Looks like no one added any tags here yet for you.
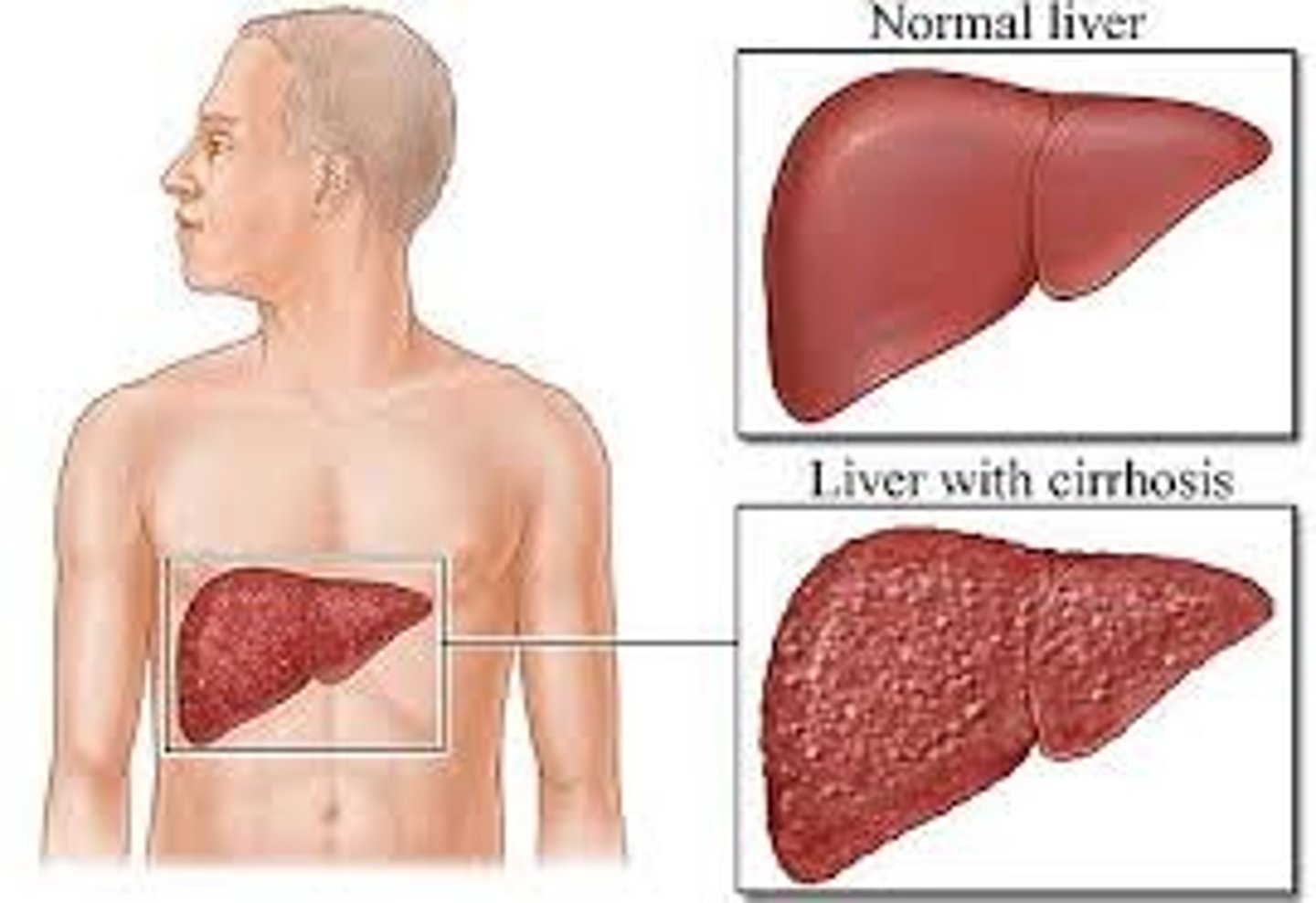
Cirrhosis
Irreversible chronic injury of the liver as a result of chronic hepatitis
Cirrhosis S&S
1. Jaundice
2. Peripheral edema
3. Dupuytren's contracture (DC)
4. Palmar erythema
5. Angiomas
6. Hepatomegaly and splenomegaly
7. Ascites
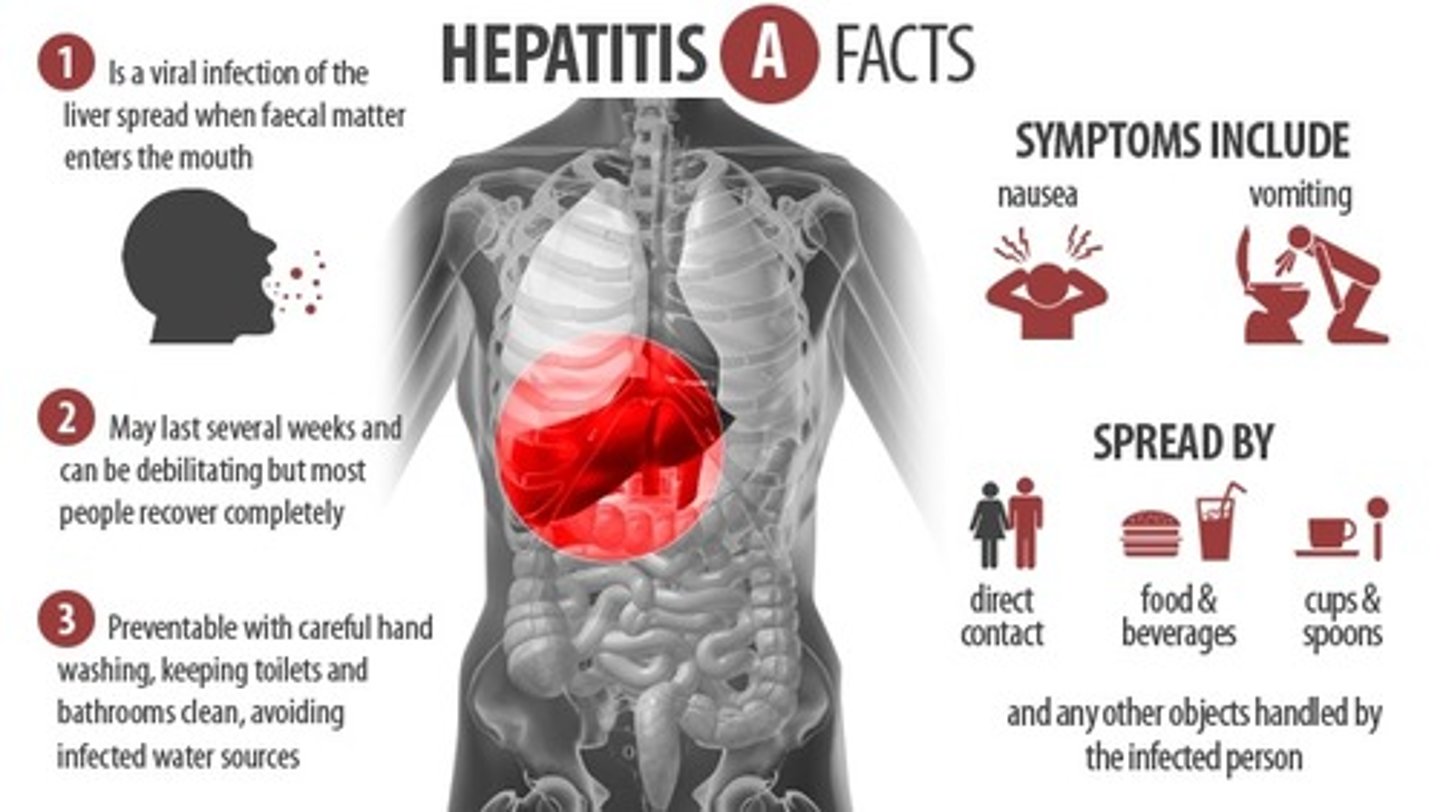
Hepatitis A (HAV)
Transmission:
Severity:
Vaccine:
Prevention:
Prognosis:
Transmission: Primarily through the fecal-oral route, often due to contaminated food or water, or person-to-person contact (e.g., infected food handlers).
Acute illness that is not chronic
Severity: Mild to severe
Vaccine: Available for prevention.
Prevention: Focuses on good personal hygiene, handwashing, sanitation, and
immunization.
Hepatitis B (HBP)
Transmission:
Illness Duration:
Severity:
Vaccine:
Prevention:
Prognosis:
Transmission: Through blood (including blood transfusions), body fluids, body tissues, oral or sexual contact with an infected person, and contaminated needles.
Severity: Mild to severe
Vaccine: Available for prevention.
Prevention: Involves education, proper use and disposal of needles, use of
personal protective equipment (PPE), and other standard precautions.
Hepatitis D (HDV): Can coinfect with ____, leading to more severe liver disease.
