Adult Complex: Exam 2
1/102
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
103 Terms
Indications: mechanical ventilation
Acute respiratory failure
Apnea
Inability to breathe/protect the airway
Severe hypoxemia and/or hypercarbia
Respiratory muscle fatigue
Hemorrhage
Trauma
Neuromuscular problems
Drug overdose
Burns
Shock
Invasive v. noninvasive ventilation
Invasive
Process by which a ventilator is used to deliver oxygen to the lungs; is a means of supporting patients until they recover the ability to breathe independently
Can serve as a bridge to long-term ventilation or until a decision is made to stop ventilatory support
Is not a curative process
Noninvasive
Uses a mask instead of an endotracheal tube to help oxygen + ventilate patients
Is ideal for those who need a higher level of ventilatory support, but their condition isn’t bad enough to warrant mechanical ventilation
Types
CPAP
BiPAP
Nursing care: mechanical ventilation
Maintain correct tube placement
Continuously monitor intubated patients for proper tube placement
Note exit point from mouth/nare
Assess integrity of tape/securement device
Observe for symmetric chest wall movement
Auscultate to confirm bilateral breath sounds
If tubes move/become dislodged, they can migrate upwards in the pharynx or enter the R/L mainstem bronchus (ventilating one lung)
Airway emergency
Stay with patient + try to maintain airway
Support ventilation with a BVM + 100% oxygen
Call for help to assess/reposition tube
Maintain proper cuff inflation
Maintain cuff pressure at 20-30 cm H2O to ensure adequate tracheal perfusion
Measure + record cuff pressure after intubation + on a routine basis (q8h) with minimally occluding volume technique
Place a stethoscope over the trachea + inflate the cuff by adding air until no air at PIP (end of ventilator inspiration)
For spontaneously breathing patients, inflate until no sound is heard after a deep breath or after inhalation with a BVM
Use a manometer to confirm cuff pressure is between 20-30 cm H2O
Document cuff pressure
If adequate pressure can’t be maintained or larger volumes of air are needed to maintain inflation, a leak or tracheal dilation at the cuff site may be present
Notify providers in such cases
Maintain tube patency
Suctioning indications
Visible secretions in endotracheal tube
Increase in respiratory rate/frequent coughing
Sudden decrease in O2 sats
Suspected secretion aspiration
Increased peak airway pressure
Auscultating adventitious breath sounds over the trachea/bronchi
Assess need for suctioning hourly
Visible coughing
Coarse crackles/wheezes over large airways
Moist cough
Increase in PIP
Restlessness/agitation
Neuro patients may not show any signs of the need for suctioning; suctioning every shift is recommended
Do not suction routinely
Note color, character, consistency, and amount of sputum suctioned
Closely assess patients before, during, and after suctioning
If patients don’t tolerate suctioning, stop immediately; continue reassessments until patients hemodynamically stabilize, recover and/or situations resolve before retrying
Maintain adequate hydration when indicated
Provide supplemental humidification of inspired gases through the ventilator to help thin secretions
Turning q2 + early ambulation helps move secretions into larger airways
Maintain alarm systems
Ensure all ventilator alarms are always on
High pressure alarms
Increased airway secretions
Wheezing/bronchospasm
Endotracheal tube is displaced
Ventilator tube is obstructed from water or kink in the tubing
Patient coughs, gags, or bites on oral endotracheal tube
Patient is anxious or fights the ventilator
Low pressure alarms
Disconnection or leak in ventilator or in patient’s airway cuff
Patient stops spontaneous breathing
Oral care
Moisten lips, tongue, and gums with saline/water swabs to prevent drying
Using chlorhexidine at least 3 times/day can help decrease oral contamination and ventilator-associated pneumonia
Skin integrity
Reposition + replace endotracheal tubes per agency policy to prevent skin breakdown
Two staff members should always perform repositioning to maintain correct positioning + prevent accidental dislodgement
Monitor patients for any signs of respiratory distress during procedure
For orally intubated patients, remove bite block + old tape, provide oral care, and reposition tube to opposite side of the mouth; replace bite block, reconfirm cuff inflation + tube placement, and resecure tube per policy
Complications: mechanical ventilation
Adverse hemodynamic effects (hypotension)
Increased intrathoracic pressure compresses thoracic vessels
Compression decreases venous return to the heart, preload, SBP, MAP, and cardiac output
Ventilator-assisted pneumonia
Pneumonia that occurs 48+ hours after intubation
Risk factors
Contaminated respiratory equipment
Inadequate hand hygiene
Adverse environment
Decreased patient ability to cough + clear secretions
Poor nutrition
Immobility
Underlying disease processes
Manifestations
Fever
High WBC counts
Change in color and/or amount of sputum
Crackles/wheezes on auscultation
New lung infiltrates on chest x-ray
Prevention guidelines
Minimizing sedation, including daily spontaneous awakening + breathing trials
Early ambulation + frequent turning (q2h)
Use of endotracheal tubes with subglottic secretion drainage ports
Elevating head of bed a minimum of 30-45 degrees unless contraindicated
Oral care with chlorhexidine
No routine changes of ventilator circuit tubing
Hand hygiene before + after suctioning whenever ventilator equipment is touched
After contact with any respiratory secretions
Always wear gloves when in contact with patient + change gloves between activities
Aspiration
Suction patient’s mouths often via Yankauer or sterile single-use catheter
Risk factors
Improper cuff inflation
Patient positioning
Decreased gastric mobility + bowel function, if patient is getting enteral nutrition
Even when cuffs are properly inflated, take precautions to prevent vomiting
Unless contraindicated, keep head of the bed elevated at least 30 degrees for all intubated patients getting enteral nutrition
Barotrauma
Results when increased airway pressure distends the lungs + possibly ruptures fragile alveoli/blebs
Risk increases as lung inflation pressures increases
Patients with noncompliant lungs are at greatest risk (patients with acute respiratory distress syndrome)
Increasing inflation pressure places patient at risk for pneumothorax, which can quickly develop to a tension pneumothorax
Volutrauma
Can occur if too large a volume of air (tidal volume) is used to ventilate noncompliant lungs
Causes alveolar rupture + movement of fluids and protein into alveolar spaces
Minimized by using low-volume ventilation in patients with stiff, noncompliant lungs
Nursing care: noninvasive ventilation
Assess LOC, hemodynamic stability, and work of breathing
Patients with a decreased LOC can’t protect their airway or clear secretions; intubation + mechanical ventilation may be needed
Any degree of hemodynamic instability warrants immediate reevaluation of noninvasive ventilation
Provide mouth, nare, and eye care
Provide measures to protect the skin from breakdown/ulceration
Any degree of redness = S1 pressure injury
Attempts of alleviate pressure for tight-fitting masks (alternative length of time the mask is on) is essential
Using masks of different sizes can help; consult RTs for additional info
Patients must be able to remove masks independently due to vomiting risk; elevate heads of bed 30-45 degrees
Clinical manifestations: asthma exacerbation
Wheezing
Unreliable sign to gauge attack severity; doesn’t always occur
Cough
Can sometimes be the only symptom (cough variant asthma)
Can be productive/nonproductive
Dyspnea
Accessory muscle use
Tripoding
Tachypnea
Anxiety
Agitation
Chest tightness
Prolonged expiration
Peak expiratory flow rate <50% PB
Patient report of usual treatments failing
Decreased/absent breath sounds
Silent chest (severely decreased breath sounds; ominous), indicative of severe airway obstruction + impeding acute respiratory failure
Interprofessional care: asthma exacerbation
Drug therapy
Corticosteroids
First line agents to treat acute asthma attacks + first step in acute asthma management
Reduce bronchial hyperresponsiveness, block late-phase asthma response, and inhibit the migration of inflammatory cells
Side effects
Easy bruising
Decreased bone mineral density
Oropharyngeal candidiasis
Hoarseness
Dry cough
Side effects are managed with metered dose inhalers and by gargling with water or mouthwash after each use
Beta agonists
Can be short or long acting
Short acting can help with acute bronchospasms, but are not first-line therapies
Short acting shouldn’t be used along for recurrent, repeated asthma attacks or for long-term control
Long acting shouldn’t be used alone as primary treatment; they can be used as treatment adjuncts
Long acting should be used only if patients don’t respond to medium dose inhaled corticosteroids
Teach patients that long acting drugs shouldn’t be used to treat acute symptoms or to obtain quick relief from bronchospasm
Tell patients that long acting drugs are used once every 12 hours
Too frequent use indicates poor asthma control, can mask severity of condition, and lead to reduced drug effectiveness
Nursing care: asthma exacerbation
In severe attacks, continually monitor vitals and work of breathing
Patients can be tachycardic/pneic and solely focus on breathing
Respirations can be >30 rpm, and accessory muscles can be in use
Patients can be agitated, restless, or confused from hypoxemia
Patients often sit forward to maximize diaphragmatic movement
Serial peak expiratory flow rates, oximetry, and ABGs give info about the severity of attacks and the response to therapy
Oxygen therapy is given to achieve a PaO2 of at least 60 mmHg or O2 sats >90%
Should be continuous + pulse ox
If patients can swallow, oral corticosteroids will be part of the treatment plan; if not, IV steroid are given
Auscultate lung sounds; wheezing may be heard, being louder in airways that are responding to therapy as airflow increases
If silent chest is observed, notify provider; acute respiratory failure is imminent
Clinical manifestations: status asthmaticus
Hypoxia
Hypercapnia
Acute respiratory failure
Chest tightness
Severely marked increase of shortness of breath
Inability to speak
Hypotension
Bradycardia
Cardiac arrest
Interprofessional care: status asthmaticus
Treated with IV magnesium sulfate
Admin shouldn’t delay the need for intubation
Immediate mechanical venilation + hemodynamic monitoring is essential
Continuous analgesic infusions + sedation with drugs help decrease work of breathing and promote synchrony with ventilators
Neuromuscular blockers can be used
Inhaled anesthetics can be used for those not responding to conventional treatment
Etiology + patho: acute respiratory failure
Hypoxemic (oxygenation failure)
Arterial oxygen <60 mmHg on room air + at sea level with normal/slightly subnormal CO2 levels
Low arterial oxygen can exist despite supplemental oxygen
The main issue is the inadequate exchange of oxygen between the alveoli + pulmonary capillaries
Physiologic mechanisms
V/Q mismatch
Not 1:1 = mismatch
Causes
Increased secretions in the airways/alveoli
Bronchospasms
Pain
Atelectasis
Pulmonary emboli
Treated by treating underlying cause
Oxygen therapy is a first step to reverse hypoxemia
Frequent ABG analysis, pulse oximetry, respiratory rate + rhythm, and response to oxygen therapy are important
Shunt
Extreme V/Q mismatch
Occurs when blood exits the heart without having its gas exchanged
Oxygen therapy may not be effective
Diffusion impairment
Occurs when gas exchange across the alveolar-capillary membrane is compromised by a process that damages/destroys the alveolar membrane or affects blood flow through the pulmonary capillaries
Caused by conditions that thicken the alveolar-capillary membrane (fibrotic) slow gas transport
Ex: pulmonary fibrosis, interstitial lung disease, and ARDS
Classic sign is hypoxemia that worsens with exercise but not at rest
Alveolar hypoventilation
Decrease in ventilation that increases arterial CO2
Common causes
CNS problems
Chest wall dysfunction
Acute asthma
Restrictive lung disease
Mainly a mechanism of hypercapnic respiratory failure, but contributes to hypoxemia
Hypercapnic (ventilatory failure)
Arterial CO2 >50 mmHg, which can be accompanies by hypoxemia and/or acidemia (blood pH <7.35)
Main issue is insufficient CO2 removal
Causes
CNS problems
Overdoses of respiratory depressing meds
Brainstem infarction
Can interfere with the medullary respiratory center; medulla fails to sense changes in arterial oxygen → no increase in respiratory rate occurs
TBIs
When occurring with a decreased LOC, patient ability to protect airway, breathe, or manage secretions is hindered
Neuromuscular problems
Diseases that cause muscle weakness/paralysis lead to patient inability to clear CO2 and maintain arterial oxygen levels
Toxin exposure can interfere with the nerve supply to muscles + lung ventilation
Respiratory muscle weakness can occur from muscle wasting during critical illness or peripheral nerve damage
Chest wall abnormalities
With severe obesity, the weight of the chest + abdominal contents limit lung expansion
In patients with flail chest, fractures prevent the ribs from expanding normally
With kyphosis, changes in spinal configuration compresses the lungs + prevents normal chest wall expansion
Problems with airways/alveoli
Patients with COPD, asthma, and cystic fibrosis are at higher risk because of the underlying patho of such conditions results in airflow obstruction + air trapping
Respiratory muscle fatigue + ventilatory failure occur from added work of breathing needed to inspire against increased airway resistance + air trapped in alveoli
Clinical manifestations: hypoxemic acute respiratory failure
Specific
Accessory muscle use
Dyspnea (early)
Observing patient position helps assess the effort associated with work of breathing
Patients with mild respiratory distress may be able to lie down, while those in moderate distress may prefer to sit
Patients in severe distress may be unable to breathe unless sitting upright
Intercostal muscle retraction
Nasal flaring
Paradoxical chest/abdominal wall movement (late + severe)
Prolonged expiration
Decreased O2 sats
Tachypnea
Cyanosis (late)
Nonspecific
BP changes (increased early; decreased late)
Dysrhythmias (late)
Tachycardia (early)
Cool, pale, clammy, diaphoretic skin (early)
Altered mental status (agitation, confusion, disorientation, restlessness, combativeness)
One of the first to appear; the brain is sensitive to changes in oxygenation + acid-base levels)
Decreased LOC
Coma (late)
Fatigue
Inability to talk in complete sentences without stopping to breathe
Clinical manifestations: hypercapnic acute respiratory failure
Specific
Dyspnea
Limited chest wall movement
Pursed-lip breathing
Tripoding
Helps decreased work of breathing in patients with moderate to severe COPD and acute respiratory failure
Bradypnea or tachypnea with shallow respirations
Increased respiratory rates require a substantial amount of work + can lead to muscle fatigue
Decreased tidal volume
Decreased minute ventilation
Nonspecific
Hypertension
Dysrhythmias
Tachycardia
Altered mental status
Morning headache
Progressive somnolence
Increased intracranial pressure
Coma (late)
Decreased DTRs
Muscle weakness
Tremors/seizures (late)
Diagnostic studies: acute respiratory failure
Chest x-rays, if ID possible causes
ABGs, to evaluate oxygenation + ventilation and acid-base balance
Pulse oximetry
CBC
Electrolytes
Urinalysis
ECG
Blood + sputum cultures
CT scan or V/Q lung scan, if pulmonary emboli are suspected
End-tidal CO2, for patients in severe respiratory failure who need mechanical ventilation
Interprofessional care: acute respiratory failure
Drug therapy
Reduce airway inflammation + bronchospasm
In acute bronchospasm, short-acting bronchodilators can be given at 15-30 minute intervals until a response occurs
Give via handheld nebulizers/metered-dose inhalers with spacers
Prolonged use can increase risk for dysrhythmias and cardiac ischemia
Monitor vitals + ECG for changes
Corticosteroids can be used in combo with other meds; it can take several hours to see their effects
Inhaled corticosteroids can take 4-5 days for optimal therapeutic effects
Monitor potassium levels
Prolonged used causes adrenal insufficiency
Hyperglycemia is a common side effects
Relieve pulmonary congestion
Diuretics can be given to decrease pulmonary congestion caused by heart failure
Changes in HR + rhythm and significant BP changes are common; give meds cautiously
Treat infection
IV antibiotics are given for treatment
Chest x-rays can show location + extent of infections
Sputum cultures can help ID organisms causing the infection and their sensitivity to antibiotics
Reduce anxiety, pain, and restlessness
For non-intubated patients, anxiety, pain, and restlessness can cause tachypnea and ineffective ventilation
For intubated patents, they can cause ventilator dyssynchrony and increase the risk for unplanned extubation
Turn + reposition patients frequently
