When Nightmare is Real: Trauma in Child & Adolescence
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Children of Chowchilla
Masked kidnappers accosted a school bus on the way home from school and abducted the bus driver and 26 children, ages 5 to 14. The kidnappers transported the children and driver to a quarry, loaded them into a buried moving truck. They were buried for 16 hours. The driver and children were able to dig themselves out and escape unharmed. Police soon arrested the quarry owner's son and his accomplices.
The children escaped unharmed
They returned to their homes
They went back to school and everyday routines right away
Everyone assumed that the kids were in fact alright
Experts consulting at the time did not suspect that there would be psychological repercussions to the kidnapping because of:
The age of the children
The limited exposure time
The lack of physical injuries
The quick arrest of the suspect
Children were assessed 5 to 13 months following the event and then again in adulthood. Each child suffered post traumatic symptoms acutely and over the following year:
Acute findings:
Fears of further trauma
Hallucinations
"Omen" formation
Later Findings:
Post-traumatic play
“Personality changes”
Repeated dreams of the event and of dying during the event
Ongoing fears of being kidnapped again
Heightened generalized fears not necessarily related to the trauma
Contact with the survivors continued for 25 years after the kidnapping. They described their ongoing post-traumatic symptoms:
Anniversary triggers lead to heightened emotional response: “Every year at this time I just get kind of weird [in] the way that I rage and the way that I am hot-headed” (Larry Park)
Experience of being forever altered by the event and loss of trust in the world generally: “I will never get back the kid that I was. That kid stayed underground, and it was a different kid that came home. And I think that that happened for each and every one of us – a different child came home” (Larry Park)
Fear that outlives the trauma, hypervigilance to risk, disruption of sleep and disruption of the sense of safety: “Kids are supposed to adjust to things, but I still have not gotten over it. As a kid, I was scared of the dark, I was scared of strangers. Even now, I still sleep with a nightlight and I’m way into my 20’s”
Children have profound reactions to traumatic events both in the short and long term.
“These kids were heroes of medicine because their experience awakened the world that children can be traumatized and the kids are not ‘too young to understand.’”
- Lenore Terr
Lenore Terr published her book Too Scared to Cry in 1990 about the negative consequences of childhood trauma, but the fact that children could experience PTSD was not recognized until the late 90s
What is trauma?
Definitions:
A single experience or repeating events that completely overwhelm the individual’s ability to cope or integrate the ideas or emotions involved with that experience. (Wikipedia)
An emotional response to a terrible event like an accident, rape or natural disaster. Immediately after the event, shock and denial are typical. Longer term reactions include unpredictable emotions, flashbacks, strained relationships, and even physical symptoms like headaches or nausea. (American Psychological Association)
“Traumatization occurs when both internal and external resources
are inadequate to cope with external threat.” Bessel van der Kolk, 1989
“Childhood trauma is the mental result of a blow, or a series of blows,
rendering the young person temporarily helpless and breaking past
ordinary coping and defensive operations.” Lenore Terr, 1991
What makes an experience traumatic?
Can one person experience something as traumatic and another not? Why or why not?
Are the following experiences examples of “trauma?”
Watching the aftermath of a hurricane or tornado on TV?
Having surgery as a young child?
Watching 9/11 from an apartment ten blocks away?
Being removed from your parents who were physically abusing you, and placed into foster care?
Being in a car accident?
Living in an neighborhood where there are nightly shootings?
Living with extreme poverty?
Having a friend who was injured in a school shooting
Different magnitudes of trauma
Big T Trauma: An event that most people would consider traumatic, such as a plane crash or sudden and unexpected loss of a loved one
Little T Trauma: An event experienced as traumatic at a personal level, such as the loss of a pet or a relationship break-up
Key Elements of Trauma, Defined Across Studies
The individual experiencing the event has minimal or NO personal control to stop the event.
The nature of the event is usually beyond the scope of ordinary human experience (usually rare or infrequent).
It is unpredictable in the sense of a sudden event (or a sudden change in mood/behavior of an abusive parent).
In an effort to process the event, the person is changed
Epidemiology
The branch of medicine which deals with the incidence, distribution, and possible control of diseases and other factors relating to health
By age 16, more than 67.8% were exposed to one or more traumas, such as child maltreatment, domestic violence, traffic injury, major medical trauma, traumatic loss of a significant other, or sexual assault.
Copeland et al. (2007) reported that children exposed to trauma had almost double the rates of psychiatric disorders of those not exposed.
Across multiple surveys of large, nationally representative samples of youth:
19% reported physical abuse, whereby an adult hit, beat, kicked, or physically hurt the child in any way (other than spanking)
70% of adolescents age 14-17 reported witnessing violence
6% of youth age 0-17 experienced at least one episode of sexual victimization in the past year
2% of American adolescent girls experienced a drug- or alcohol- facilitated sexual assault
Nearly 1 in 5 (18%) of American youth experienced a traumatic death of a loved one
Approx. one-quarter of adolescents were involved in a natural disaster in their lifetime
10% reported involvement in a motor vehicle accident
The prevalence of psychiatric disorders in children after the exposure to a disaster varies significantly (between 4 to 6% in low violence and disaster areas to up to 70 to 80% for those directly experiencing violence such as a school shootings).
Six months after 9/11, approximately 10.6% of NYC public school children met criteria for Post Traumatic Stress Disorder (PTSD)
The stress response system
Fight, flight, freeze
Ex: Walking in the calm woods, but disrupted by the fright of a bear in sight
National Prevalence of Child Maltreatment
Nationally during FFY 2022, 3,096,101 children received either an investigation response or alternative response at a rate of 42.4 children per 1,000 in the population.
