A&P ii Unit 4: The Respiratory System
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
Distinguish between external respiration, internal respiration, and cellular respiration.
external respiration – exchanges between air and blood in the lungs
internal respiration – exchanges between blood and tissues
cellular respiration – different use of the term; processes used to extract energy from nutrients and store in the form of ATP (O2 required) (CO2 offloaded)
Describe the general functions of the respiratory system.
air passageway – from the external environment to the alveoli (air sacs of the lungs)
site for exchange of oxygen and carbon dioxide – Very thin barrier between pulmonary capillaries and air in alveoli allows gas exchanges by diffusion: (O2 moves from air to blood / CO2 moves from blood to air)
detection of odors – Olfactory sensory receptors in superior nasal cavity
sound production – Vocal Cords in larynx vibrate as air moves past to produce voice sounds
List the structures of the upper respiratory tract and lower respiratory tract.
Upper Respiratory Tract – nose, nasal cavity, pharynx
Lower Respiratory Tract – larynx, trachea, bronchi, bronchioles, alveolar ducts, and alveoli
Conducting Zone – parts that transport air (nose to ends of terminal bronchioles)
Respiratory Zone – respiratory bronchioles, alveolar ducts, and alveoli (where gas exchange occurs)
Describe the features of the respiratory mucosa, including the function of the cilia.
respiratory passageways lined with a mucosal membrane, ciliated epithelial lining in most locations
•mucosa becomes thinner progressively from nasal cavity to the alveoli (pseudostratified ciliated columnar epithelium in most places from nasal cavity down to lobar (secondary) bronchi — beyond secondary bronchi, the mucosa becomes thinner and is a simple squamous epithelium in the alveoli)
•cilia sweep particles away from lower respiratory tract.
•mucus and saliva trap particles and other substances.
Describe the features of the nose and nasal cavity, including their functions.
Nose – formed by paired nasal bones and cartilages
Nostrils (nares) – flared openings into the nasal cavity
Nasal Cavity – extends from the nostrils to the nasopharynx (openings to the nasopharynx are called choanae) (floor is formed by the hard and soft palates)
Nasal septum – thin, bony wall that divides left and right sides
Nasal Conchae – Superior, Middle, and Inferior along lateral walls of cavity (Provide turbulence to air — Nasal meatuses are air passage “valleys” between the conchae — Turbulence helps warm inhaled air)
Respiratory Region – air passageway
Olfactory Region – Sensory receptors present to detect odors
Functions- air is warmed and humidified; mucus traps dust, microorganisms; cilia sweep mucus and particles to pharynx for swallowing
Describe the features of the paranasal sinuses and their connections to the nasal cavity.
paranasal sinuses- spaces within skull bones, connected to the nasal cavity by ducts, lined with ciliated mucosal membrane continuous with lining of nasal cavity
•Mucus traps inhaled particles, and cilia sweep out to nasal cavity
Sinus infections – can occur if mucosal membranes become inflamed and mucus drainage decreases
Sinus headaches – occur because of increased pressure due to mucosa swelling or pressure changes
Describe the locations of the different parts of the pharynx.
Air is conducted along entire path; food and liquids in lower portions
Nasopharynx – passage for air from nasal cavity to oropharynx (Uvula portion of soft palate elevates during swallowing to prevent entry of food/liquids — Has paired openings into auditory tubes (eustachian tubes) that lead to middle ear)
•Allows equalization of pressure along tympanic membrane — Microorganisms can enter and cause infections — Single pharyngeal tonsil along posterior wall
Oropharynx – Middle part of the pharynx; posterior to the oral cavity (Level of the soft palate to the hyoid bone — Paired palatine tonsils on lateral walls — Lingual tonsils at the base of the tongue)
Laryngopharynx – Most inferior part of the pharynx; connects pharynx to larynx and esophagus
Both of these parts of the pharynx are lined with a thicker stratified squamous epithelium for protection from abrasive foods.
Explain the basic functions of the larynx and epiglottis.
First compartment of the lower respiratory tract; connects laryngopharynx to the trachea
Larynx Functions:
•Air passageway
•Epiglottis prevents ingested food/liquids from entering lower respiratory tract
•Produces speech sounds
•Closure of epiglottis assists with Valsalva maneuver of increasing abdominal pressure by preventing air escape from lungs.
•Participates in sneeze and cough reflexes
Distinguish between the functions of the vocal folds and vestibular folds.