Provide reassurance + emotional support to patients + caregivers
IV benzos + opioids can help
Start at the lowest dose possible
Assess for treatable causes of restlessness (hypoxemia, pain, delirium) + manage as needed
Restlessness + mental status changes are the first signs of hypoxemia or patient-ventilator dyssynchrony
Address underlying causes + avoid only depending on analgesics and sedatives
Chest physiotherapy
Indicated for all patients producing sputum or have severe atelectasis or pulmonary infiltrates on chest x-ray
Postural drainage, percussion, and vibration to the affected lung segments help move secretions to the larger airways, for removal via suctioning/coughing
Contraindications
TBI
Increased ICP
Unstable orthopedic injuries
Recent hemoptysis
Nursing care: acute respiratory failure
Acute care
Primary goal is to ID and treat the underlying cause
Monitor patients continuously for therapeutic response, ABG trends, and signs of clinical improvement
Respiratory therapy
Oxygen therapy
Main goal is to correct hypoxemia
Never withhold oxygen from patients
Always administer at the lower possible FIO2 (oxygen concentration) needed to keep the arterial, pulse, and saturation of oxygen within patient-specific goals
Observe patient response to oxygen therapy
Closely monitor for mental status changes, respiratory rates, and ABGs
Oxygen delivery device choices depend on patient condition, degree of respiratory failure, ability to maintain a patent airway, amount of FIO2 delivered, and patient ability to breath spontaneously
The selected device must help maintain arterial oxygen at >60 mmHg and saturation at >90%
Face masks can cause anxiety; if patients try to remove them, explore other device options
Risks of prolonged oxygen delivery
Oxygen toxicity
Exposure to FIO2 (>60%) for longer than 48 hours
Absorption atelectasis
Oxygen replaces nitrogen and other gases usually present in alveoli
Increased pulmonary capillary permeability
Decreased surfactant production
Surfactant inactivation
Fibrotic changes in the alveoli
Mobilize secretions
Positioning
Position patients upright, with heads of the bed elevates at least 30 degrees, or with a reclining chair/chair bed
If there’s a chance for aspiration, position patients in side-lying position
Patients with a unilateral lung problem can be placed in a lateral/side-lying position (good lung down)
Allows for improved V/Q matching in the affected lung
Coughing
Augmented coughing can help some patients
To help, place 1/both hands at the anterolateral base of the patient’s lungs
As deep inspirations end + expirations start, move hands forcefully upward
Increases abdominal pressure + helps patient cough
Huffing is a series of coughs performed while saying the word “huff”
Prevents the glottis from closing, forcing air + mucous out of the airways
Patients take a deep breath, hold if for 2-3 seconds, and forcefully exhale
Staged coughing
With patients sitting, have them breath in/out 3-4 times through the mouth, then cough while bending forward and pressing a pillow inward against the diaphragm
Suctioning
May be needed if patients are unable to expectorate secretions
Perform cautiously, as stimulating the gag reflex can induce vomiting
Suctioning through artificial airways are done as needed
Humidification
Adjunct to secretion management
Be aware that aerosol therapy can cause bronchospasm + severe coughing, causing a decrease in arterial oxygen
Frequent assessment of patient tolerance to therapy is critical
Hydration
Unless contraindicated, adequate fluid intake (2-3 L/day) keeps secretions thin + easier to remove
May not be possible in patients with respiratory failure
Patients who can’t take in enough fluids PO need IV hydration
Assess cardiac + renal status to determine if patients can tolerate IV fluid volume and avoid heart failure and pulmonary edema
Regularly assess for signs of fluid overload
Early ambulation
Etiology + patho: ARDS
Phases
Injury (exudative)
Usually occurs 24-72 hours after the initial insult (direct/indirect)
Generally lasts 7-10 days
Engorgement of peribronchial and perivascular interstitial space → interstitial edema
V/Q mismatch and shunt develop because the alveoli fill with fluid
Reparative (proliferative)
Starts 1-2 weeks after the initial lung injury
Fibrotic (fibroproliferative)
Can start as early as 24 hours after initial lung injury
Not all patients enter the fibrotic stage; those who do have a poorer prognosis
Causes
Direct
Aspiration
Pneumonia
Sepsis
Chest trauma
Embolism
Inhalation of toxic substances
Near-drowning
O2 toxicity
Radiation pneumonitis
Indirect
Massive trauma
Sepsis/septic shock
Severe TBI
Shock (hypovolemic, cardiogenic)
Acute pancreatitis
Cardiopulmonary bypass
DIC
Opioid overdose
Transfusion-related acute lung injury
Urosepsis
Clinical manifestations: ARDS
Initial injury + 24-72 hours after
Mild dyspnea
Tachypnea
Cough
Restlessness
Lung auscultation can be normal or reveal fine, scattered crackles
With progression
Increased work of breathing → respiratory distress
Tachypnea + retractions
Tachycardia
Diaphorsis
Altered mental status
Cyanosis
Pallor
Lung auscultation can reveal scattered/diffuse crackles and course crackles on expiration
Complications: ARDS
Can develop from the disease itself/its treatment
Abnormal lung function
Most patients will recover within a year, and many will have normal/near-normal lung function, but not this isn’t true for all patients
Contributing factors
The severity of scarring + changes within the lungs
Mechanical ventilation
Duration of time ventilated
Use of extracorporeal life support
Patients may report fatigue, chest pain, shortness of breath after minimal activity, and persistent dyspnea post-ARDS
Ventilator-associated pneumonia
Risk factors
Immunocompromised patients
Invasive monitoring devices
Aspiration
Prolonged mechanical ventilation
Barotrauma
Occurs when fragile alveoli are overdistended with excess pressure during mechanical ventilation
High peak airway pressures needed to ventilate lungs predispose patients to barotrauma
Results in alveolar air escaping from ruptured alveoli
Can lead to
Pulmonary interstitial emphysema
Pneumothorax
Subcutaneous emphysema
Pneumopericardium
Tension pneumothorax
Providing ventilation with a smaller tidal volume and varying amounts of PEEP minimizes the risk
GI ulcers
Due to blood diversion from the GI to the respiratory system to help meet oxygen demands
Management strategies include correcting predisposing conditions (hypotension, shock, acidosis)
Prophylactic management
Antiulcer drugs (PPIs)
Mucosal-protecting drugs (sucralfate)
Early enteral nutrition helps prevent mucosal damage
VTE
Complication of immobility + venous stasis
Prophylaxis
SCD/TED hoses
Anticoagulation
Early ambulation
AKI
Can occur from decreased renal perfusion + subsequent decreased oxygen delivery to the kidneys
Most often occurs due to hypotension in septic shock
Can result from hypoxemia or nephrotoxic drugs used to treat ARDS-related infections
Monitor I/O, daily weights, and daily BUN + creatinine levels
Patients often receive continuous renal replacement therapy; they’re often hemodynamically unstable and need vasopressors and/or inotropes to maintain HR + BP
They can’t tolerate large volumes of fluid that traditional hemodialysis would remove
Patients can receive therapy 24 hours/day
Psychological issues
Survivors of ARDS can have anxiety, issues with memory/attention, inability to focus, nightmares, depression, and sometimes, varying degrees of PTSD
Nursing + interprofessional care: ARDS
Mechanical ventilation
Required for patients with moderate/severe ARDS
Pressure-control ventilation helps keep inspiratory + plateau pressures form getting too high
Prevents alveolar overdistention + rupture
Drug therapy
Antibiotics to treat underlying infection
Corticosteroids to decrease inflammatory response
partial-thickness burns
Superficial (1st degree)
Epidermis affected
Blanchable erythema
Pain
Mild swelling
Blistering/peeling skin after 24 hrs
Deep (2nd degree)
Epidermis + dermis affected
Red, shiny, wet, fluid-filled vesicles
Several pain
Mild/moderate edema
full-thickness burns
3rd/4th degree burns
Dry, waxy, white, brown/charred, leathery, hard skin
Visible thrombosed vessels
Insensitive to pain due to nerve destruction
Possible muscle, tendon, and bone involvement
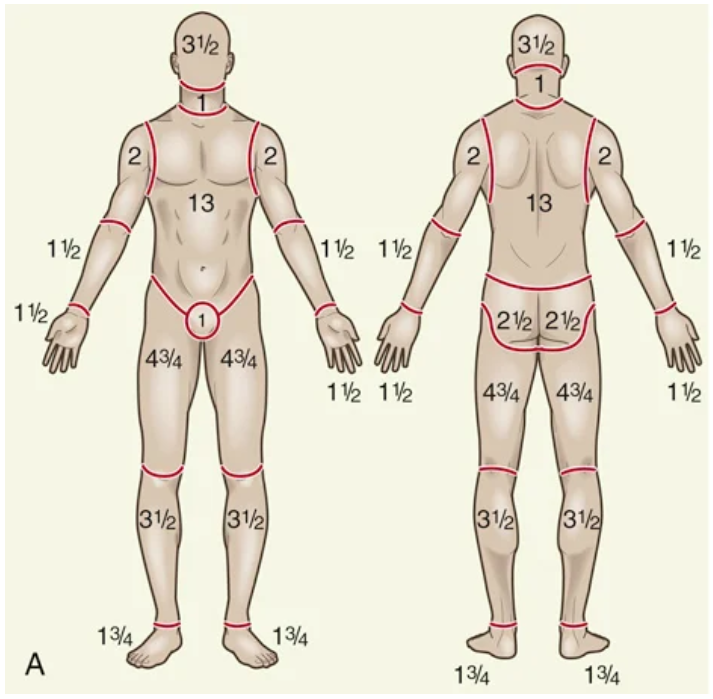
Rule of Nines
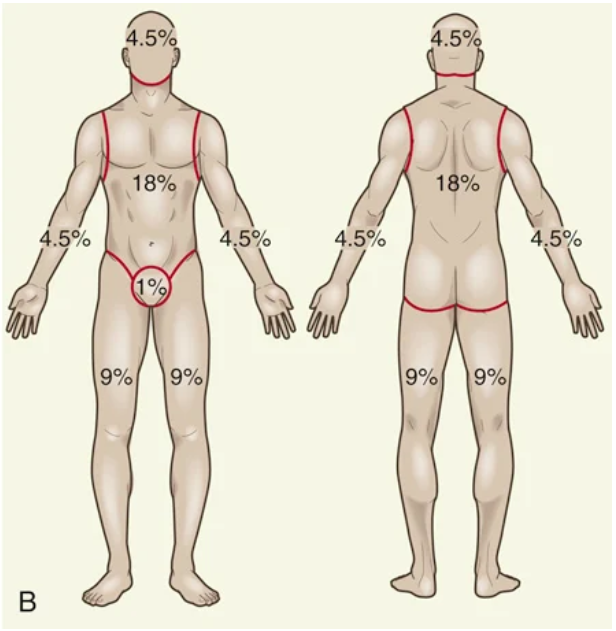
Lund-Browder chart
Best used for kids because it considers patient age in proportion to relative body-area size
Patho: emergent burn phase
Usually lasts 72 hours after initial injury
Fluid + electrolyte shifts
burn shock - Combo of distributive + hypovolemic shock; significant threat to major burn patients
Patients vitals will begin to change as third spacing occurs
Mass edema + significant wound drainage may be seen
Loss of intravascular fluid can cause burn shock
Monitor for hypotension, tachycardia, and tachypnea
Report changes in vitals to providers
AKI + death can develop if not resuscitated sufficiently
Hemolysis of RBCs from circulating factors released at the time of injury from burned tissue affects perfusion
Monitor for high hematocrits from hemoconcentration from fluid loss
Levels will return to normal after burn shock resolves
Major electrolyte shifts of sodium + potassium can occur during this phase
Potassium shifts develop first when injured cells + hemolyzed RBCs release potassium into circulation (hyperkalemia)
Sodium rapidly moves to interstitial spaces (hyponatremia)
Ends once capillary membrane permeability is restored after successful fluid resuscitation
Inflammation + healing
Burns cause coagulation necrosis
Neutrophils + monocytes accumulate at injury sites
Fibroblasts + newly formed collagen fibrils appear + begin wound repaid within the first 6-12 hours after injury
Immunologic changes
Burns challenge immune systems by altering the skin’s barrier to invading organisms
Bone marrow depression occurs + circulating levels of immunoglobulins decrease
Defects occur in WBC function
Inflammatory cytokine cascade impairs the function of lymphocytes, monocytes, and neutrophils → high infection risk
Clinical manifestations: emergent burn phase
Patients are normally alert + able to answer questions during admission or until intubated, if there’s respiratory compromise
Monitor cognition + report changes
Unconsciousness/altered mental status
Causes
Hypoxia, from inhalation injury
Head trauma
Substance use
Side effects of sedation/pain meds
Anxiety
Give patients simple explanations of what to expect
Heat loss
Provide warm blankets, increase room temp, or use heat lamps
Hypovolemia → shock
Pain
Blisters
Paralytic ileus
Shivering
Complications: emergent burn phase
Respiratory
Types of inhalation injuries
Injuries form toxic gas exposure
Supraglottic injury from direct heat or chemicals causing severe mucosal edema
Subglottic injury from airway inflammation + edema → atelectasis + pneumonia
Severity can be mild to severe; rapid initial + ongoing assessment is critical
Airway compromise + pulmonary edema can develop within hours of injury
Patients may need a fiberoptic bronchoscopy + carboxyhemoglobin blood levels to confirm suspicions
Patients exposed to carbon monoxide will have elevate carboxyhemoglobin levels
Examine sputum for carbon particles
Watch for signs of respiratory distress (increased agitation, anxiety, restlessness, or changes in rate/character of breathing); symptoms may not be present at first
Patients with preexisting lung diseases are more likely to develop respiratory infections
Cardiovascular
Deep circumferential burns + subsequent edema formation can impair peripheral perfusion
If untreated, ischemia, paresthesia, and necrosis can occur
Escharotomies restore circulation to compromised extremities or improve chest expansion
Patients are at risk for VTE, especially if other risk factors are present
Risk factors
Advanced age
Obesity
Extensive/lower extremity burns
Concomitant lower extremity trauma
Prolonged immobility
It’s recommended for patients to receive low-molecular-weight heparin or low-dose unfractioned heparin, if there are no contraindications
Apply SCDs if patients are immobile
Renal
AKI are the most common renal complication
If hypovolemia is left untreated, renal ischemia can occur → AKI development
Monitor the adequacy of fluid replacement, proper admin can prevent the myoglobin + hemoglobin from blocking renal tubules
Nursing + interprofessional care: emergent burn phase
Airway management
Place patients in high-Fowler’s unless contraindicated (spinal injury)
Treatment for inhalation injuries include
100% O2 via nonrebreather
Aerosolized heparin
N-acetylcysteine
Albuterol
Reposition patients q1-2h
Suction prn
Encourage deep breathing + coughing hourly
Monitor ABGs to assess adequacy of gas exchange
Keep patients on tele
Monitor pulse oximetry + capnography
Evaluate patient response to interventions + report adverse reactions/deterioration to providers
Generally, patients with significant face/neck burns need intubation within 1-2 hours after injury
Early intubation prevents the need for emergency cricothyrotomy
Other patients need intubation if symptoms of severe respiratory distress develop
Extubation can occur at the end of the emergent phase when airway edema resolves
Usually 3-5 days after initial injury
Others may be intubated for longer, due to extensive lung damage
Fluid therapy
Insert at least 2 large-bore IVs when burns are >15% TBSA
Central lines can be used for burns >20% TBSA
Calculate TBSA of burns to calculate initial IV fluid needs
Use ABA or Parkland formula to calculate fluid needs for the first 24 hours after injury
Formulas provide estimates; titrate based on patient response
A-lines are best for measuring MAP + BP; manual BP measurements are often invalid due to edema + vasoconstriction
Crystalloids + sometimes colloids (albumin) are used for resuscitation
Insert Foleys in patients with >20% TBSA burns
Monitor patients for early signs of fluid overload, especially older ones or those with chronic heart, lung, or kidney diseases
Assess for the adequacy of fluid resuscitation hourly via urine output + cardiac parameters
Output should be 0.5-1 mL/kg/hr for adults; 1-1.5 mL/kg/hr for kids
Cardiac parameters
MAP >65
SBP >90 mmHg
HR <120
Patients with electrical burns have greater fluid needs to prevent AKI
They often need osmotic diuretics to increase urine output + overcome hemoglobinuria or myoglobinuria
Higher hourly outputs of 75-100 mL/hr are best
Wound care
On admission to burn units, patients will shower or receive a trolley bath
Use mild cleansers + washcloths, and perform cleansing and gentle wound debridement
Debridements
Surgical
Done in ORs
Necrotic skin is removed
Open
Burns are covered with topical antimicrobials + left open toair
Usually limited to facial burns
When bathing is complete, skin + burns are dried, the total burn percentage is re-estimated
Providers will prescribe topical dressings/agents based on burn depth, bacterial count, and cost
Dressing changes continue once/twice a day, depending on burn severity + dressing types
Check patients for sulfa allergies; many burn antimicrobials contain it
Always wear PPE when patient burn wounds are exposed
Wear nonsterile disposable gloves when removing contaminated dressings + when washing wounds
Facial
Keep ears free from pressure due to poor vascularization + infection tendency
Do not use pillows for patients with ear burns; cartilage pressure can cause chondritis
Ears may stick to the pillowcase → pain + bleeding
Raise patient heads with a rolled towel under the shoulder to avoid pressure necrosis
Also used for neck burns to hyperextend the neck + prevent contracture
Extremities
Extend burned hands + arms and raise them on pillows/foam wedges to reduce edema
Remove splints often + inspect the skin + bony prominences to avoid areas of pressure from inappropriate/prolonged application
Perineum
Keep perineum clean + dry after voiding/bowel movements
Remove Foleys from fluid resuscitation asap
If patients have frequent, loose stools, consider using a fecal diversion device
Drug therapy
Analgesics + sedatives
Early in the post-burn period, give IV pain meds
Evaluate pain management plans often, as needs can change + tolerances can develop, especially in the acute phase
Patient pain level may not directly correlate with the depth + extent of the burn
Consider multimodal approaches to pain control
Sedative/hypnotics + antidepressants with analgesics help with anxiety, insomnia, and depression
Tetanus immunization
Patients routinely get tetanus toxoid due to the exposure risk to clostridium tetani
Tetanus immunoglobulin would be considered if the patient hasn’t received an active immunization in within 10 years before the burn
Nutrition therapy
Hypermetabolic states proportional to wound size occurs after major burns
Resting metabolic expediture can increased 50-100% above normal
Core temps increase
Catecholamine release → catabolism stimulation
When fluid replacements needs are addressed, nutrition takes prioirty
Early + aggressive nutritional supports starts in hours of injury
