Cardiovascular Clinical Symposium
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
anatomical structures affected by pulmonary embolism
all lobes in right and left lungs
right and left pulmonary arteries with branches
physiology affected by PE
gaseous exchange in the alveoli of the lung
structural abnormalities associated with PE
blockage of pulmonary arterial treedue to embolism (movement) of blood clot/fat/air/amniotic fluid
blockage of deep veins of leg/abdomen by blood clot
physiological abnormalities associated with PE
impaired perfusion of alveoli/lungs
results in low oxygen in blood
prior events leading to a pulmonary embolus
usually source of thrombus that moves to the lungs→ deep veins of legs
hospital admission for surgery and immobility may predispose
experienced symptoms of PE
sudden onset dyspnoea
tachypnoea
pleuritic chest pain
cough
haemoptysis
clinical signs of PE
sinus tachycardia
collapse, circulatory instability due to decreased blood flow through lungs and left side of heart
assessment for DVT if PE suspected
raised jugular venous pressure
abnormal test results identified in PE
low oxygen saturation
low oxygen on blood gases
elevated D-dimer
VQ lung scan showing lack of blood flow to part of lung
CT showing blood clot showing blood clot in artery
medical/surgical intervention for pulmonary embolism
high flow rate oxygen
thrombolytic drugs given by IV to dissolve blood clot
primary and secondary intervention for PE
anticoagulants used immediately and for some moths
initially low molecular weight heparin
then direct oral anticoagulant e.g. apixaban, warfarin
anatomical structures affected by myocardial infarction
left coronary artery with branches
physiology affected by myocardial infarction
delivery of blood to myocardial tissues
structural abnormalities associated with myocardial infarction
narrowing of arteries due to coronary atheroma
blockage of artery
physiological abnormalities associated with myocardial infarction
ischaemia leading eventually to infarction→ necrosis of myocardium
impaired contraction of myocardium
abnormal electrical activity of heart cells
prior events causing myocardial infarction
more common in men than women
risk factors:
smoking
dyslipidaemia
diabetes
sedentary lifestyle
obesity
family history
symptoms experienced in a MI
severe crushing central/generalised chest pain
pain often spreads to arms/neck
nausea, vomiting
sweatiness, breathlessness
clinical signs of MI
patient clearly distressed
low BP
fast heart rate
breathlessness may be obvious with fluid heard on lungs during inspiration
abnormal test results associated with MI
ECG showing ST elevation
Blood test demonstrates raised troponin levels
echocardiogram shows reduced contraction of affected area
coronary angiogram shows blocked artery
medical/surgical intervention for MI
medical emergency
pain relief→ morphine, antiemetic, oral aspirin
primary percutaneous coronary intervention:
through tube in arm/leg
metal stent inserted
primary and secondary intervention for MI
avoidance of risk factors
Key drugs used:
aspirin
clopidogrel
beta-blockers
statins
ACE inhibitors
anatomical structures affected by DVT
deep veins of the leg and pelvis
physiology affected by DVT
return of deox. blood to the right side of the heart and then on to the lungs
structural abnormalities associated with DVT
blockage of the vein by blood clot
usually first appears in calf but then extend above knee and into pelvis and abdomen
physiological abnormalities associated with DVT
thrombophilia→ often expresses itself with recurrent thromboses
prothrombotic states e.g. pregnancy, paraneoplastic factors can increase risk
prior events leading to DVT
recent surgery/hospitalisation
LMWH helps reduce risk
advanced age
obesity
infection
immobilisation
oestrogen containing contraceptives
family history
symptoms experienced in DVT
swelling of right/left calf
pain in calf
no symptoms related to the leg but sudden PE may occur