Vocal folds – vocal ligaments covered by a mucosal membrane (True vocal cords)
Rima glottidis – opening between the vocal folds
Glottis – Vocal folds plus the opening in between
Vestibular folds (false vocal cords) – Also mucosal membrane-covered ligaments that help protect the vocal folds, but no sound production
Define laryngitis, and describe the main symptoms and problems associated with the condition.
laryngitis = Inflammation of the larynx
•symptoms - hoarse voice, sore throat, sometimes fever
•caused by bacterial or viral infection, or overuse (yelling)
•severe cases can extend to the epiglottis
•may lead to sudden airway obstruction, especially in children
Describe the location and structure of the trachea, including the inner mucosal lining.
trachea = tube connecting the larynx with the two main (primary) bronchi, anterior to the esophagus.
Carina – projection of cartilage at base of trachea where it splits into the left and right main bronchi
Inner lining = pseudostratified ciliated columnar epithelium
•mucus production by Goblet cells in the lining and larger mucous glands in underlying connective tissues — mucus traps particles and microorganisms.
•cilia sweep trapped material up and away from the lower respiratory tract.
Distinguish between the different types of bronchi and bronchioles along the pathway of airflow.
•trachea delivers air to the left and right main (primary) bronchi (one leads to each lung)
•right main bronchus is more vertical, shorter and wider; more likely to trap large particles
•main bronchi lead to lobar (secondary) bronchi, one for each lung lobe (two lobes on the left and three on the right).
•lobar bronchi lead to segmental (tertiary) bronchi).
•segmental bronchi lead to smaller bronchi. smaller bronchi lead to small tubes with no cartilage in their walls called bronchioles. (less than 1 millimeter in diameter — capable of constriction and dilation and have proportionally thicker layer of smooth muscle in their walls).
•terminal bronchioles are the last tubes in the conducting pathway for air flow.
•terminal bronchioles lead to respiratory bronchioles, the first tubes of the respiratory zone
Define bronchoconstriction and bronchodilation; explain benefits or potential problems associated with them.
Bronchoconstriction – occurs when smooth muscle in walls of bronchial tree passages contracts
•limits air flow
•limits entry of dangerous substances
Bronchodilation – occurs when smooth muscle in bronchial tree passages relaxes
•Increases air flow, O2 intake, CO2 removal
Describe the pathway of air from the bronchioles to alveoli.
•terminal bronchioles lead to respiratory bronchioles, the first segments of the respiratory zone.
•respiratory bronchioles divide into thin alveolar ducts.
•alveolar ducts lead to alveolar sacs.
•alveolar sacs are clusters of alveoli, very small spherical structures where gas exchanges occur with the blood.
Describe the structure of an alveolus and the surrounding pulmonary capillaries.
•alveoli are clustered together in alveolar sacs.
•each alveolus is only 0.25 to 0.5 mm in diameter.
•each lung contains 300 to 400 million alveoli.
•wall of an alveolus is a very thin simple squamous epithelium.
•each alveolus is surrounded by pulmonary capillaries
List three types of cells found in alveoli, and describe the function of each.
Alveolar Wall – composed of two types of cells:
Alveolar Type I Cells – simple squamous epithelial cells that comprise most of the wall
Alveolar Type II Cells – secrete oily pulmonary surfactant:
•moist alveolar walls have a high surface tension because water molecules attract each other.
•surfactant reduces surface tension and prevents alveoli from collapsing.
Alveolar Macrophages – May be fixed or free macrophages (phagocytose microorganisms and particles) dust cells
Describe the structure of the respiratory membrane, and explain its purpose.
•the thin barrier between air inside an alveolus and blood inside a pulmonary capillary
•only 0.5 micrometer thick
•permits gas exchange between air and blood
•composed of type 1 alveolar cells and individual cells of capillary walls, plus the thin basement membranes between them
•so thin that O2 can diffuse from air into the blood passing through a pulmonary capillary, and CO2 can diffuse from blood into the air inside the alveolus.
Define asthma, and explain the problems associated with the condition.
•Chronic bronchoconstriction with excess pulmonary mucus production, coughing, wheezing, shortness of breath
•Affected people usually have developed a hypersensitivity to an inhaled agent and react with severe inflammation → bronchoconstriction.
•Can lead to permanently thickened respiratory passageway walls
•Can be exercised-induced due to inhaled air irritating respiratory mucosal linings → triggering inflammation
•Treated with inhaled steroids to reduce inflammation and bronchodilators (cortisone)
Define pneumonia, and explain how the condition interferes with respiration.
pneumonia - Infection of the lungs that leads to alveoli filling with fluid, exudate, or pus
•usually caused by bacteria or viruses spread by respiratory droplets (SARS-CoV-2 is the virus that causes COVID-19 — Infection in the lungs can lead to COVID-19 pneumonia).