Decreases complications + mortality
Optimizes wound healing
Minimizes negative effects of hypermetabolism + catabolism
Patho: acute burn phase
Starts with the mobilization of interstitial fluid + subsequent diuresis and continues until wound are nearly healed
Ends when partial-thickness wound heal or full-thickness burns are covered by skin grafts
Can take weeks/months depending on the burn severity + patient response to treatment
Oxygenation problems can resolve, but inhalation injuries won’t for days/weeks/months
Vitals are more stable
Would healing starts as WBCs surround the burn wound + phagocytosis occurs
Necrotic tissues starts to slough
Patients become more aware of the enormity of their situation
Clinical manifestations: acute burn phase
Partial thickness wounds start healing at the wound margins
Epithelial buds from hair follicles/glands in the dermal bed eventually close the wound
Healing is spontaneous + usually occurs in 10-21 days
Patients often have more pain due to repeated dressing changes, therapy exercises, opioid tolerance, fatigue, and reduced coping ability
Complications: acute burn phase
Infection
Normal skin flora will quickly colonize burn wounds
Manifestations
Hypo/hyperthermia
Tachycardia
Tachypnea
Hypotension
Oliguria
Elevated WBC count
Fungal infections can develop in mucous membranes due to systemic antibiotic therapy + low resistance
Give antifungals (nystatin + fluconazole) as ordered
Neuro
Can result from severe hypoxia from respiratory injuries or as a complication from electrical injuries
Other causes
Electrolyte imbalances
Stress
Cerebral edema
Sepsis
Sleep problems
Analgesic/antianxiety meds
Patients can be disoriented, withdraw, be combative, hallucinate, or have frequent nightmare-like episodes
Delirium is more acute at night + occurs more often in older patients
Use screening tools to diagnose; start interventions to prevent
Orient + reassure patients who are confused/agitated
Musculoskeletal
ROM can be affected by less supple + compliant skin
Skin + joint contractures can occur
Patients may prefer flexed positions for comfort
Have patients stretch + move burned parts as much as possible
Consult with PT/OT about proper positioning + splinting to prevent/reduce contractures
GI
Diarrhea can result form enteral nutrition or antibiotic use
Constipation can occur from opioid use, decreased mobility, and low-fiber diets
Curling ulcers can occur (diffuse superficial lesions, including mucosal erosion)
Prevent by feeding patients asap after burns
Antacids, histamine receptor blockers, and PPIs are used prophylactically to neutralize stomach acids + inhibit histamine + secretion of hydrochloric acid
Patients with major burns can have occult blood in stools + need close monitoring for bleeding
Stress response can decrease GI blood flow
Endocrine
Watch for transient increase in glucose levels due to stress-mediated cortisol + catecholamine release
Insulin’s effectiveness decreases because of relative insulin insensitivity → high glucose levels
Increased caloric intake to address metabolic needs can increase
When hyperglycemia occurs, check glucose levels + give insulin as ordered
Monitor glucose lab results
Electrolyte imbalances
Hyponatremia can develop from excess GI suction + diarrhea
Manifestations
Headache
Irritability
Confusion
Vomiting
Seizures
Coma
Patients can develop dilutional hyponatremia from excess water intake
To avoid, offer patients fluids besides water
Hypernatremia can occur after successful fluid resuscitation, if large amounts of hypertonic solutions were given
Manifestations
Altered mental status
Drowsiness
Restlessness
Confusions
Lethargy
Seizures
Coma
Sodium restrictions, in IV fluids and enteral nutrition, can reduce levels
Hyperkalemia can occur if patients have renal failure, adrenocortical insufficiency, or massive deep muscle injury (electrical burns)
Manifestations
Dysrhythmias
Confusion
Tetnay
Muscle crmpas
Paresthesia
Weakness
Hypokalemia occurs with V/D, prolonged GI suction, IV therapy, and through wounds without supplementation
Manifestations
Dysrhythmias
Weakness
Paresthesia
Decreased GI motility
Decreased reflexes
Nursing + interprofessional care: acute burn phase
Wound care
Consists of ongoing observation, assessment, cleansing, debridement, and dressing changes
Dressing changes, topical antimicrobial therapy, graft are, and donor site care is done as often as prn, depending on topical cream/dressing
Collagenase is used for enzymatic debridement; promotes removal of nonviable tissue from health wound beds
Gently cleanse wounds to remove old antimicrobials + any loose necrotic tissue, scabs, or dried blood
After cleansing, cover wound with topical antimicrobial creams or silver-impregnated dressings
Avoid silver sulfadiazine if patients are allergic/sensitive to sulfa
Excision + grafting
excision - Devitalized tissue (eschar) is surgically removed down to SQ tissue/fascia
Dermatomes are used to remove donor skin for grafting
Abdomen + thighs are common donor sites
Grafts are placed on clean, viable tissue to achieve good adherence, and stapled/sutured in place
Wound vac dressings are often placed on top of skin grafts to optimize adherence to the excised wound bed
Nursing care of donor site is specific to the dressing used
Pain management
Burn patients experience two types of pain
Continuous background pain
Treatment-induced pain
First line of treatment is medication
For background pain, frequent IV admin of an opioid provides a steady, therapeutic level
If tolerating foods, slow-release, twice-daily opioids can be used
Anxiolytics + adjuvant analgesics can enhance opioid effectiveness
Breakthrough doses of analgesia must be available
For treatment-induced pain, pre-medicate with analgesics IV/PO
Complementary pain therapies can also work
PT/OT
Continuous therapy is critical if patients are to regain + maintain muscle strength + optimal joint function
Exercise during dressing changes, when bulky dressings are removed + patients medicated, can be effective
Passive + active ROM should be performed on all joints
Maintain the schedule for wearing splints
Check skin to ensure splints aren’t causing excess pressure
Nutrition therapy
Goal is to provide adequate calories + protein to promote healing; when wounds are still open, patients are in a hypermetabolic + catabolic state
Patients can benefit from antioxidant protocols
Selenium
Vitamin E
Acetylcysteine
Ascorbic acid
Zinc
Multivitamins
Meeting daily calorie needs is essential + should start in 1-2 days post-burn
Dieticians regularly calculate daily calorie needs + adjust as conditions change
Monitor labs (albumin, prealbumin, total protein, transferring) regularly
Encourage patients to eat high protein + carb foods to meet calorie goals
Ask caregivers/family to bring favorite foods from home
Reinforce steps being taken to achieve adequate intake
Ideally, weight loss shouldn’t be >10% of pre-burn weight
Record daily caloric intake using calorie- count sheets + review with dieticians
Weigh patients weekly to evaluate progress
Patho: rehab burn phase
Starts when wounds have nearly healed, and patients are engaging in some level of self care
Can happen as soon as 2 weeks or as long as 7-8 months after major burns
Wounds health either by spontaneous re-epithelialization or skin grafting
New skin appears flat + pink; in ~4-6 weeks, area becomes raised + hyperemic
If adequate ROM isn’t continued, the new tissue will shorten → contracture
Mature healing is achieved in ~12 months when suppleness has returned, and pink/red color has faded to a slightly lighter hue than the surrounding unburned tissue
Factors influencing recovery
Age
Chronic illness
Physical disabilities
Substace absue
Clinical manifestations: rehab burn phase
Scarring characteristics
Discoloration
Fades over time
Tell patients with darker skin that it’ll take longer to regain tone due to altered melanocytes
Provide teaching + emotional support to help patients with grief over body changes
Cosmetic camo/pigment implantation can help even out unequal skin tones + improve overall appearance + self-image
Contour
Gentle pressure is maintained on health burns with custom-fitted pressure garments + clear, thermoplastic face masks
Pressure garments + masks should never be worn over unhealed wounds
Pressure garments are worn up to 23 hours/day for as long as 12-18 months
Patients may report discomfort from itching where healing is occurring
Teach patients that water-based moisturizers + short-term use of oral antihistamines can help reduce itching
Have patients protect healed burn areas from direct sunlight for ~3 months to prevent hyperpigmentation + sunburns
Tell patients to wear sunscreen when exposing healed skin to the sun
Complications: rehab burn phase
Skin + joint contractures
Joint contractures can develop from the shortening of scar tissue in the flexor tissues of a joint
Susceptible areas
Anterior/lateral neck areas
Axillae
Antecubital fossae
Fingers
Groin areas
Popliteal fossae
Knees
Ankles
Hypertrophic scarring
Carefully monitor patients for complications
Encourage proper positioning, splinting, and exercise
Tell patients to continue with prevention strategies until skin matures ~1 year post healing
Burned legs can be wrapped with elastic bandages to assist with circulation of leg-graft + donor sites before ambulation
Burned arms can be wrapped with a layer of tubular elastic gauze; prevents blister formation, promotes venous return, and decreases pain + itchiness
Nursing + interprofessional care: rehab burn phase
Ask patients about thoughts + feelings about discharge
Encourage patients + caregivers to participate in care
Provide wound care instructions, if needed
Tell patients to shower to wash wounds
Have patients and/or caregivers perform dressing chaanges
Provide advice on scar management, moisturizing, and sun protection
Suggest using water-based creams that penetrate the dermis on healed areas to keep skin supple + moisturized
Ensure patients know when to contact burn team + stress need to keep outpatient visits
If needed, collab with social work/case management to arrange home care servies
Assess pain management + nutrition needs during each visit
Encourage patients to perform PT/OT exercises
Reassure patients to maintain morale, especially when they realize that healing takes time
Emotional + psych needs: burns
Assess circumstances of the burn, family relationships, and prior ways of coping with stress
Open + frequent communication among patients, caregivers, close friends, and burn team members is essential
Be sensitive to the patient’s emotions + concerns
Encourage patients to discuss fears about loss of lifestyle/function, temporary/permanent deformity + disfigurement, return to work + home life, and financial burdens from long hospital stays + rehab
Encourage independence + eventual return to pre-burn activities
Peer counseling + informal interactions with other burn survivors can bring comfort during adjustment periods + help restore confidence
Reassure patients that their feelings during the adjustment period are normal; frustration + impatience are expected as a new life is established
Help patients in adapting to a realistic, yet positive appraisal of their specific situation, emphasizing when they can/can’t do
Continued support from trusted + familiar burn team members is essential for caregivers
Help them assist with aspects of patient care to help them reconnect with with their loved one + ease the transition back home
Acknowledge the reality + normalcy of their emotions
Address spiritual + cultural needs
Pastoral care can help
ID what’s important to patients + caregivers and communicate such info in plans of care
Encourage burn teams to be culturally aware of + sensitive to the patient + caregiver’s cultural needs
Address concerns about sexuality with honesty
Immature scar tissue can make touch unpleasant or can dull sensations
Assure patients + partners that it’s normal and to heed anticipatory guidance from the burn team to avoid undue emotional strain
Early psych interventions are essential if patients have psychiatric illnesses or if the injury was a suicide attempt
Histories of mental health issues can influence the length of hospitalization + time needed to prep for discharge
Psychological support starts in the hospital, but links to community resources are needed to ensure continuity of care
Caregiver + patient emotional support groups can be beneficial in meeting patient + caregiver emotional needs at any phase of the recovery process
Parkland formula
4 mL x body weight (kg) x percentage of TBSA burned
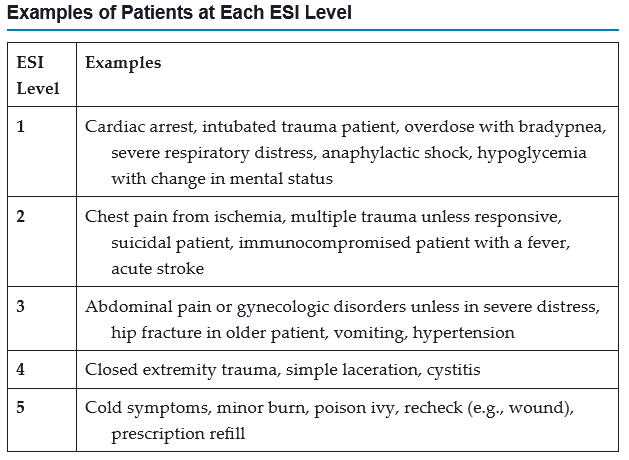
Emergency Severity Index
5-level triage system that incorporates concepts of illness severity + resource use to determine who is treated first
Includes a triage algorithm that directs users to assign a level to patients coming to the ED
ESI-1
Unstable ABCs
Obvious life/organ threat
Death risk high
High resource intensity with staff at bedside continuously
ESI-2
Threatened ABCs
High-risk patients should be seen in 10 mins
High resource intensity with multiple, often complex, diagnostics
ESI-3
Stable ABCs
Patients should be seen in an hour
Medium/high resource intensity with multiple diagnostics
ESI-4
Stable ABCs
Can wait to be seen
Simple diagnostics/procedures; low resource intensity
ESI-5
Stable ABCs
Can wait to be seen
Simple physical exam can suffice
primary survey
Focuses on ABCs, disability, exposure, full set of vitals + family presence, and getting other monitoring devices
If there’s uncontrolled external bleeding, ABCs can be modified to CABCs (catastrophic hemorrhage, airway, breathing, circulation)
If present, the bleeding must be controlled first; apply direct pressure with a sterile dressing → pressure dressing to any obvious bleeding sites
Aims to ID life-threatening problems so that appropriate interventions can be started
Components
Alertness + airway
Signs of a compromised airway
Dyspnea
Inability to speak
Gasping (agonal) breaths
Foreign bodies in the airway
Face/neck trauma
Patient alertness level is a crucial factor for choosing correct airway interventions
Determine LOC by assessing patient response to verbal and/or painful stimuli
Use AVPU to help determine LOC
Alert
Responsive to voice
Responsive to pain
Unresponsive
Airway maintenance should progress rapidly from least → most invasive method
Treatment includes opening airway via:
Jaw-thrust maneuver, avoiding neck hyperextension
Suctioning and/or foreign body removal
Inserting naso/oropharyngeal airway (unconscious patients only)
Endotracheal intubation
If intubation is impossible due to airway obstruction, emergency cricothyroidotomy/tracheotomy is done
Ventilate patients with 100% oxygen via BVM before intubation/cricothyroidotomy
Rapid-sequence intubation is the preferred procedure for securing an unprotected airway in the ED
Involves sedative + paralytic use to aid in intubation + reduce risk of aspiration and airway trauma
If patients have a suspected spinal cord injury and isn’t already immobilized, c-spines must be stabilized at the same as the airway assessment
Keep beds flat + continue monitoring airway patency and breathing effectiveness
Breathing
Every critically injured/ill patient has increased metabolic + oxygen demand; they should receive supplemental oxygen
Give high-flow oxygen via nonrebreather masks + monitor patient response
Interventions for life-threatening issues:
BVM ventilation with 100% oxygen
Needle decompression
Intubation
Treatment of underlying cause
Circulation + control of hemorrhage
Uncontrolled internal/external bleeding places patients at risk for hemorrhagic shock
Check for femoral/carotid pulses
Peripheral pulses may be absent due to direct injury or vasoconstriction
Assess quality + rate oof pulses
Assess skin for color, temp, and moisture
Altered mental status + delayed cap refill care common signs of shock
When assessing cap refill in cold temps, the coldness delays refill
Establish IV access in upper extremities unless contraindicated (open fracture or injury that affects limb circulation)
Insert 2 large-bore catheters
Start aggressive fluid resuscitation via normal saline or lactated Ringer’s
Consider intraosseous or central venous access if peripheral access cannot be rapidly established
In emergency (life-threatening) situations, give blood that’s not cross-matched (O-) if immediate transfusions are needed
Disability
Conduct brief neuro assessments
LOC is a measure of the degree of disability
Use GCS scores to determine LOC; allows for consistent communication among interprofessional care team
Is not accurate for intubated or aphasic patients
Assess pupils for PERRLA
Exposure + environmental control
Remove patient clothing to perform thorough assessments
Try not to cute through areas that can be forensic evidence (bullet holes)
Don’t remove impaled objects; can cause bleeding + further injury
When patient is exposed, use warming blankets, overhead warmers, and warmed IV fluids to limit heat loss, prevent hypothermia, and maintain privacy
Full set of vitals + family presence
Obtain full set of vitals after patient is exposed