74.3% of victims experience neglect
17.0% percent are physically abused
10.6% percent are sexually abused
6.8% percent are psychologically maltreated
Types of traumatic events
Neglect, physical abuse, sexual abuse
Additional types of trauma and stressors:
Removal from Home
Multiple Foster Placements
Extreme Neglect
Extreme Poverty
Systemic Racism
Domestic Violence (IPV)
Community Violence
Natural Disasters
Emotional/Psychological Abuse
Loss of Significant Others
Debilitating Medical or Psychiatric Condition
Medical Instrumentation/Procedures
Primary Caretaker with a Debilitating
Medical or Psychiatric Condition
Terrorism
Immigration
Kidnapping
Sex Trafficking
Extreme Bullying
High Conflict Divorce
Discrete (Single Incident) – Car
Accident/Dog Bite
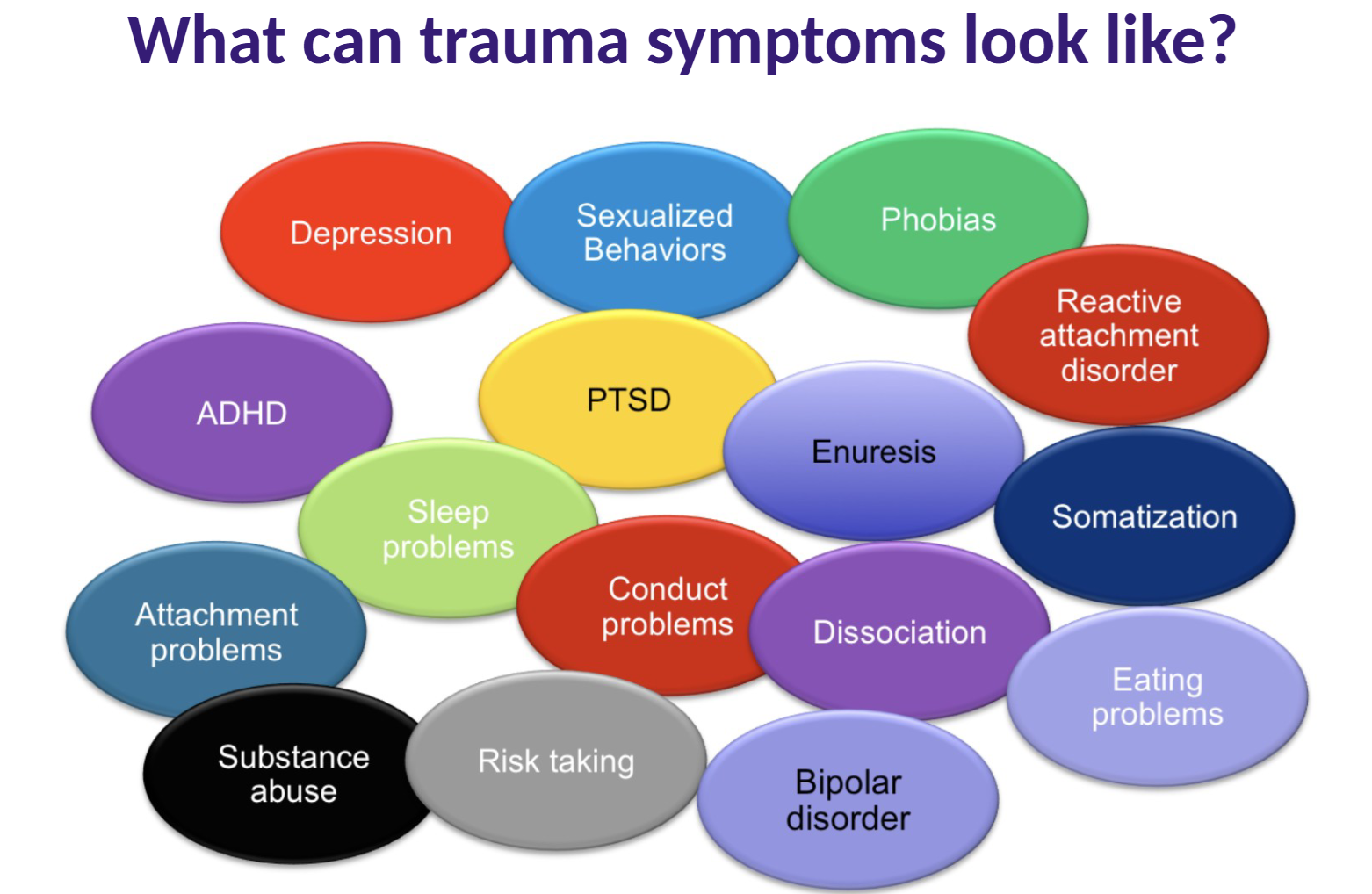
Effects of trauma
Disruption of healthy development
Higher risk of emotional and behavioral problems in the present and future
Trauma symptoms: attached image
Maltreatment
A person who is supposed to protect you from harm, keep you safe becomes a source of alarm/danger/pain
Maltreated children:
Tend to have lower social competence
Are less able to recognize their own emotional states
Have greater difficulty in recognizing other’s emotions
Have greater difficulty regulating their own emotions
Tend to over-read anger
Are more likely to be insecurely attached to their caregivers
Are frequently hypervigilant to threat
Child Maltreatment as a Risk Factor for School Problems
Greater than 50% of abused children have significant school problems (including conduct problems)
Greater than 25% of abused children require special education programs