•cough, fever, difficulty breathing, weakness, chills, chest pain, increased heart rate
•excess sputum production
•swelling of tissues and fluid accumulation interferes with gas exchanges; can be fatal.
Describe the location and general structure of the lungs.
•located within the thoracic cavity on either side of the mediastinum
•right lung is larger and wider; divided into three lobes
•left lung has two lobes
•lungs are protected by the rib cage
•the lobes are separated from each other by fissures.
•on the mediastinal surface of each lung, there is an indented region called the hilum.
•main bronchi, the pulmonary artery, the pulmonary veins, lymphatic vessels, and autonomic nerves pass through the opening at the hilum = root of the lung.
Compare and contrast the right lung versus the left lung.
•right lung is larger and wider; divided into three lobes
•left lung has two lobes
•the lobes are divided into bronchopulmonary segments (10 in the right lung and 8 to 10 in the left lung).
each segment functions as its own unit (served by its own segmental (tertiary) bronchus — served by its own branch of the pulmonary artery and a branch of a pulmonary vein)
•segments can be removed without affecting function of others.
Explain the differences between the pulmonary and bronchial circulations and their functions.
Pulmonary circulation (as studied in previous chapters) – transports blood from the heart to the lungs for gas exchange and then back to the heart
Bronchial circulation – Part of the systemic circulation
•brings oxygenated blood to the tissues of the lung
•small arteries and veins supply the walls of the bronchi and bronchioles
•alveoli receive oxygen directly from air inside them.
Describe the pleural membranes and pleural cavity.
Each lung and the adjacent internal thoracic wall is lined with a double serous membrane (pleural membrane).
•Inner layer – visceral pleura: contacts the surface of the lung
•Outer layer – parietal pleura: lines the wall of the pleural cavity
Pleural Cavity –space between the two layers of the pleural membrane, filled with pleural fluid
•this is a potential space when the lungs are inflated.
Explain the function of pleural/serous fluid in the pleural cavity.
Pleural fluid – oily and lubricates to reduce friction between lungs and cavity wall when breathing
Explain the properties that keep the lungs inflated, including differences between intrapleural and intrapulmonary pressures.
Lungs cling to inner surface of the chest wall as it expands because of surface tension created by the pleural fluid, Lungs contain elastic connective tissue that recoils.
Intrapleural Pressure – pressure in the pleural cavity
•contrasting outward pull of the chest wall and inward pull of elastic lungs
•creates a vacuum in the pleural cavity
•this pressure is lower than pressure inside the lungs
Intrapulmonary Pressure – pressure inside the lungs
•higher than intrapleural pressure when lungs are inflated
Recall the impacts of smoking, lung cancer, pleurisy, and pleural effusion on lung function.
Smoking = Damaged alveoli fuse together, reducing surface area for gas exchange, Increases risk of respiratory infections, emphysema, and lung cancer — secondhand smoke exposure increases risk of asthma, bronchitis, and ear infections. Smoking also decreases blood flow and tissue oxygenation: Nicotine triggers vasoconstriction — Carbon monoxide interferes with O2 binding to hemoglobin — Increased atherosclerosis
Lung Cancer = Three types: Squamous Cell Carcinoma – most common, develops from epithelial cells that line bronchial passages after the lining thickens to withstand smoking damage. Adenocarcinoma – develops from mucus-producing glands along mucosal linings. Small-Cell Carcinoma – develops from neuroendocrine cells located in larger bronchi
Pleurisy – inflammation of the pleural membranes (Increased friction between membranes, Very painful)
Pleural Effusion – excess fluid in the pleural cavity, can be caused by: Left side heart failure, Pulmonary embolisms, Liver damage, Infections of the lungs, Lung cancer triggering inflammatory response.
Describe how a pneumothorax can occur, and explain how it can lead to atelectasis.
For lungs to inflate properly, intrapulmonary pressure must be higher than intrapleural pressure.
Pneumothorax – air enters the pleural cavity and raises intrapleural pressure; can be caused by:
•injury to the chest wall admitting air into the cavity (stabbing)
•injury to a lung (as with a broken rib) allows air to escape into the cavity
Atelectasis – collapsed lung
•air has to be removed from the cavity either naturally (minor cases) or through a chest tube.