If patients have sustained/suspected of having sustained chest trauma, or if BP is abnormally high/low, obtain BP in both arms
Assign a care team members to explain the care being given + answer questions if a caregiver is present during resuscitation/invasive procedures
Get monitoring devices + give comfort
Start adjunct measures for monitoring patient condition if not already done
Use the LMNOP acronym to remember resuscitation aids
secondary survey
Brief, systematic process that aims to ID all injuries
Helpful for discovering unknown problems in patients with a poor/confusing history
Components
History + head-to-toe
Obtain a history + mechanism of the injury/illness
Use MIST to help obtain a prehospital report of the incident/illness
Mechanism of injjry
Injuries sustained
Signs/symptoms before arrival
Treatment before arrival
Details of the incident are important because the mechanism of injury + injury patterns can predict specific injuries
Use SAMPLE to ask about patient history
Symptoms from the injury/illness
Allergies
Medication history
Past history
Last meal/oral intake
Events/environmental factors leading to the illness/injury
Head, neck, and face
Check eyes for extraocular movements
Disconjugate gaze is a sign of neuro damage
Battle’s sing can indicate basilar skull fractures
Raccoon eyes (periorbital bruising) usually occurs from fractures of the base of the frontal part of the skull
Check ears for blood + CSF
Do not block clear drainage from the ear or nose
Chest
Inspection + palpation of the chest can help detect heart + lung injuries
Abdomen + flanks
Stabilize, don’t remove, any impaled objects
If patients have blunt abdominal trauma, or if there’s suspected intraabdominal hemorrhage, perform a focused abdominal sonography for trams (FAST)
Can ID blood in the peritoneal space + assess cardiac function
Noninvasive + done quickly at bedside
Can’t rule out a retroperitoneal bleed; if suspected, CT scans are needed
Pelvis + perineum
Inspect + gently palpate the pelvis
Do not rock the pelvis
Pain can indicate a pelvic fracture + need for imaging
Assess for bladder distention, hematuria, dysuria, or inability to void
Extremities
Assess upper + lower extremities for point tenderness, crepitus, and deformities
If not done prehospital, splint injured extremities above + below injury to decrease further soft tissue injury + pain
Check pulses before + after movement/splinting
Pulseless extremities are time-sensitive emergencies
Immobilize + elevate injured extremities + apply ice packs
Antibiotics are given for open fractures to prevent infection
Assess extremities for compartments syndrome
Pain
Pallor
Pulselessness
Paresthesia
Paralysis
Inspect posterior surfaces
Logroll trauma patients while protecting the c-spine
Just keep reevaluating
After secondary survey is complete, document findings
Ongoing monitoring + evals are critical
Provide appropriate care and assess patient response
Use VIPP for reevaluation process
Vitals
Injuries sustained + interventions
Primary survey
Pain level
Evals of airway patency + effectiveness of breathing are always the highest priorities
Monitor respiratory rate + rhythm, O2 sats, and ABGs, if ordered
Portable chest x-rays confirm tube placements
Give tetanus prophylaxis based on vaccination history + condition of any wounds
Closely monitor LOC + vitals
Note quality of peripheral pulses + skin temp, color, and moisture for any info about circulation and perfusion
When indicated, insert Foleys to decompress the bladder, monitor urine output, and check for hematuria
Notify providers of any changes that can occur to patients during ongoing assessments
Etiology + patho: increased ICP
Results from an increase of brain tissue, blood, or CSF in the skull
Clinically significant because it decreases cerebral perfusion pressure and increases risks for brain ischemia and infarction
Common causes
Mass
Cerebral edema
Contributing factors
Arterial pressure
Venous pressure
Intraabdominal + intrathoracic pressure
Posture
Temp
ABGs (CO2)
Cerebral insults increase formation + spread of cerebral edema → hypercapnia, cerebral acidosis, impaired autoregulation, and systemic hypertensio
Edema distorts brain tissue, further increases ICP + leads to more tissue hypoxia and acidosis
Maintain cerebral blood flow to preserve tissue + minimize secondary injury
Sustained increases in ICP result in brainstem compression + brain herniation
Herniation occurs as brain tissue is forcibly shifted from a compartment of greater pressure to a compartment of less pressure
Clinical manifestations: increased ICP
Altered LOC
Changes in vitals
Cushing’s triad
Systolic hypertension + widened pulse pressure
Bradycardia + full, bounding pulse
Irregular respirations
Often don’t occur until ICP increase is prolonged or is suddenly + markedly increased
Medical emergency; is a sign of brainstem compression + impending death
Ocular signs
Compression of cranial nerve III
Ipsilateral pupil dilation (dilation on affected side)
Pupils may be sluggish/unresponsive to light
Inability to move eye upward + adduct
Ptosis
Effects from other cranial nerves
Blurred vision
Diplopia
Changes in extraocular eye movements
Decreased motor function
Contralateral hemiparesis/hemiplegia, depending on location of the source of increased ICP
Decorticate/decerebrate posturing, from noxious stimuli
Decerebrate posturing can indicate more serious damage
Headache
Nocturnal and/or morning headaches are causes for concern
Straining, agitation or movement can worsen pain
Vomiting
When unpreceded by nausea = unexpected
Nonspecific sign of increased ICP that’s related to pressure changes in the cranium
Diagnostic studies: increased ICP
CT + MRI can discover many conditions that can cause increased ICP and assess effects of treatment
EEG
Cerebral angiography
ICP measurement
Brain tissue oxygenation measurement via LICOX catheter
PET scns
Transcranial Doppler studies
Evoked potential studies
Lumbar punctures are contraindicated; cerebral herniation can occur from sudden release of pressure
Nursing care: increased ICP
Assessment
LOC
Body functions
Vitals
GCS scoring
15 = fully alert
<8 = coma
Plot scores on graphs for comparisons + determination of stability, improvement, or deterioration
Allows different healthcare pros to come to the same conclusion about patient status
Neuro assessment
Compare pupils for size, shape, movement, and reactivity
If cranial nerve II is compressed, ipsilateral pupil dilation will be seen, and get larger until fully dilated
If ICP continues increasing, both pupils dilate
Testing the corneal reflex gives info about cranial nerve V + VII; if absent, start routine eye care to prevent corneal abrasion
Test all extremities for strength + note any asymmetry in strength or movement
Assess motor response of unconscious/cooperative patient by observing spontaneous movement
If not possible, apply pain stimulus + note response
Do not include hand grasps as part of assessment; it’s a reflex action and can misrepresent patient status
Record vitals
Acute care
Respiratory function
Maintain patent airway
Remove secretions via suctioning PRN
Patients with GCS scores <8 or altered LOC who aren’t able to maintain patent airways or ventilate effectively need intubation and mechanical ventilation
Monitor ABGs + act to maintain levels in prescribed/acceptable parameters
Prevent hypoxia and hypercapnia to minimize secondary injury
Suctioning + coughing cause transient decreases in arterial oxygen + increase ICP
Keep suctions to a minimum and <10 seconds
Give 100% oxygen before/after to prevent decreases in arterial oxygen
Limit suctioning to passes/suction procedure if possible
Avoid abdominal distention; it can interfere with respiratory function
NG tube insertion to aspirate stomach contents can prevent distention, vomiting, and aspiration
Sedation
Pain, anxiety, and fear related to primary injury, therapeutic procedures, or noxious stimuli can increase ICP + BP
Admin of sedatives, paralytics, and analgesics can alter neuro states, masking true changes
Drug therapy may need to be temporarily stopped to appropriately assess neuro status
Choice, dose, and combo of drugs can vary depending on patient history, neuro state, and overall clinical presentation
Opioids have minimal effects on cerebral blood flow or oxygen metabolism
Be aware of the side effects of alpha adrenergic agonists (dexmedetomidine), especially hypotension, which can lower cerebral perfusion pressure
Nondepolarizing neuromuscular blocking agents can help achieve complete ventilatory control in the treatment of refractory intracranial hypertension
Must be used in combo with sedatives, analgesics, or benzos
Benzos are usually avoided due to hypotensive effects + long half-lives
Patients should be kept in quiet, calm environments with minimal noise + interruptions
Observe patients for agitation, irritation, or frustration
Teach families + caregivers about decreasing stimulation
Coordinate with care teams to minimize procedures that can cause agitation
Fluid + electrolyte balance
Closely monitor IV fluids via infusion pumps
Assess I/O, including insensible losses, and obtain daily weights
Monitor electrolytes, especially glucose, sodium, potassium, magnesium, and osmolality
Monitor urine output to detect problems related to diabetes insipidus + SIADH
Monitoring ICP
Used with other parameters to guide patient care + assess response to treatment
Be alert to factors that increase ICP + try to minimize them
Increased intrathoracic pressure can increased ICP by impeding venous return
Patients should avoid coughing, straining, sneezing, and the Valsalva maneuver
Body position
Maintain patients in head-up position; keep heads midline, avoiding extreme neck flexion
Flexion can cause venous obstruction + contribute to increased ICP
Adjust body position to decrease ICP + improve cerebral perfusion pressure
Elevating heads of beds to 30 degrees promotes head drainage + decreases vascular congestion that can produce cerebral edema
Elevation >30 degrees can decrease cerebral perfusion pressure by lowering systemic BP
Carefully evaluate effects of elevation on both ICP + cerebral perfusion pressure
Position beds so that they lower ICP while optimizing cerebral perfusion pressure + other indices of cerebral oxygenation
Turn patients with slow + gentle movements; rapid changes can increase ICP
Prevent discomfort when turning + repositioning; pain/agitation increases ICP
Avoid extreme hip flexion to decrease risk for raising intraabdominal pressure, which increases ICP
Provide physical care to minimize complications of immobility; turn q2h
Protection from injury
Use restraints carefully in agitated patients
If they’re needed, they should be secure enough to be effective
Observe the skin underneath restraints regularly for signs of irritation/breakdown
Agitation can increase from restraint use, indicating the need for other measures (sedation, family company)
Place patients with/at risk for seizures on seizure precautions
Padded side rails
Ambu bags at bedside
Readily available suction
Accurate + timely admin of antiseizure meds
Close observation
Antiseizure prophylaxis against early seizures (within first 7-10 days) is recommended in severe brain injury
Keep patients in quiet, nonstimulant environments; use calm and reassuring approaches when interacting
Psych considerations
Be aware of the psychologic wellbeing of patients + families
Keep explanations short + simple
Allow patients + caregivers to acquire the amount of info they want
Assess family members’ desires to help with providing care for patients + allow their participation as appropriate
Encourage interprofessional management involving the patient + family in decision making as much as possible
Interprofessional care: increased ICP
Maintenance of adequate oxygenation to support brain function + prevent secondary injury is essential
Endotracheal tubes or tracheostomies may be needed to maintain adequate ventilation
ABGs guide oxygen therapy
If increased ICP is caused by a mass, surgical removal is the best treatment
Drug therapy
Mannitol
Osmotic diuretic given IV to decrease ICP via plasma expansion and osmosis
Reduces hematocrit + blood viscosity → increases cerebral blood flow + oxygenation
Creates a vascular osmotic gradient; decrease in total brain fluid content causes fluid movement from tissues to blood vessels → reducing ICP
Monitor fluid + electrolyte balance
Contraindicated with renal disease + increased serum osmolality
Hypertonic saline solutions
Produce massive movement of water out of edematous swollen brain cells and into blood vessels, reducing swelling + improving cerebral blood flow
During (slow) infusion, monitor BP + serum sodium levels, as intravascular fluid volume excess can occur
Corticosteroids
Treat vasogenic edema around tumors + abscesses
Not recommended for TBIs
Stabilize cell membranes + inhibit prostaglandin synthesis, preventing the formation of proinflammatory mediators
Improve neuronal function by improving cerebral blood flow + restoring autoregulation
Complications
Hyperglycemia
Perform glucose checks q6h
Infections
GI bleeds
Patients should be on histamine receptor blockers or PPIs
Normal saline
Preferred solution for giving secondary meds
Hypotonic solutions can decrease serum osmolality + increase cerebral edema
Acetaminophen
Used to maintain temps between 96.8 - 98.6 F
Metabolic demands (fever, agitation, shivering, pai, seizures) can increase ICP
If shivering occurs, patients may need sedation or a different cooling method
Barbiturates
High doses are used in patients with increased ICP refractory to other treatments
They decrease cerebral metabolism → decreasing ICP + reducing cerebral edema
Dosing is based on analysis of bedside EEG tracing + ICP
Types + clinical manifestations of skull fractures
Basilar
CSF/brain otorrhea
Tympanic membrane bulging, from blood/CSF
Battle sign
Tinnitus/difficulty hearing
Rhinorrhea
Facial paralysis
Conjugate deviation of gaze
Vertigo
Frontal
Exposure of brain to contamiants via frontal sinus
Possible associate with air in forehead tissue
CSF rhinorrhea
Facial paralysis
Loss of taste
Battle sign
Orbital
Raccoon eyes
Optic nerve injury
Parietal
Deafness
CSF/brain otorrhea
Tympanic membrane bulging
Facial paralysis
Loss of taste
Battle sign
Posterior fossa
Occiptal bruising → cortical blindness
Visual field defects
Ataxia/other cerebellar signs (rare)
Temporal
Boggy temporal muscle, from blood extravasation
Battle sign
CSF otorrhea
Middle meningeal artery disruption
Epidural hematoma
Nursing care: cranial surgery
Acute care
Is similar to that of patients with increased ICP
Preop teaching is important in reducing fears in patients, families, and caregivers
Provide general info about surgery type + postop expectations
Explain that some hair may be shaved to allow for better exposure + prevent contamination
Inform patients that they’ll be in the ICU/IMC postop
Main goal of postop care is preventing increased ICP
Frequent neuro assessments are essential in the first 48 hours
Closely monitor fluid + electrolyte levels and serum osmolality to detect changes in sodium regulation, onset of diabetes insipidus, or severe hypovolemia
Manage problems associated with increased ICP
Monitor patients for pain + nausea; give antiemetics as ordered
Do not give promethazine; it can increase somnolence + change the accuracy of a neuro assessment
Control pain with short-acting opioids + monitor neuro status
When the incision over the skull is in the anterior (middle) fossa, elevate the head of the bed at least 30 degrees
If the surgical approach is in the posterior fossa, or a Burr hole is present, keep patients flat or at a slight elevation (10-15 degrees)
Turning + repositioning depends on the site of the operations
If a bone flap was removed, don’t position patients on the operative side
Place sigs at the head of the bed alerting all of the craniectomy site + position of surgical site
Observe dressing for color, odor, and drainage amount
Check drains for placement
Assess area around the dressing
Scalp care should include meticulous incision care to prevent infection
Cleanse area + treat per agency protocol/provider orders
When dressings are removed, use antiseptic soaps for washing the scalp
Psych impacts of hair removal can be lessened via wigs, turbans, scarves, or hats
For patients on radiation, teach them to use sunblock and head coverings if any sun exposure is expected
Ambulatory care
Base care on a realistic appraisal of factors for patient rehab potential
Surgery indication
Postop course
General health
Specific rehab potential can’t be determined util cerebral edema + increased ICP subside postop
Take care to maintain as much function as possible through measures such as
Careful positioning
Meticulous skin + mouth care
Regular ROM exercises
Bowel + bladder care
Adequate nutrition
Address needs + problems of each patient individually because many variables affect care plans
Collab with other care team members
PTs can give exercise plans
Speech therapists can help with communication + swallowing skills
Social workers can help patient + family adapt to changes in home life, work, and financial circumstances