Several studies suggest a history of trauma decreases IQ
Greater than 50% of abused children have significant school problems (including conduct problems)
Greater than 25% of abused children require special education programs
Several studies suggest a history of trauma decreases IQ
How and Possibly Why Does Childhood Maltreatment Exert Such Powerful Effects?
It occurs during sensitive developmental periods
It may be a way of helping the organism adapt to an anticipated dangerous, unpredictable environment (Kurt Fischer, 1997)
It impacts fundamental developmental processes:
Attachment
Emotional regulation
Impulse control
Integration of self
Socialization
Adverse childhood experiences
Vincent Felitti MD & Robert Anda, MD, MS
Kaiser San Diego’s Department of Preventive Medicine &
The Center for Disease Control (CDC)
17,000 patients participated (out of 26,000 adults asked to participate)
Began 1995 and followed long term for health outcomes
Results Revealed:
50% female
75% white
average age 57
75% college educated
100% employed
100% health insurance
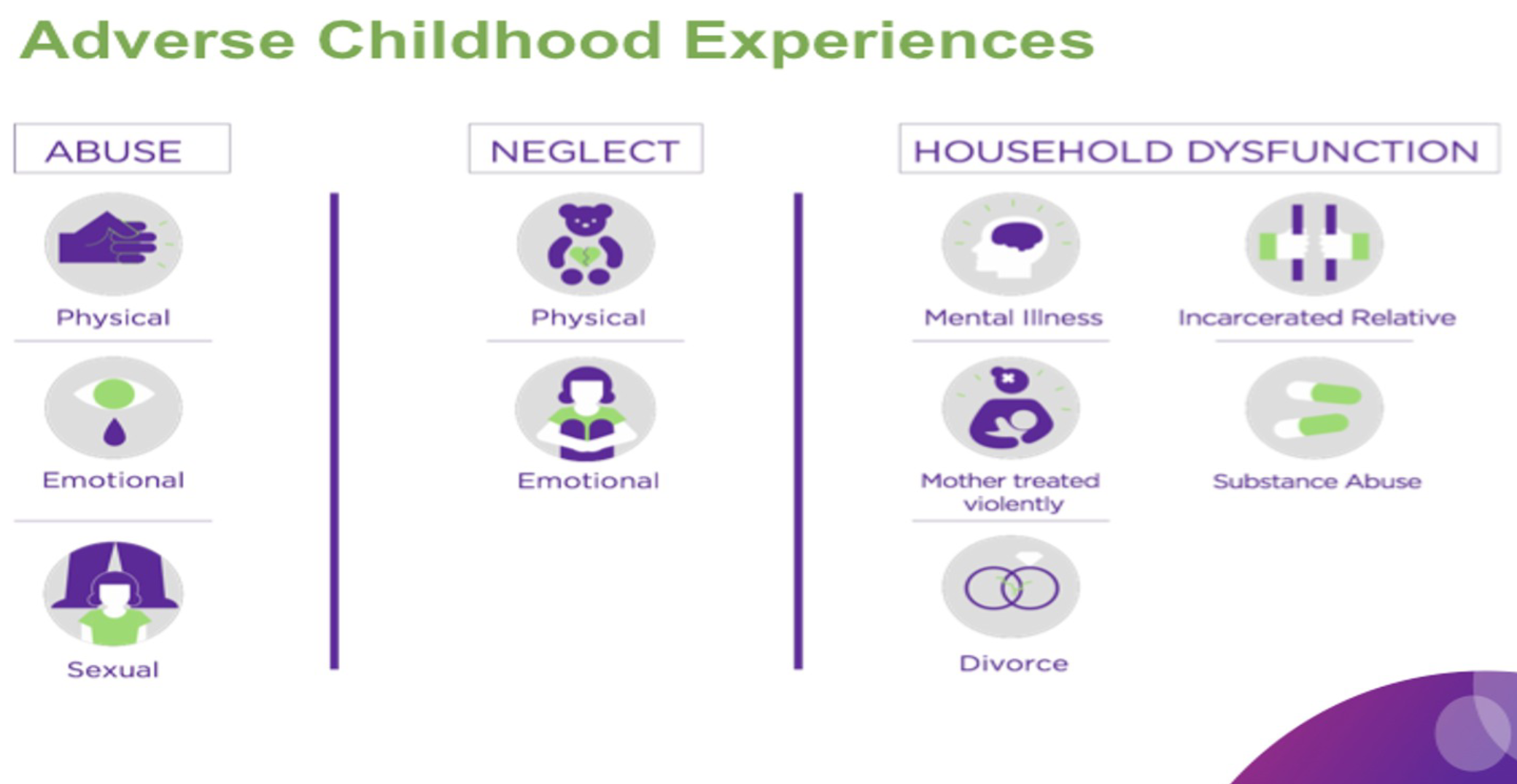
ACE Trauma Types
Household Dysfunction:
Substance abuse - 27%
Parental sep/divorce - 23%
Mental Illness - 19%
Mother treated violently - 13%
Incarcerated Relative - 5%
Abuse
Psychological - 11%
Physical - 28%
Sexual - 21%
Neglect
Emotional - 15%
Physical - 10%
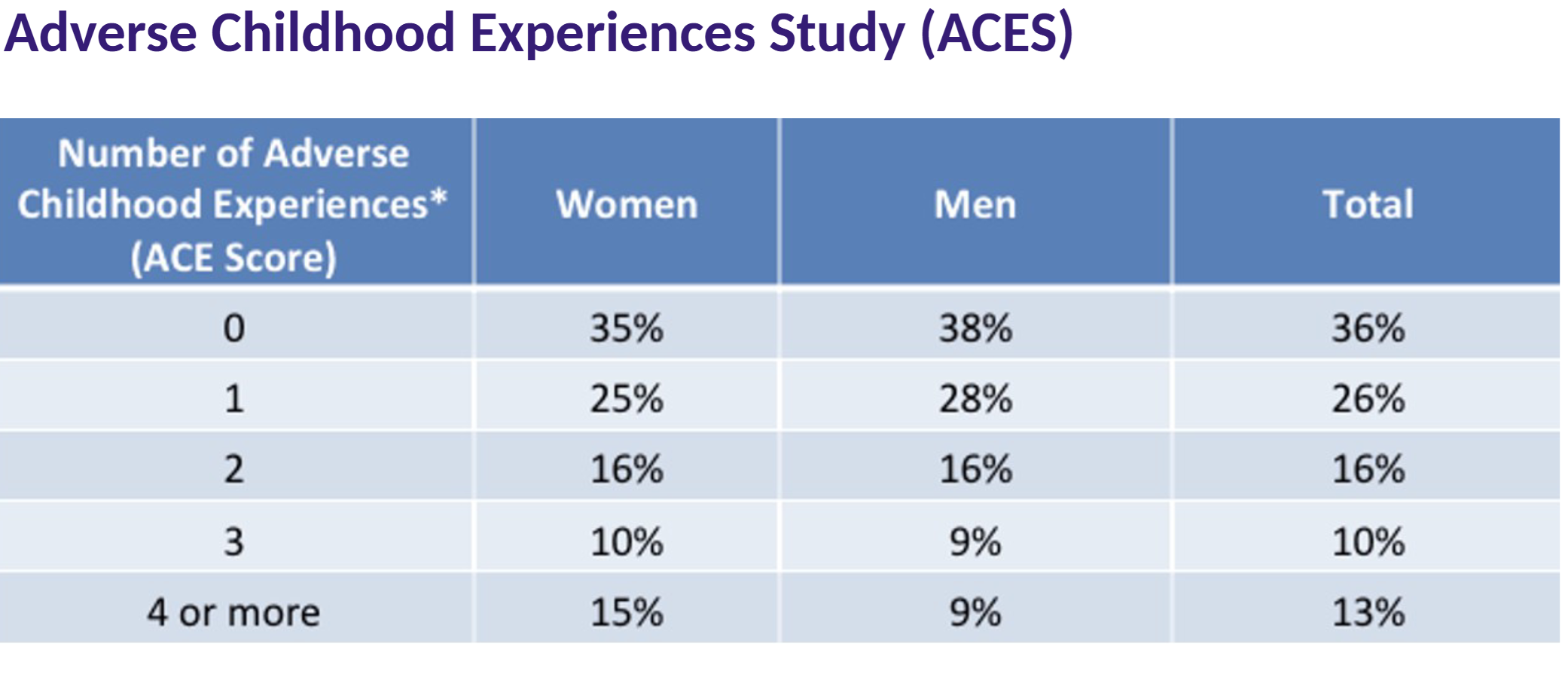
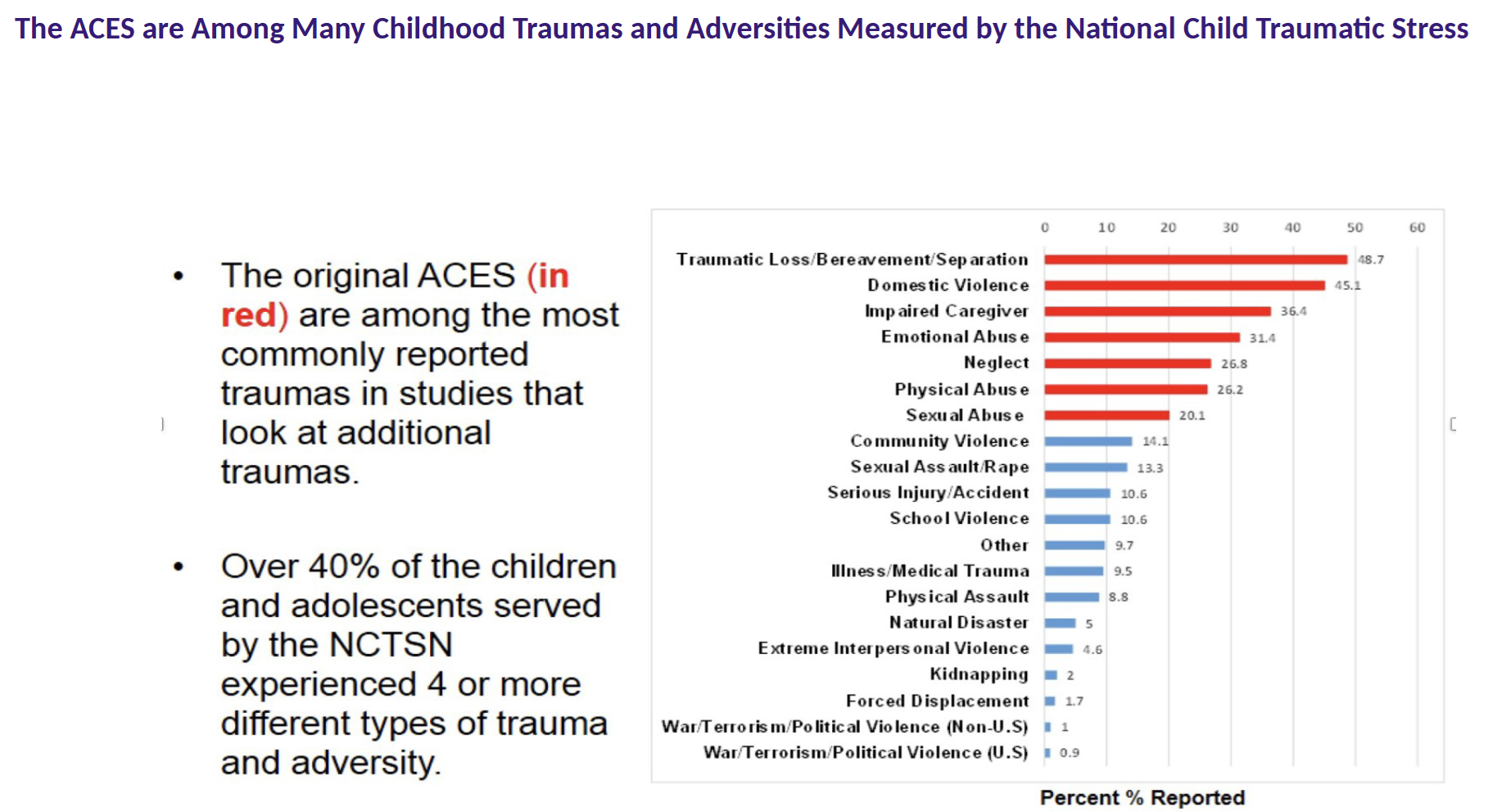
Beyond the Original ACEs Study
ORIGINAL ACEs Study
Surveyed middle-class, primarily white (non- Hispanic) individuals with some college education.
