[2Y2T2S] [PT10111] [3.1] Traumatic Brain Injury
1/145
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
146 Terms
Major cause of disability and death that is the leading cause of death in <25 y/o
Traumatic Brain Injury (TBI)
What are the two (2) major causes of traumatic brain injury (TBI)?
MVA (motor vehicle accident)
Falls in elderly
Up to how many percent of cases can violence cause closed head injury?
7-10%
Traumatic brain injury can occur in all ages but peaks among?
Young adults
Violent shaking or jarring of the brain and resultant transient functional impairment
Concussion
Defined by transient appearance of neurologic signs and symptoms following either:
Direct or indirect rapid movement in the brain —> extreme rotational/translational brain acceleration
Deceleration injury
Sudden change in the momentum of the head
Mild TBI
What are the two (2) core features of concussion?
Immediately after trauma
Largely reversible
CONCUSSION
True or False: Loss of consciousness at impact is required for diagnosis
False: Loss of consciousness at impact is not required for diagnosis
CONCUSSION
True or False: There is no evidence of structural brain injury (using conventional neuroimaging) in concussion.
True
However, there is physiological injury to the brain
What is the most commonly used procedure to check for structural brain injury in concussion?
Non-Contrast CT Scan (NCCT)
What is the mechanism of injury in concussion? (2)
Mechanisms of Injury — Concussion
Linear acceleration
Rotational acceleration
Both intracranial brain deformation forces can cause a stretch that damages the brain.
What causes the transient functional disruption of the ARAS in a concussion?
Rotational forces to the upper brainstem
What is the initial clinical manifestation of a concussion?
Brief period of disorientation, staggering or amnesia
Patient will also appear normal
What are the clinical manifestations of a concussion later on after having its initial presentation? (5)
Immediate loss of consciousness
Suppression of supporting reflexes
Transient respiratory arrest
Brief bradycardia
Fall in BP following a momentary rise
CONCUSSION — CLINICAL MANIFESTATIONS
What are other possible clinical manifestations of amnesia (aside from initial response and its progression later on)? (3)
Concussive convulsions
Retrograde amnesia
Anterograde amnesia
CONCUSSION — CLINICAL MANIFESTATIONS
May occur immediately after LOC and confer an increased risk of later seizures
Concussive convulsions
CONCUSSION — ATHLETES
True or False: Athletes who have had a concussion are more likely to have another concussion in the same playing season than others.
True
CONCUSSION — ATHLETES
What happens to athletes after a concussion?
Decline in reaction time and other neuropsychologic tests
CONCUSSION — ATHLETES
After a concussion, how long will an athlete take to recover their reaction time and other neuropsychologic tests back to baseline?
Several days or weeks
CONCUSSION — ATHLETES
The number of recollected concussions is ____________ to the degree of impairment on neuropsychological tests.
The number of recollected concussions is proportional to the degree of impairment on neuropsychological tests.
CONCUSSION — ATHLETES
Because of concussion among athletes, there is an increased risk of: (2)
Increased risk of:
Dementia
Other neurodegenerative disorders
CONCUSSION — DIAGNOSIS AND TREATMENT
Based on clinical suspicion
Neurological symptoms without significant _____ __________ ________
Based on clinical suspicion
Neurological symptoms without significant focal neurologic findings
CONCUSSION — DIAGNOSIS AND TREATMENT
True or False: There is no rigorously studies or FDA approved medical or physical therapies that are clearly proven to hasten recovery.
True
CONCUSSION — OUTCOME
How many persons with single uncomplicated concussions can fully recover within two weeks?
80-90%
CONCUSSION — OUTCOME
What concussion has a more prolonged recovery with decreasing threshold to injury?
Recurrent concussions
CONCUSSION — OUTCOME
Concussions can likely express as: (3)
Migraine headaches
Mood disorders
BPPV
CONCUSSION — OUTCOME
What concussion has increased risk of developing major neuropsychiatric disorders associated with aging?
