm below the celiac axis
Runs parallel to aorta posterior to body of pancreas
Supplies blood to jejunum, ileum, cecum, ascending colon, proximal 2/3 trans colon
Communicates with celiac artery via pancreaticoduodenal arcade
Terminates near ileocecal valve
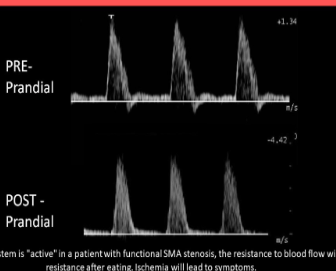
US and Doppler of SMA:
Pre-Prandial: High resistance flow with minimal flow in late diastole; peaked waveform
Post-prandial: Low resistance flow with continuous flow in diastole and more rounded waveform
No resistance change if stenosis present
PSV can also increase normally after eating
IMA
3-4cm above the aortic bifurcation, on the left anterolateral aspect of the aorta and courses inferiorly to the left
IMA provides blood supply to distal colon and proximal rectuM
Provide potential for collateral flow
Can be located in trans inferior to renal arteries
IMA Doppler
High resistance with minimal later diastolic flow
If IMA is EASILY identified on ultrasound, SMA stenosis or occlusion should be suspected
IMA dilutes due to compensatory flow related to an SMA stenosis
Mesenteric ischemia
Patient experiences reproducible pain after eating due to bowel ischemia caused by stenosis
Post-prandial evaluation should be performed 20-30mins after meal
Abnormal SMA and IMA post-prandial flow = High resistance/no change
Diagnosed with stenosis/occlusion of TWO OR MORE of the 3 major arteries
Collateral pathways that can form with mesenteric ischemia
Pancreaticoduodenal arcade (MOST COMMON)
Arc of Riolan
Marginal artery of Drummond
Mesenteric PSV/Aortic PSV Ratio is usually:
1.0
Abnormal Mesenteric PSV/Aorta PSV ratio =
>3.0
Abormal SMA Doppler
PSV >275cm/s = 70% stenosis
EDV >45cm/s = 50% stenosis
Abnormal IMA Doppler
PSV >200cm/s = stenosis
EDV >25cm/s = stenosis
If flow in the SMA and IMA is low resistance with increased diastolic flow even in a fasting patient =
Capillary beds are constantly vasodilated due to ischemia
Compensatory flow can sometimes mimic___________
Stenosis
Compensatory flow = increased _______ and spectral window
Velocity
Treatment for mesenteric ischemia
Angioplasty, stent, bypass graft
SMA Stenosis
Median arcuate ligament syndrome
Can be mistaken for celiac stenosis with mesenteric stenosis
Intermittent extrinsic compression of the celiac axis
Caused by diaphragm moving superiorly and the median arcuate ligament pinching the celiac axis
Rarely causes symptoms, but may see pain with expiration
USA Median arcuate ligament syndrome
Intermittent increased PSV in celiac axis with respiration maneuvers
SMA syndrome is also known as
Wilkie syndrome
SMA syndrome
Acute angulation of SMA causes compression and obstruction of the third part of the duodenum
An angle less than 22 degrees indicates compression is likely
Measurement of the aortomesenteric angle can demonstrate the risk of compression syndromes
Requires surgical intervention
If a patient suffers from severe weight loss, the latty tissue around the SMA is diminished, causing …
Acute angulation and reduction in distance between the aorta and superior mesenteric artery
Symptoms of SMA syndrome
Early satiety, recurrent episodes of abdominal pain, vomiting
What artery is visualized coursing anterior to the main portal vein
Common hepatic artery
What is the difference between a waveform from a stenotic vessel and one from a vessel with compensatory flow?
A spectral window is present with compensatory flow, but not with stenosis
What causes stenosis in median arcuate ligament syndrome
Compression
The aortomesenteric angle is used to predict the risk of:
Compression