Digestive system - chapter 24
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
digestion and metabolism primary role
break down food we consume and absorb the digested (broken down) fragments into the blood
The GI tract or alimentary canal is a muscular tube that is open to the environment on both ends
accessory digestive organs produce secretions that help with digestion of food (saliva, bile, enzymes)
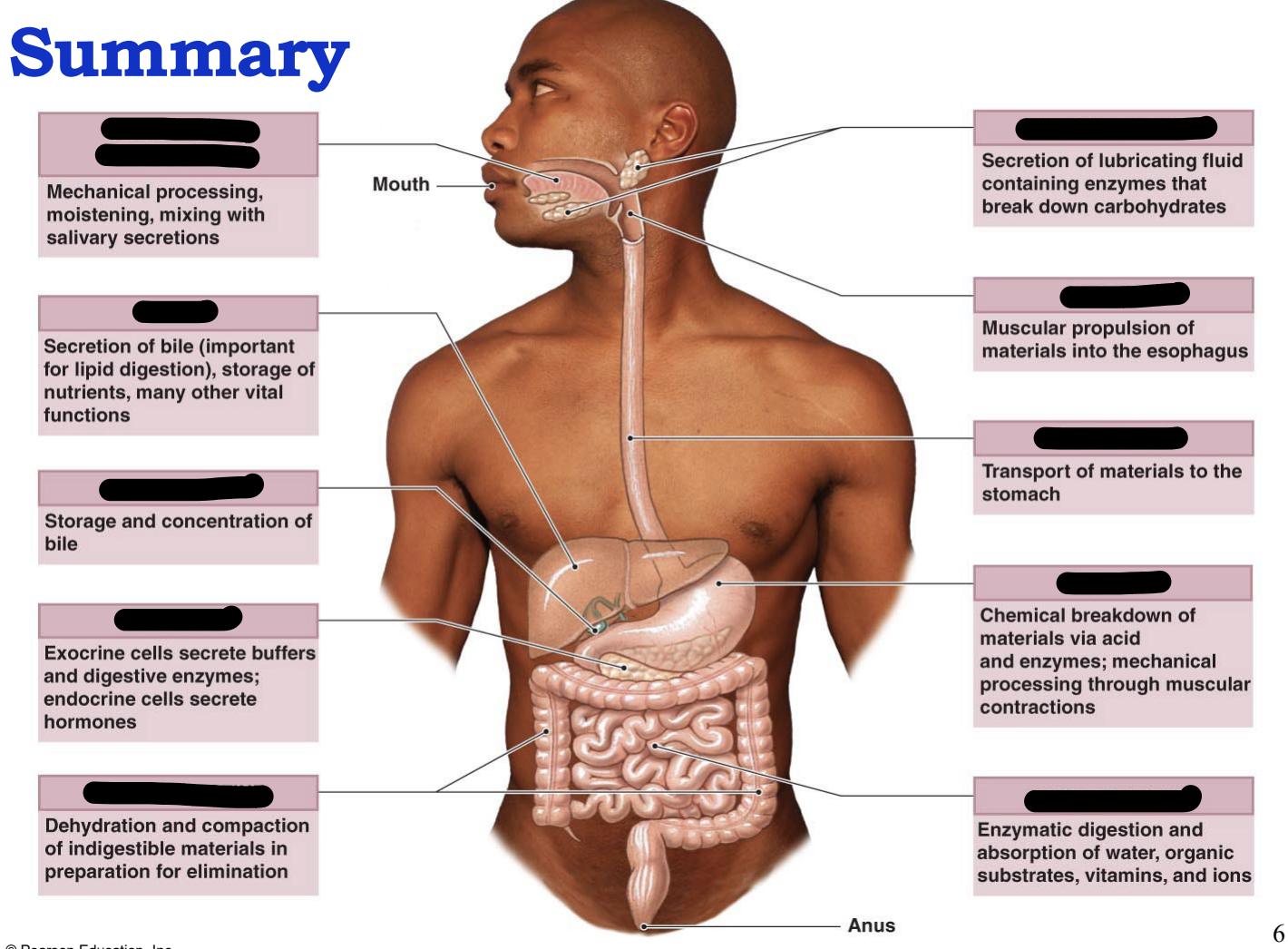
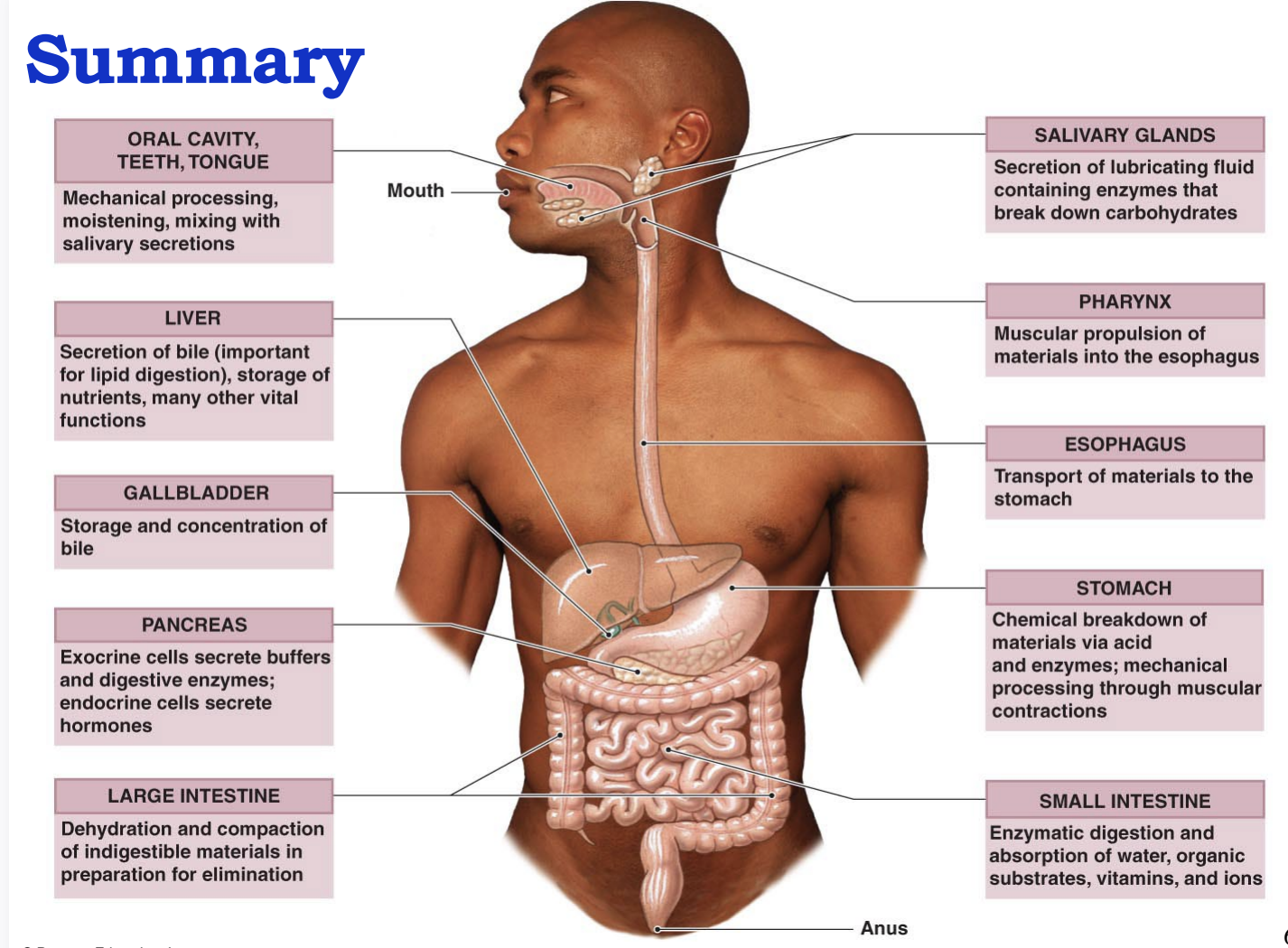
summary of digestion
Ingestion: taking food into the mouth