64% At least 1 ACE
12.5% 4 or more ACEs
Philadelphia Urban ACEs Study
Surveyed racially diverse sample of adults who completed high school.
83% At least 1 ACE
37% 4 or more ACEs
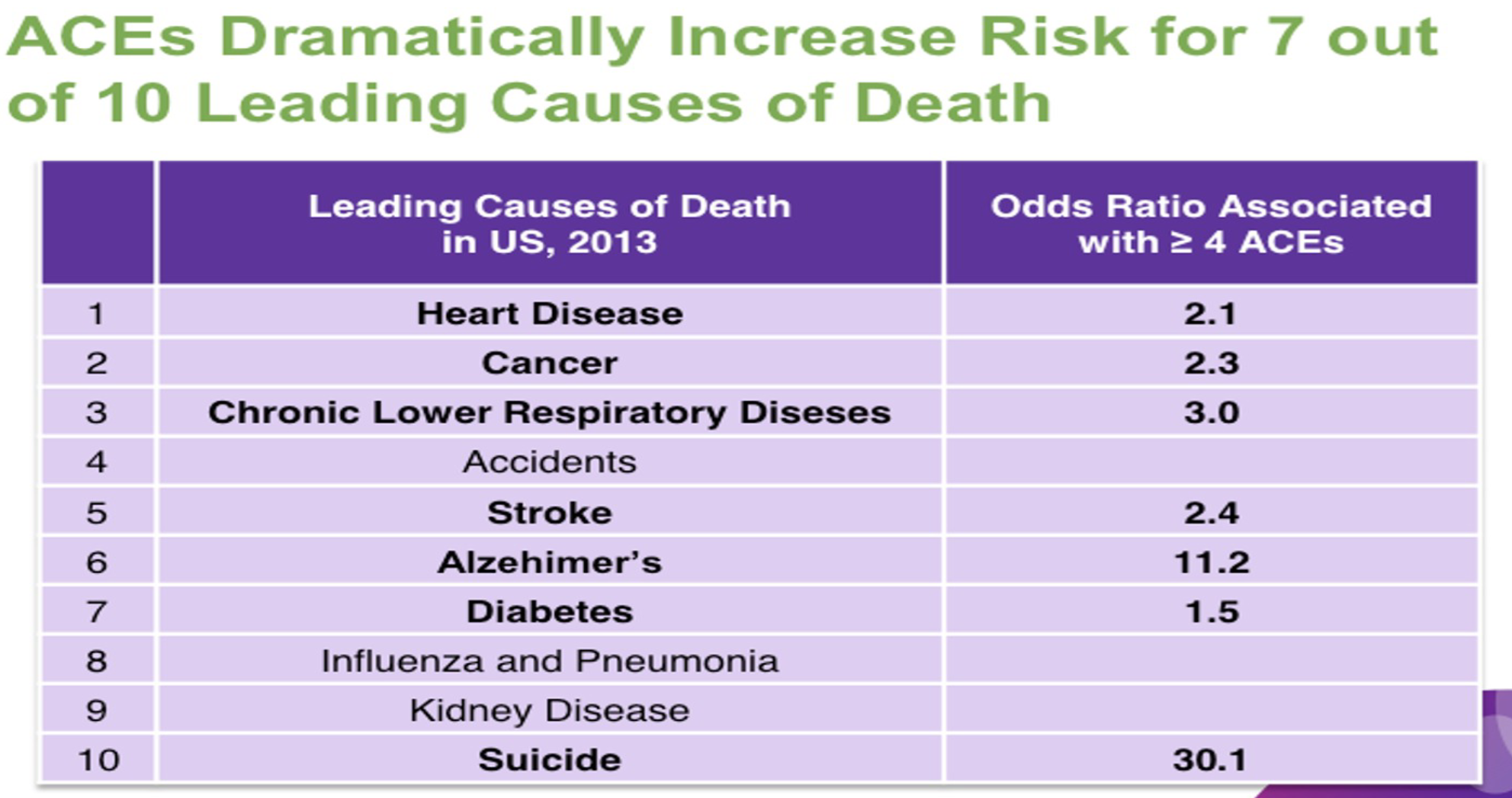
ACEs as a Risk Factor for Health
Multiple Adverse Childhood Experiences increase adjusted† odds ratios (= more likely to have) for:
Ischemic heart disease - 2.2 X's
Any cancer - 1.9 X's
Stroke - 2.4 X's
Chronic bronchitis/emphysema -3.9 X's
Diabetes - 1.6 X's
Hepatitis - 2.4’x
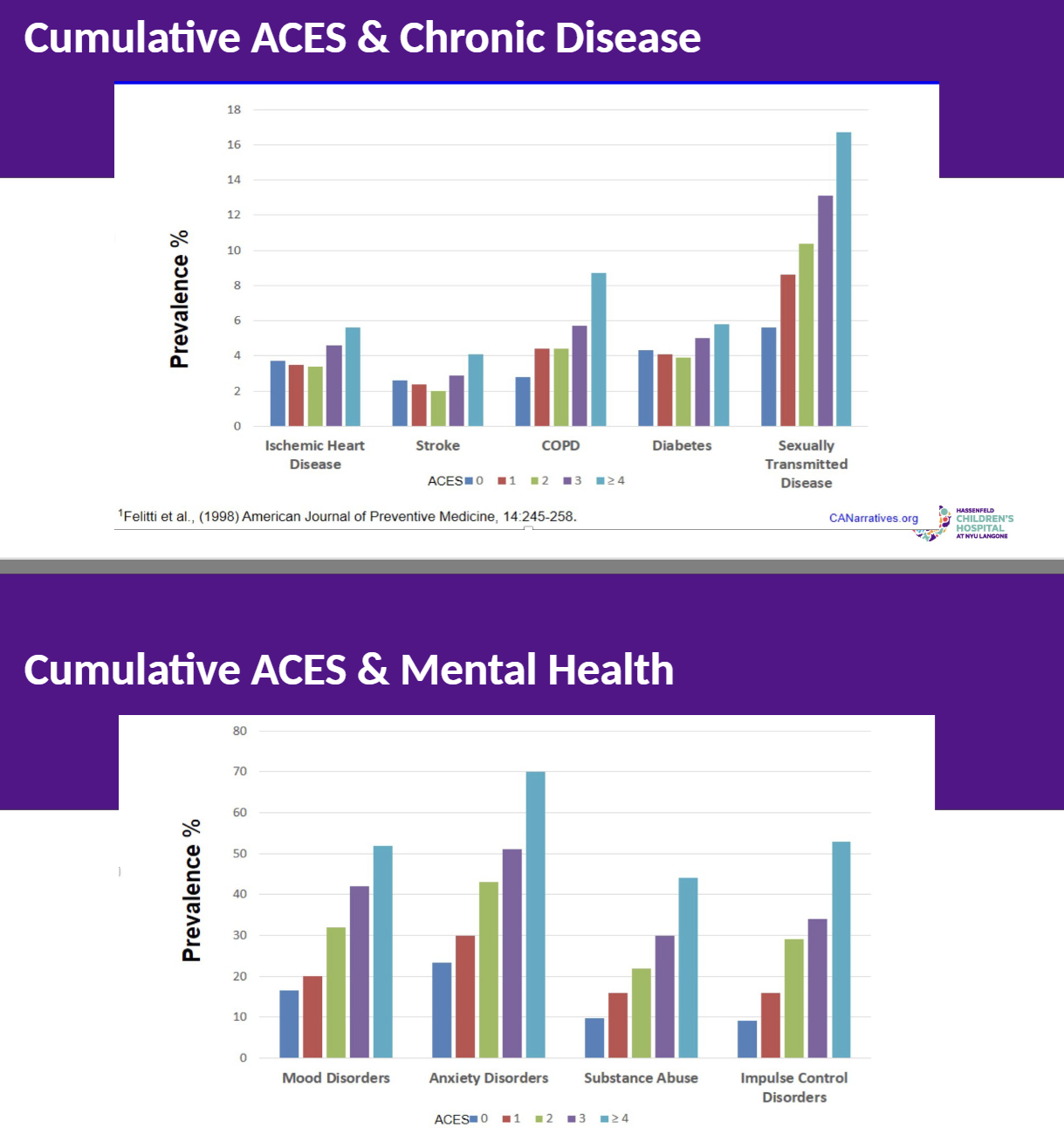
Cumulative ACES
Impact of Cumulative ACES & Social Dysfunction
Lower educational, occupational attainment
Increased social services cost
Increased Medical cost
Shortened life span
Increased risk for HIV, teen pregnancy, maternal depression
Intergenerational transmission of ACEs to offspring