•______ prognosis, results in acute liver failure
Hepatitis B (HBP)
•Poor prognosis, results in acute liver failure
pancreas endocrine function
pancreatic islets secrete insulin and glucagon
role of insulin and glucagon
Insulin promotes uptake of glucose
Glucagon promotes the breakdown of glycogen into glucose (to release into the blood stream)
pancreas exocrine function
•Secretion of digestive enzymes into the small intestine that break down carbohydrates, fats, proteins, DNA, and RNA
function of the liver
•Drug and hormone metabolism/elimination
•Energy metabolism
•Protein/amino acid production
•Micronutrient storage and metabolism
•Endocrine function
•Contribution to immune responses
Only human organ capable of regenerating lost tissue
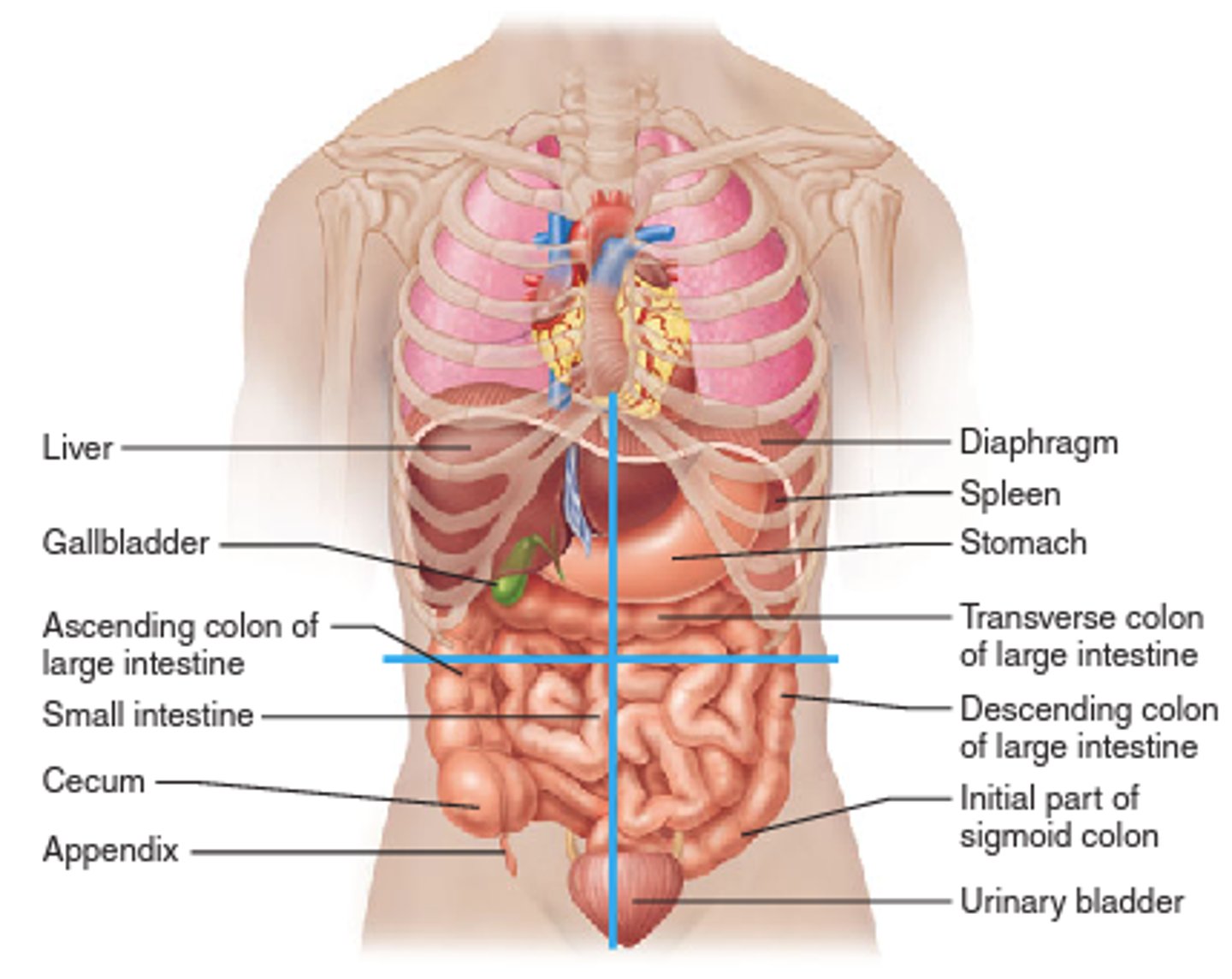
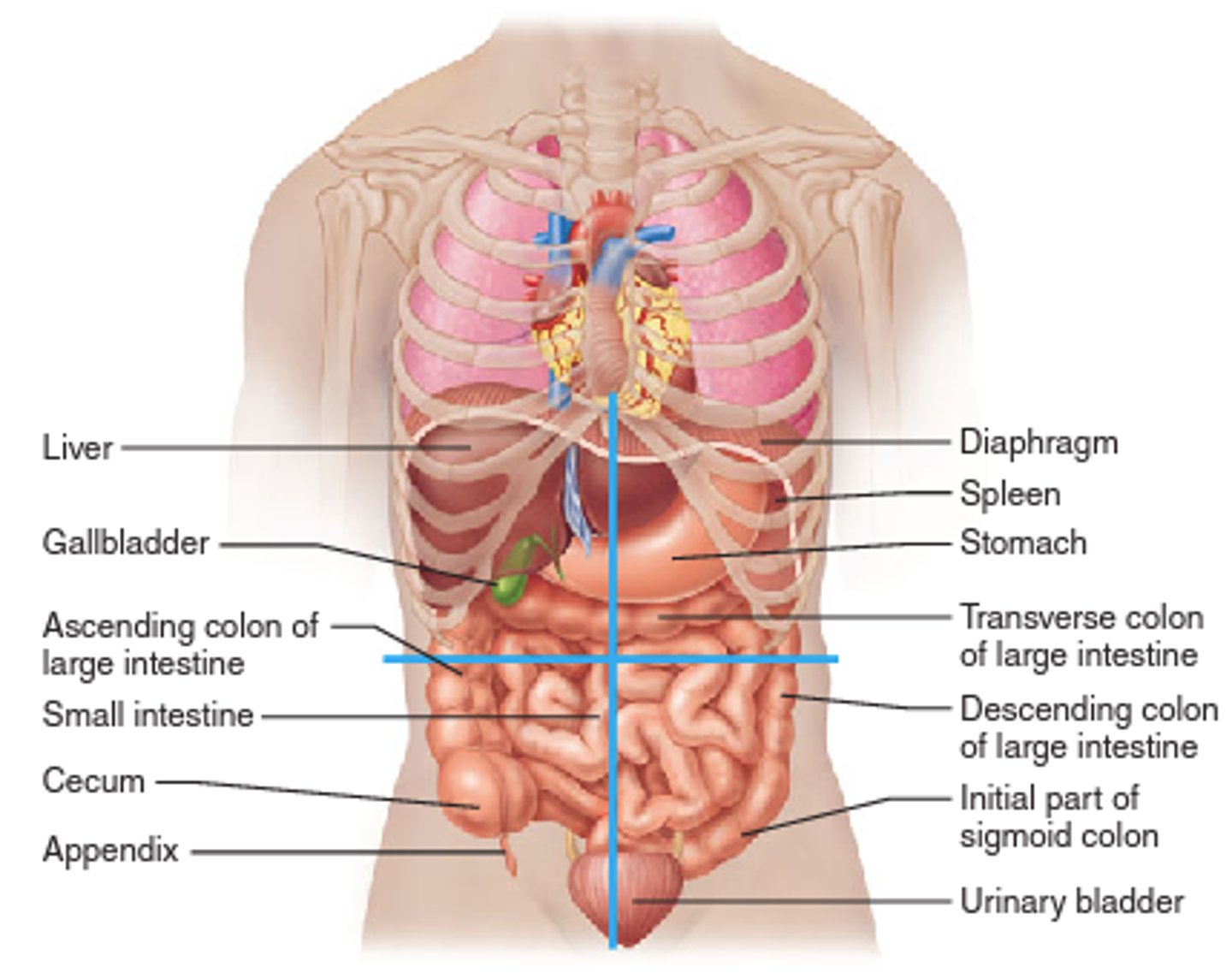