Etiology + patho: ischemic strokes
Results from inadequate blood low to the brain from partial/complete arterial occlusion
Classes
Thrombotic
Occurs from injury to a blood vessel wall + formation of blood clot
Develops readily where atherosclerotic plaques have already narrowed blood vessels
Most common stroke cause
More common in older adults, especially those with
High cholesterol
Atherosclerosis
Diabetes
Extent depends on
Onset speed
Size of damaged area
Prescence of collateral circulation
Most patients don’t have a decreased LOC in the first 24 hours, unless due to a brainstem stroke or other condition (seizure, increased ICP, hemorrhage)
Manifestations can progress in the first 2 hours as infarction and cerebral edema increase
Embolic
Occurs when an embolus lodges in + occludes a cerebral artery, resulting in infarction and edema of the area supplied by the involved vessel
Second most common cause of stroke
Most emboli originate in the endocardial layer of the heart when a plaque breaks off the endocardium and enters the circulation
Causative conditions
A-fib
MI
Infective endocarditis
Valvular heart prostheses
Patent foramen ovale
Atrial septal defects
Emboli from air or fat from long bone fractures (rare)
Can affect any age group
Rheumatic heart disease is a cause of embolic stroke in young/middle-aged adults
Patients have severe manifestations that occur suddenly
Patient are usually conscious with a headache
Effects are initially characterized by severe neuro deficits, which can be temporary if the clot breaks up and allows blood to flow
Smaller emboli then continue to obstruct smaller vessels, which then involve smaller portions of the brain with fewer deficits noted
Etiology + patho: hemorrhagic strokes
Result from bleeding into brain tissue or the subarachnoid space/ventricles
Types
Intracerebral
Bleeding within the brain caused by a rupture of a vessel (usually in the basal ganglia)
Poor prognosis; half of deaths occur in the first 48 hours
Causes
Hypertension (most common)
Vascular malformations
Coagulation disorders
Anticoagulant/thrombolytic drugs
Trauma
Brain tumors
Ruptured aneurysms
Often occurs during periods of activity
There’s often a sudden onset of symptoms, with progression over minutes/hours due to ongoing bleeding
Manifestations
Neuro deficits
Headache
N/V
Decreased LOC
Hypertension
Symptom extent depend on the amount, location, and duration of bleeding
Blood clots in the closed skull can result in masses that cause pressure on/displace brain tissue and decrease cerebral blood flow, leading to ischemia and infarction
Common locations:
Cerebral lobes
Cerebellum
Characterized by:
Severe headache
Vomiting
Loss of ability to walk
Dysphagia
Dysarthria
Eye movement changes
Pons
Is the most serious bleed location; basic life functions are affected
Characterized by:
Hemiplegia leading to:
Complete paralysis
Coma
Abnormal body posturing
Fixed pupils
Hyperthermia
Death
Thalamus
Results in hemiplegia with more sensory than motor loss
Bleeding in subthalamic areas lead to vision + eye movement
Subcortical white matter
Internal capsule
Putamen (part of basal ganglia)
Manifestations of putaminal/internal capsule bleeding:
Weakness of one side, including the face, arm, and leg
Slurred speech
Deviation of the eyes
Progressions of symptoms related to a severe hemorrhage:
Hemiplegia
Fixed + dilated pupils
Abnormal body posturing
Coma
Subarachnoid
Occurs when there’s intracranial bleeding into the CSF-filled space between the arachnoid and pia mater membranes on the brain’s surface
Causes
Cerebral aneurysm rupture
Trauma
Illicit drug (coke) use
Patient can present with warning signs if the ballooning artery applies pressure to brain tissue
Minor warning symptoms can result from leaking of an aneurysm before major rupture
Manifestations
LOC may/may not occur
LOC ranges from alert → comatose, depending of bleeding severity
Focal neuro deficits (including cranial nerve deficits)
N/V
Seizures
Stiff neck
Complications
Rebleeding before surgery/other therapies start
Cerebral vasospasm, which can result in infarction
Patients with subarachnoid hemorrhage who’re are at risk for vasospasm are often in the ICU for up to 14 days or until the threat of vasospasm is reduced
Peak time is 6-10 days after the initial bleed
Clinical manifestations: strokes
Related to stroke location
Motor function
Most obvious effects of stroke
Deficits include:
Mobility
Respiratory function
Swallowing + speech
Gag reflex
Self-care activities
Symptoms are caused by the destruction of motor neurons in the pyramidal pathway (nerve fibers from the brain that pass through the spinal cord to motor cells)
Characteristic motor deficits
Loss of skilled voluntary movement (akinesia)
Impaired integration of movements
Changes in muscle tone
Altered reflexes
Hyporeflexia → hyperreflexia for most patients
Deficits follow certain specific patterns; a lesion of one side of the brain affects motor function on the opposite side of the body
Communication
Left hemisphere is dominant for language skills in right-handed patients and in most left-handed patients
Aphasia may be present
Types
Receptive - Loss of comprehension
Expressive - Inability to produce language
Global - Total inability to communicate
Occurs when a stroke damages the dominant hemisphere of the brain
Patterns may differ, since strokes affect different portions of the brain
Described as:
Nonfluent - Minimal speech activity with slow speech that requires obvious effort
Fluent - Speech is present, but has little meaningful communication
Dysarthria (problem with muscular speech control) can occur
Impairment can involve pronunciation, articulation, and phonation
Affects the mechanics of speech
Affect
Emotional responses can be exaggerated/unpredictable
Intellectual function
Left-brain strokes are more likely to result in memory problems related to language
Patients with left-brain strokes are cautious in making judgements
Patients with right-brain strokes tend to be more impulsive and move quickly
Patients with either type of stroke find it hard to make generalizations, interfering with their ability to learn
Spatial-perceptual problems
More common in patients after right-brain strokes, but can occur in patients after left-brain strokes
Categories
Incorrect perception of self + illness
Spatial neglect
Agnosia - Inability to ID objects via sight, touch, or hearing
Apraxia - Inability to carry out learned, sequetial movemnts on command
Elimination
Most urinary/bowel problems are temporary
When strokes affect 1 hemisphere, prognosis for normal bladder function is excellent
Though motor control of the bowel usually isn’t a problem, patients are often constipated
Constipation is associated with:
Immobility
Weak abdominal muscles
Dehydration
Decreased response to the defecation reflex
Incontinence can occur if patients can’t communicate their needs to eliminate or have difficulty managing clothing
Scheduled toileting + easily removable clothing encourages independence
Diagnostic studies: strokes
Performed to:
Confirm stroke occurrence
ID likely cause
Guide therapy decisions
Key assessment is to determine symptom onset time
Noncontrast CTs/MRIs
Rapidly distinguish between ischemic/hemorrhagic stroke
Determine size + location of stroke and treatment options
MRIs are more effective in IDing ischemic strokes than CTs
CTs are rapid diagnostic tools to rule out hemorrhage
CT angiography provides visualization of cerebral blood vessels
Can be done at the same time as noncontrast CTs
Give an estimate of perfusion and detect filling defects in cerebral arteries
Magnetic resonance angiography detects vascular lesions/blockages
Cardiac imaging is recommended because many strokes are caused by blood clots from the heart
Blood tests can help ID conditions contributing to stroke and guide treatment
Angiography can:
ID cervical and cerebrovascular occlusion
Atherosclerotic plaques
Malformation of vessels
Cerebral angiographies can find subarachnoid hemorrhages
Angiography risks
Dislodging emboli
Causing vasospasm
Inducing further hemorrhage
Provoking an allergic reaction to contrast media
Intraarterial digital subtraction angiography allows for visualization of blood vessels in the neck and large vessels in the circle of Willis
Reduces contrast dose, uses smaller catheters, and shortens procedure length compared to normal angiography
Considered safer than cerebral angiography due to less vascular manipulation
Transcranial doppler ultrasonography measures velocity of blood flow in major cerebral arteries
Effective in detecting microemboli and vasospasm
Ideal for patients suspected of subarachnoid hemorrhage
Carotid duplex scans detect the cause of the stroke and stratify patients for either medical management/carotid intervention if they’ve carotid stenosis
Lumbar punctures can determine if blood is in the CSF if subarachnoid hemorrhage and CT scans don’t prove it
Avoided in patients if they’re suspected of having obstructed foramen magnums or other signs of increased ICP due to the risk of downward herniation of the brain
This can lead to pressure on cardiac/respiratory centers in the brainstem and potentially death
Inteprofessional care: ischemic strokes
Acute care
Symptoms onset time is the most important part of the patient’s history
Care goals
Preserve life
Prevent further brain damage
Reduce disability
For emergency care, patients should go to the nearest certisfied stroke center
If one’s not available. they should be sent to the closest place offering emergency stroke care
For unconscious patients, care starts with ABC assessment
Perform baseline neuro assessment
Monitor closely for signs of increasing neuro deficit
Elevated BP is common after strokes
It can be protective to maintain cerebral perfusion, but also detrimental
For patients who don’t receive fibrinolytic therapy, antihypertensive usages is recommended only if BP is markedly increased (SBP >220 mmHg or DBP >120 mmHg)
For patients on fibrinolytic therapy, BP must be <185/110 mmHg, then maintained at/below 180/105 mmHg for at least 24 hours after fibrinolytic therapy
In acute strokes, IV antihypertensives are preferred
Fluid/electrolyte balance must be carefully controlled
Goal is to keep patient adequately hydrated to promote perfusion and decrease further brain injury
Decisions are made based on:
Extent of intracranial edema
Manifestations of increased ICP
Central venous pressure levels
Electrolyte levels
I/O
Overhydration can compromise perfusion by increasing ICP and cerebral edema
Adequate fluid intake is a priority
Monitor urine output to ensure + prevent dehydration
Hyponatremia can occur if ADH secretion increases
IV solutions with glucose and water are avoided because they’re hypotonic and can further increase cerebral edema and ICP
Glycemic control should be maintained
Increased ICP is less likely to happen, but usually peaks in 72 hours and cause brain herniation
Management includes
Elevating heads of the bed
Keep the head + neck aligned
Avoid hip flexion
Manage fever (keep temp between 96.8 - 98.6 F)
Drug therapy to prevent seizures
Pain management
Prevent constipation
Drug therapy
Fibrinolytic therapy should not be delayed
IV tissue plasminogen activator (tPA) can reestablish blood flow through a blocked artery and prevent cell death in patients with acute onset of ischemic stroke
Must be given 3 - 4.5 hours of symptom onset
Careful screening must be done before drug admin
Noncontrast CT/MRI to rule out hemorrhagic stroke
Blood tests for coagulation disorders
Screening for recent history of GI bleeding, stroke, or head trauma in the last 3 months
Major surgery in 14 days
Recent active internal bleeding in 22 days
During infusion, close monitor vitals and neuro status to assess for signs of improvements or for potential deterioration related to intracerebral hemorrhage
BP control (SBP <185 mmHg) is critical during treatment and for 24 hours after
Patients can receive intraarterial tPA if mechanical thrombectomy isn’t an option
For effectiveness, must be given in 6 hours of symptom onset
Anticoagulant use in the emergency phase isn’t recommended due to the risk for intracranial hemorrhage
High aspirin doses can be started in 24-48 hours after symptom onset
After patient stabilization and to prevent further clot formation, patients with strokes caused by thrombi/emboli can be treated with anticoagulants and platelet inhibitors
Interprofessional care: hemorrhagic strokes
Drug therapy
Anticoagulants and platelet inhibitors are contraindicated
Involves hypertension management
Oral + IV agents can be used to maintain BP in a normal/high-normal range (SBP <160 mmHg)
Seizure prophylaxis is patient-specific
Surgical therapy
Includes immediate evacuation of:
Aneurysm-induced hematomas
Cerebellar hematomas >3 cm
Treatment of arteriovenous malformations is surgical resection and/or radiosurgery
Catheter embolization of affected vessels can block the blood supply to the AVM
Aneurysms are often treated by permanent clipping/coiling the aneurysm to prevent rebleeding
Interventional radiology procedures include coiling and flow diversion
After clipping/coiling hyperdynamic therapy (hemodilution-induced hypertension) can be started to increased mean arterial pressure and cerebral perfusion
Volume expansion is achieved with crystalloid/colloid solutions
Patients with subarachnoid hemorrhage can receive nimodipine to treat cerebral vasospasms and minimize cerebral damage
Etiology + patho: spinal cord injuries
Types
Primary injury
Results form direct physical trauma to the spinal cord due to blunt/penetrating trauma
Trauma can cause cord compression via bone displacement, interruption of blood supply, or distraction from pulling
Penetrating trauma can cause tearing + transection
Secondary injury
Ongoing, progressive damage that occurs after primary injury
Causes further permanent damage
Starts a few mins after injury + lasts for months
Cascades of events results in edema, ischemia, and inflammation → cell death, blood-brain barrier disruption, and demyelination
Edema from inflammation is especially harmful due to limited space for tissue expansion → cord compression
Extends above + below the injury, increasing ischemic damage
In 24 hours, permanent damage can occur
Apoptosis continues for weeks, contributing to post-injury demyelination
Inflammatory response at the site of the initial injury focuses on clearing up the initial cell debris without damaging normal tissue
Results in a central non-neural core of connective tissue (glial scar)
Glial scars create physical barriers that restrict spinal cord cells from migration + regeneration → irreversible nerve damage + permanent neuro deficit
Spinal + neurogenic shock
Spinal shock can occur shortly after injury; characterized by loss of deep tendon + sphincter reflexes, sensation loss, and flaccid paralysis below level of injury
Lasts days to weeks
Often masks post-injury neuro function
Neurogenic shock can occur in cervical or high thoracic injury (T6 or higher)
Occurs form unopposed parasympathetic response due to loss of sympathetic nervous system innervation
Causes peripheral vasodilation, venous pooling, and decreased cardiac output
Manifestations
Significant hypotension (<90 mmHg)
Bradycardia
Temp dysregulation
Can persist for as long as 5 weeks post-injury
Hypotension can result in poor perfusion + oxygenation to the spinal cord and worsen spinal cord ischemia
Classification
Mechanism of injury
Flexion
Flexion-rotation
Most unstable; ligaments that stabilize the spine are torn
Most often contributes to severe neuro deficits
Hyperextension
Vertical compression
Extension-rotation
Lateral flexion
Level of injury
Skeletal level
Vertebral level with the most damage to vertebra + related ligaments
Neurologic level
Lowest segment of the spinal cord with normal sensory and motor function on both sides of the body
Can be cervical, thoracic, lumbar, or sacral
Cervical + lumbar injuries are most common because those areas are associated with the greatest flexibility + movement
Injury from C1 - T1 can cause tetraplegia
Degree of impairment in the arms after cervical injury depends on level of injury
Lower level = more functionality retained
Paraplegia can occur in injuries below T2
Degree of injury
Complete
Results in total loss of sensory + motor function below level of injury
Incomplete
Results in a mixed loss of voluntary motor activity + sensation and leaves some tracts intact
Degree of sensory + motor loss depends on the level of injury and reflects specific damaged nerve tracts
Five major associated syndromes
Central cord
Anterior cord
Brown-Séquard
Cauda-equina
Conus medullaris
Clinical manifestations: spinal cord injuries
C-spine injuries
Dysnpea/apnea
Quadriplegia
Cervical injuries above C3 present special problems because of the total loss of respiratory muscle function
Patients have respiratory arrest within minutes of injury if not intubated
Patients with high C-spine injury C3-5 have respiratory insufficiency due to loss of phrenic nerve innervation to the diaphragm and decreased chest + abdominal wall strength
Patients with complete injury above C5 should be intubated immediately