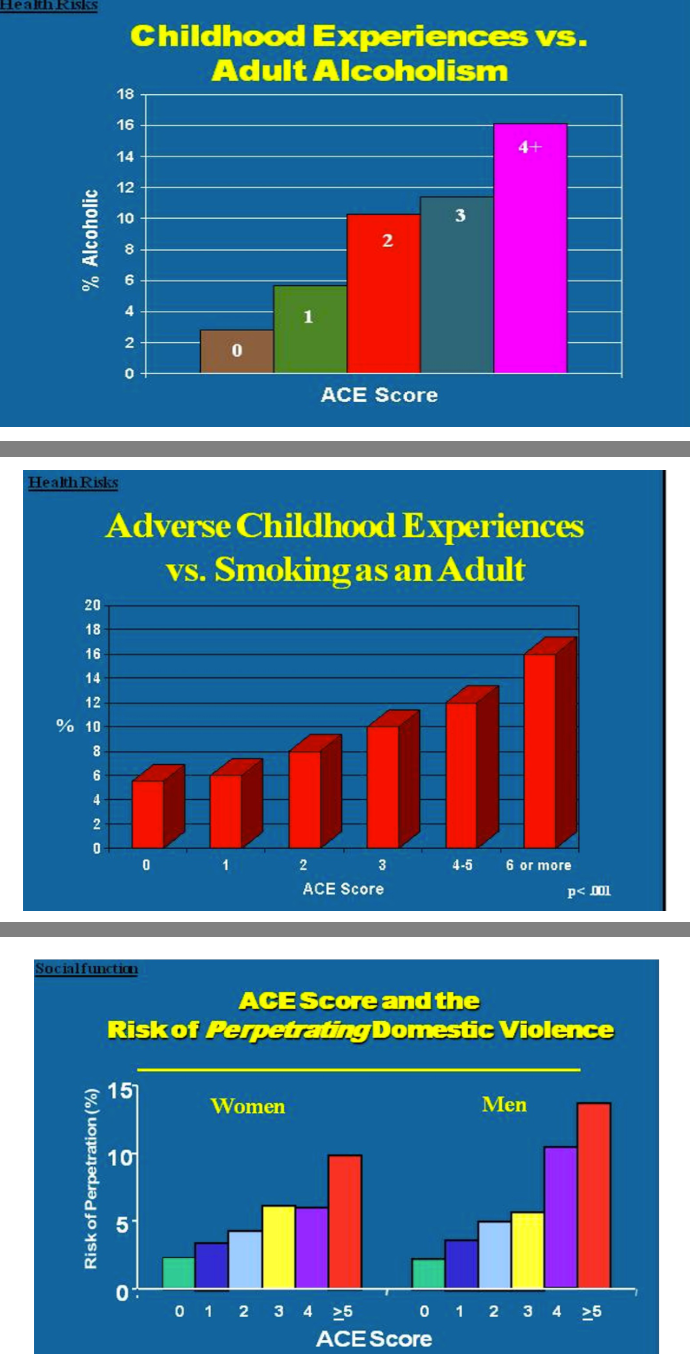
Implications of Cumulative ACEs
“Dose-Effect” - increasing ACES increases number of problems
Child Maltreatment victims have 2-7 times higher risk of being re-victimized in the future compared with non victims
Preventing ACES in previously traumatized children is an important intervention
Systems that serve traumatized children - e.g child protection, juvenile justice, mental health - should include trauma screening and prevention intervention
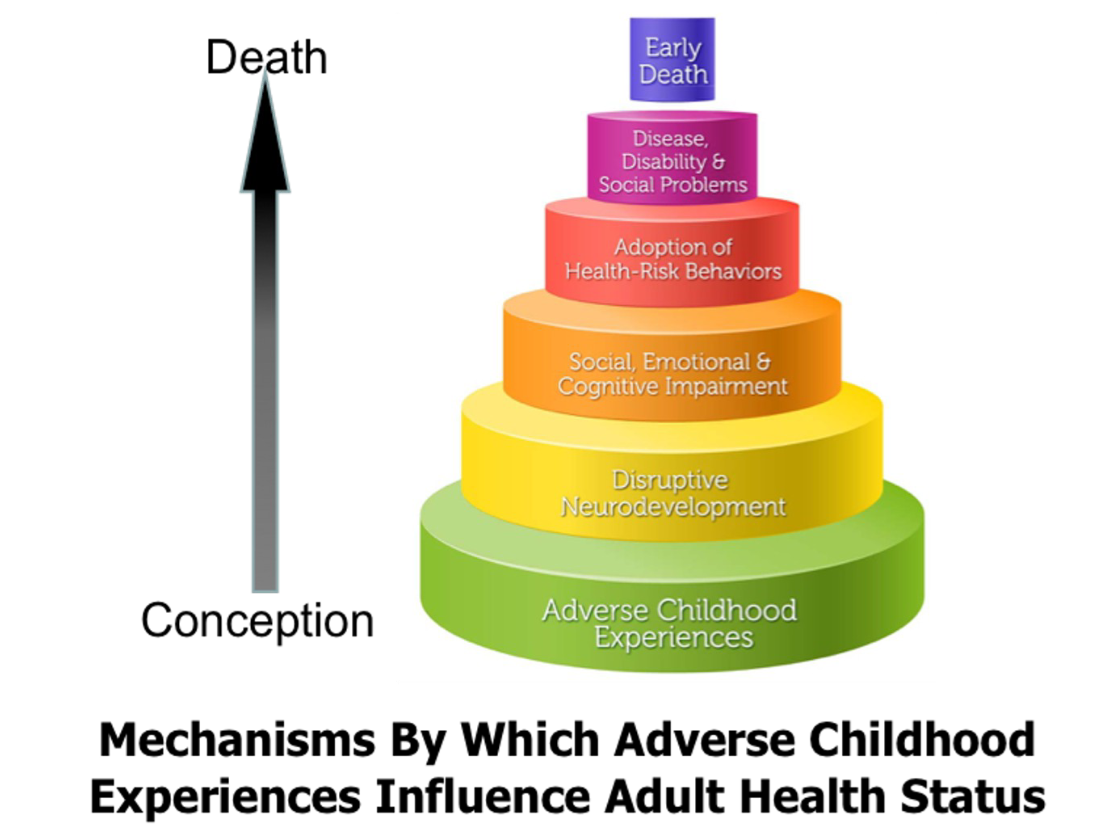
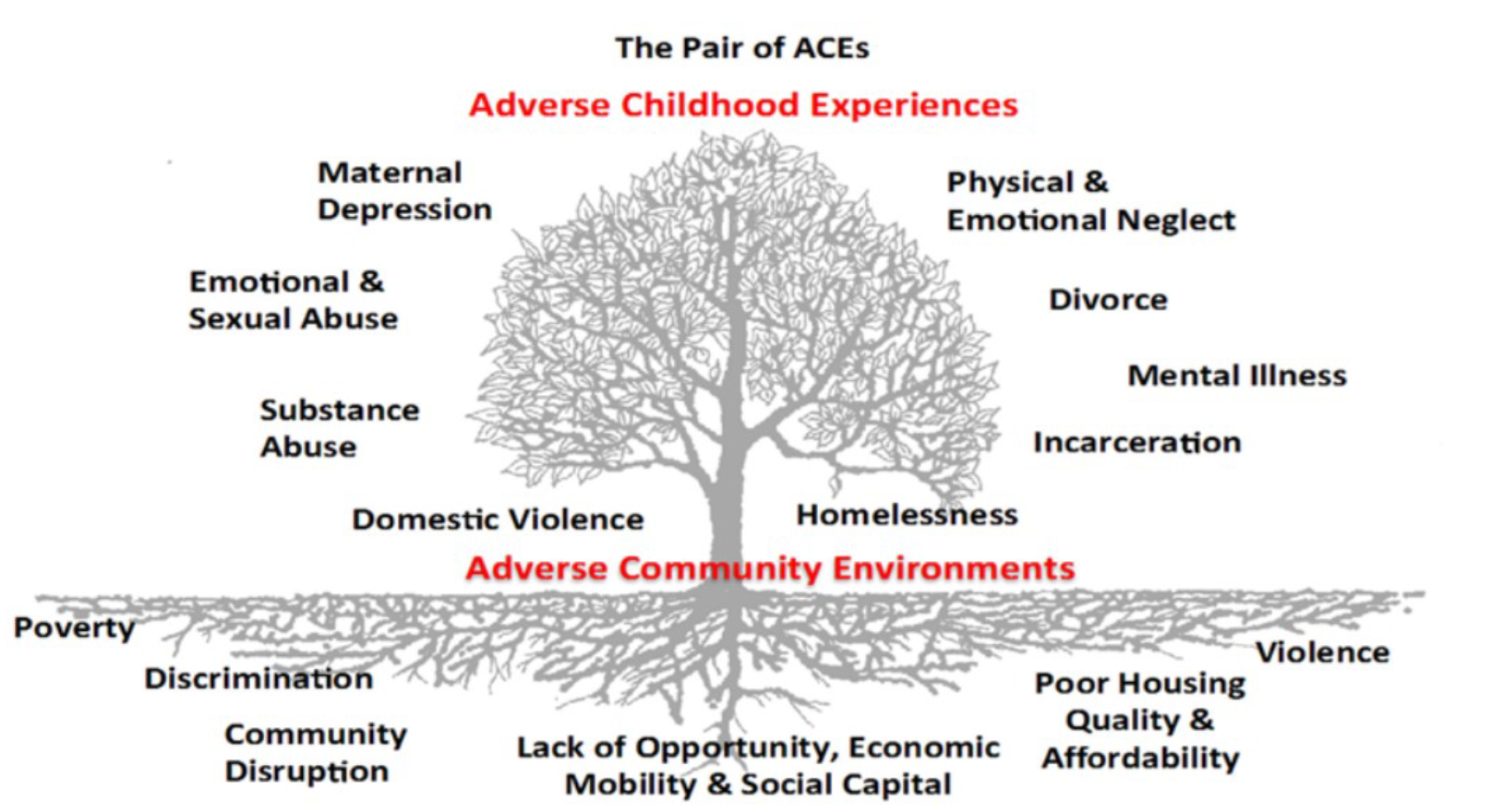
How ACES work
Adverse Childhood Experiences:
Abuse and Neglect (e.g psychological physical, sexual)
Household Dysfunction (e.g domestic violence, substance abuse, mental illness)
Impact on Child Development
Neurobiological Effects (e.g brain abnormalities, stress hormone dysregulation)
Psychosocial Effects (e.g poor attachment, poor socialization, poor self- efficacy)
Health Risk Behaviors (e,g smoking obesity, substance abuse, promiscuity)
Long-term consequences:
Major Depression
Suicide
PTSD
Homelessness
Drug Alcohol Abuse
Prostitution
Heart Disease
Criminal Behavior
Cancer
Unemployment
Chronic Lung Disease
Parenting problems
Sexually Transmitted Disease
High Utilization of health and social services
Intergenerational transmission of abuse
Examples of Differential Impact
Children exposed to a flood in Poland had rates of PTSD of 17.7%, 28 months after the event
On the other hand, A year post-wildfire, the rate of PTSD in children and adolescents has been found to be between 27 and 37%
What factors do you think might contribute to these different rates?