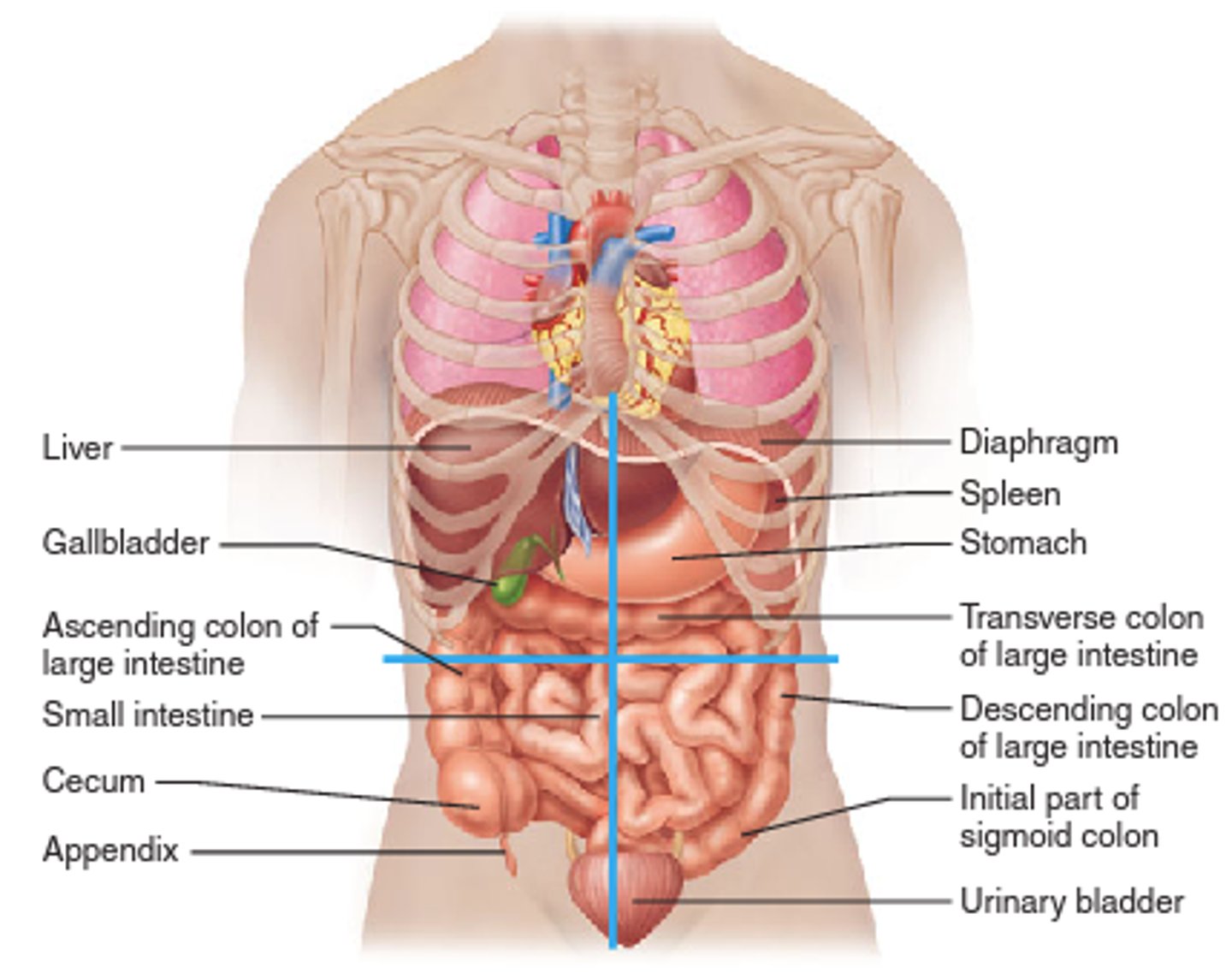
liver
LUQ
•Left lobe of liver
•Stomach
•Spleen
•Pancreas
RUQ
•Gall bladder
Right lobe of liver
RLQ
•Appendix
acute renal failure
sudden loss of kidney function with resulting elevation in BUN (blood urea nitrogen) and creatinine
acute renal failure etiology
•circulatory disruption to kidneys, toxins, bacterial toxins, acute obstruction, trauma
chronic renal failure
progressive loss of kidney function leading to end-stage renal failure
chronic renal failure etiology
Prolonged urinary tract obstruction and infection, diabetes mellitus, systemic lupus erythematosus, uncontrolled HTN
Uremia is____ resulting from _________. symptoms:
An end-stage toxic condition resulting from renal insufficiency and retention of nitrogenous wastes in blood. Symptoms include anorexia, nausea, and mental confusion.
