16 - management of ocular pain
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
What are common causes of acute ocular pain?
1. conj or corneal foreign body
2. conj or corneal abrasion
3. iritis
4. HZO
5. post-surgical → PRK, PTK, superficial keratectomy
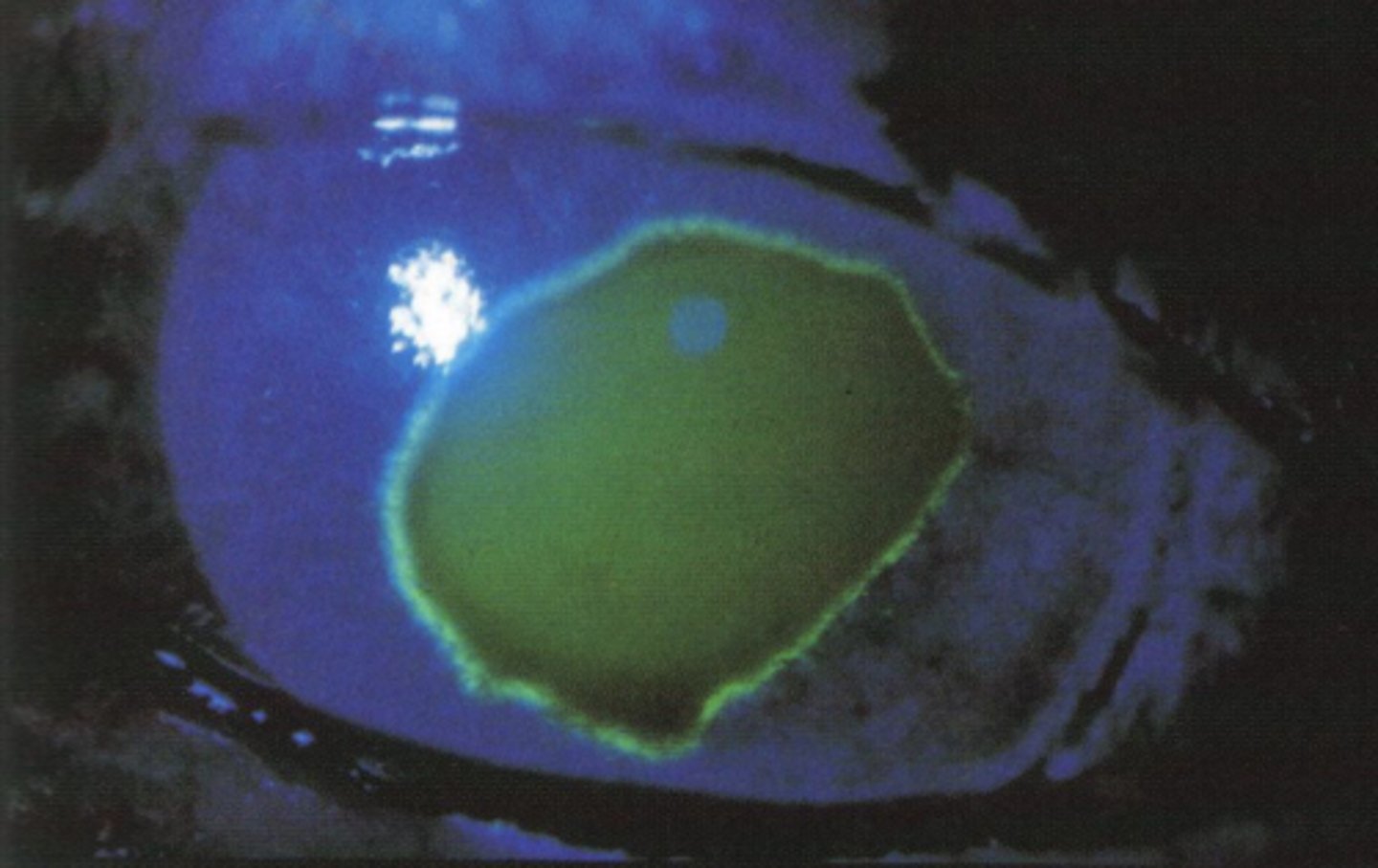
image - corneal abrasion
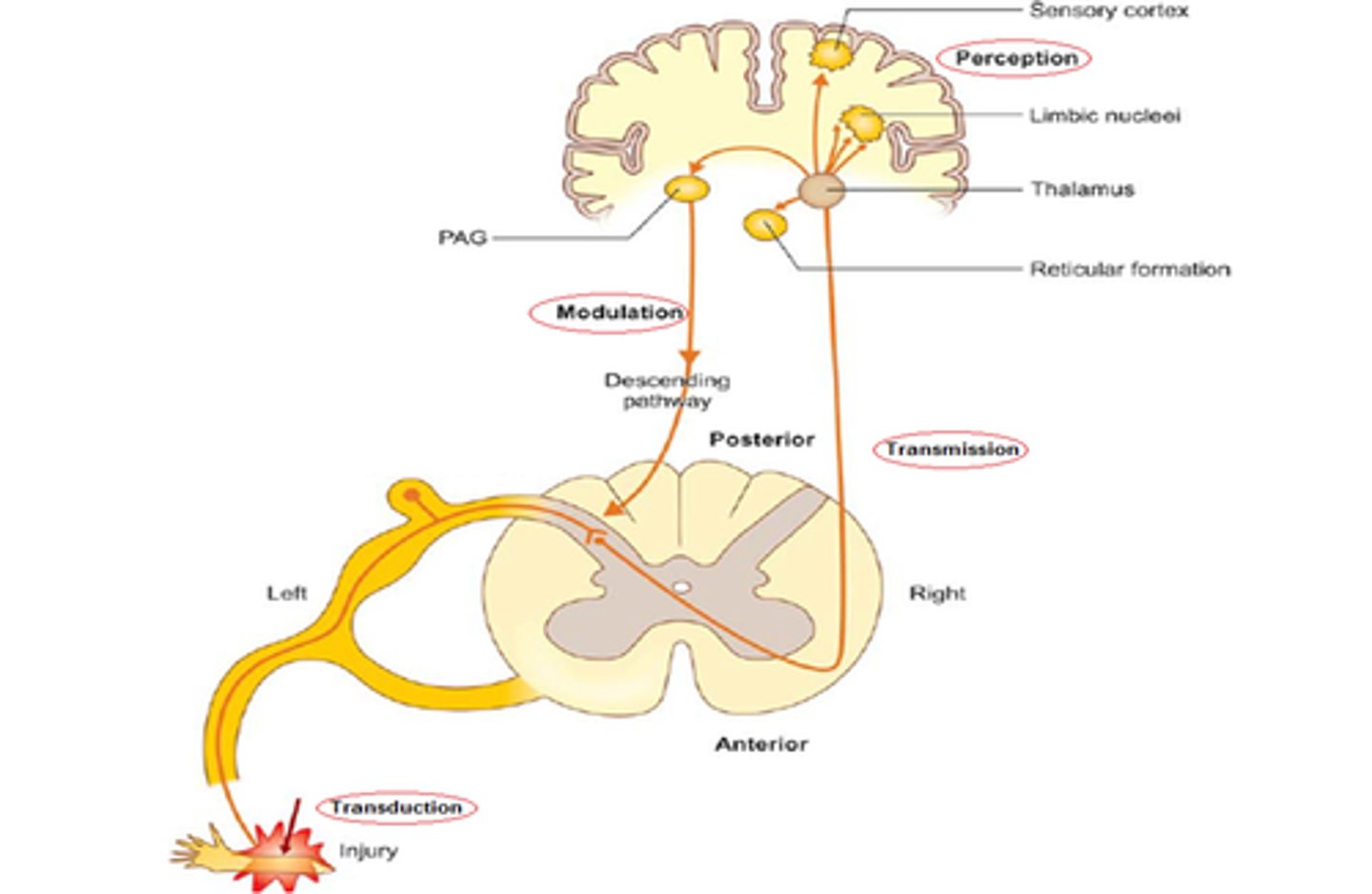
what are nociceptors?
specialized nerve endings in the tissue that transmit pain signals
where does nociceptor activation transmit signals to?
cerebral cortex
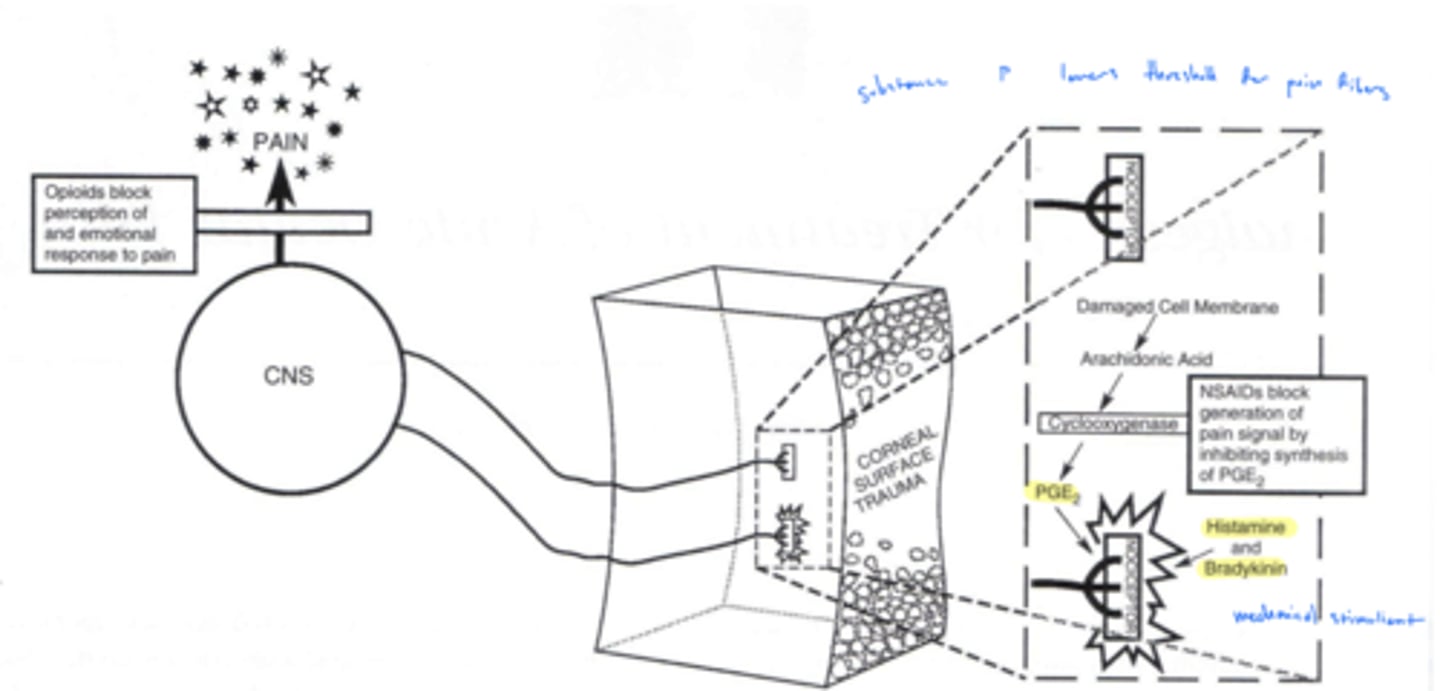
What activates nociceptors?