Define respiration, and explain its four processes.
Respiration – general term for exchange of gases between the air and systemic cells of the body
Four Processes:
•Pulmonary Ventilation – movement of gases between atmosphere and alveoli
•Alveolar Gas Exchange (External Respiration) – exchange of gases between air in alveoli and blood in pulmonary capillaries
•Gas Transport – transport of respiratory gases within the blood between lungs and systemic cells
•Systemic Gas Exchange (Internal Respiration) – exchange of respiratory gases between the blood and systemic cells
Summarize the gas movements from the four processes of respiration.
1) Air containing O2 is inhaled into alveoli during inspiration
2) O2 diffuses from alveoli into pulmonary capillaries
3) Blood from lungs transports O2 to systemic cells
4) O2 diffuses from systemic capillaries into systemic cells
5) CO2 diffuses from systemic cells into systemic capillaries
6) CO2 is transported in blood from systemic cells to lungs
7) CO2 diffuses from pulmonary capillaries into alveoli
8) Air containing CO2 is exhaled from alveoli into the atmosphere
Define inspiration, expiration, quiet breathing (eupnea), and forced breathing.
Movement of air between the atmosphere and the alveoli
•Inspiration (inhalation) – brings air into the lungs
•Expiration (exhalation) – forces air out of the lungs
•Quiet breathing (eupnea) – rhythmic breathing at rest
•Forced breathing – more vigorous breathing during exertion
Requires pressure changes within the lungs for air movement
Distinguish between the functions of the different groups of skeletal muscles of breathing.
Muscles of quiet breathing (contraction leads to inspiration):
•Diaphragm (flattens), External Intercostals
Muscles of forced inspiration – used during deep inspiration as during heavy exercise
•examples – sternocleidomastoideus, pectoralis minor
Muscles of forced expiration – contract during hard expiration (blowing up balloon)
•examples – internal intercostals, abdominal muscles
Quiet expiration is a passive process that requires no muscle contraction, driven instead by the elastic recoil of the lungs and thoracic cavity as inspiratory muscles relax
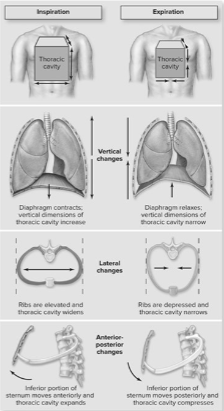
Describe how contractions of breathing muscles change the volume of the thoracic cavity.
Contractions of breathing muscles cause volume changes in the thoracic cavity in three dimensions
Vertical changes:
•diaphragm contraction causes flattening and expansion of the thoracic cavity
Lateral changes:
•elevation of the ribs widens the thoracic cavity (inhaling)
•depression of the ribs narrows the thoracic cavity (exhaling)
Anterior-posterior changes:
•inferior portion of the sternum moves anteriorly → expands cavity (inhaling)
•when it moves posteriorly, cavity compresses (exhaling)
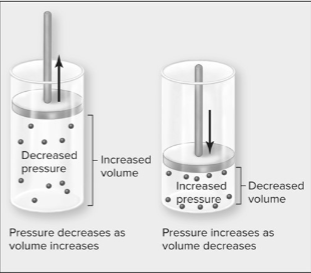
Explain the relationship between volume and pressure.
At constant temperature:
•the pressure of a gas decreases if the volume increases.
•the pressure of a gas increases if the volume decreases.
Think about squeezing a balloon:
•squeeze balloon → decreases balloon volume → pressure increases and the balloon may burst
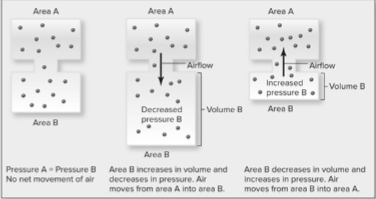
Define pressure gradient, and explain how they affect the movement of gasses.
pressure gradient = occur when the force per unit area is higher one location than another
•air moves from area of greater pressure to lesser pressure if two locations are connected until the pressures equalize.
•air pressure can be measured in mm Hg
Describe the volumes and pressures associated with breathing.
Atmospheric Pressure: pressure of all air gases together in the air that surrounds us
•760 mm Hg is standard value at sea level, Decreases with altitude
Intrapulmonary Pressure: pressure of air inside the alveoli
•Fluctuates with breathing changes, but equalizes with atmospheric pressure at the end of inspiration and expiration (760 mm Hg also)
Intrapleural Pressure: pressure within the pleural cavity; always lower than intrapulmonary pressure if lungs are inflated.