clinical signs of DVT
swelling/redness of leg
dilation of surface veins
tenderness over veins when applying gentle pressure
abnormal test results associated with DVT
ultrasound of leg demonstrates absence or reduction of venous flow and presence of thrombus
low-probability situation→ D-dimer test
medical/surgical intervention associated with DVT
immediate anticoagulation with LMWH
3-6 month anticoagulation with DOAC or warfarin
primary and secondary prevention of DVT
early and regular walking
hospitalised patients→ LMWH
compression stockings for patients undergoing surgery
long-term anticoagulation therapy
anatomical structures affected by cerebral infarction
all parts of the brain
arteries to the brain
large and small arteries of the brain
physiology affected by cerebral infarction
supply of oxygen and nutrients to the brain
removal of CO2 and waste products from the brain
structural abnormalities associated with cerebral infarction
disease of the wall of arteries going to or within brain e.g. atherosclerosis
dilated atria of the heart
physiological abnormalities associated with cerebral infarction
ischaemia of brain tissue
necrosis of brain tissue
raised intercranial pressure due to brain swelling→ can risk further nerve damage
prior events leading to cerebral infarction
CV risk factors→ smoking, hypertension, dyslipidaemia, diabetes etc
atrial fibrillation
TIA
symptoms experienced in cerebral infarction
face→ drooping/weakness of one side of face
arms→ weakness of one leg or arm
speech→ slurred or incoherent
clinical signs of cerebral infarction
possible evidence of atrial fibrillation
possible high blood pressure
possible bruit heard over carotid artery in the neck
abnormal test results associated with cerebral infarction
brain CT or MRI shows changes of brain ischaemia, swelling and infarction
ultrasound of carotid artery may show narrowing
echocardiogram may show evidence of a blood clot in the atrial appendage
ECG may show evidence of atrial fibrillation
medical/surgical intervention for cerebral infarction
thrombolytic drugs→ dissolve blood clots from within artery
thrombectomy
primary and secondary intervention for cerebral infarction
treat patients with atrial fibrillation w DOAC/warfarin
management of high blood pressure
anatomical structures associated with atrial fibrillation
left and right atria of heart, left atrial appendage
pulmonary veins and their junctions with the left atrium
physiology affected by atrial fibrillation
pacemaker activity of the heart
conduction of electrical depolarisation through the atrium
stimulation of electrical activity in ventricles
structural abnormalities associated with atrial firbrillation
dilated atria
fibrosis (scarring) of atrial muscle
physiological abnormalities associated with atrial firbrillation
arrhythmogenic environment e.g. electrolyte imbalance, sepsis
ectopic activity from around pulmonary veins
prior events causing atrial fibrillation
hypertension
coronary artery disease
excessive alcohol consumption
hyperthyroidism
heart failure
symptoms experienced in atrial fibrillation
palpitations
fatigue and/or breathlessness with exercise
sometimes chest tightness or ankle swelling
clinical signs of atrial fibrillation
pulse is irregularly irregular
sings of underlying causes e.g. high BP, valve murmur, weight loss
abnormal test results associated with atrial fibrillation

medical/surgical intervention for atrial fibrillation
rate control→ seeks to slow down heart rate to prevent palpitations
beta blockers, digoxin, Ca2+ channel blockers
rhythm control→ seeks to convert heart rhythm back to normal, regular sinus rhythm
electrical shock (DIC cardioversion)
drugs e.g. amiodarone
pulmonary veins can be electrically isolated/insulated→ from LA by surgery/catheter ablation
primary/secondary intervention for atrial fibrillation
early and effective treatment of diseases that cause atrial fibrillation e.g. high blood pressure