Examples:
Depression
Dementia
PD
ALS
Erratic psychosocial behavior
Recurrent concussions
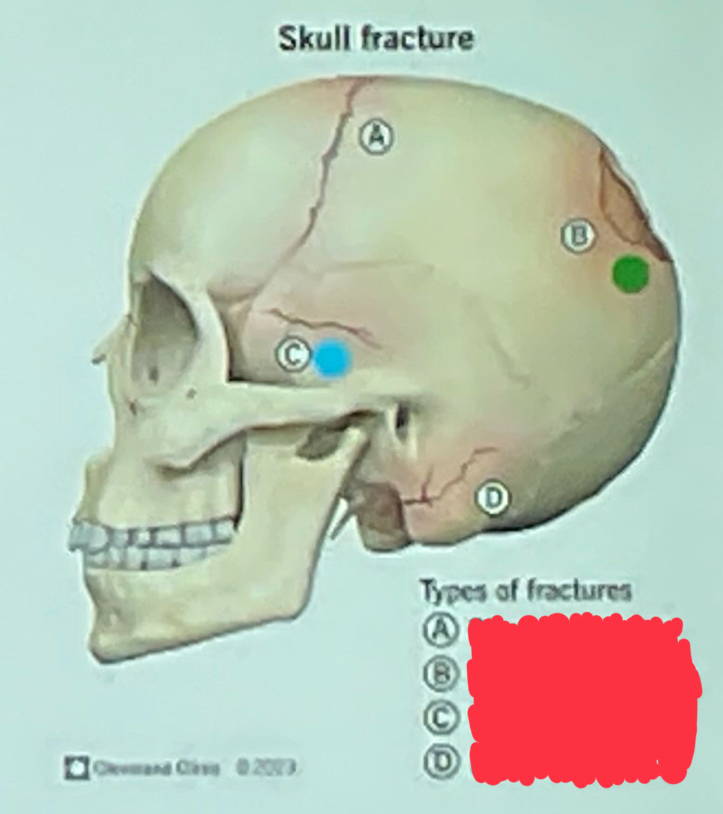
What type of skull fracture is letter C?
Linear Fracture
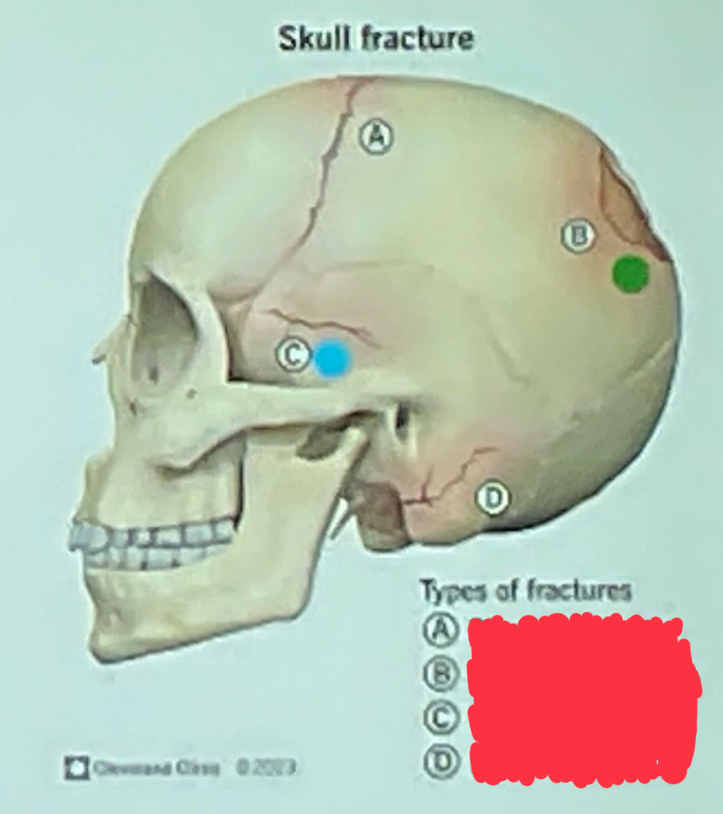
What type of skull fracture is letter B?