substance P
What enhances/stimulates substance P activity?
arachidonic acid metabolites → prostaglandins
When is a pain signal felt?
only if it is fully received and processed in the cerebral cortex
What are the 3 categories of drugs for pain management?
1. peripheral acting agents
2. signal inhibiting agents
3. central acting agents
What do peripheral acting agents for pain do?
1. inhibit substance P directly → ↓ nociceptor activation
2. inhibits prostaglandin synthesis to prevent sensitization to substance P
substance P is enhanced by arachidonic acid metabolites
What are examples of peripheral acting agents for pain?
1. capzasin
2. NSAIDs
How does capzasin block pain?
inhibits substance P directly to decrease nociceptor activation
typically only used for joint pain or HZO
How do NSAIDs block pain?
reduce arachidonic metabolites (prostaglandins) which prevent the sensitization of receptors to substance P
What do signal inhibiting agents for pain do?
prevent pain signal (action potentials) from traveling to cortex
What is an example of a signal inhibiting agent for pain?
anesthetics
not therapeutic agents
What do central acting agents for pain do?
act on pain perception centers in the cortex
What are examples of central acting agents for pain?
1. acetaminophen
2. opioids
What are the advantages of using topical NSAIDs for pain?
direct application to site of injury/inflammation:
1. limits side effects
2. MOA takes place in PNS → acts directly at nociceptor
What are the uses of topical NSAIDs for pain?
1. post refractive/cataract surgery
2. post FB removal
3. pre/post betadine tx - typically surgical disinfectant
4. bullous keratopathy
5. corneal hydrops
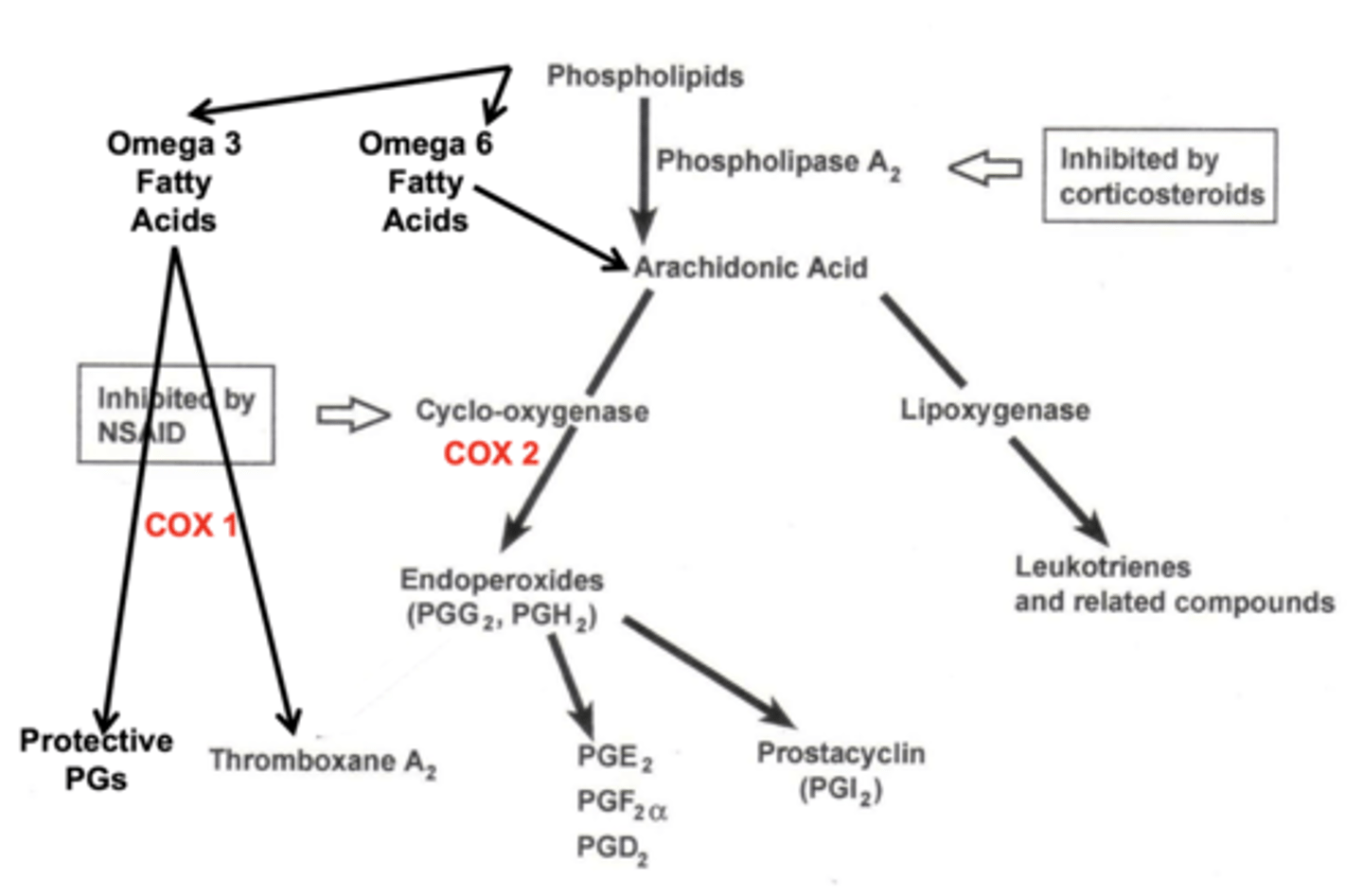