how are renal and cardiovascular function interrelated
· High blood pressure is the 2nd leading cause of kidney failure in the U.S.
· Hypertension and other types of cardiopulmonary dysfunction can also occur secondary to kidney disease
major processes in the nephron to form urine
Excretion = Filtration + Secretion - Reabsorption
Filtration:
•Filtration: Substances move out of the blood plasma and into the nephron
•Occurs in the glomerulus
Secretion:
•Secretion: Substances move out of the blood plasma into the nephron
•Occurs in the tubules and collecting ducts
function of the kidneys major theme=
regulation
•Regulates body fluid composition and pH
•Regulates blood pressure
•Regulates production of RBCs and platelets
•Regulates bone metabolic function
•Eliminates/degrades substances
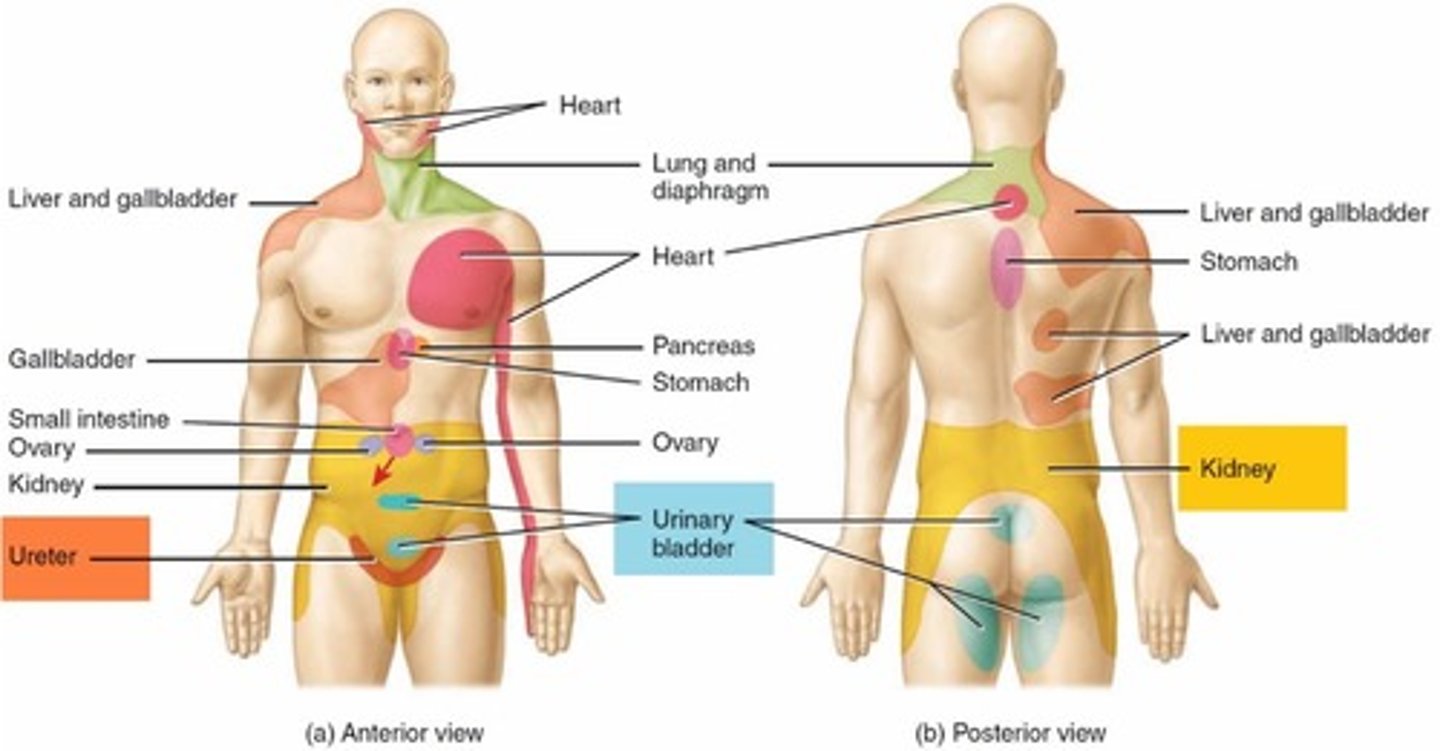
referred pain patterns of the kidney
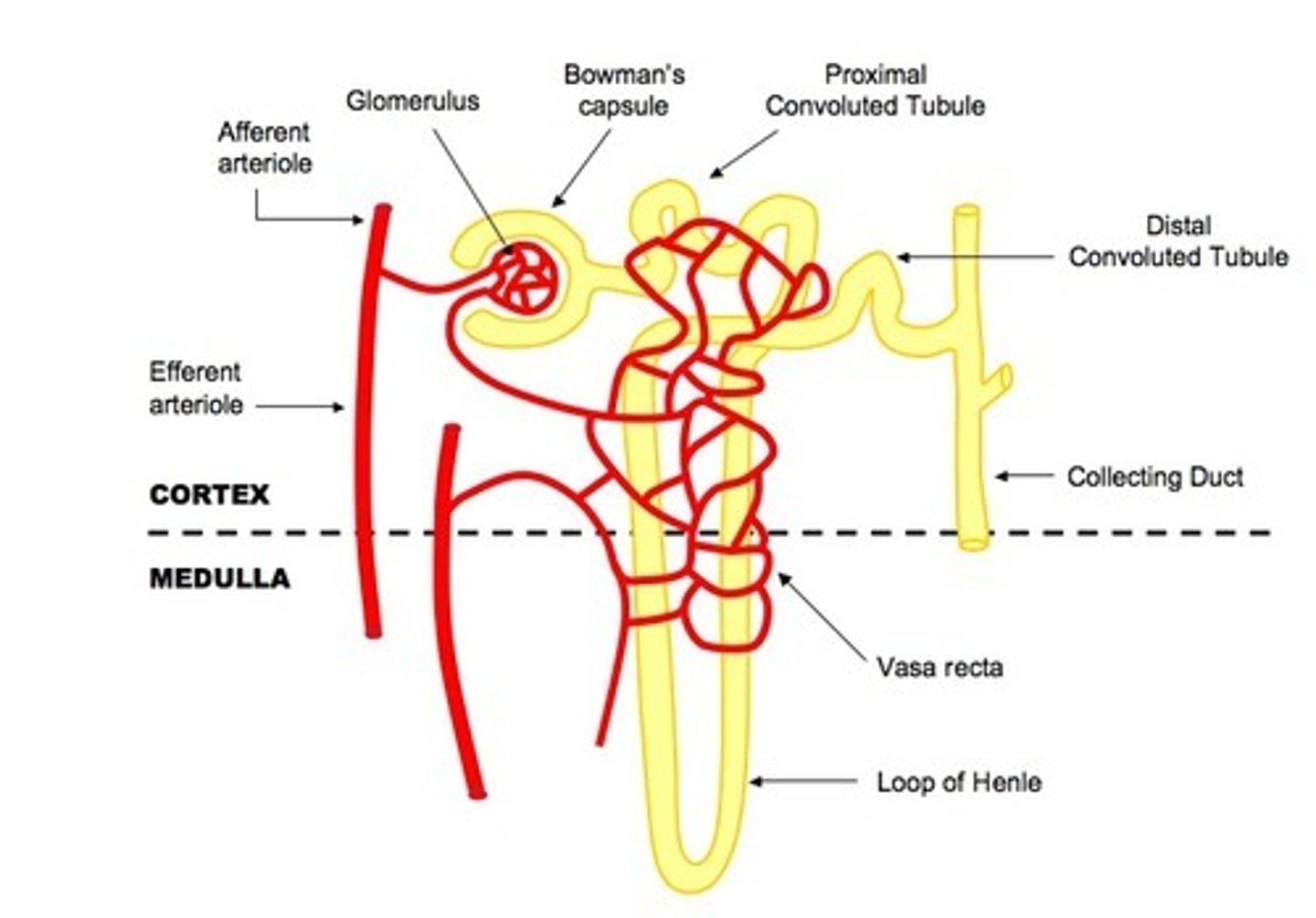
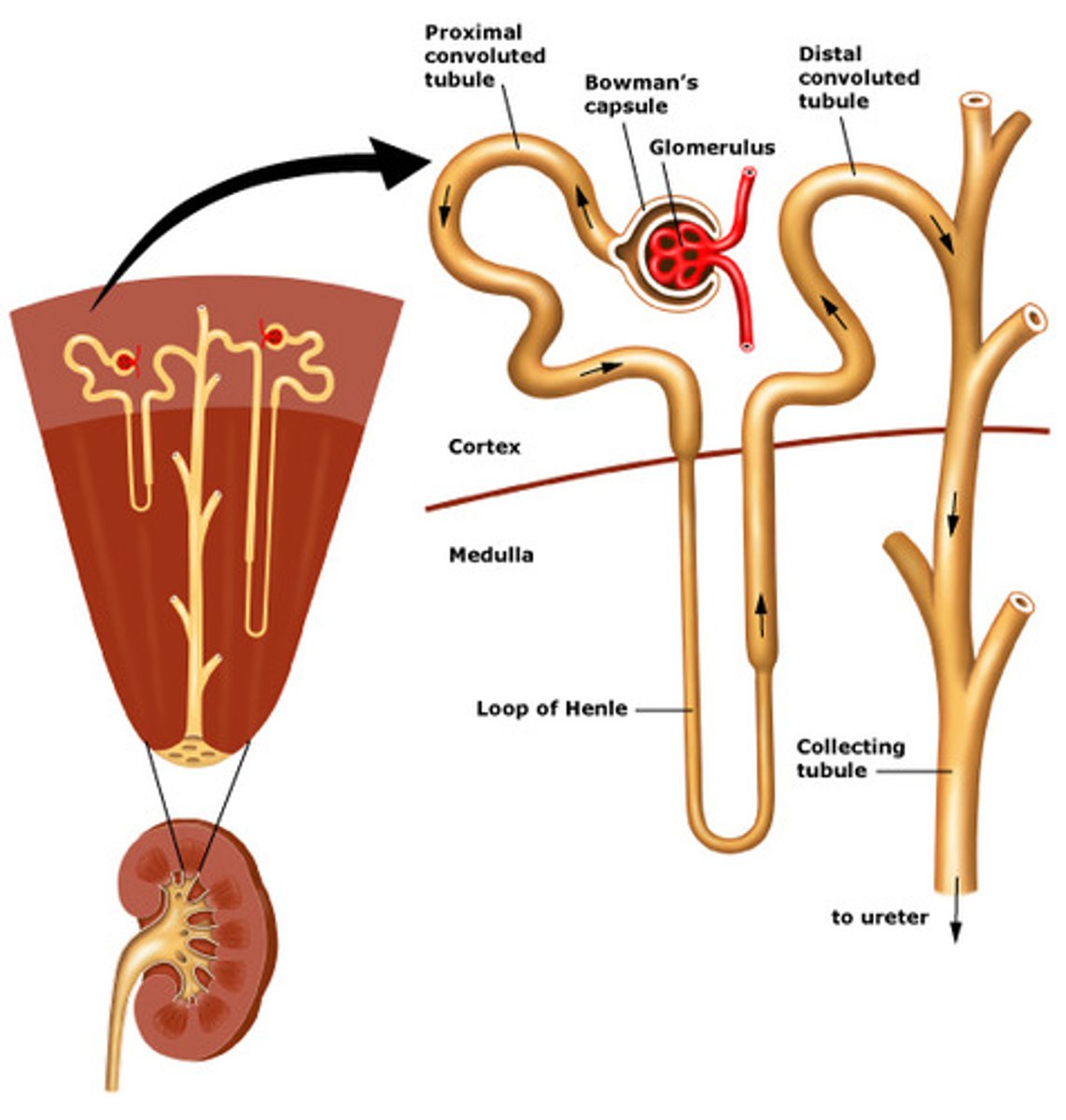
structure of the nephron
•Renal corpuscle: glomerulus surrounded by the Bowman's capsule
•Renal tubule: proximal tubules, loop of Henle, distal tubules, collecting duct system
nephron parts
-glomerular + bowman capsule
-proximal convoluted tube
-loop of henle
-distal convoluted tube
-cortical collecting duct
-medullary collecting duct