Depressed fracture
Where is linear fracture most commonly occurring?
Temporoparietal region
One or more bony fragments are displaced inward —> compressing the underlying brain
Depressed fracture
How many percent of depressed fractures are open and prone to infection and CSF leakage?
85%
Skull fracture that shows multiple, shattered bony fragments
Comminuted
Skull fracture presenting a lacerated scalp over the fracture
Open or compound
What types of skull fractures require surgical management? (2)
For:
Debridement
Elevation of bone fragments
Repair of dural lacerations
Depressed fracture
Comminuted fracture
What skull fracture may be missed by a skull x-ray?
Basal skull fractures
Basal skull fracture is best identified by what imaging procedure?
NCCT bone window
What are the possible symptoms if there is a fracture along the petrous portion of the temporal bone?
Hemotympanum or tympanic perforation
Hearing loss
CSF otorrhea
PFP
Battle sign
What are the possible symptoms if there is a fracture along the sphenoid, frontal, or ethmoid bones?
Anosmia
Bilateral periorbital ecchymosis
CSF rhinorrhea
Initial axonal stretch causes temporary ondulation and cytoskeletal misalignment
Associated with mechanical injury to the Na channels, causing massive Na influx
Diffuse axonal injury
DIFFUSE AXONAL INJURY
What causes massive Ca influx in Diffuse Axonal Injury?
Depolarization of the axonal openings for voltage gated Ca channels
DIFFUSE AXONAL INJURY
Along with activation of various metabolic pathways and cytoskeletal changes, what protease is also activated which degrades microtubule proteins?
Calpain
DIFFUSE AXONAL INJURY
What region/s is axon shearing injury most severe?
Regions that are anatomically predisposed to maximal stress from rotational forces
DIFFUSE AXONAL INJURY
Macroscopic tears occur in midline structures. What are these specific structures? (5)
Dorsolateral midbrain and pons
Posterior corpus callosum
Parasagittal white matter
Periventricular regions
Internal capsule
DIFFUSE AXONAL INJURY
Diffuse microscopic damage occurs as manifested by:
Axonal retraction bulbs throughout the white matter of the cerebrum
DIFFUSE AXONAL INJURY
Diffuse microscopic damage occurs as manifested by axonal retraction bulbs throughout the white matter of the cerebrum following… (3)
Microporation of membranes
Leakage of ion channels
Stearing conformational changes of proteins
DIFFUSE AXONAL INJURY
How many hours will a traumatic coma last?
> 6 hours
DIFFUSE AXONAL INJURY
What causes traumatic coma?
Multiple small lesions in the white matter tracts
DIFFUSE AXONAL INJURY
True or False: Localized micro- and macroscopic axonal shearing injury. There is also localized degeneration of white matter.
True or False: Widespread micro- and macroscopic axonal shearing injury. There is also diffuse degeneration of white matter.
DIFFUSE AXONAL INJURY
How long does it take with mild diffuse axonal injury?
6-24 hours
DIFFUSE AXONAL INJURY
How long does it take with moderate/severe diffuse axonal injury?