•typically 756 mm Hg before inspiration
Explain the processes of quiet breathing, including changes in breathing muscles, volumes, and pressures.
During Quiet Inspiration:
•Diaphragm and external intercostals contract → increases thoracic cavity volume
•Reduces intrapulmonary pressure
•Lungs expand → decreasing intrapulmonary pressure BELOW atmospheric pressure because alveolar volume increases
•Air flows from the atmosphere into the alveoli because of the pressure gradient.
Tidal volume: increased volume inside the lungs from quiet inspiration (approximately 500 mL)
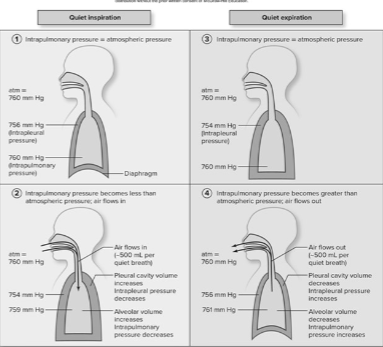
Explain the processes of quiet breathing, including changes in breathing muscles, volumes, and pressures.
During Quiet Expiration:
•Atmospheric pressure and intrapulmonary pressure have equalized at the end of inspiration.
•Diaphragm and external intercostals relax. (Thoracic cavity decreases in size, Intrapleural pressure and intrapulmonary pressure both increase)
•Since intrapulmonary pressure exceeds atmospheric pressure air flows from alveoli out of the lungs to the atmosphere.
Tidal volume of air is released; pressures return to normal.
Describe how forced breathing leads to greater air movement into and out of the lungs.
•Contraction of muscles of forced inspiration and/or forced expiration cause greater volume changes.
•Greater volume changes cause greater pressure changes and steeper gradients.
•Causes more movement of air into or out of the lungs.
Describe the location and components of the respiratory centers in the brainstem.
Respiratory Center Components: Medullary Respiratory Center (located in the medulla oblongata, Two clusters of nuclei)
Ventral Respiratory Group – contains neurons that stimulate inspiration and expiration muscles
Dorsal Respiratory Group – receives sensory input and then sends signals to the ventral respiratory group
Pontine Respiratory Center – located in the pons, sends signals to the Ventral Respiratory Group
Describe the locations of chemoreceptors, and explain how they influence the respiratory centers in the brainstem by monitoring levels of three molecules.
Chemoreceptors are the main sensory receptors for breathing adjustments.
Monitor changes in body fluids:
•H+ concentration
•CO2 levels
•O2 levels
Central chemoreceptors are located in the medulla oblongata. (CSF) H+ concentration in cerebrospinal fluid
Peripheral chemoreceptors are located in the aortic arch and at the splits of the common carotid arteries.
Explain how carbon dioxide release into body fluids increases hydrogen ion concentration (lowers pH).
Carbon dioxide reacts with water in body fluids to become carbonic acid(H2CO3)
•Carbonic acid dissociates into a hydrogen ion and a bicarbonate ion (HCO3).
•Chemical equation:
•CO2 + H2O → H2CO3 → H+ + HCO3
If CO2 builds up in body fluids → more carbonic acid produced → dissociates and increases the concentration of hydrogen ions in body fluids.
pH is a measurement of the concentration of H+. (7.35-7.45)
•Higher pH value = lower H+ concentration = less acidic/more alkaline.
•Lower pH value = higher H+ concentration = more acidic/less alkaline.
Describe how regulating carbon dioxide levels through breathing helps control body fluid pH.
CO2 + H2O → H2CO3 → H+ + HCO3-
•Body fluid pH should be maintained between 7.35 and 7.45.
•Exhaling out more CO2 reduces H+ concentration and raises body fluid pH.
•Exhaling out less CO2 increases H+ concentration and lowers body fluid pH.
•Breathing rate and depth adjustments play a very important role in maintaining the pH of body fluids.
Recall how additional sensory receptors function in control of breathing.
Irritant Receptors in the respiratory passages – stimulated by dust and other particles
Baroreceptors in the visceral pleura and bronchiole smooth muscle function as lung stretch receptors.
Proprioceptors in the joints and muscles are triggered by body movements
Central chemoreceptors monitor H+ levels in cerebrospinal fluid.
•high H+ indicates that more CO2 needs to be exhaled out of the body.
•sensory signals sent to respiratory center to trigger these changes.