Proximity
Direct threat of loss of life or limb
Exposure to loss of life or limb among others, particularly loved ones
Time since the event
Availability of emergency relief and support services
Availability of a perceived way out, an escape
Premorbid nature of the population affected (high vs low risk– see next slide
Factors that ‘Increase’ Trauma Effects
Exposure to direct life threat
Injury (oneself) – extent of physical pain
Witnessing of mutilating injury/grotesque death (especially to family or friends)
Hearing unanswered screams or cries of distress
Being trapped or helpless
Unexpectedness or duration of the experience
Number and nature of threats during episode
Degree of violation of physical integrity of child
Degree of brutality and malevolence
Factors that Influence Trauma Effects
IQ
Presence/absence of supportive adult(s)
Ability to create/find safety
Previous trauma
Family history of psychological or substance abuse problems
Gender
Age
Low SES (socio-economic-status)
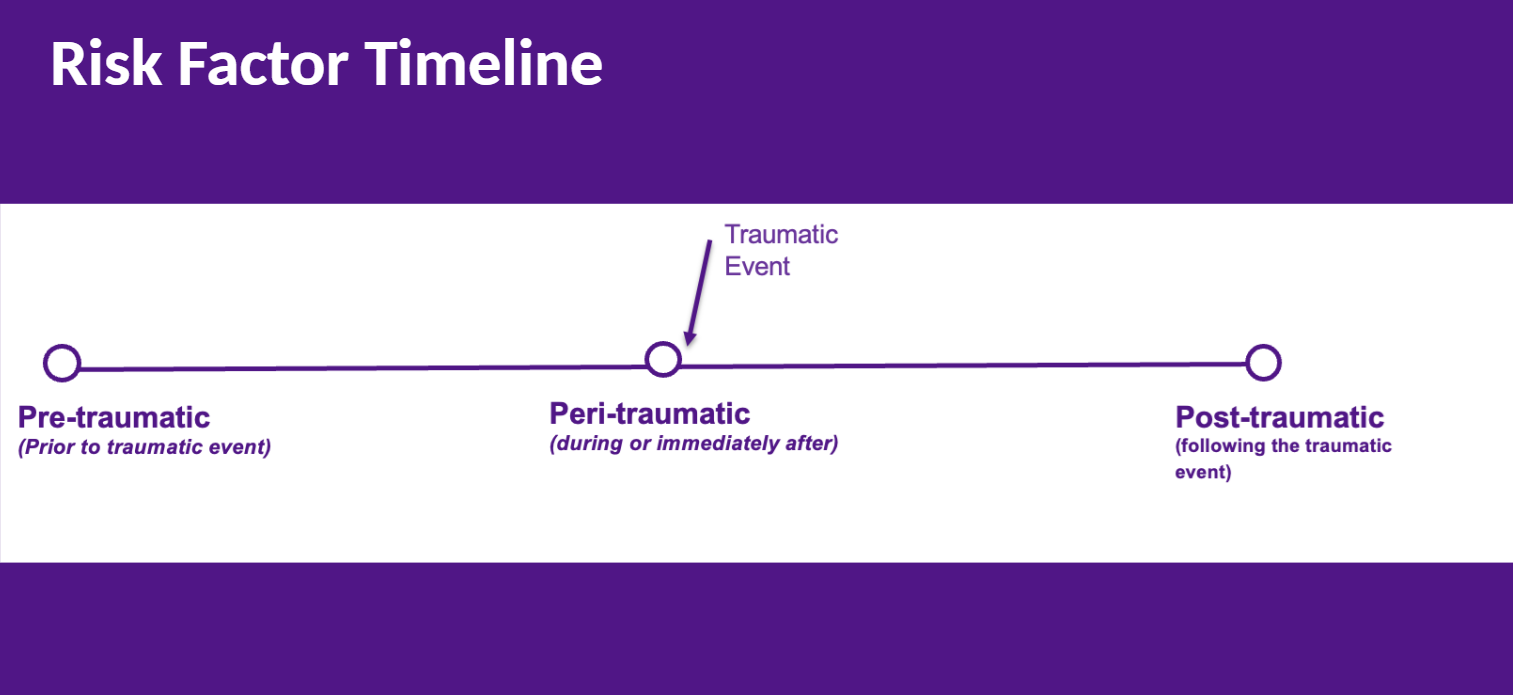
Risk Factor Timeline
Pre-traumatic Risk Factors
Quality of Attachment during early development
Neurobiological factors: Dysregulation of the Hypothalamic Pituitary
Adrenal axis (low cortisol levels, lack of reactivity, disruption of circadian rhythms)
Genetics and Epigenetics
Peri-traumatic Risk Factors(during or immediately after)
Duration and severity of the traumatic exposure
Uncertainty that the danger has passed
Post-traumatic Risk Factors
Sufficient access to needed resources
Real vs Perceived Social Support
Cognitive belief (i.e. a bad coincidence vs. trauma was deserved)
Physical activity, capacity to place attention elsewhere during critical period of memory consolidation
Memory reconsolidation and updating with reinforcement of trigger
A Developmental Psychopathology Perspective on Abuse and Neglec
Takes into account how trauma affects development & how development affects the outcome of trauma
Considers the interaction of the child, parent, and their environment
Examines the roles each play in the development of psychopathology
Considers Vulnerability and protective factors in the outcome of trauma
Developmental Psychopathology and Trauma
Studies have found that children who have been maltreated and/or neglected perform lower on developmental scales and on tests of intellectual and academic functioning (Erickson, et al, 1989)
A history of maltreatment and neglect has been found to be predictive of problems in expressive and receptive language (Allen et al, 1982)
Children who have suffered neglect and/or maltreatment are more likely to be placed in special education (Egeland et al, 2009)
For every additional ace, the risk of psychopathology augments geometrically
1 in 5 children in the US is raised below the poverty line, and is at greater risk for adversity (McLaughlin, 2017)
Children who have been maltreated or neglected AND WHO HAVE PARENTS WHO SUFFER FROM SIGNIFICANT PSYCHOPATHOLOGY are more likely to have insecure attachments and reactive attachment disorders (Egeland et al, 2007)
They are more likely to have negative mental representations of themselves and others (Toth et al, 2007)
They are more likely to have abnormal social interactions, including social withdrawal and aggression (Bousha et al and Egeland et al, 2007)
They have been found to have higher levels of pathological behaviors including tics, tantrums, stealing, somatic symptoms, and self injurious behaviors (Egeland et al, 2007)
What are the Essential Elements that Children Need to Develop Normatively?
Health: nutrition, hygiene, environment, healthcare, education, maternal health
Stimulation and the opportunity to interact with the environment in ways that support cognitive, motor, language, and social-emotional development
Stable supportive interpersonal relationships: attachment to a consistent primary caregiver
Adequate Nutrition
Undernutrition Results in:
Wasting (low weight-for-height), Stunted growth (low height-for-age) and Underweight (low weight-for-age)
1/2 of deaths in children under 5
Decreased cognitive, social, and emotional capacities
Behavioral dysregulation
Hunger in America
Facts about Child Hunger:
More than 13 million children experienced hunger in 2022
Black and Latino children are twice as likely to face hunger
33% of households headed by single moms experienced food insecurity
Hunger risks for development:
Physical: Stunted growth, abnormal brain development, low energy, increased susceptibility to infection
Emotional: Irritability, helplessness, depression, hallucinations, decreased ability to accurately assess reality
Cognitive: Difficulty with attention, concentration, decision making, acquiring new knowledge and memories, poor academic performance
Behavioral: Impulsivity, stealing, aggression
Education
Over 140 million children in developing countries have never attended school
122 million, or 48% of the out-of-school population, are girls and young women
Educated children are more likely to be productive in the home and in the workplace
Educated children are less likely to be victims of abuse and exploitation
Adequate Healthcare
An estimated 5.2 million children under 5 years died mostly from preventable and treatable causes. Children aged 1 to 11 months accounted for 1.5 million of these deaths while children aged 1 to 4 years accounted for 1.3 million deaths. Newborns (under 28 days) accounted for the remaining 2.4 million deaths
Leading causes of death in children under-5 years are: preterm birth complications, birth asphyxia/trauma, pneumonia, congenital anomalies, diarrhoea and malaria, all of which can be prevented or treated with access to simple, affordable interventions including immunization, adequate nutrition, safe water and food and quality care by a trained health provider when needed
Six million children who die each year could be saved by low-tech measures such as vaccines, antibiotics, insecticide-treated bed nets and improved breastfeeding practices
Maternal Health
A woman dies from complications in childbirth every minute – the vast majority of them in developing countries
At least 20% of the burden of disease in children below the age of 5 is related to poor maternal health and nutrition, as well as quality of care at delivery and during the newborn period
Environmental Health