>24 hours
DIFFUSE AXONAL INJURY
What parts of the brain are injured with a moderate/severe diffuse axonal injury? (associated symptoms can also be included)
Brainstem injury
Hypothalamic injury
Associated Symptoms
Autonomic dysfunction
Brainstem signs and extensor posturing
Single most important cause of persistent disability after traumatic brain damage
Diffuse Axonal Injury
Mild Concussion — Loss of Consciousness (duration)
None
Mild Concussion — Decerebrate posturing (occurrence)
None
Mild Concussion — Posttraumatic amnesia (duration)
mins
Mild Concussion — Memory deficit (severity)
None
Mild Concussion — Motor deficit (severity)
none
OUTCOME AT THREE MONTHS
Mild Concussion — Good recovery outcome (%)
100%
OUTCOME AT THREE MONTHS
Mild Concussion — Death (%)
0%
Cerebral Contusion — Loss of consciousness (onset)
Immediate
Cerebral Contusion — Duration of LOC (duration)
<6 hours
Cerebral Contusion — Decerebrate posturing (occurrence)
None
Cerebral Contusion — Posttraumatic amnesia (duration)
Mins to hours
Cerebral Contusion — Memory deficit (severity)
Mild
Cerebral Contusion — Motor deficit (severity)
None
OUTCOME AT THREE MONTHS
Cerebral Contusion — Good recovery outcome (%)
95%
OUTCOME AT THREE MONTHS
Cerebral Contusion — Death (%)
0%
Mild DAI — Loss of consciousness (onset)
Immediate
Mild DAI — Duration of LOC (duration)
6-24 hours
Mild DAI — Decerebrate posturing (occurrence)
Rare
Mild DAI — Posttraumatic amnesia (duration)
Hours
Mild DAI — Memory deficit (severity)
Mild to moderate
Mild DAI — Motor deficits (severity)
None
OUTCOME AT THREE MONTHS
Mild DAI — Good recovery outcome (%)
63%
OUTCOME AT THREE MONTHS
Mild DAI — Death (%)
15%
Moderate DAI — Loss of consciousness (onset)
Immediate
Moderate DAI — Duration of LOC (duration)
>24 hours
Moderate DAI — Decerebrate posturing (occurrence)
Occasionally
Moderate DAI — Posttraumatic amnesia (duration)
Days
Moderate DAI — Memory deficit (severity)
Mild to moderate
Moderate DAI — Motor deficits (severity)
Mild
OUTCOME AT THREE MONTHS
Moderate DAI — Good recovery outcome (%)
38%
OUTCOME AT THREE MONTHS
Moderate DAI — Death (%)
24%
Severe DAI — Loss of consciousness (onset)
Immediate
Severe DAI — Duration of LOC (duration)
Days to weeks
Severe DAI — Decerebrate posturing (occurrence)
Present
Severe DAI — Posttraumatic amnesia (duration)
Weeks
Severe DAI — Memory deficit (severity)
Severe
Severe DAI — Motor deficits (severity)
Severe
OUTCOME AT THREE MONTHS
Severe DAI — Good recovery outcome (%)
15%
OUTCOME AT THREE MONTHS
Severe DAI — Death (%)
51%
CEREBRAL SWELLING
True or False: It can manifest as diffuse or focal.
True
CEREBRAL SWELLING
What are the four (4) mechanisms of cerebral swelling?
Mass
Cerebral edema
Increased cerebral blood volume d/t abnormal vasodilation
Delayed inflammatory response or dysfunction of cerebral vasomotor regulatory centers in the brainstem
CEREBRAL SWELLING
What happens when there is increased cerebral blood volume d/t abnormal vasodilation?
Hyperperfusion, increased vascular permeability causing plasma leakage and vasogenic edema
CEREBRAL SWELLING
What happens when there is delayed inflammatory response or dysfunction of cerebral vasomotor regulatory in the brainstem? (3)
During the first 24 hours
Cerebral hypoperfusion
1-3 days after severe head injury
Hyperemia
4-7 days after severe head injury
Arterial vasospasm
CEREBRAL SWELLING
Does the magnitude of swelling always correlate with the severity of injury?
No.
The magnitude of swelling does not always correlate with the severity of injury
Focal parenchymal hemorrhages that result from “scraping” and “bruising” of the brain as it moves across the inner surface of the skull
Cerebral contusions
What are the most common sites of cerebral contusions? (2)
Inferior frontal lobe
Temporal lobe
Why are the inferior frontal and temporal lobes commonly subjected to cerebral contusions?
D/t irregular protuberances at skull base