Propulsion: moving food along the GI tract, followed by peristalsis
Mechanical digestion: begins with checking, followed by churning in the stomach, and segmentation and emulsification by small intestine
Chemical digestion: breakdown of large molecules, into their building blocks by digestive enzymes
Absorption: digested food is transported into blood or lymph
Defecation: undigested material is eliminated from GI tract
teeth
or dentes, gomphosis joint
enamel: harder than bone = 96% CaPO4, no cells
dentin: calcified connective = 70% CaPO4, no cells
Pulp: CT containing blood & lymphatic vessels and nerves
two dentitions (sets of teeth)
20 deciduous or “baby teeth” which begin to erupt at 6 months and are lost between 6-12 years
32 permanent teeth, the last molars are the wisdom teeth
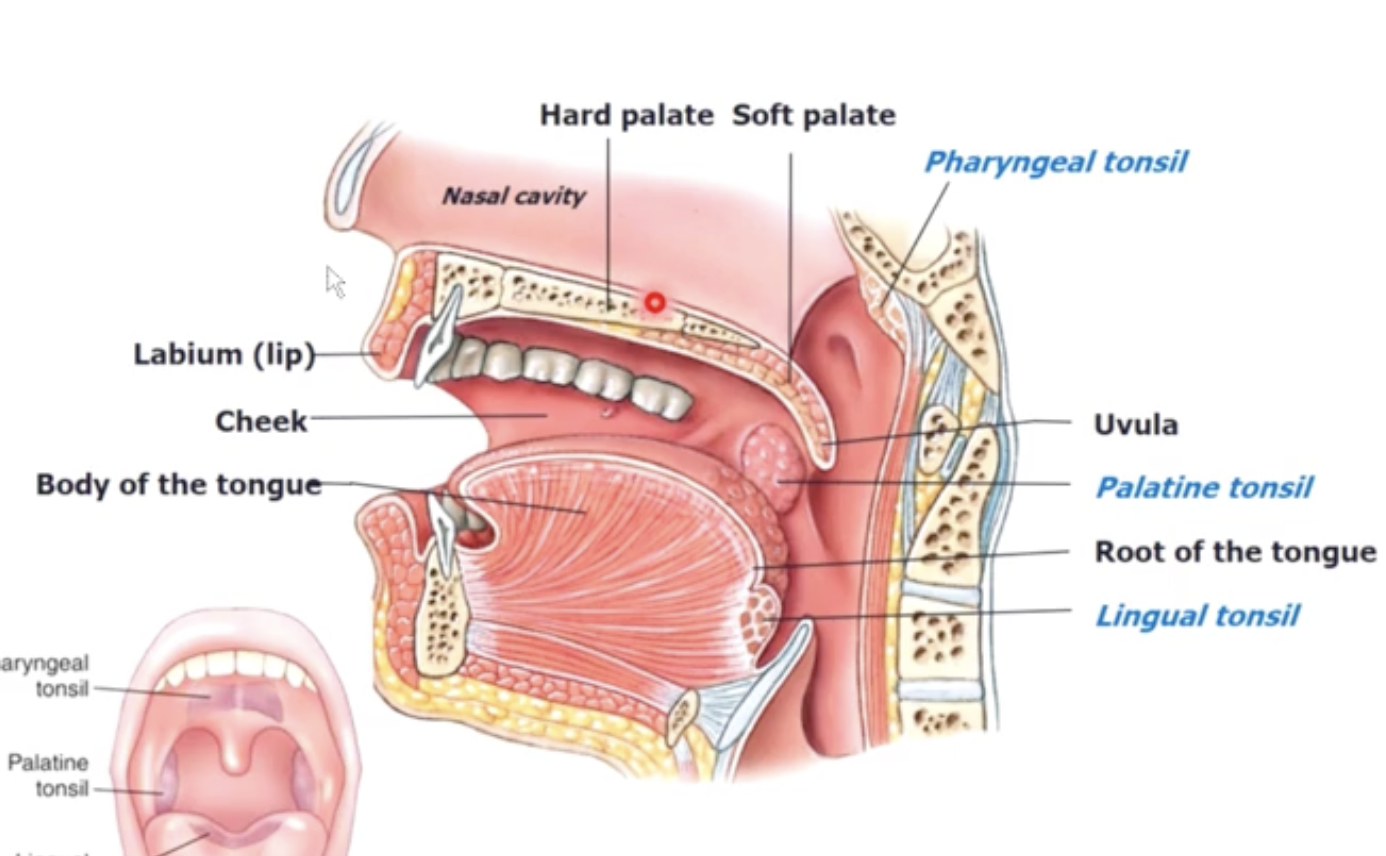
Tonsils
lymphoid containing WBC’s
Pharyngeal tonsil - behind nasal cavity
palatine tonsil - beside/behind tounge
lingual tonsil - bottom of tongue
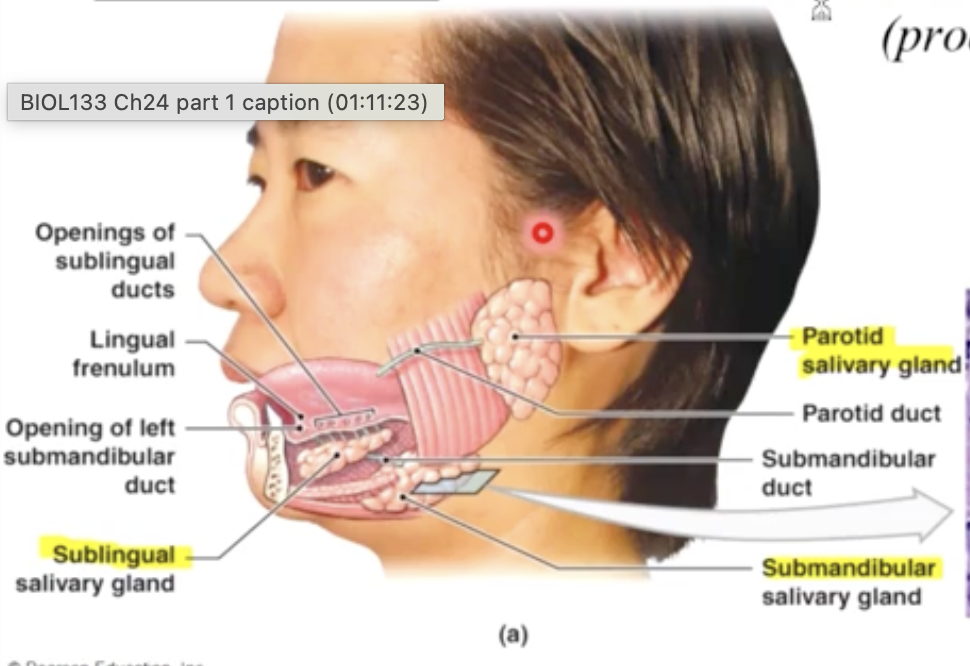
3 pairs of salivary glands
1.5L of saliva/ day (mostly water 99.4% H2O + 0.6% ions, enzymes keep pH 7)
