Physiology Unit 3
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
Intercalated Discs
interdigitating folds between cells; mechanical junction (desmosomes) + electrical junctions (gap junctions) = syncytium
gap junctions allow for low resistance 1/400 pathway for electrical signal to spread cell-to-cell
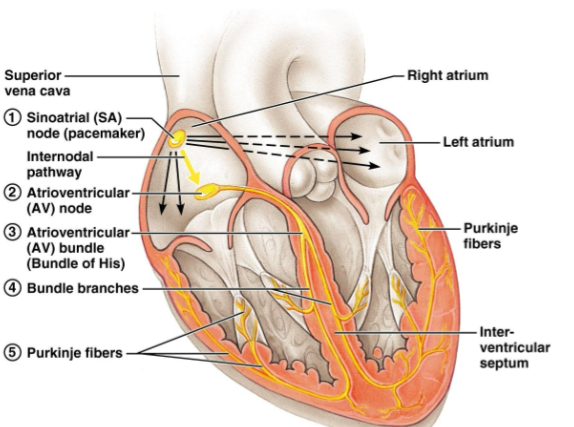
Specialized Cells
“leading”
low contractility, no stable RMP = reach TH sans neuronal stimulus
located in: SA node, internodal bundles, AV node, bundle of His, bundle branches + purkinje fibers
Contractile Cells
“following”
Capillaries
greatest total cross-sectional area (6000cm2) so blood flow velocity is slowest + most efficient
Veins
type of vessel where BP is lowest
Arterioles
vessel where BP will drop the most
Cardiac Output
HR x SV (mL/min)
proportional relationship to stroke volume and heart rate (SV + HR)
inverse relationship to total peripheral resistance (TPR)
Total Peripheral Resistance TPR
force the heart must overcome to push blood thru systemic circulation; main sources are vessel diameter, blood viscosity + vessel length
inversely proportional to cardiac output CO
Laminar Flow
blood cells in the center of a vessel flow faster; silent
Pulse Pressure
systolic - diastolic
Poiseuille’s Law
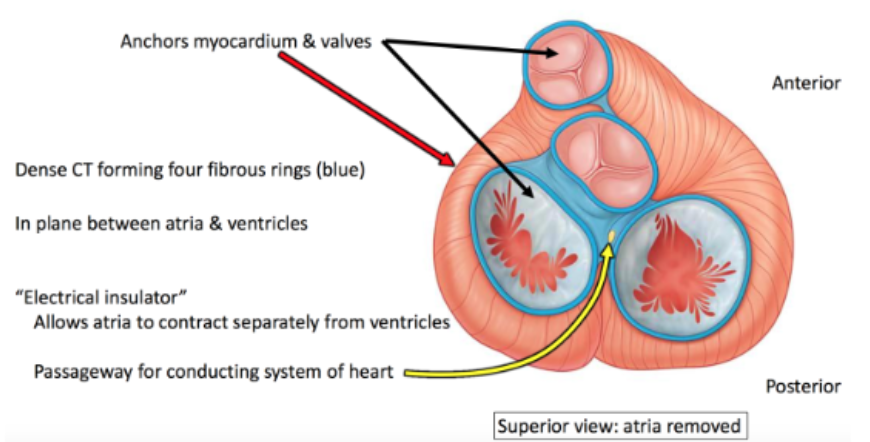
Fibrous Insulator
collagenous skeleton; rigid framework for dense regular connective tissue between atria and ventricles
gives delay + produces sequential events — allows time for electrical signal to spread thru atria for contraction, then for signal to spread thru ventricles for contraction
Sarcomeres
striated actin and myosin filaments
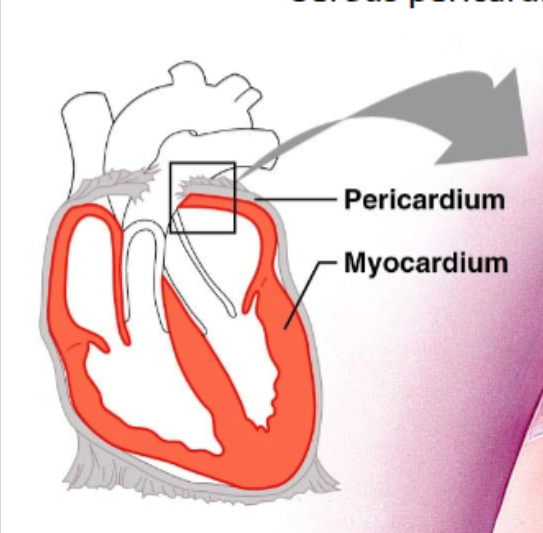
Pericardium
fibrous + serous sac surrounding heart, cushions / prevents friction b/c fluid
fibrous pericardium - outer, tough, dense connective tissue
pericardial cavity filled w/ fluid
serous pericardium - inner, thin, double layer
Parietal Surface
lines inner surface of parietal pericardium; attached to diaphragm and base of heart
Visceral Surface
surrounds heart surface (epicardium)
External Epicardium
first heart wall layer, visceral pericardial layer
Myocardium
middle heart wall layer, cardiac muscle tissue
Endocardium
innermost heart wall layer; simple squamous epithelium, covers internal surfaces of the heart / external surface of heart valves
Chordae Tendineae
“heart strings", collagen fibers attached to lower surfaces of AV valve cusps; prevent valve cusps from flipping into atria during ventricular contraction
Papillary Muscles
muscular ridges anchoring chordae tendineae
Right Atria
auricle, smooth wall (posterior), pectinate muscles (ridges), crista terminalis (muscular ridge), fossa ovalis, coronary sinus, IVS, SVC openings, right AV valve
Left Atria
auricle, mostly smooth wall, pectinate muscle (anterior), left AV valve (chordae tendineae)
Lub
(S1) closing of AV valves
Dub
(S2) closing of semilunar valves
Fossa Ovalis
fetal = foramen ovale (small valve on left side closes d/t higher BP on left atrium side)
hole in atrial septum, most blood goes thru here; right → left shunt in systemic circuit
Ligamentum Venosum
fetal = ductus venosus (closes d/t increased pressure in portal vein forcing blood flow thru liver sinuses)