Peripheral chemoreceptors monitor H+, CO2 concentration, and O2 concentration.
•high H+, high CO2, or very low O2 indicate that breathing rate and depth need to be increased.
•sensory signals sent to respiratory center to trigger these changes.
Describe the functions of the inspiratory neurons of the ventral respiratory group.
Inspiratory neurons in the ventral respiratory group (VRG) trigger skeletal muscles of quiet breathing.
•Contraction triggers inspiration because of volume and pressure changes.
Inhibition of the inspiratory neurons triggers relaxation of the skeletal muscles and expiration occurs. (decrease volume of thoracic cavity, intrapulmonary forces air out of lungs to atmosphere until intrapulmonary equalizes atm.)
•VRG expiratory neurons inhibit the inspiratory neurons.
Average quiet breathing rate = approximately 12 to 15 breaths per minute (eupnea).
•The pontine respiratory center sends signals that help smooth transition from inspiration to expiration.
Explain the step-by-step processes for how chemoreceptors trigger changes in breathing rate and depth through reflexes.
•Sensory nerve signals from chemoreceptors travel to neurons in the Dorsal Respiratory Group (DRG).
•The DRG sends signals to the VRG to alter breathing rate and depth. (Rate is altered by changing how frequently inspirations occur, Depth is adjusted by stimulating accessory breathing muscles).
•High H+ and CO2 trigger increased breathing rate and depth so more CO2 will be exhaled out. (Lower H+ and CO2 levels will cause breathing rate and depth to decrease).
•O2 concentration in blood must decrease dramatically before peripheral chemoreceptors trigger increased breathing rate and depth.
•CO2 concentration is the most potent stimulator of breathing changes.
•Proprioceptors detect “exercise” and trigger increased breathing rate and depth.
•Lung baroreceptors detect stretch and inhibit inspiration to prevent overstretching of the lungs.
•Irritant receptors in the nasal cavity trigger sneezing, and irritant receptors in the trachea and bronchi trigger coughing.
Describe the two factors that affect airflow in the respiratory tract.
Airflow – the amount of air that moves into and out of the respiratory tract with each breath.
1.Pressure gradient between atmospheric pressure and intrapulmonary pressure
•remember – air flows from higher pressure to lower pressure, higher gradient = greater air flow
2.Resistance to airflow that occurs within the respiratory tract, lungs, and chest wall
•higher resistance = lower air flow
Explain how changes in thoracic cavity volume create the pressure gradients required for inspiration and expiration.
•remember that increased thoracic cavity volume DECREASES intrapulmonary pressure.
•the decreased pressure allows air to flow from the atmosphere into the lungs.
•thoracic cavity volume increases when the diaphragm and external intercostals contract (flattens).
•for deeper inhalation, accessory muscles of breathing contract → thoracic cavity expands more → decreases intrapulmonary pressure more than usual (steeper gradient).
•air flows into the lungs until intrapulmonary pressure equals atmospheric pressure again.
Describe three factors that increase resistance to airflow.
Resistance includes all factors that make it more difficult to move air from the atmosphere to the alveoli:
•Decreased elasticity of the chest wall and lungs increases resistance.
•Bronchoconstriction decreases the diameter of the bronchioles and increases resistance to airflow. (example - asthma)
•Increased surface tension in the alveoli if surfactant levels are low. (mainly a problem in premature infants)
Define compliance and describe conditions that can reduce it and affect breathing.
Compliance – how easily the lungs and chest wall can expand.
•Can be affected by surface tension in the alveoli and elasticity of the chest wall/lungs.
•Reduced elasticity of lungs and/or chest wall with aging → lower compliance → reduced airflow into the lungs.
•Fibrosis (scarring) of lung tissue reduces compliance. (more collagen fibers)
•Burns and/or scar tissue around the chest can also reduce compliance.
Distinguish between pulmonary and alveolar ventilation.
Pulmonary Ventilation – amount of air moving into and out of the lungs.
•can be given as amount of air inhaled in one minute. (tidal volume = 500 mL, breathing rate = 12 breaths per minute, Pulmonary ventilation = 500 mL/breath X 12 breaths/minute = 6000 mL/minute (6 Liters per minute)
Alveolar Ventilation – amount of air actually reaching alveoli
•Pulmonary Ventilation Volume MINUS Anatomic Dead Space in the Lungs, determined per minute
•Anatomic Dead Space – volume of air in the lungs not involved in gas exchanges
•Loss of alveoli increases anatomic dead space (less space for gas exchanges).
