Hemostasis, DVT, PE, Anticoagulation SG
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
hemostasis
the arrest of bleeding, a process important to minimizing blood loss when body structure are injured
hematology
study of blood and blood forming tissue
hematocrit
plasma 55%, the rest is other components
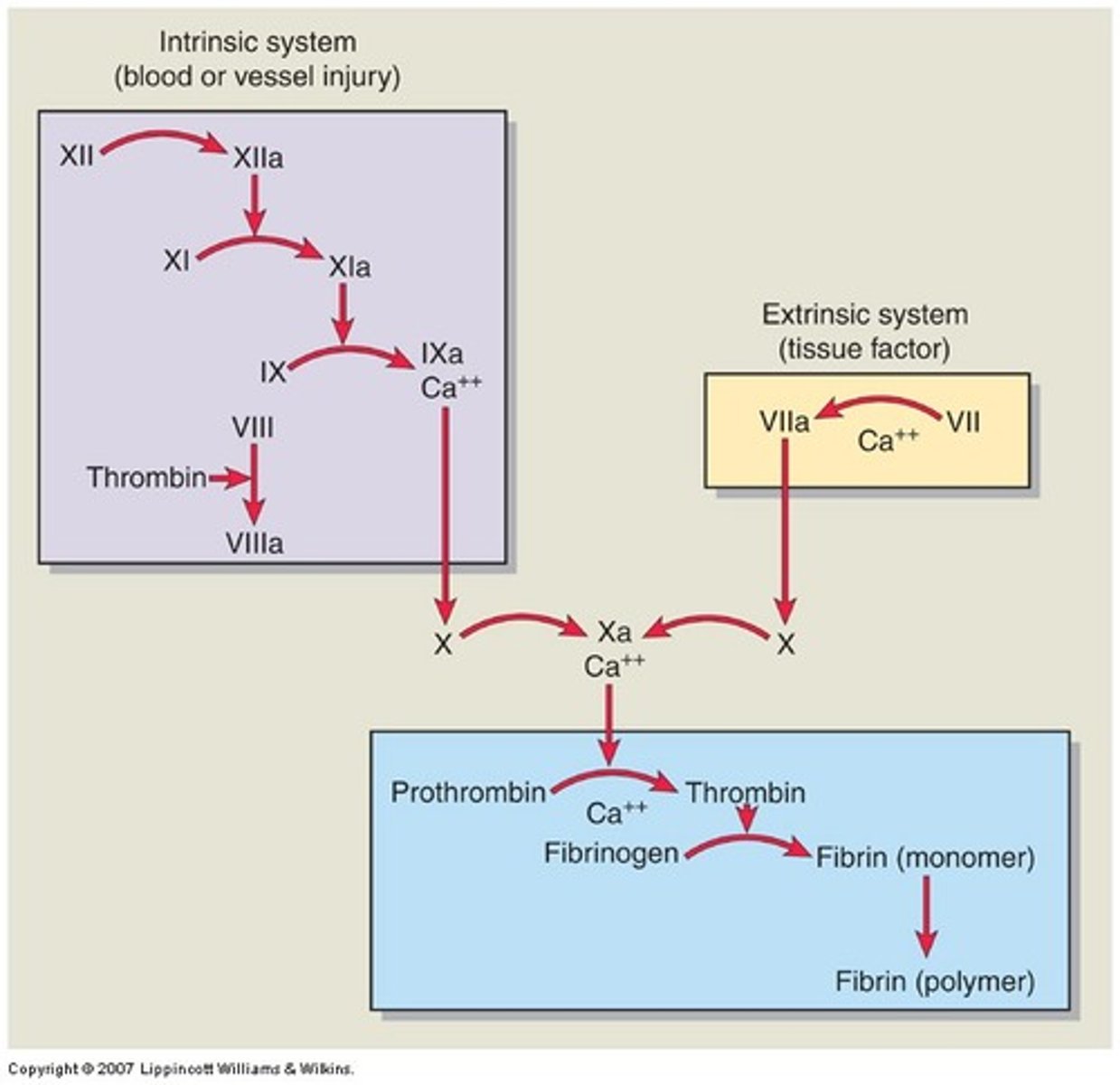
normal clotting mechanism
initiated through one of two pathways, intrinsic or extrinsic
clotting process
vascular injury, vasoconstriction, and subendothelial exposure
adhesion
activation of clotting cascade
formation of a blood clot, aggregation
platelet plug formation
clot retraction and dissolution
aging effects on clotting
changes in bone marrow, Hgb levels, vascular integrity, and blood cell responsiveness and reserves
diminishes ability of older adults to recover from acute illness or compensate for chronic diseases
why is thrombus formation important to achieve hemostasis?