What is the MOA of oral NSAIDs? What are their effects?
cyclo-oxygenase inhibitors that prevent/decrease the formation of prostaglandins (PGE₂ for pain) to carry out:
1. analgesic
2. anti-inflammatory
3. anti-pyretic
4. anti-platelet effects
What oral NSAIDs are used for acute ocular pain?
1. Ibuprofen 400-600mg PO QID
2. Ketoprofen 50 mg PO q6-8hr
3. Naproxen sodium 250-500mg PO BID
what is the maximum amount of ibuprofen that can be ingested?
2400 mg/24 hrs
what is the DOC for acute ocular pain?
Ibuprofen 400-600mg PO QID → fastest onset of action
what is the second DOC for acute ocular pain?
Ketoprofen 50 mg PO q6-8hr
what is the third DOC for acute ocular pain?
Naproxen sodium 250-500mg PO BID
how to reduce GI effects of oral NSAIDs?
take oral NSAIDs with food
why? - NSAIDs can decrease healthy prostaglandins of the stomach
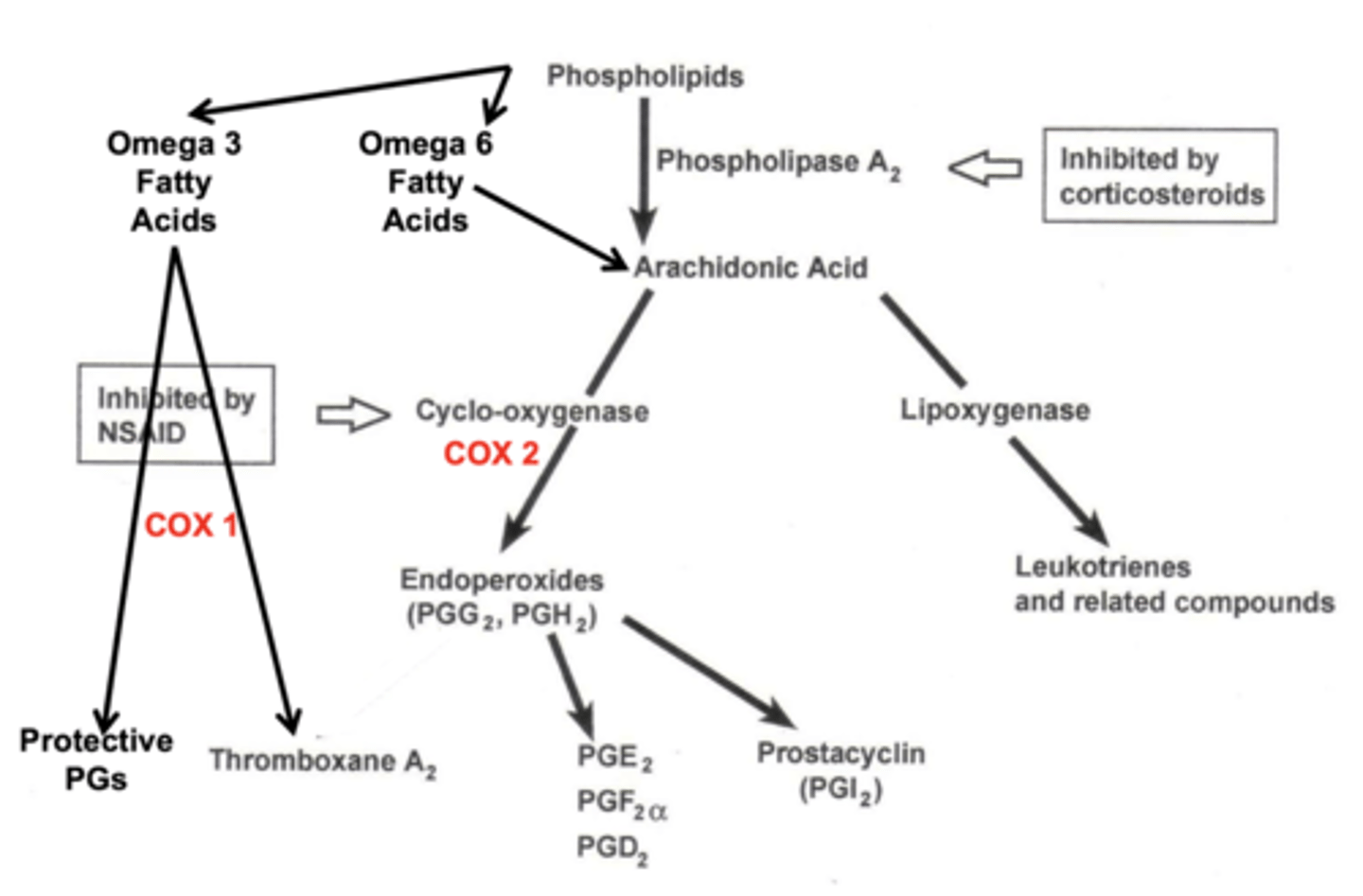
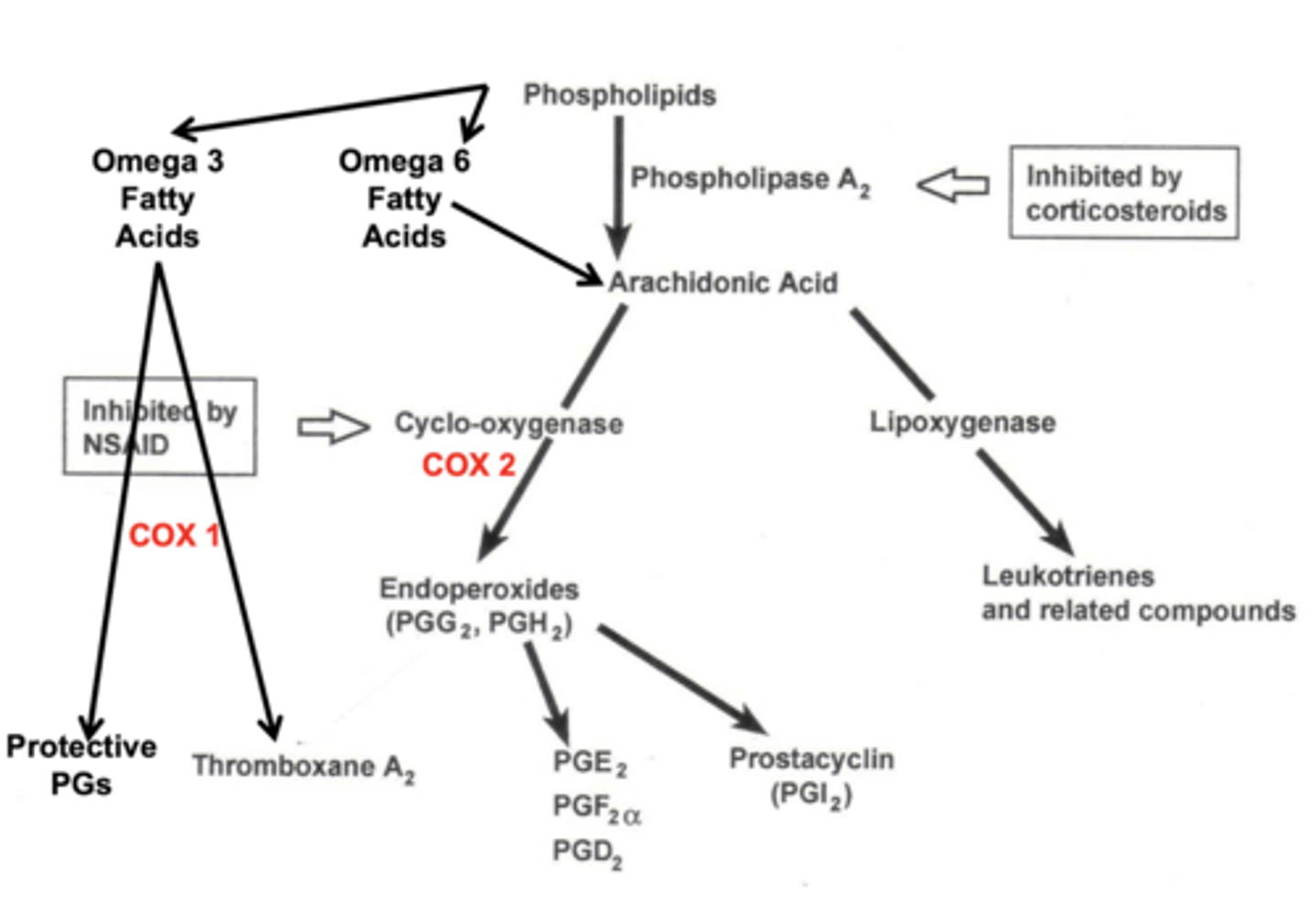
Which COX pathway creates the protective prostaglandins (starting fatty acid & enzyme)?
omega 3 fatty acid (from phospholipids) & COX-1
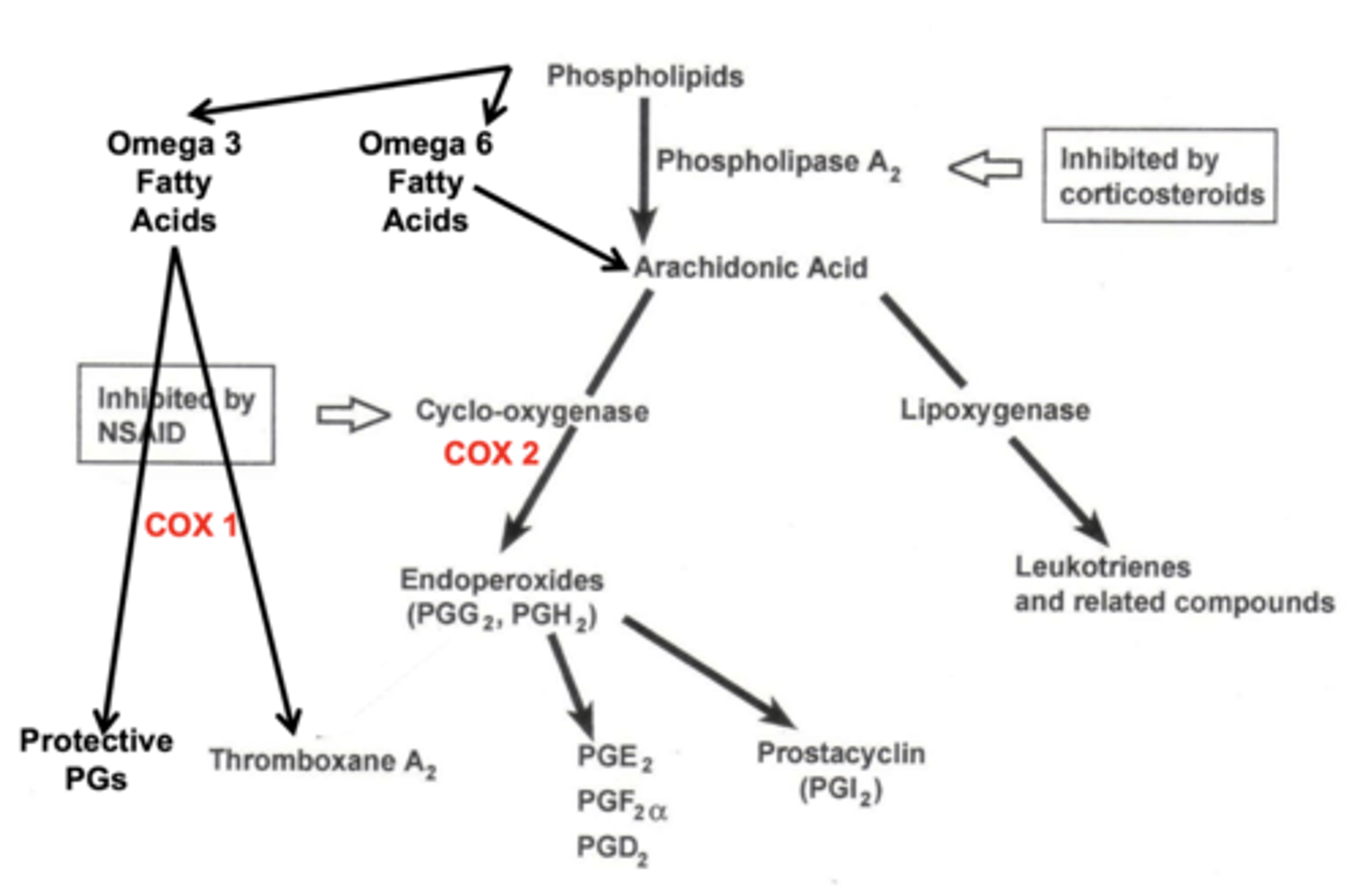
Which COX pathway creates the endoperoxides (painful) prostaglandins (starting fatty acid & enzyme)?