Define the four different respiratory volume measurements.
Tidal Volume (TV) – volume of air inhaled or exhaled per breath during quiet breathing.
Inspiratory Reserve Volume (IRV) – extra volume of air that can be inhaled with maximum inspiration beyond TV.
Expiratory Reserve Volume (ERV) – extra volume of air that can be forcibly exhaled beyond TV.
Residual Volume (RV) – volume of air remaining in lungs after the most forceful exhale.
Define and calculate the four major respiratory capacities.
Inspiratory Capacity (IC) = TV + IRV – Maximum amount of air that can possibly be inhaled
Functional Residual Capacity (FRC) = ERV + RV – Amount of leftover air in lungs after normal exhale
Vital Capacity (VC) = TV + IRV + ERV – Total amount of air that can be moved in and out of the lungs with forceful breathing
Total Lung Capacity (TLC) = TV + IRV + ERV + RV – Total amount of air the lungs can possibly hold
Define partial pressure and the movement of gases relative to a partial pressure gradient.
Air is a mixture of gases – Mixture includes O2, CO2, N2, and water vapor, Air moves from higher to lower pressure, down its pressure gradient.
Partial Pressure – the pressure exerted by an individual gas within a mixture, measured in mm Hg.
•Written as PO2 or PCO2 for respiratory gases.
•Atmospheric pressure = sum of the partial pressures of all gases. (760 mm Hg)
•Partial pressure represents the percentage of the particular gas in the mixture.
•Individual gases move down their own partial pressure gradients, independently of each other. (O2 and CO2 can move in opposite directions).
Explain the movements of respiratory gases between the alveoli and pulmonary capillaries based on their partial pressures.
Air in the alveoli:
•PO2 = 104 mm Hg
•PCO2 = 40 mm Hg
Blood arriving in the pulmonary capillaries:
•PO2 = 40 mm Hg
•PCO2 = 45 mm Hg
Gases diffuse until partial pressures equalize in alveolar air and blood.
•O2 moves into the blood.
•CO2 moves from blood to air.
Explain the movements of respiratory gases between the systemic capillaries and tissues based on their partial pressures.
Blood arriving in the systemic capillaries:
•PO2 = 95 mm Hg
•PCO2 = 40 mm Hg
Interstitial fluids:
•PO2 = 40 mm Hg
•PCO2 = 45 mm Hg
Gases diffuse until partial pressures equalize in interstitial fluids and blood.
•O2 moves into the interstitial fluids.
•CO2 moves from interstitial fluids to blood.
•Note after the exchanges, the blood leaving the capillary has values that match deoxygenated blood entering a pulmonary capillary.
Describe the problems associated with emphysema.
emphysema - Loss of gas exchange due to inflammation of tissues in the respiratory zone (respiratory bronchioles, alveolar ducts, alveoli) and destruction of elastic connective tissues in the lungs.
•alveoli dilate or fuse together, lowering surface area for gas exchange.
•loss of lung elasticity → poor expiration
•damaged tissues do not regenerate.
•most cases are caused by smoking; however, some patients have a genetic deficiency in an enzyme that breaks down elastase produced by neutrophils.
•normally produced by neutrophils to help fight infections, but needs to be broken down quickly to avoid lung damage.
List ways that respiratory diseases can interfere with alveolar gas exchange.
Several diseases decrease gas exchanges by thickening the respiratory membrane and/or reducing the number of alveoli.
•emphysema, lung cancer, and tuberculosis all decrease the number of alveoli, reducing surface area for gas exchange.
•pneumonia and congestive heart failure increase fluid in the alveoli and increase thickness of the respiratory membrane.
•bronchitis and asthma narrow bronchial passages and limit airflow into the alveoli.
•blood flow obstruction from pulmonary emboli can reduce gas exchange as well.
Describe how the blood transports oxygen gas.
•O2 doesn’t dissolve efficiently in blood plasma.
•98% of O2 is transported in blood, bound to iron in the heme molecules of hemoglobin. (Oxyhemoglobin – Hb with O2 bound, Deoxyhemoglobin – Hb with no O2 bound)
•Over 20 trillion erythrocytes in the blood, each with about 280 million hemoglobin molecules.
Describe the three means of carbon dioxide transport in the blood.
CO2 has three means of transport in the blood:
•Dissolved in the plasma (7%)
•Attached to the globin portions of hemoglobin (23%)
•As bicarbonate ions (HCO3-) dissolved in plasma (70%)
Describe the chemical reaction that leads to bicarbonate formation from carbon dioxide and water.