the final blood clot stabilizes the platelet plug and traps other cells, such as RBCs, phagocytes, and microorganisms
adhesion
the loss of endothelial cells exposes adhesive glycoproteins to which more platelets adhere
aggregation
the formation of platelet plugs
activation
the actions so far cause the platelets to undergo activation process which causes them to change shape and bind adhesive proteins
clot retraction and dissolution
counter mechanism of blood clotting that keeps blood in its fluid state
venous thrombosis
involves the formation of a thrombus with vein inflammation, most common disorder of the vein
VTE develops from hereditary and acquired risk factors
virchow's triad
vessel wall injury, venous stasis, and hypercoagulability is central to understanding thrombosis
venous thrombosis process
mechanical or physiologic vessel wall damage activates platelets, causing them to stick together and form a clot
thrombus may dissolve naturally or enlarge, eventually obstructing blood flow, dilating veins, and promoting additional clot formation
venous thrombosis detection
approximately 50% of people are asymptomatic, detection is challenging
risk factors for VTE
venous stasis, endothelial damage, hypercoagulability of blood
venous stasis
occurs when the valves are dysfunctional or the muscles of the extremities are inactive
common in people who are obese or pregnant, have chronic HF or A Fib, have been traveling on long trips, or are immobile for long periods of time
endothelial damage
may be caused by direct or indirect injury, stimulates platelet activation and starts the coagulation cascade, this predisposes the patient to thrombus development
direct endothelial damage
surgery, intravascular catheterization, trauma, burns, prior VTE
indirect endothelial injury
chemotherapy, diabetes, sepsis
hypercoagulability of blood
occurs with many problems that includes severe anemias, polycythemia, cancers, nephrotic syndrome, high homocysteine levels, and proteins C, S, and antithrombin deficiency
superficial vein thrombosis manifestations
palpable, firm, subcutaneous cordlike vein, area around vein may be itchy, painful to touch, reddened, or warm
mild temp elevation and leukocytosis may be present
extremity edema may occur, lower extremity SVT often includes varicose veins
SVT risk factors
increased age, pregnancy, obesity, cancer, recent fracture, estrogen therapy, recent sclerotherapy, recent surgery or long distance travel, hypercoagulability, and history of chronic venous insufficiency
SVT care
ultrasound to confirm, anticoagulants may be needed
graduated compression stockings or bandages, apply warm compresses, elevate affected limb above heart, apply topical NSAIDs, and perform mild exercise such as walking
Deep vein thrombosis
serious condition where blood clot forms in a deep vein, usually in the legs or the pelvis region
DVT manifestations
swelling, pain and tenderness, warmth, redness/discoloration, swollen veins
DVT complications
PE, post thrombotic syndrome, recurring DVT
DVT risk factors
long term bed rest, hospitalization or travel, injury/surgery, cancer, HF, inflammatory bowel, obesity, smoking, pregnancy, and oral contraceptives
DVT care
anticoagulants, compression stockings, inferior vena cava cilter, thrombolytic agents
proximal DVTs
have a higher chance of breaking off and causing a PE
most DVTs
occur in lower extremities but some occur in upper
VTE manifestations
unilateral leg edema, pain, tenderness with palpation, dilated superficial veins, sense of fullness in the thigh or calf, paresthesias, warm skin, redness, or systemic temp greater than 100.4 degrees
VTE complications
pulmonary embolism, chronic thromboembolic pulmonary hypertensions, post thrombotic syndrome, and phlegmasia cerulea dolens
VTE diagnostics
based on assessment combined with D-dimer testing and ultrasound
blood: ACT, aPTT, INR, bleeding time, Hgb, Hct, platelet count, D-dimer, fibrin monomer complex
noninvasive: venous compression ultrasound and duplex ultrasound
invasive CT venography, MRI venography, contrast
VTE care
prevention drug therapy, surgery or radiologic therapies
early and progressive mobilization, graduated compression stocking, intermittent pneumatic compression devices
venous thromboembolism
detached thrombus results in embolus, travels through the venous system to right side of heart and lodges in pulmonary circulation, becomes PE
post thrombotic syndrome symptoms
pain, aching, fatigue, heaviness, sensation of swelling, cramps, pruritus, tingling, paresthesia, bursting pain with exercise, and venous claudication
PTS manifestations
persistent edema, spider veins, venous dilation, redness, cyanosis, increased pigmentation, eczema, pain during compression, atrophic blanche, and lipodermatosclerosis