shunt: blood bypasses liver to heart
Ligamentum Arteriosum
fetal = ductus arteriosus (closes d/t oxygen change after umbilical cord removed, vessel constricts and closes)
pulmonary artery to aorta shunt; right → left shunt to systemic circuit
PDA Patent Ductus Arteriosus
ductus arteriosus fails to close after birth = blood repeatedly flows back to lungs
net CO decreases so blood volume increases to compensate (high EPO); L+R ventricular hypertrophy, murmur thru systole + diastole
cyanosis of left skull + upper limb
Tetralogy of Fallot
4 heart defects —
pulmonary valve stenosis = decreased outflow to lungs
R ventricular hypertrophy = pumping lotta blood
ventricular septal defect
aorta displaced over ventricular septum
septal defect d/t right → left shunt, most blood bypasses lungs = majority aortic blood is deoxygenated
AV Nodal Delay
Specialized Fibers
Contractile Fibers
SA SinoAtrial Node
first to depolarize, no stable RMP (never at rest)
leaky Na+ channels open as soon as depolarize → repolarize → open Na+ → rise to threshold
dont’t need voltage, strategically open sodium channels
70-80 depol/min → steepest potential (highest intrinsic rythym)
ANS innervation most dense
Purkinje Fibers
fast conduction d/t many gap junctions at intercalated discs
15-30 depol/minute → more gradual prepotentials
Prepotential
AKA pacemaker potential, unique to hear cells, generate own AP without stimulus
AV AtrioVentricular Node
delays depolarization b/c cells smaller in diameter, more resistance, slower movement of electrical signal to bundle branches
40-60 depol/min
Chronotropy
decreased by parasympathetic: Ca++, Na+, K+
increased by sympathetic: Ca++, Na+, K+
Inotropy
force / strength of contraction, muscle fiber tension development
sympathetic (NE) division affects in all fibers (specialized + contractile), parasympathetic has little affect
Baroreceptor Reflux
detect stretch in aorta + carotid body, too much =
high BP → high frequency AP down sensory neurons to medulla oblongata → integration center for cardioinhibotory center → vagus nerve to effector SA node of heart → mAChR
low BP → low frequency AP to cardioaccelatory center →parasympathetic nerve fibers → (nor)epinephrine increases rate of depolarization
Absolute Refractory Period
very long in heart cells to prevent summation + tetany; cardiac contractile cell begins relaxation
Latent Period
need Ca++ out of sarcoplasmic reticulum first, contraction happens after
very short in cardiac cell, allows muscle to start contracting during AP
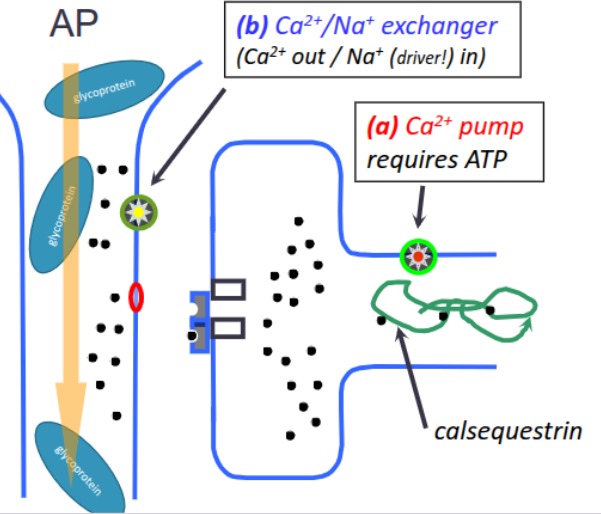
SKELETAL MUSCLE Excitation Contraction Coupling
AP moves along T-tubule,
voltage change senses by Na+VCG,
signal communicated to VOCC, contraction occurs,
calcium pumped back into sarcoplasmic reticulum,
Ca++ binds to calsequestrin to facilitate storage,
contraction terminated
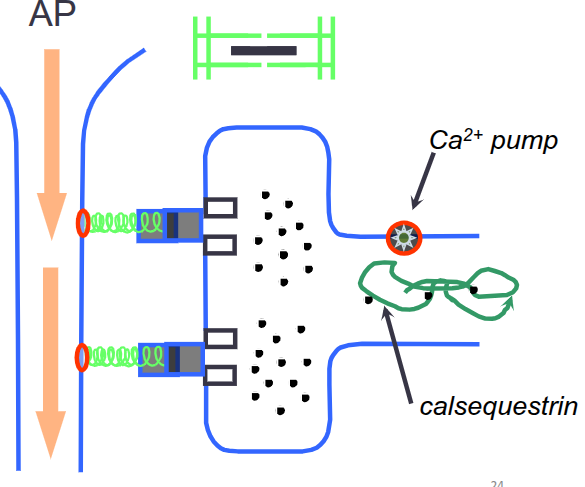
CONTRACTILE CARDIOCYTE Excitation Contraction Coupling
AP moves along large T-tubule
EDV
ESV
Preload
degree of muscle tension when it begins to contract
frank-starling principle: more in, more out
Afterload
contractile force needed for ejection; affected by peripheral vasculature
Contractility of Ventricle
availability of calcium, positive and negative intropoy (rare)
Diastis