avoidance of excess alcohol and stimulants e.g. nicotine, caffeine
prevent formation of blood clots in atrium by treatment w DOAC/warfarin
anatomical structures affected by aortic stenosis
aortic valve at outflow of left ventricle and origin of ascending aorta
physiology affected by aortic stenosis
aorta usually opens to allow blood to exit LV and closes to prevent blood from passing backwards from aorta to LV
structural abnormalities associated with aortic stenosis
congenital→ bicuspid aorta
valve becomes calcified gradually over many years
physiological abnormalities associated with aortic stenosis
left ventricle has to generate more force to eject blood through narrowed aortic valve→ becomes hypertrophied
‘pressure overload’ in LV
prior events leading to aortic stenosis
patients are most frequently male over 65
aortic stenosis can cause no symptoms for many years
symptoms experienced in aortic stenosis
angina type chest pain→ worsened with exercise
breathlessness with exercise
light-headedness or collapse with exercise
clinical signs of aortic stenosis
harsh loud ‘ejection systolic’ heart murmur
reduced pulse pressure
forceful apex beat
abnormal test results associated with aortic stenosis
ECG shows evidence of more muscular left ventricle→ QRS increased
echocardiogram shows a narrowed aortic valve→ more muscular left ventricle
medical/surgical intervention for aortic
if the pressure difference between left ventricle and aorta< 60→ patient kept under observation
If LV starts to dilate or symptoms are present, surgery is considered
aortic valve can be replaced by open chest surgery or using percutaneous approach
surgical valves either made of metal or plastic
primary and secondary intervention for aortic stenosis
patients with metallic artificial aortic valves require life-long anticoag. treatment with warfarin
patients with tissue valves do not require warfarin
anatomical structures affected by fallot’s tetralogy
ventricular septum
pulmonary valve
aorta
right ventricle
physiology affected by fallot’s tetralogy
sequential flow of deoxygenated blood through right heart to lungs and oxygenated blood through left heart body
structural abnormalities associated with tetralogy of fallot
ventricular septal defect
pulmonary stenosis
overriding aorta
right ventricular hypertrophy
prior events
patients are born with thus set of abnormalities with no recognisable prior events/ causes
experienced symptoms of fallots tetralogy
primary symptom→ low blood oxygen with/without cyanosis
congenital or developing in first year of life
difficulty feeding and gaining weight
delayed growth and physical development
dyspnoea on exertion
clinical signs of fallots tetralogy
heart murmur
clubbing of fingernails and toenails
hypercyanotic spells→ may result in brain injury and death
older children may squat during hypercyanotic spell→ increases vascular resistance and allows for temporary reversal of a shunt
abnormal test results
echocardiogram demonstrates abnormal anatomy and can assess degree of shunting from left to right or from right to left
medical/surgical intervention
oxygen is effective in treating hypercyanotic spells
surgery designed to designed to relive right ventricular outflow tract stenosis by removal of muscle and repair of VSD
primary and secondary prevention
despite surgery patient remain at increased risk of sudden cardiac death and heart failure
anatomical structures affected by systolic heart failure
usually left ventricle
right ventricle can be involved
physiology affected by systolic heart failure
normal blood supply to lungs and body at the appropriate pressure to allow adequate blood flow
structural abnormalities associated with systolic heart failure
ventricles may be dilated, thinned, thickened
valve regurgitation
mitral/tricuspid valve regurgitation may result from ventricular dilation due to stretching of valve ring
physiological abnormalities associated with systolic heart failure