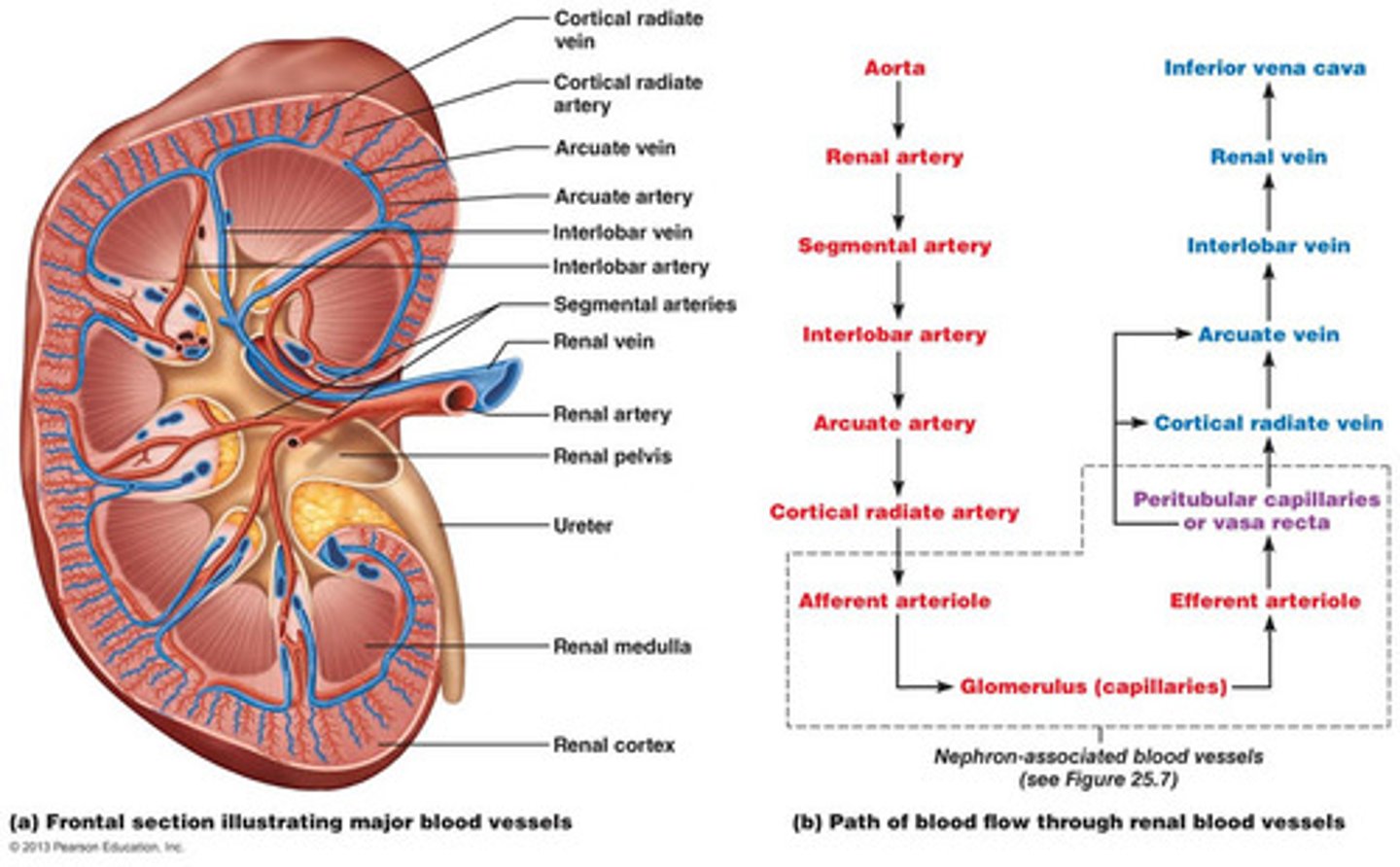
path of blood flow through kidney
Afferent arteriole → Glomerulus → Efferent arteriole
RER=
ratio between CO2 released and O2 consumed
VCO2 / VO2
RER 1.00 = ____ metabolism
100% carbs, 0% fat
RER .70= ____ metabolism
100% fat, 0% carbs
Glycogenolysis:
breakdown of glycogen
Gluconeogenesis:
formation of glucose from a non-CHO source
Lipolysis:
breakdown of triglycerides (fat) to make ATP
1 g carb= ___ kcal
1 g fat= ___ kcal
1 g carb= 4 kcal
1 g fat= 9 kcal
Catabolism-
Reactions that breakdown compounds into small units
Anabolism-
Reactions that build complex molecules from smaller one
3 functions of nutrients
Provide energy for metabolism
Build and repair body tissue
Regulate bodily processes
clinical relevance of lactate threshold
Point where lactate accumulates, used to predict endurance
performance and design training programs by shifting threshold to higher intensities
Many of our patients would exceed lacate threshold trying to do ADLs
ATP-CPr System:
Immediate energy through ATP and creatine phosphate, short duration, high intensity.
Glycolysis:
Breakdown of glucose for ATP, moderate duration, moderate intensity.
Oxidative System:
Long-term energy through aerobic metabolism of
carbohydrates and fats, long duration, low to moderate intensity