pulmonary embolism
sudden, life threatening blockage in one of the pulmonary arteries in the lungs
PE diagnosis
CT pulmonary angiography is gold standard, D-dimer blood test, chest x-ray, venous ultrasound, ventilation perfusion scans
PE treatment
aims to stop the clot from getting bigger and prevent new formation, anticoagulants or thrombolytics in severe cases, procedures to remove the clot
heparin
IV or SubQ, indirect thrombin inhibitor, IV given as adjunct for existing blood clots, SQ given prophylactically to prevent development of clots, affects intrinsic plasma antithrombin coagulation pathway; inhibits thrombin mediated conversion of fibrinogen to fibrin
heparin considerations
effects measured at regular intervals with aPTT, or ACT, monitor CBC, administration guidelines
LMWH considerations
monitor CBC, reduced dosage in pt with renal problems or history of HIT prophylaxis given SQ, existing VTE give continuous IV, monitor aPTT, more predictable, long half-life, fewer bleeding complications
LMWH
SQ, indirect thrombin inhibitor
heparin side effects
HIT, long term osteoporosis
warfarin
oral, k=long term extended anticoagulation
inhibits activation of vitamin K dependent coagulation factors II, VII, IX, and X as well as anticoagulant proteins C and S
warfarin considerations
INR used to monitor therapeutic levels, same time each day, variations of certain genes may influence response to drug
takes 48-72 hours to be effective, often overlapping with parenteral anticoagulants for 5 days
do not give with NSAIDs or antiplatelet drugs, avoid changing intake of vitamin K in diet because it alters INR
dabigatran
oral direct thrombin inhibitor used for VTE prevention after elective joint replacement, for stroke prevention in nonvalvular A fib, and as a treatment for VTE
dabigatran considerations
rapid onset, no need to monitor anticoagulation, few food-drug interactions, lower risk for major bleeding, and predictable dose response
idarucizumab
dagibatran antidote
rivaroxaban and apixaban
inhibit factor Xa directly or indirectly, producing rapid anticoagulation
used for both VTE preventions and treatment
direct factor Xa inhibitors considerations
coagulation monitoring or dose adjustment not needed, anticoagulant activity measured using anti Xa assays
adnexant alfa
reverses actions of direct Xa inhibitors
aspirin
irreversibly inhibits COX-1, prevents platelet aggregation, used for MI and stroke prevention and acute coronary artery syndrome
aspirin considerations
monitor for bleeding, GI risk factors, hold before surgery, avoud in children
P2Y12 ADP receptor antagonists
clopidogrel and ticagrelor, block ADP receptors on platelets preventing activation, clopidogrel requires liver activation and ticagrelor has a faster onset with no liver activation required
clopidogrel considerations
bleeding, avoid with omeprazole
ticagrelor considerations
dyspnea
tirofiban
blocks final pathway of platelet aggregation, used during PCI, unstable angina, and high risk ACS
tirofiban considerations
given IV, continuous cardiac monitoring, high bleeding risk, and monitor platelet count
alteplase
recombinant tissue plasminogen activator used for acute ischemic stroke, STEMI, and massive PE
reteplase
modified tPA, used primarily for STEMI
tenecteplase
long half-life, given as a single IV bolus, used for STEMI
thrombolytics considerations
active bleeding absolute contraindication, monitor neuro status, signs of internal bleeding, and Hgb/Hct, avoid IM injections, limit venipunctures, no invasive procedures during infusion
hospitalization patient not bleeding
UH, LMWH, or fondaparinux
low risk VTE
no prophylaxis
moderate risk
UH or LMWH, trauma, abdominal or pelvic surgery for cancer, or orthopedic surgery
VTE surgery
open venous thrombectomy, inferior vena cava interruption devices
open venous thrombectomy
incision into vein to remove clot
inferior vena cava interruption devices
filters places via right femoral or internal jugular veins, trap clots without impeding blood flow, recommended for acute PE or proximal VTE of leg with active bleeding or if anticoagulation is contraindicated or ineffective
IVCID complications
air embolism, improper placement, filter migration, perforation of vena cava with retroperitoneal bleeding, clogged filter
VTE interventional radiology therapies
mechanical thrombectomy, pharmacomechanical devices, post thrombus extraction, angioplasty, and/or stenting
can be used with catheter directed thrombolytic therapy
VTE radiology nursing cares
maintain catheter systems, monitor for bleeding, embolization, and impaired perfusion, teach VTE prevention
clotting cascade