omega 6 fatty acid (from phospholipids) & COX-2
What is the ceiling effect and what drug does it occur with?
beyond a certain dosage → no further therapeutic effect is realized
seen with oral NSAIDs
What are the side effects of oral NSAIDs?
1. hemorrhage
2. gastric distress, heartburn, duodenal ulcer
3. nephrotoxicity
what are the contraindications for oral NSAIDs?
1. hyphema - rebleed
2. gastic/peptic ulcer
3. renal insufficiency of CHF
4. pregnant/nursing mothers
5. no aspirin for children d/t risk of Reye's Syndrome
what is the MOA of acetaminophen?
unknown CNS effect → some impact on cortex
What is the therapeutic effect of acetaminophen?
1. analgesia (anti-pain)
2. anti-pyretic (anti-fever)
no effect on inflammation or platelets
when do you prescribe acetaminophen?
if pt is contraindicated for NSAIDs
What are the side effects of acetaminophen?
liver toxicity if exceed recommended dosage or if in alcoholic or known liver disease
What is a contraindication of acetaminophen?
chronic alcoholics
What are advantages of acetaminophen?
1. no GI SE
2. no anticlotting/bleeding effects
3. safe for kids and pregnancy
4. no cross reactivity with NSAIDs
What are disadvantages of acetaminophen?
1. liver toxicity
2. no effect on inflammation
What must you make sure to tell your patient when prescribing acetaminophen?
do NOT follow package instructions → may take med every 6 hours but do NOT exceed 2000mg in 24 hours
package says 3000mg
what is a typical dose of acetaminophen?
325-1000 mg PO q6h
How should oral NSAIDs and Tylenol be prescribed before using opiates?
exhaust pain management by switching between NSAIDs and acetaminophen (switch every ~4 hrs)
AM - NSAID
Noon - Tylenol
early PM - NSAID
late PM - Tylenol
What is the MOA of opioids?
alters CNS perception of pain via 3 receptor types → mu, kappa and delta
What are the opiates/opioid analgesics derivatives of (aka pharmacology)?
all derivatives of opium flower
what is the prototypical agent of opiates/opioid analgesics?
morphine
What does receptor Mu do?
1. supraspinal analgesia
2. sedation
3. respiratory depression
what does receptor kappa do?
spinal analgesia
what does receptor delta do?
relatively unknown effects
What are the ocular indications of opioid use?
SEVERE, acute pain from:
1. severe corneal abrasion or FB
2. post-PRK or other corneal surgery
3. HZO + post-herpetic neuralgia
if non-opioid analgesics have failed to work
What are the side effects of opioids?
1. constipation → OIC (opioid induced constipation)
2. dry mouth
3. nausea
4. sedation, dizziness, weakness
5. respiratory depression → can be fatal
6. addiction/dependence → d/t euphoric effects (not for every patient)
top 5 are parasympathetic inhibiting
What are the contraindications of opioids?
1. asthma, COPD → beware of sleep apnea
2. pregnancy
3. an unidentifiable cause of pain → could be drug seeker
What should you tell your patient when prescribing opioids?
1. take with food to decrease GI effects
2. avoid driving or other activities requiring alertness
3. avoid alcohol + muscle relaxants
How are DEA controlled substances ranked?
based on abuse/dependency - schedule 1 worse than 5
schedule 1 - very high abuse potential
schedule 5 - limited abuse potential
What opioid controlled substances can be prescribed by Ohio ODs?
1. tramadol
2. ≤60mg of codeine
3. ≤7.5mg of hydrocodone
total quantity prescribed must not exceed a 4 day supply per episode of illness, injury and/or tx
What is the total quantity limit of opioid controlled substance for ODs in Ohio?
shall not exceed a single 4 day supply of opioid substance per episode of illness, injury and/or treatment → no considered primary care anymore!
What is the trade name of tramadol?
ConZip
how does tramadol compare to codeine?
1. synthetic analog of codeine
2. low addiction potential but same SE of codeine
What must you be aware of when prescribing tramadol?
make sure patient is not on antidepressant → DDI
if they are, make sure they do not take it for the few days they are taking tramadol
What is the dosing for tramadol?
50-100mg PO q4-6h
What is a tramadol combination drug?