T-spine injuries often result in paraplegia
C + T-spine injuries cause paralysis of abdominal muscles and often the intercostal muscles
Patients can’t cough effectively enough to remove secretions → increased risk for aspiration, atelectasis, and pneumonia
Hypoventilation + impairment of intercostal muscles lead to decreased vital capacity + tidal volume
Any cord injury above T6 leads to sympathetic nervous system dysfunction
Can result in bradycardia, peripheral vasodilation, and hypotension (neurogenic shock)
Lumbar/sacral spine injuries often result in decreasing control of
Legs
Bowel/bladder function
Sexual function
Nursing care: spinal cord injuries
Health promo
ID high-risk patients + provide education
Support measures to combat distracted/impaired driving
Teach peoples to use child safety seats + helmets for motor/bicyclists
Promote programs for older adults aimed at preventing accidental death + injury
Emphasize the importance of health promo + screening behaviors after injuries
Acute care
Immobilization
Maintain necks in neutral positions
Closed reductions with skeletal traction is used for early realignment of C-spine injuries
If pin displacement occurs, hold patient’s head in neutral position + call for help
Immobilize the head while providers reinsert tongs
Pin care is essential; clean pins twice daily with CHG
Skin care is vital; decreased sensation + circulation increase the risk for skin breakdown
Remove patient backboards asap + replace with other forms of immobilization to prevent skin breakdown in the coccygeal + occipital areas
Fit C-collars properly
Assess areas under any devices used for immobilization
Respiratory problems
Monitor patients for respiratory compromise
Regularly assess
Breath sounds
ABGs
Tidal volume
Vital capacity
Skin color
Breathing patterns
Subjective comments about breathing ability
Amount + color of sputum
Patients who can’t count to 20 without taking a breath need immediate attention
Provide measures to maintain ventilation
Apply oxygen + provide appropriate ventilatory support until ABGs stabilize
If patients are exhausted from labored breathing or ABGs show inadequate oxygenation/ventilation, endotracheal intubation or tracheostomy, and mechanical ventilation is needed
Perform suctioning if crackles or coarse breath sounds are present
Cardiovascular instability
Frequently assess vitals
If bradycardia is symptomatic, give anticholinergics (atropine)
Maintain SBP >90 mmHg and keep MAP between 85-90 mmHg for first 7 days after injury
Manage hypotension with fluid replacement + vasopressors
Maintain normal blood volume
Monitor H/H per protocol
Assess patients for sign of hypovolemic shock from hemorrhage
Assess orthostatic BP when mobilizing the patients
For symptomatic patients, use abdominal binders + TED hoses to promote venous return
Give meds to increase intravascular volume (salt tabs, fludrocortisone) as ordered
Midodrine can be given to promote vasoconstriction + increase venous return
Use low-molecular-weight heparin in combo with SCDs or TED hoses to promote venous return + reduce VTE risk
Elimination
Maintain patency of Foleys
Check catheters to prevent kinking and ensure free flow of urine
Use strict aseptic technique for catheter care to prevent infection
Encourage large fluid intake while catheters are in place
When patients are stable, assess best means of managing long-term urine function
Straight caths are the preferred methods
Should be done 4-6 times/day to prevent bacterial overgrowth from urine stasis
Keep urine residuals <500 mL to prevent bladder distention
If signs of a UTI present, send specimens for culturing
Start bowel programs to combat constipation from neurogenic bowel
Can be started with patients still in bed, but when they start sitting, they should be upright on a bedside commode
Enforce measures to reduce constipation
Interprofessional care: spinal cord injuries
Prehospital
Spinal motion should be restricted with a combo of a rigid C-collar and a supportive backboard with straps
Most patients are kept supine, and some in revere Trendelenburg
Sedation can be given to keep combative patients safe from further injury
Intubation to secure airways is done asap for patients with respiratory distress
End-tidal CO2 monitoring can help determine the need for rapid sequence intubation
Thorough assessments determine the degree of deficit and the level + degree of injury
Acute care
Obtain histories + mechanism of injury
Assess injury extent perceived by patient or EMS
Ensure secure airway
Maintain O2 sats >92% and MAP >85 mmHg
Avoid SBP <90 mmHg
Neurogenic shock is treated with IV fluids + pressors to maintain SBP >90 mmHg after other causes of hypotension are ruled out
Perform complete neuro assessments using ASIA tool
Muscle groups are tested with + against gravity, alone + with resistance, on both sides of the body
Record strength, symmetry, and spontaneous movement
Complete sensory assessment, including touch + pain, as tested by pinprick
Start at toes + work upward to the head
Assess rectal tone
Voluntary anal contractions indicate incomplete injuries
Note presence of priapism
If time + conditions permit, assess position sense + vibration
Note signs of concussion + increased ICP
Assess for musculoskeletal injuries + trauma to internal organs
The only clue to internal trauma + bleeding may be a rapidly dropping BP + increasing pulse
Move patients via logrolls during transfers + when repositioning to prevent further injury
Monitor respiratory, cardiac, urinary, and GI functions
Drug therapy
VTE prophylaxis should start in 72 hours of injury unless contraindicated
Internal/external bleeding
Recent surgery
For those with abnormal kidney function, heparin is best
Vasopressors are used in the acute phase of injury as adjuvant treatment
They maintain MAP to improve perfusion to the spinal cord
Complication risk is high
V-tach
Troponin elevation
Metabolic acidosis
A-fib
Complications: spinal cord injuries
Autonomic dysreflexia
Massive, uncompensated cardiovascular reaction mediated by the sympathetic nervous system
Involves stimulation of sensory receptors below injury level
Most common precipitating cause is a distended bladder/rectum, but any sensory stimulation can cause it
Life-threatening + requires immediate resolution
Proper ID + elimination of inciting stimulus can resolve the event
If untreated, can lead to status epilepticus, stroke, MI, and death
Clinical manifestations
Hypertension
Throbbing headache
Marked diaphoresis above injury level
Bradycardia
Piloerection from pilomotor spasm
Flushing, above injury level
Blurred/spotty vision
Nasal congestion
Anxiety
Nausea
Measure BP when patients with spinal cord injuries report headaches
Suspected in adults with SBP elevation of 20-40 mmHg above baseline
Interventions
Elevate head of bed 45 degrees or sit patients upright
Determine cause
Most commonly bladder distention; immediate catheterization can be done
If catheters are in placed, check for kinks/folds in tubing
If clogged, perform small-volume irrigation slowly and gently to open or insert a new one
If stool impaction, apply anesthetic ointments to avoid increasing symptoms, then perform digital rectal exam
Notify provider
Remove all skin stimuli (constrictive clothes, tight shoes)
Monitor BP
If symptoms persist after source removal, give rapid-onset + short-duration agents (nitroglycerin, nitroprusside, hydralazine)
Continue careful monitoring until vitals stabilize
Teach patients + caregivers to recognize causes + symptoms; they must know the extreme danger and know to call for help if needed
Neurogenic bladder
The type of bladder dysfunction determines management options
When patients stabilize + assessments show return of neuro reflexes, urodynamic testing + urine cultures can be done
Patients need a comprehensive program to manage bladder function
For chosen plans, teach patients + caregivers successful self-management
Teach about various management techniques, how to obtain supplies, care of supplies + equipment, and when to seek health care
Meds
Anticholinergics suppress bladder contraction
Alpha-adrenergic blockers relax the urethral sphincter
Antispasmodics decrease spasticity of pelvic floor muscles
Botulism toxin helps patients with neurogenic detrusor overactivity who can’t tolerate or have an inadequate response to anticholinergics
Evaluate long-term use of Foleys due to high CAUTI incidence, fistula formation, and diverticula
Patients must have adequate fluid intake (3-4 L/day)
Regularly check catheter patency
Straight caths are the first-line option for bladder management
Initially done q4h
Measure PVR before catheterization
If <200 mL, the time interval until catheterization can be extended
If >500 mL, the time interval is reduced
Usually done 4-6 times/day
Neurogenic bowel
Usual measures for constipation prevention include high-fiber diets + adequate fluid intake
Suppositories + small-volume enemas and digital stimulation (done 20-30 mins after suppository insertion may be needed
For patients with upper motor neuron injuries, digital stimulation can relax external sphincters to promote defecation
Stool softeners can help regulate stool consistency
Oral stimulant laxatives should be used only when necessary and not on a regular basis
Valsalva maneuvers + manual stimulation are useful in patients with lower motor neuron injuries
Valsalva is used in patients with injuries below T12
Generally, bowel movements every other day is adequate, but consider pre-injury bowel patterns
Defecation timing is important; planning bowel evacuation for 30-60 mins after first meals of the day can enhance success by taking advantage of the gastrocolic reflex induced by eating
Discuss timing of bowel programs so there are no interruptions when patients are performing therapy
Record all bowel movements, including amount, time, and consistency
hyperacute rejection
Occurs in 24 hours of transplantation
Occurs because recipient had preexisting antibodies against the transplanted tissue/organ
No treatment exists; transplanted organ must be removed
Rare due improved immunosuppression meds + final tests done before transplantations to determine recipient sensitivity to donor HLAs
acute rejection
Most often occurs in the first 6 months of transplantation
Usually cell-mediated response by recipient lymphocytes, which are activated against donated tissue/organ
Can occur when recipients develop antibodies to the transplanted organ (humoral rejection)
Common, especially with organs from deceased donors
Usually reversed with additional immunosuppressant therapy
Increased corticosteroids or poly/monoclonal antibodies
chronic rejection
Occurs over months/years + is irreversible
Can occur from unknown reasons or from repeated episodes of acute rejection
Results in fibrosis + scarring
Heart → accelerated CAD
Lung → bronchiolitis obliterans
Liver → Loss of bile ducts
Kidney → Fibrosis + glomerulopathy
No definitive treatment; care is mainly supportive
Immunosuppression therapy + side effects
Calcineurin inhibitors (cyclosporine, tacrolimus)
Work by preventing cell-mediated attacks against transplanted organ
Patients should avoid grapefruit/grapefruit juice; increases toxicity
Side effects
Kidney toxicity
Increased infection risk
Neurotoxicity (tremors/seizures)
Lymphoma
Hypertension
Hirsutism
Leukopenia
Gingival hyperplasia
Purine synthesis antagonists
Azathioprine
Side effects
Bone marrow suppression
Neutropenia
Anemia
Thrombocytopenia
Mycophenolate mofetil
Inhibits purine synthesis + suppressive effects on T + B cells
Can only be reconstituted in D5W
Never bolus doses; admin over 2 hours
Side effects mediated by lowering doses or giving smaller doses more often
Side effects
N/V/D
Neutropenia
Thrombocytopenia
Increased infection risk
Increased cancer risk
Sirolimus
Suppresses T-cell activation + proliferation
Side effects
Increased infection risk
Leukopenia
Anemia
Thrombocytopenia
Hyperlipidemia
Hypercholesterolemia
Arthralgias
Diarrhea
Increased cancer risk
Clinical manifestations: graft v. host disease
Skin
Can be an itchy/painful maculopapular rash
Initially involves palms + soles
Can progress to generalized erythema + bullous formation + desquamation
Liver
Can range from mild jaundice + high liver enzymes → hepatic coma
GI tract
Manifestations
Mild/severe diarrhea
Severe abdominal pain
GI bleeding
Malabsorption
Nursing + interprofessional care: graft v. host disease
No adequate treatment exists
Corticosteroids are most often used, but enhance infection risk
Immunosuppression has been most effective in prevention rather than treatment
Radiating blood products before admin can help prevent T-cell replication
Clinical manifestations: malnutrition
Most obvious signs are seen in the:
Skin
Dry + scaly
Brittle nails
Rashes
Hair loss
Mouth
Crusting + ulceration
Tongue changes
Muscles
Decreased mass
Weakness + fatigue
CNS
Mental changes (confusion, irritability)
Delayed wound healing
Increased infection risk
Anemia
Nursing + interprofessional care: malnutrition
Assessment
TJC requires nutrition screening for all patients in 24 hours of admission with detailed assessments for at-risk patients
The Malnutrition Universal Screening Tool + Nutrition Risk Screening are commonly used with adults in acute care
Mini Nutritional Assessments are used for older adults
Obtain height, weight, and girth measurements
Calculate BMI
<18.5 = underweight
18.5 - 24.9 = normal weight
25 - 29.9 = overweight
30+ = obese
40+ = extremely obese
When possible, measure actual height instead of using patient’s self-report
When assessing weight, obtain a detailed weight history, noting weight loss + intentionality and duration
Losses of >5% of usual weight over 6 months is a critical indicator for further assessment, especially in older adults
If involuntary losses are >10% of usual weight, determine the reason
Health promo
Teach + reinforce healthy eating habits
Use MyPlate, the Dietary Guidelines for Americans, and Nutrition Facts food labels to promote health nutrition
Help patients find reliable internet sources that provide evidence-based food + nutrition recommendations
Acute care
Collab with providers + dieticians to ID patients with malnutrition and implement appropriate interventions to meet patient’s nutrition needs
Assess nutrition during physical assessments
ID risk factors + rationale behind them
Teach patients + caregivers the importance of good nutrition
Discuss rationale for daily weights, + I/O
Measure height + weight on admission
If can eat PO, obtain daily calorie count + diet dairy to give an accurate of food intake
Help patients + caregivers choose high-calorie and high-protein foods unless medically contraindicated
Offering foods the patient likes enhances intake
Ensure environments are conducive to eating
Provide quiet time
Offer hand + oral hygiene
Help patients get comfortable positions
Place bedside tables at right heights + clear of clutter
Place urinals, basins, and bedpans out of sight
Open cartons + packages if needed
Protect mealtimes for unnecessary interruptions by performing nonurgent care before/after mealtime
Malnourished patients may need between-meal supplements; if patients can’t consume enough nutrients via high calorie + protein diets, consider oral liquid supplements
Monitor for refeeding syndrome
Body’s response to the switch from starvation to a fed state in the initial phase of nutrition therapy in patients who are severely malnourished
Risk factors
Chronic alcohol use
Cancer
Trauma
IBD
Major surgery
Manifestations
Hypophosphatemia
Hyperglycemia
Fluid retention
Hypokalemia
Hypomagnesemia
Dysrhythmias
Respiratory arrest
Ambulatory care
Teach patients + caregivers about the cause for malnutrition and ways to avoid
Malnourishment can recur
Adhering to their diet for a few weeks can’t fully restore a normal nutrition state; can take months to reach such a goal
Assess ability to follow diet instructions considering past eating habits, religious/ethnic preferences, age, income, resources, and general health
Emphasize the need for continual follow-up care to achieve + maintain rehab
Determine needs for nutritious meals + snacks after discharge
Encourage patient self-assessment of progress by having them weigh themselves 1-2x/week + keep weight record
Health risks: obesity
Cardiovascular problems
Android obesity is the best predictor of cardiovascular disease + strokes in men + women
It’s linked with increased LDLs, high triglycerides, and decreased HDLs
Hypertension can occur due to
Increased circulating blood volume
Abnormal vasoconstriction
Increased inflammation (damaging blood vessels)
Increased risk for sleep apnea (raises BP)
Excess body fat can lead chronic inflammation through the body, especially blood vessels, increasing the risk for heart disease
Diabetes
Obesity is the greatest risk for developing T2D
Hyperinsulinemia + insulin resistance are often found in obesity
Excess weight decreases insulin effectiveness → hyperglycemia
Obesity complicates management of T2D by increasing insulin resistance + glucose intolerance
Adiponectin (adipokine that increases insulin sensitivity) is decreased → decreased drug effectiveness