in the mitochondria
rate limiting enzyme of glycolysis
Phosphofructokinase (PFK)
ATP-CPr system, Glycolysis, and the Oxidative System
each system exists in a specific place in the cell and serves a specific energy production need
Ventilatory threshold-
where minute ventilation stops rising linearly and begins to rise exponentially
cardiovascular adaptations to aerobic exercise training.
Increased CO, SV, blood volume, and capillary density;
decreased HR at rest and submaximal exercise; improved blood flow to muscles
pulmonary adaptations to aerobic exercise training.
Increased ventilation efficiency, better gas exchange, and increased
pulmonary capillary density
Minute ventilation increases linearly with exercise until
~50-75% of VO2 max
a-vO2 Difference (atriovenous oxygen difference):
Difference in oxygen content
between arterial and venous blood, reflecting oxygen extraction by tissues
cardiovascular adaptations to aerobic exercise training goal
match blood flow to metabolic needs of exercising skeletal muscle
cardiovascular adaptations to aerobic exercise training includes:
increased left ventricular volume
increased blood volume
increased capillary density in skeletal muscles
blood flow distribution changes with increasing exercise intensity
· At rest 15-20% of Q goes to skeletal muscle BUT During heavy exercise this increases to 80-85%
· Systemic vasoconstriction and local vasodilation in exercising skeletal muscle
how systolic blood pressure change with increasing exercise workloads.
Increase SBP:
• Increased myocardial contractility and SV
• Due to muscular need for greater force and pressure to deliver blood to exercising muscle
how diastolic blood pressure changes with increasing exercise workloads.
Minimal changes in DBP:
• Arteriolar vasodilation within exercising muscle,
• more blood draining from arteries, through arterioles, and into muscle capillaries
dynamic vs isometric exercise
SBP and DBP
dynamic: level diastolic and increased systolic
isometric: increase in diastolic and systolic
how mean arterial blood pressure changes with increasing exercise workloads.
Increase in SBP typically leads to an increase in MAP
relationship between exercise workload and heart rate
HR and work load cardiac output = linear
relationship between exercise workload and stroke volume
Stroke Volume (SV): In untrained/moderately trained, SV plateaus at 40-60% of VO2max due to reduced ventricular filling time. In highly trained athletes, SV continues to increase until VO2 max due to improved venous return, ventricular filling, and contractile force (Frank-Starling mechanism).