37.5mg tramadol + 325mg acetaminophen
What is dosing for 37.5mg tramadol + 325mg acetaminophen?
2 tabs PO q4-6h
What is the max dose for 37.5mg tramadol + 325mg acetaminophen combo drug?
8 tabs in 24hours
What schedule drug is tramadol?
Schedule IV
Which opioid should you prescribe first (if all other treatment has failed)?
Tramadol - higher schedule (4), less dependency/abuse potential
what is codeine?
prodrug of morphine
What schedule drug is codeine combo drugs?
Schedule III
What are the formulations of codeine?
15 mg of codeine + 300 mg acetaminophen
30 mg of codeine + 300 mg acetaminophen
60 mg of codeine + 300 mg acetaminophen
only available in generic forms!
what is the dosage for codeine?
30-60 mg PO q4-6 hrs
What schedule drug is hydrocodone?
Schedule II
What is a benefit to hydrocodone?
1. less constipation
2. less side effects
3. more euphoria (possibly) → 6x more potent than codeine
much lower dosage could be the reasons
what is the dosage of hydrocodone?
5-7.5 mg PO q4-6hrs
What other drugs is hydrocodone commonly combined with?
1. Acetaminophen (325mg)
2. Ibuprofen (200mg)
what are the formulations for the hydrocodone combos with acetaminophen?
2.5 mg hydrocodone + 325 mg acetaminophen
5 mg hydrocodone + 325 mg acetaminophen
7.5 mg hydrocodone + 325 mg acetaminophen
what are the formulations for hydrocodone combos with ibuprofen?
2.5 mg hydrocodone + 200 mg ibuprofen
5 mg hydrocodone + 200 mg ibuprofen
7.5 mg hydrocodone + 200 mg ibuprofen
what opioid agents can ohio ODs cannot prescribe?
1. oxycodone
2. hydromorphone
both are schedule II
what are the trade names of oxycodone?
1. oxycontin
2. oxaydo
3. roxicodone
4. roxybond
5. xtampza ER
what are the effects of oxycodone?
10-12x more potent than codeine
significant euphoric effects with high potential for dependence
what are the trade names for oxycodone & acetaminophen combos?
1. percocet
2. endocet
3. roxicet
4. primlev
what is the trade name for hydromorphone?
dilaudid
what are the causes of opioid addiction?
linked to euphoric effect of drugs
what are the adverse effects of opioids?
respiratory depression → fatalities
What is a MED unit and how it used?
MED = morphine equivalent dose
used to measure cautionary doses of opioids that may cause overdose
what is the dose-related risk of overdose?
caution at doses > 50 MED/day
avoid doses > 90 MED/day
avg dose in overdose = 98 MED/day
MED = morphine equivalent dose
what antidepressant should you avoid prescribing opioids with?
benzodiazepines - CNS depressant
What are the rules when prescribing an opioid in Ohio?
1. rx must be written or e-prescribed, cannot be called in
2. keep log of controlled substance rxs with pt signature (recommendation), should check OARRS to make sure they didn't get a script elsewhere (rule)
What are two drugs used to treat an opioid overdose?
1. Naloxone (narcan)
2. Naltrexone
what is naloxone?
opioid antagonist used to reverse the effects of opioid overdose
available as injectable or nasal spray
What is naltrexone?
opioid antagonist used to manage long term treatment of opioid dependence
what is methadone?
synthetic opioid developed as an alternative to morphine, involved in 31% of opioid-related death
why would you use an opioid like methadone/buprenorphine to tx drug addicts?
both have a longer (60-hr) half-life → slowly feeds dependence and helps avoid withdrawal symptoms (takes up to 12 days to reach a steady-state conc)
stops peaks and troughs
what is buprenorphine?
partial agonist tx opioid use
has a lower risk d/t respiratory depression plateaus
what are the risks when initiating tx (for each drug) for opioid use disorder?
methadone: risk of OD during initiation
buprenorphine: risk of precipitated withdrawal → must be in opioid withdrawal before initiation
naltrexone: need to be fully abstinent from opioids prior to initiation
what are the pros and cons of buprenorphine?
pros: quick stabilization of withdrawal, may tx pain
cons: possible overdose risk with alcohol use
what are the pros and cons of methadone?
pros: quick stabilization of withdrawal, may be more effective in tx pain
cons: possible overdose risk with alcohol use
what are the pros and cons of naltrexone?
pros: will tx alcohol use disorder, no risk of withdrawal if pt incarcerated
cons: more severe withdrawal, delay in initiation of tx
What are the options we have to treat ocular pain?
1. cycloplegia
2. bandage CL
3. topical NSAID
4. oral NSAID
5. oral acetaminophen
6. oral opioid
what should you do if pt continues to get worse or do not improve within 2-3 days?
re-evaluate cause of pain and manage or refer as necessary
What must you do for any patient with ocular pain?
make a follow up appointment
Ocular pain is almost always due to what?
inflammation