GI + liver problems
GERD + gallstones are more prevalent
Nonalcoholic steatohepatitis (NASH) is a condition in which lipids are deposited in the liver → fatty liver
NASH can increase hepatic glucose production, worsen to cirrhosis and lead to death
Respiratory + sleep problems
Increased fat mass → sleep apnea + obesity hypoventilation syndrome
Poor sleep + sleep deprivation can increase appetite
Building up sleep debt over a matter of days can impair metabolism and disrupt hormone levels
Leptin levels fall in those who are sleep deprived → increased appetite
Musculoskeletal problems
Obesity is associated with an increased incidence of osteoarthritis from the stress put on weight-bearing joints, especially knees + hips
Increased body fat triggers inflammatory mediators + contributes to cartilage deterioration
Hyperuricemia + gout often occurs in patients who are obese and those with metabolic syndrome
Cancer
Obesity is the one of the most preventable causes of cancer
Cancers linked to excess body fat
Breast
Endometrial
Esophageal
Gallbladder
Kidney
Liver
Ovarian
Stomach
Thyroid
Psychosocial problems
Obesity is heavily stigmatized, which can have a emotional toll on psychologic wellbeing
Restrictive bariatric surgeries
Adjustable gastric banding
Involves limiting stomach size with an inflatable band placed around the fundus of the stomach
Band is connected to a SQ port that can be in/deflated to meet patient needs
Divides the stomach into 2 unequal parts
Upper part acts as the new stomach; it holds less → patients feel full faster
Bands delays stomach emptying, providing patients with further satiety
Can be modified/reversed at later dates if needed
Preferred option for patients who are surgical risks because its done laparoscopically
Risks
Band slippage
Some food intolerance
Patients must follow strict diets to lose + not regain the weight
Sleeve gastrectomy (gastric sleeve)
~75% of the stomach is removed, leaving a sleeve-shaped stomach
Size is reduce + function preserved
Eliminates hormones made in the stomach that stimulate hunger (ghrelin)
Gastric plication
Reduces stomach size by folding stomach inwards
Reversible
Intragastric balloons
Use inflated balloons to occupy stomach space
Helps patients feel more full + reduce amount of food they can eat
Contraindications
Past GI surgery
IBD
Large hiatal hernia
Delayed gastric emptying
Active H. pylori infection
Side effects
N/V
Abdominal pain
Indigestion
Combo (restrictive + malabsorptive) bariatric surgeries
Roux-en-Y gastric bypass
Combo of restrictive + malabsorptive surgery
Results in food bypassing 90% of the stomach, duodenum, and a small segment of the jejunum
Complications
GI tract leaks
Gastric remnant distention
Ulcers
Gallstones
Hernias
Iron deficiency anemia
Cobalamin deficiency → chronic anemia
Dumping syndrome
Too rapid emptying of gastric contents into the small intestine → overwhelming nutrient digestion
Manifestations
N/V/D
Weakness
Faintness
Patients are discouraged from eating sugary foods for prevention
Complications: bariatric surgeries
Nursing care: bariatric surgeries
Preop
Interview patients to obtain past + current health info and assistive devices currently use
Focus on IDing comorbidities that increase the risk for postop complications
Have plans in place before patients arrive so they receive optimal care + don’t feel embarrassed
Have appropriately size gowns, beds, and commodes that accommodate increased body sizes + needed patient transfer equipment
Use larger BP cuffs to avoid measurement errors + ensure availability and placement in patient room
Wheelchairs with removable arms that’s large enough to safely accommodate patients + pass easily through doors should be available
Modify assessment methods/tools to ensure accuracy
Teach coughing + deep breathing techniques and methods to turning to prevent pulmonary complications
Show appropriate use of incentive spirometry
If patients use CPAPs at home, arrange for its use in the hospital
Special considerations
Ensure patients understand the procedure
Emphasize frequent assessments of vitals + general assessments to monitor for complications
Tell patients they’ll be helped with ambulation soon after surgery
Postop
Initially focuses on careful assessment + immediate intervention cardiopulmonary complication
During patient transfers, keep airways stabilized
If sedation persists after surgery, be prepared to perform head-tilt jaw thrusts to keep oral + nasal airways open
Keep heads of bed elevated to reduce abdominal pressure + increased lung expansion
Administer oxygen as needed
Implement VTE precautions; diligence in turning + ambulation will help
Patients usually will start walking the evening after surgery and then at least 3-4 times/day
Have proper help + equipment available
Assess skin often
Keep skin fold clean + dry to prevent dermatitis + infection
Implement measures to reduce pressure injuries
Special considerations
Give pain meds PRN
Monitor vitals to help ID problems
Patients usually start low-sugar, clear-liquid diets in 24 hours postop
Start with 150mL increments every 10-15 mins; if no nausea/problems arise, gradually increase intake to a goal of 90 mL/30 mins
Teach patients to avoid gulping fluids or drinking with straws to reduce the incidence of air swallowing
Instruct patients to avoid caffeinated drinks
Ambulatory care
Patients must clearly understand their diet restrictions
They’re usually discharged on full liquid diets
In 10-14 days, depending on tolerance, pureed/soft foods + vitamin supplementation is started
Most patients start usual diets 4-6 weeks postop
Diets are usually high in protein with some carbs + fiber
They should consist of 6 small feedings/day
Patients shouldn’t drink fluid with meals; increases risks of diarrhea + dumping syndrome
Calorie-dense foods should be avoided to permit more nutritious food to be consumed
Teach patients to eat slowly + stop when feeling full
Emphasize the importance of follow-up care due to potential complications
Teach patient to inform providers of any changes to physical/emotional condition
Patient should take multivitamins with folate, calcium, vitamin D, iron, and cobalamin for life
Peptic ulceration, dumping syndrome, and small bowel obstructions can be seen late in recovery and rehab stage
Psychologic issues can arise postop
Assess social functioning, self-esteem, sex life, and ADLs in follow-up care
Be prepped to provide support + assist patients in moving away from negative feelings
Help patients adjust to new body image several months postop
Discuss the possibility of excess loose skin postop + during the rehab phase
Don’t hesitate to encourage counseling for unresolved psychologic issues
Encourage women to postpone pregnancy for 12-18 months postop
Etiology + patho: peptic ulcer disease
Ulcers develop only in acidic environments, but excess acid isn’t needed for development
Risk factors
H. pylori
Major risk factor
Infection usually occurs during childhood with transmission form family to kids, possibly through fecal → oral or oral → oral
Medication-related
NSAID use is responsible for most non-H. pylori ulcers
NSAID use + H. pylori infection increases risk of peptic ulcer disease
Corticosteroids and anticoagulants + NSAIDs increase risk
Lifestyle factors
High alcohol intake can cause acute mucosa lesions
Alcohol + smoking stimulate acid secretion
Coffee is a strong stimulant of gastric acid secretion
Smoking + psychologic distress (stress + depression) can delay ulcer healing upon development
Clinical manifestations: peptic ulcer disease
Gastric
Epigastric pain, 1-2 hours after meals
Described as burning/gaseous
If ulcer erodes through mucosa, food can worsen pain
Duodenal
Pain occurs when in contact with stomach acid
Food eases pain; symptoms occur 2-5 hours after eating
Described as burning/cramping
Located in midepigastric region, beneath xiphoid process
Back pain
N/V
Early satiety
Some patient can be asymptomatic “silent peptic ulcers”
More likely to occur in older adults + those on NSAIDs
Complications: peptic ulcer disease
GI bleeding
Most common; duodenal ulcers cause more bleeding episodes
Perforation
Most lethal complication
Risk is highest with large penetrating duodenal ulcers
Clinical manifestations
Sudden + severe upper abdominal pain that radiates quickly throughout the abdomen
Radiating pain to the back + shoulders
Pain unrelieved by food/antacids
Abdominal rigidity; appears board-like
Absent bowel sounds
N/V
Increased + weak pulse
Untreated, bacterial peritonitis can occur in 6-12 hours; severity is proportional to the amount + duration of spillage through the perforation
Immediate management
Stop spillage of gastric/duodenal contents into the peritoneal cavity
NG tubes provide continuous aspiration + gastric decompression to stop spillage throughout the perforation
For duodenal aspiration, NG tubs are placed as close to the perforation site as possible to promote decompression
Restore blood volume
Replaced with LR + albumin solutions
Substitute for fluids lost from vascular + interstitial space as peritonitis
Packed RBCs can be needed
CVLs + Foleys can be placed + monitored hourly
Patients with a history of heart disease need ECG monitoring or a PA cath for assessing left ventricular function
Broad-spectrum antibiotics are started immediately to treat bacterial peritonitis
Small perforations can seal themselves + symptoms stop
Can lead to fibrinous fusion of the duodenum or gastric curvature to adjacent tissues (mainly the liver) and strictures that can obstruct the flow of intestinal contents and the passage of stool
Large perforations need immediate surgical closure; laparoscopic or open repair depends on ulcer location + provider preference
Gastric outlet obstruction
Obstruction is the distal stomach + duodenum is the result of edema, inflammation, pylorospasm, or fibrous scar tissue formation
Patients report discomfort + pain that’s worse at the end of the day as the stomach fills + dilates
Burping/vomiting can provide some relief
Vomiting is common + often projectile in nature
Vomitus can contain food particles that were consumed hours/days before
Constipation occurs from dehydration + decreased diet intake form anorexia
Treatment aims to decompress the stomach, correct fluid/electrolyte imbalances, and improve patient general health
NG tubes can provide continuous decompression, allowing the ulcer to start healing + edema is subside
Pain relief results from decompression
IV fluids/electrolytes are replaced according to the degree of dehydration, vomiting, and electrolyte imbalance shown by lab tests
PPI/H2 receptor blockers are used if obstruction are due to active ulcers
Interprofessional care: peptic ulcer disease
Conservative
Consists of adequate rest, drug therapy, smoking cessation, diet mods (if needed), and long-term follow-up care
Pain disappears after 3-6 days
Ulcer healing is slower; completion can take 3-9 weeks, depending on size, treatment, and patient adherence to care plan
Follow-up endoscopic exams are done 3-6 months after diagnosis + treatment
Aspirin + nonselective NSAIDs are stopped for 4-6 weeks
Wen aspirin must be continued, its given with a PPI, H2 receptor blocker, or misoprostol
Enteric-coated aspirin decreases localized irritation but doesn’t reduce overall risk for GI bleeding
Drug therapy
Focuses on reducing gastric acid secretion and/or eliminating H. pylori infection
Patients with H. pylori infections need treatment with antibiotics + PPIs
Due to high recurrence rates, interruptions/sudden cessation of meds can be harmful
Encourage patients to adhere to therapy + continue with follow-up care as ordered
Teach patients + caregivers about each prescribed med, its rationale, and expected benefits
Review actions to take if pain + discomfort recur or if there’s blood in vomit/stool
Antibiotics
Is prescribed with a PPI for 14 days
If patients are allergic to penicillin, metronidazole is used instead
Bismuth can given alone or in a combo capsule with bismuth, tetracycline, and metronidazole
PPIs
More effective than H2 receptor blockers in reducing gastric acid secretion + promoting ulcer healing
Used in combo with antibiotics to treat ulcers caused by H. pylori
Cytoprotective drugs
Sucralfate is used for short-term ulcer treatment; provides mucosal protection for the esophagus, stomach, and duodenum
Most effective in acidic environments; give 60 mins before/after antacids
Reduces bioavailability of
Cimetidine
Digoxin
Warfarin
Phenytoin
Tetracycline
Adjunct drugs
H2 receptor blockers + antacids can used as adjunct therapy to promote healing
Antacids neutralize stomach acid → reducing acid content of chyme reaching the duodenum
Some can bind to bile salts (aluminum hydroxide) → decreasing damaging effects of bile on gastric mucosa
Misoprostol prevents gastric ulcers caused by NSAIDs + low dose aspirin therapy
Can cause diarrhea + abdominal pain
Teratogenic; pregnant patients should avoid
TCAs (imipramine, doxepin)
Help with pain relief via effects on afferent pain fiber transmission
Anticholinergic effects → reduced acid secretion
Anticholinergics can also be used
Nutrition therapy
No specific diets helps to treat
Patients should consume things that don’t cause distressing symptoms
Common irritable foods
Pepper
Carbonated drinks
Broths
Hot + spicy
Caffeinated foods/drinks
Patients should avoid alcohol; it delays healing
Surgical therapy
Reserved for those who are unresponsive to medical management or concerns about stomach cancers
Nursing care: peptic ulcer disease
Health promo
ID at-risk patients
Encourage patients on ulcerogenic meds to take them with food
Teach patients to report symptoms related to gastric irritation, including epigastric pain, to their providers
Acute care
Explain to patients + caregivers the rationale for therapies
Provide regular regular oral care to relieve dry mouths
Clean + lubricate nares to decreased soreness
Take vitals initially and then at least hourly to detect + treat shock
Give IV fluids as ordered
Record I/O
Promote quiet + restful environments
Give pain meds as ordered
Be cautious when give sedatives to patients who are becoming increasingly restless; meds can mask signs of shock form GI bleeds
GI bleeding
Changes in vitals + increase in amount and redness of aspirate can indicate bleeding
Pain often decreased because blood helps neutralize acidic gastric contents
Maintain NG tube patency so that blood clots don’t obstruct tubes
Perforation
If patients develop manifestations of perforations, notify providers immediately
Take vitals promptly + record q15-30mins
Give IV fluids as ordered to replace the depleted plasma volume
Give pain meds as ordered
If possible, prep patients + caregivers on the possibility/reality of surgical therapy
Gastric outlet obstruction
Regularly irrigate NG tube with normal saline per agency policy to assist proper functioning
Reposition patients from side to side so that the tubes are constantly lying the mucosal surface
Maintain accurate I/O records, especially of the gastric aspirate
To check for ongoing obstruction, clamp NG tubs intermittently and measure gastric residual volume
Frequency + amount of time that tubes are clamped are related to the amount of aspirate obtained and patient comfort level
Common method is to clamp tubes overnight (8-12 hours) and measure gastric residual volume in the morning
When aspirate is <200 mL, patients can start clear liquid diets; fluids start at 30 mL/hr and gradually increased
As gastric residual decreased, solids are added, and tubes removed
If patients resume oral feeds and symptoms of obstruction are noted, notify providers immediately
Usually, gastric aspiration is continued until edema + inflammation resolve
IV fluids/electrolytes keep patients hydrated
If conservative therapy fails, surgery is done after the acute phase passes
Ambulatory care
Teach patients about prescribed drugs, actions, side effects, and dangers if omitted
Ensure patients know not to take OTCs unless approved by providers
Tell patients to check with providers before changing from a prescription → OTC H2 receptor block/PPI med to avoid side effects and incorrect dosing
Obtain info on patient psychosocial status
Provide info on negative effects of alcohol and cigarettes on ulcers + healing
Teach patients with chronic peptic ulcer disease about potential complication + actions to take until they see provider
Emphasize the need for long-term follow-up care
Encourage patients to seek immediate intervention if symptoms recur
Patient teaching
Avoid distressing foods, such as acidic foods
Avoid smoking + alcohol
Avoid OTCs unless approved by provider
Don’t change brands of meds without provider approval
Followed prescribed drug therapy to prevent relapse
Report
Increased N/V
Increased epigastric pain
Blood emesis/tarry stools
Learn + use effective stress management methods
Share concerns about lifestyle change + living with chronic condition
Etiology + patho: gastric ulcers
Can occur in any part of the stomach; most often in the antrum
Less common than duodenal
Higher mortality rate
More likely to cause obstructions
Risk factors
H. pylori
NSAIDs
Bile reflux
Etiology + patho: duodenal ulcers