More than 1,300 children under the age of five die every day because of diseases caused by unsafe drinking water, poor sanitation and hygiene
These diarrhoeal diseases include cholera and dysentery
Unsafe drinking water also puts children at risk of malnutrition, as well as the risk of contracting typhoid and polio
400 million children have no access to clean water
Temperament
Easy:
Biological regularity
Positive approach to most situations
Easy adaptability to change
Mild or moderately intense mood that is predominantly positive
Difficult:
Biological irregularity
Negative withdrawal from most new situations
Slow adaptability to change
Intense mood that is predominantly negative
Slow to Warm:
Negative response to new situations
Slow adaptation
May have good biological regularity
Mild expressions of mood
Characteristics of Temperament
Activity Level
Regularity
Approach or Withdrawal
Adaptability
Sensory Threshold
Quality of Mood
Intensity of Reaction
Distractibility
Persistence and Attention Span
Early Brain Development
Brain at birth weighs about 1/3 of adult brain
83% of dendritic growth occurs after birth
By age 2-3 years, the brain is 80% of adult brain size
By age 5, the brain is 90% of adult brain size
The Experience Dependent Brain
Synapses are overproduced
Pruning of synapses takes place from early childhood through adolescence
The least used synapses are pruned
Experience determines which synapses will be the most used – therefore retained
Pruning makes our mental processes more streamlined and coherent
Origins of Attachment Theory- John Bowlby
British psychoanalyst and psychiatrist
Early work with institutionalized “juvenile delinquents” (“44 Juvenile Thieves”)
Established the Separation Research Unit in 1948 at the Tavistock Clinic (where he was Deputy Director)
Interest in the “Ill effects on personality development of prolonged institutional care and/or frequent changes of mother-figure during the early years of life” (Bowlby, 1988)
Findings:
“Deprivation” could result from separation from the primary caregiver or from a cold, inconsistent relationship with the primary caregiver
Prolonged exposure to “Deprivation” could have lasting effects on the child
The World health organization invited Bowlby to study maternal deprivation and in 1951 he published “maternal care and mental healt
Konrad Lorenz - Imprinting
Austrian zoologist, ethnologist, and ornithologist, founder of Ethology
Studied instinctive behavior in animals (1930s)
Gave the name “Imprinting” to the behavior of Greylag Goslings who followed the first moving object they saw after hatching
Imprinting occurs during a 12-17 hour “critical period” after hatching – suggesting that “attachment is innate” (Hess, 1958)
If no attachment has developed within 32 hours, it is unlikely that any attachment will ever develop (Hess, 1958)
Shift to Direct Child Observation 1940s/1950
WWII parent-child separation in London (Anna Freud & Dorothy Burlingham, 1944)
Phases of Response to Hospitalization and Parent-Child Separation (A Two Year Old Goes to Hospital (documentary)
Protest
Despair
Detachment
Comfort > Food
Wire Mother vs. Cloth Mother
John Bowlby: A Theory of Motivation and Behavior
Psychoanalysis
Ethology
Evolutionary Biology
Control Systems Theory
Cognitive Science
Direct Child Observation
Primate Research
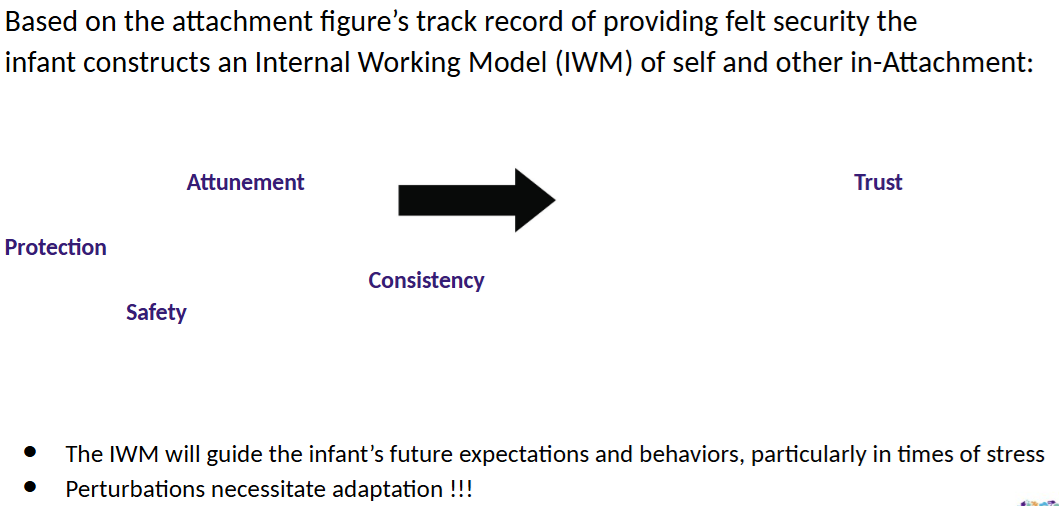
Attachment Behavioral System
A Caregiver-infant behavioral system that insures species survival
The Centrality of Threat / Fear
A Purposeful goal of achieving “Felt-Security”
Attachment Behavioral System
Proximity-Seeking When There Is Threat vs. Exploration When There Is Safety
Infant Attachment Behavioral System:
Cry, grasp, babble, smile, cling, protest separation, visual checking/following, following by crawling/walking
Caregiver Behavioral System:
Watchfulness, protective behavior, response to distress, closeness
Multiple Attachments
Attachments are consolidating between 6 and 24 months of age
Definitive attachment preferences are established by 18-24 months of age
Children will develop an Attachment relationship to any caregiver providing regular care, regardless of the quality of the care provided. Play partners are not necessarily attachment figures
Children may have multiple Attachment figures (e.g. mother, father, grandmother, nanny, day care provider)
The quality of Attachment to each of these significant figures can be hierarchical (per need) and different (e.g. secure, insecure, disorganized)
Secure Attachment to at least one significant caregiver is considered to be a buffering agent against stress
Mary Ainsworth 1913-1999
Canadian psychologist who began her career as a research assistant to John Bowlby
Studied children in Kampala, Uganda and made careful observations of mother-child interaction, published “Infancy in Uganda” (1967)
Back in the United states, initiated a study of middle-class babies and their mothers in Baltimore, Maryland
The “Strange Situation”
Ainsworth visited the homes of Baltimore families every 3 weeks from birth
At 12 months she began to consider how the manner in which infants coped with separation, and behaved upon reunion, reflected the quality of the caregiver-infant relationship
Ainsworth created “The Strange Situation”, a research paradigm consisting of 8 episodes, 3 minutes each
First separation mother leaves the child with a stranger
Second separation mother leaves the child alone
Ainsworth developed a coding system to categorize the child’s pattern of attachment behaviors as reflective of the quality of caregiver-infant attachment relationship
Patterns of Attachment: Behavioral adaptations to manage stress/felt-anxiety/fear
Organized:
Secure (B)
Insecure Avoidant
Insure Ambivalent
Disorganized/Disoriented (D)
Attachment Classifications
Secure:
Distressed, seeks contact, easily soothed, returns to play
Parent is responsive and available
Insecure-Avoidant:
Not overtly distressed, ignores or turns away, does not resume prior level of play
Parent is unavailable and rejecting
Insecure-Ambivalent:
Distressed, seeks then angrily rejects contact, not soothed, does not return readily to play
Parent is inconsistent, unreliable, sometimes intrusive
Disorganized:
Distressed, approach/avoid, mistimed, incoherent, freezing
Irresolvable dilemma: Parent is source of security AND ALSO source of fear, typically associated with parental trauma and maltreatment