Bicarbonate formation occurs inside erythrocytes by an enzyme called carbonic anhydrase.
Chemical reaction catalyzed by carbonic anhydrase:
CO2 + H2O <-> H2CO3 <-> HCO3- + H+
•Note that the reaction arrows show this chemical reaction can proceed in both directions.
•When CO2 diffuses into the blood, the reaction is pushed to the right and bicarbonate ions form.
•When CO2 needs to be released from blood to air in alveoli, the reaction is pushed to the left, and bicarbonate ions release CO2.
Define oxygen-hemoglobin saturation, and describe the normal saturation changes during external and internal respiration.
four binding sites per hemoglobin(Hb) for O2, O2 saturation percentage refers to the percentage of all binding sites that are occupied by O2 molecules.
•as PO2 increases, oxygen saturation of Hb increases.
Alveolar PO2 is 104 mm Hg at sea level, so Hb becomes about 98% saturated as it passes through the pulmonary capillaries.
At high altitudes, the PO2 decreases, which lowers saturation.
•drops as low as 75% at around 17,000 feet of altitude, Altitude sickness can develop with lower O2 saturation.
Systemic PO2 is 40 mm Hg at resting conditions, so Hb is approximately 75% saturated when it leaves systemic capillaries.
•only 25% of O2 is released to tissues as blood passes through a systemic capillary.
Amount of remaining O2 bound to Hb = oxygen reserve.
•the oxygen reserve provides extra O2 for release to tissues during periods of high metabolic activity.
Describe the factors that increase oxygen gas release from hemoglobin, and explain why this is beneficial.
As temperature increases, more O2 is released from hemoglobin.
•higher temperature indicates higher metabolism.
As H+ concentration increases, more O2 is released from hemoglobin.
•H+ increases with metabolic activity (CO2 is converted to carbonic acid).
2,3-bisphosphoglycerate production in erythrocytes increases O2 release
•thyroid hormone, epinephrine, GH, and testosterone stimulate production.
Increased CO2 binding to Hb causes more O2 to dissociate.
•Increased CO2 indicates increased metabolism.
Describe how the blood transports oxygen gas.
Hemoglobin transports three substances from respiratory activities:
•O2 attached to iron
•CO2 bound to globin
•H+ ions bound to globin
Remember that hydrogen ion concentration determines pH.
•Very chemically reactive, so their concentrations have to be maintained within a narrow range (pH 7.35 to 7.45)
•The binding or release of one substance changes the shape of hemoglobin as a whole and affects binding of other substances.
Define hyperventilation, and describe the problems associated with it.
Hyperventilation – breathing rate or depth increased beyond the body’s demand – triggered by anxiety, panic, ascending to high altitude
Hyperventilation increases PO2 and lowers PCO2 in the alveoli.
•O2 saturation of Hb not really affected by increase because saturated at lower partial pressures.
•Excess CO2 leaves the blood → hypocapnia.
•Low CO2 levels → less carbonic acid production → higher body fluid pH. (can result in respiratory alkalosis if pH exceeds 7.45).
•Blood vessels constrict when CO2 levels are low. Even blood delivery to the brain is decreased.
Define hypoventilation, and describe the problems associated with it.
Hypoventilation – breathing that is too slow (bradypnea) or too shallow (hypopnea), can be caused by airway obstruction, pneumonia, brainstem injury, obesity, or any condition that interferes with ventilation or alveolar gas exchange.
O2 levels decrease and CO2 levels increase in the alveoli, causing:
•Lower PO2 in the blood (hypoxemia)
•Skin may look blue (cyanosis) due to decreased Hb saturation.
•Lower PO2 in tissues (hypoxia)
•Higher PCO2 in the blood (hypercapnia) (Higher CO2 levels → more carbonic acid production → lowers body fluid pH, Can develop into respiratory acidosis if pH drops below 7.35)
Chemoreceptors detect high CO2 and H+ and trigger increased breathing rate and depth if hypoventilation is done deliberately.
Describe hyperpnea as a normal breathing adjustment to exercise.
Hyperpnea occurs during exercise.
•depth of breathing increases, but not the rate.
•differs from hyperventilation (both breathing rate and depth are increased).
During exercise, more O2 is consumed and more CO2 is produced.
PO2 and PCO2 remain relatively the same as at rest because:
•deeper breathing, increased cardiac output, and increased blood flow occur.
•these changes deliver more O2 and remove more CO2.