Account for most occurrences
Can occur at any age
H. pylori is the most common risk factors
Development is often related to high stomach acid secretion
Tend to occur continuously for a weeks/months, disappear, and recur later
Risk factors
COPD
Cirrhosis
Pancreatitis
Hyperparathyroidism
CKD
Zollinger-Ellison syndrome
Nursing care: bowel resection surgery
Preop
Special considerations
Psychologic prep
Educational prep
Selecting the best stoma site
If possible, WOCNs should visit with patients + caregivers to determine patient ability to perform self-care, ID support systems, and determine and mods that can promote learning during recovery
Psych + emotional support are important, as patients start to cope with the changes in body image + elimination
Patients + caregivers should understand the extent of surgery planned
Provide them with chances to share concerns/questions; will enhance patient feelings of control + coping ability
WOCNs should choose the site where ostomies will be + mark abdomens before surgery
Sites should be within the rectus muscle, on a flat surface, and in a place where patients can see
When possible, it should be discreetly hidden under clothes + appropriate for normal activities
Postop
If patients’ wound are closed/partially closed, assess integrity of the incision
Monitor for complications
Delayed wound healing
Hemorrhage
Fistulas
Infections
Assess wounds regularly + record bleeding, excess drainage, and unusual odors
Monitor for edema, redness, and drainage, as well as fever and a high WBC count
Keep areas around drains clean + dry
Patients with open wounds with packing need meticulous care
Reinforce dressings + change often during first several hours postop when drainage is likely to be profuse
Carefully assess all drainage for amount, color, and consistency
If ostomies are present, assess stoma + place clear pouching system
Stomas should be rosy pink → red + mildly swollen
Assess + document stoma color q4h + ensure there’s excess bleeding
Report any sustained color changes or bleeding to providers
Edema will resolve over the first 6 weeks
Colostomies start functioning when peristalsis returns
Record volume, color, and consistency of drainage
When done on colons not cleared preop, stool will drain when peristalsis returns
If colons were cleared preop, stool will produce a few days after patients start eating again
Excess gas are common during the first 2 week; assure patients that this is temporary
In the first 24-48 hours postop, drainage amount form ileostomies can be negligible
When peristalsis returns, output can be as high as 1500 - 1800 mL/day
If the small bowel is shortened by surgery, drainage can be greater due to the loss of absorptive functions provided by the colon + delay provided by the ileocecal valve
Observe patients for fluid/electrolyte imbalances, particularly potassium + sodium
Over a period of days/weeks, proximal small bowel adapts + increases fluid absorption; feces will thicken to a paste-like consistency + volume will decreased to ~500 mL/day
Patients, especially those with Crohn’s are at risk for developing obstructions during the first 30 days postop
After intraoperative manipulation of the anal canal, transient incontinence of mucus can occur
Have patients start Kegel exercises ~4 weeks postop to strengthen the pelvic floor + sphincter muscles
Teach patients to perform perianal skincare to protect the epidermis from mucous damage and maceration
They should gently the skin with a mild cleanser, rinse well, and dry thoroughly
Some report phantom rectal pain or still feel the need to have a bowel movement; normal + will subside over time
Be aware to distinguish phantom pain from perineal abscess pain
Sexuality
Discuss sexuality + sexual functions with patients; help them realize that it takes time to adjust to the pouch + body changes before feeling secure with sex
Teach patients to empty pouches before sex
Ostomy care
Inpatient care
Assess + document stoma + peristomal skin appearance
Assess patient prep for ostomy care
Help patient with managing psych impact of stoma + effect on body image and self esteem
Choose appropriate ostomy pouching system
Monitor volume, color, and odor of drainage
Develop care plan for peristomal skin care
Teach ostomy self-care to patients
Irrigate new ostomies, if needed
Teach patient + caregiver about proper diet choices
Patient teaching
Explain ostomy + functionality + rationale for operation
Demonstrate + request return demo of:
How to remove old barriers, clean peristomal skin, and properly apply new barriers
Apply, empty, clean, and remove pouch
Empty pouch before 1/3 full
Irrigate ostomy to regulate bowel elimination (optional)
Explain how to contact WOCN
Describe how to obtain ostomy supplies
Explain diet + fluid management
Avoid foods that cause diarrhea/gas
Maintain fluid intake of 3k L/day, unless contraindicated
Increase fluid intake in hot weather
Recognize signs of fluid/electrolyte imbalance
Chew food well to reduce blockage risk
Psychologic adaptation
Provide info in an easily understood manner + help patients develop confidence + competence in stoma management
Help patients ID coping methods
Encourage participation + support from families/caregivers/friends
Encourage patients to share concerns + ask questions
Etiology + patho: abdominal trauma
Blunt trauma often occurs from MVCs, direct blows, and falls
May not be obvious due to no open wound
Compression + shearing injuries can occur with blunt trauma
Penetrating injuries occur when GSWs/stabbings leave obvious + open wounds
When solid organs are injured, bleeding can be profuse → hypovolemic shock
When content form hollow organs spill into the peritoneal cavity → peritonitis risk
Clinical manifestations: abdominal trauma
Intraabdominal injuries are often associated with
Rib fractures
Fractured pelvis
Spinal injury
Thoracic injury
Patients in MVCs can have contusions/abrasions across the lower abdomen
Indicative of internal organ trauma from seatbelts
Seatbelts can produce blunt trauma to abdominal organs by pressing intestines + pancreas into the spinal column
Guarding + splinting of the abdominal wall (indicative of peritonitis)
Hard + distended abdomen (indicative of intraabdominal bleeding)
Decreased/absent bowel sounds
Abrasions/bruising over the abdomen
Abdominal pain
Hematemesis/hematuria
Signs of hypovolemic shock
Hypotension
Tachycardia
Decreased LOC
Tachypnea
Cullen sign (bruising around the umbilicus)
Grey Turner sign (bruising around the flanks)
Bowel sounds in the chest, with diaphragm rupture
Bruit auscultation → arterial damage
Nursing + interprofessional care: abdominal trauma
Volume expanders + blood are given if patients are hypotensive
NG tubes + low suction will decompress stomach + prevent aspiration
Frequent + ongoing assessments are done to monitor fluid status, detect deteriorations, and determine surgical needs
Do not remove impaled objects until skilled care is available
Etiology + patho: abdominal compartment syndrome
Sustained/repeated excessively high pressure (>12 mmHg) in the abdomen; aka abdominal hypertension
Anything that increases volume in the abdominal cavity increases abdominal pressure
High pressure restricts ventilation → respiratory failure
High pressures decrease cardiac output, venous return, and arterial perfusion of organs
Causes
Fluid resuscitation
Ascites
Abdominal trauma
Surgery
Bleeding
Clinical manifestations: abdominal compartment syndrome
Distended abdomen
Decreased urine output
Increased ventilator pressures
Hypotension
Nursing + interprofessional care: abdominal compartment syndrome
Often measured via bladder catheter
ID cause + intervene to improve abdominal wall compliance
Evacuate intraluminal contents
Surgical decompression
Etiology + patho: ischemic bowel
Reduced blood flow → oxygen starvation to intestines, possibly leading to tissue damage, necrosis, and perforation
Causes
Blocked arteries (atherosclerosis)
Blood clots (embolism)
Venous thrombosis
Hypotension
Clinical manifestations: ischemic bowel
Sudden + intense abdominal pain often disproportionate to physical exam findings
Vomiting
Bloody diarrhea
Confusion (severe)
Nursing + interprofessional care: ischemic bowel
Restore blood flow immediately
IV fluids
Bowel rest
Antibiotics
Surgical intervention
Remove clots
Bypass blocked vessels
Remove necrotic tissue
Etiology + patho: acute liver failure
Characterized by a rapid onset of severe liver dysfunction in one with no history of liver disease
Often accompanied by hepatic encephalopathy
Causes
Meds (most common)
Acetaminophen
Isoniazid
Sulfa-containing drugs
Anticonvulsants
Herbal + diet supplements
Autoimmune hepatitis
Viral hepatitis, especially HBV
Clinical manifestations: acute liver failure
Jaundice
Coagulation problems
Encephalopathy
Fatigue
Nausea
Appetite loss
Right sided abdominal pain
Confusion
Coma
Complications: acute liver failure
Cerebral edema
Renal failure
Hypoglycemia
Metabolic acidosis
Sepsis
Multiorgan failure
Diagnostic studies: acute liver failure
Lab tests
High bilirubin
Prolonged PT time
High liver enzymes
Blood chemistry, especially glucose
CBC
Acetaminophen level
Toxin screens
Viral hepatitis virology, especially HAV + HBV
Ceruloplasmin + alpha-1 antitrypsin levels
Iron
Ammonia
Autoantibodies
CT/MRI, to give info on liver size + contour, tumor/ascites presence, and patency of blood vessels
Nursing + interprofessional care: acute liver failure
Planning for transfer to a transplant center should start for patients with grade 1-2 encephalopathy because patients can worsen rapidly
Early transfer is important because the risks involved with transport can increase or prevent transfer if stage 3-4 encephalopathy develops
Protect renal function by maintaining adequate fluid balance, avoiding nephrotoxic drugs, and promptly IDing + treating infection
Monitor + manage hemodynamic + renal function, glucose, electrolytes, and acid-base status
Conduct frequent neuro evals for signs of increased ICP
Elevate heads of bed to 30 degrees
Avoid excessive patient stimulation (straining/Valsalva maneuvers)
Assess patients regularly for baseline LOC + orientation; report changes immediately
Avoid sedative use due to their effects on mental status; they can be confused for worsening encephalopathy
Use minimal doses of benzos due to delayed metabolism by failing livers
Closely observe patients to prevent injuries + pad bedrails to avoid injury from possible seizures
Monitor I/O for renal function
Provide good skin + oral care to avoid breakdown + infection
Etiology + patho: acute pancreatitis
Most commonly caused by gallbladder disease (gallstones); is more common in women
Next commonly caused by chronic alcohol use; is more common in men
Most pathologic mechanism is autodigestion of the pancreas; the causative factors injure pancreatic cells or activate pancreatic enzymes instead of in the intestine
Can be due to reflux of bile acids into the pancreatic ducts through an open/distended sphincter of Oddi
Further classed as:
Mild pancreatitis
Severe pancreatitis
About half of patients have permanent decreases in pancreatic endocrine and exocrine function
Clinical manifestations: acute pancreatitis
Abdominal pain is the main manifestation
Is caused by pancreatic distention, peritoneal irritation, and biliary tract obstruction
Is usually in the LUQ but may be epigastric
Often radiates to the back due to the retroperitoneal location of the pancreas
Has sudden onset and described as severe, deep, piercing, and continuous/steady
Worsened by eating but not relieved by vomiting; may be accompanied by flushing, cyanosis, and dyspnea
Often starts when patient is recumbent
N/V
Low-grade fever
Leukocytosis
Hypotension
Tachycardia
Jaundice
Abdominal tenderness + guarding
Decreased/absent bowel sounds
Paralytic ileus → abdominal distention
Crackles
Grey Turner sign
Cullen sign
Shock
Complications: acute pancreatitis
Severity of acute pancreatitis depends on the extent of pancreatic destruction
Pseudocyst
Accumulation of fluid, pancreatic enzymes, tissue debris, and inflammatory exudates surrounded by a wall next to the pancreas
Manifestations
Abdominal pain
Palpable epigastric mass
N/V
Anorexia
Spotted by CT, MRI, and endoscopic ultrasound
Treatment options
Surgical drainage
Percutaneous catheter placement + drainage
Endoscopic drainage
Abscess
Infected pseudocyst; results from extensive necrosis in the pancreas
Manifestations
Upper abdominal pain
Abdominal mass
High fever
Leukocytosis
Autodigestion
Main systemic complications are cardiovascular and pulmonary
Pulmonary complications are due to the passage of exudate-containing pancreatic enzymes from the peritoneal cavity through transdiaphragmatic lymph channels
Enzyme-induced inflammation of the diaphragm occurs, with the result being atelectasis caused by reduced diaphragm movement
Trypsin can activate prothrombin and plasminogen, increasing patient risk for intravascular thrombi, pulmonary emboli, and disseminated intravascular coagulation
Hypotension can occur from fluid shifts sepsis
Interprofessional care: acute pancreatitis
Conservative therapy
Treatment focused on supportive care
Includes:
Aggressive hydration
Pain management
Management of metabolic complications
Minimizing pancreatic stimulation
Atropine and other anticholinergics are avoided when paralytic ileus is present because they can slow GI motility and make the problem worse
Patients with severe pancreatitis have glucose levels monitored for hyperglycemia
Blood volume replacements are given if shock is present
Central venous pressure readings can help determine fluid replacement requirements
It’s important to reduce/suppress pancreatic enzymes to decrease pancreatic stimulations and let it rest
Methods:
NPO status
NG suctioning to reduce vomiting and gastric distention and to prevent gastric acidic contents from entering the duodenum
Monitor patients at risk of acute necrotizing pancreatitis closely to start antibiotic therapy if necrosis and infection occur
Surgical therapy
May be done when the diagnosis is uncertain or if the patient fails to response to conservative therapy
Nutrition therapy
Initially, patients with acute pancreatitis are made NPO to reduce pancreatic secretion
Depending on severity, enteral nutrition is started
Parenteral nutrition is reserved for those who can’t tolerate enteral nutrition due to infection risk
As pancreatitis resolves, oral intake resumes
When food is allowed, start with small, frequent feedings
High carb diets are used because they’re the least stimulating to the exocrine pancreas
Suspect intolerance to oral foods when:
Patient reports pain
Abdominal girth increases
Serum amylase and lipase levels increase
Nursing care: acute pancreatitis
Health promo
Major factors:
Assessing the patient for risk factors
Encouraging early treatment of these factors to prevent acute pancreatitis
Encourage cessation of alcohol intake, especially if they have history of pancreatitis
Acute care
Monitor vitals; hypotension, fever, and tachypnea can compromise hemodynamic stability
Monitor response to IV fluid
Closely assess fluid/electrolyte balance
Assess respiratory function
Due to hypocalcemia risk, assess for signs of tetany (jerking, irritability, muscular twitching, numbness/tingling around lips and fingers)
Assess for positive Chvostek/Trousseau sign
Monitor magnesium levels; hypomagnesemia can develop
Assess + document duration of pain relief
Comfortable positioning, frequent position changes, and relieving N/V help reduce restlessness accompanying pain
Oral/nasal care for NPO or NG intubated patients relieve dryness of the mouth and nose
Observe for fever pr other signs of infection in patients with pancreatitis
Respiratory tract infections are common and cause patients to take shallow, guarded abdominal breaths
Prevention methods:
Turning
Coughing
Deep breathing
Semi-Fowler’s positioning
Observe for signs of paralytic ileus, renal failure, and mental changes
Ambulatory care
PT may be needed due to loss of physical and muscle strength
Continued care to prevent infection and detect complications is important
Counseling about alcohol abstinence is important to prevent patients from future attack and developing chronic pancreatitis
Patients should avoid smoking, as nicotine stimulates the pancreas
Teach patient + caregiver on treatment plans, including the importance of taking the required meds and following the recommended diet
Diet teaching should include fat restriction; fat stimulates the pancreas
Encourage carbs as they are less stimulating to the pancreas
Teach patient + caregiver to recognize and report symptoms of infection, diabetes, or steatorrhea (foul smelling, fatty stools)
Etiology + patho: chronic pancreatitis
Continuous, prolonged, inflammatory, and fibrosing process of the pancreas
Pancreas is progressively destroyed + replaced by fibrotic tissue
Most common cause of nonobstructive pancreatitis (most common type of chronic pancreatitis) is chronic alcohol use
Most common cause of obstructive pancreatitis is inflammation of the sphincter of Oddi form gallstones
Cancers of the ampulla of Vater, duodenum, or pancreas are also causative