loses the ability to pump enough blood to meet body’s metabolic needs
heart loses its pumping reserve
prior events leading to systolic heart failure
MI
viral myocarditis
use of chemotherapy drugs
symptoms experienced in systolic heart failure
fatigue
dyspnoea
breathlessness when lying flat
paroxysmal nocturnal dyspnoea
oedema
clinical signs of systolic heart failure
tachypnoea
oedema
high jugular venous pressure
tachycardia
hypotension
cachexia
abnormal test results associated with systolic heart failure
echocardiogram shows red. pumping of heart
dilation of ventricle may be seen and valved can be assessed
ejection fraction
blood test of NT-proBNP
ECG often abnormal
medical surgical/intervention
daily weight can help detect changes in fluid status
standard drug therapy includes ACE inhibitor and beta-blocker
other drugs e.g. mineralocorticoid receptor antagonists
combination therapy with angiotensin II receptor blocker and neprilysin inhibitor
loop diuretics such furosemide
primary and secondary interventions in systolic heart failure
diagnose any underlying disease that might be treated directly
secondary prevention may involve an implanted cardioverter defibrillator to reduce risk of sudden cardiac death
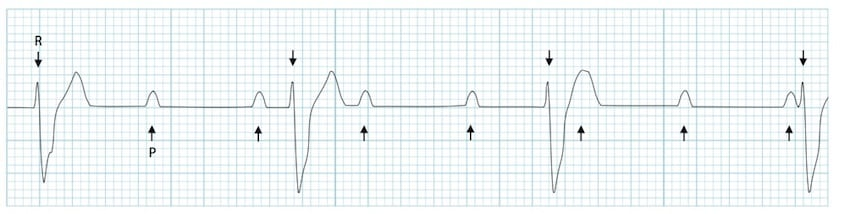
anatomical structures affected by complete heart block
AVN
physiology affected by complete heart block
transmission of wave of electrical depolarisation from atria to ventricles
structural abnormalities associated with complete heart block
fibrosis of AVN
necrosis/infarction of AVN
physiological abnormalities associated with complete heart block
complete failure of AVN to transmit electrical impulse from atria to ventricles
atria have electrical activity and contract independently of ventricles
ventricles develop their own pacemaker activity→ much slower rate
prior events associated with complete heart block
MI
medications e.g. beta blockers or other rate lowering drugs that act to block AVN
symptoms associated with complete heart block
light-headedness
presyncope or syncope
chest pain
signs of heart failure
clinical signs associated with complete heart block
pulse/ heart rate is slow (<60bpm)
low bp
sudden loss of concioussness
abnormal test results associated with complete heart block
medical/surgical intervention associated with complete heart block
atropine→ blocks parasympathetic action w ACh= inc. HR
temporary pacemaker on arrival at hospital
primary and secondary prevention associated with complete heart block
permanent pacemaker needed if complete heart block persists
anatomical structures affected by ventricular fibrillation
left and right ventricles
septum
free walls
right outflow tract
physiology affected by VF
ventricles pump blood to lungs for oxygenations and to the body to supply tissues with oxygen and nutrients
structural abnormalities associated with ventricular fibrillation
heart COULD have normal structure→ Long QT-syndrome
hypertrophied ventricles due to high bp or disease
dilated/scarred ventricles
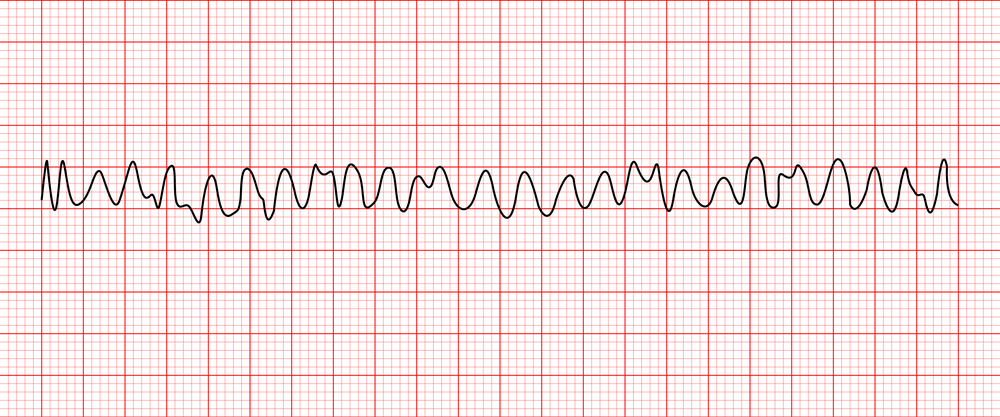
physiological abnormalities associated with ventricular fibrillation
all electrical activity becomes disorganised and chaotic
heart fibrillates (quivers) but does not beat
no blood pumped to lungs or body
prior events associated with ventricular fibrillation
no warning
commonly occurs after myocardial infarction
symptoms associated with ventricular fibrillation
may be some prior warning signs:
palpitations
light headedness
chest pain
loss of consciousness within seconds of fibrillation
abnormal test results associated with ventricular fibrillation
medical/surgical intervention associated with ventricular fibrillation
basic life support
DC electrical shock→ defibrillation
primary and secondary intervention associated with ventricular fibrillation
assessment of risk of VF in young adults requires knowledge of family history
beta blockers are sometimes used
implanted cardioverter defibrillators for high risk patients