Parotid: produces salivary amylase: enzyme that breaks down starch (produces 25% of total saliva)
sublingual: secretes buffer & lubricant (produces 5% of saliva)
submandibular: Secretes buffers, mucins, salivary amylase & IgA (produces 70% of total saliva)
saliva production - stimulated by tactile and taste receptors & ANS activity in salivary reflex centres of medulla oblongata
Functions of the tongue
mechanical processing
assist chewing & swallowing
sensors to touch, temperature & taste
4 secretes lubricating mucins, lingual lipase
(breakdown TGs @ pH 3-6)
pharynx
a common passageway for solid foods, liquids and air
regions of the pharynx
nasopharynx - back of nasal cavity
Oropharynx - back of mouth, behind tongue
laryngopharynx - right before esophagus
deglutition steps
swallowing (the contraction and relaxation of esophageal sphincter)
2400x per day
step 1 - buccal phase (food is being swallowed) voluntary
step 2 - pharyngeal phase (epiglottis is covering trachea) reflex
step 3 - esophageal phase (parastalsis pushes food down esophagus)
step 4 - bolus enters stomach
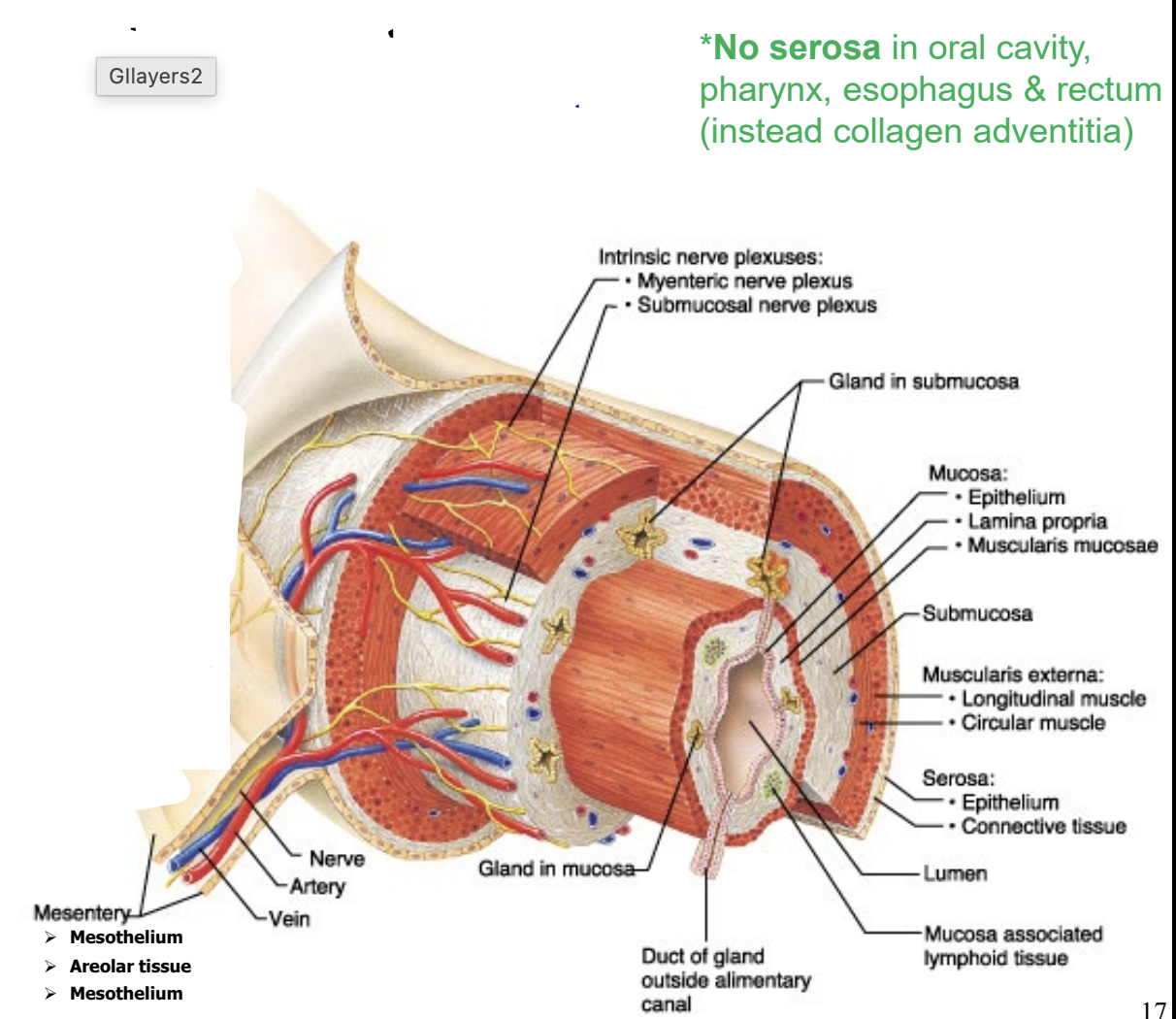
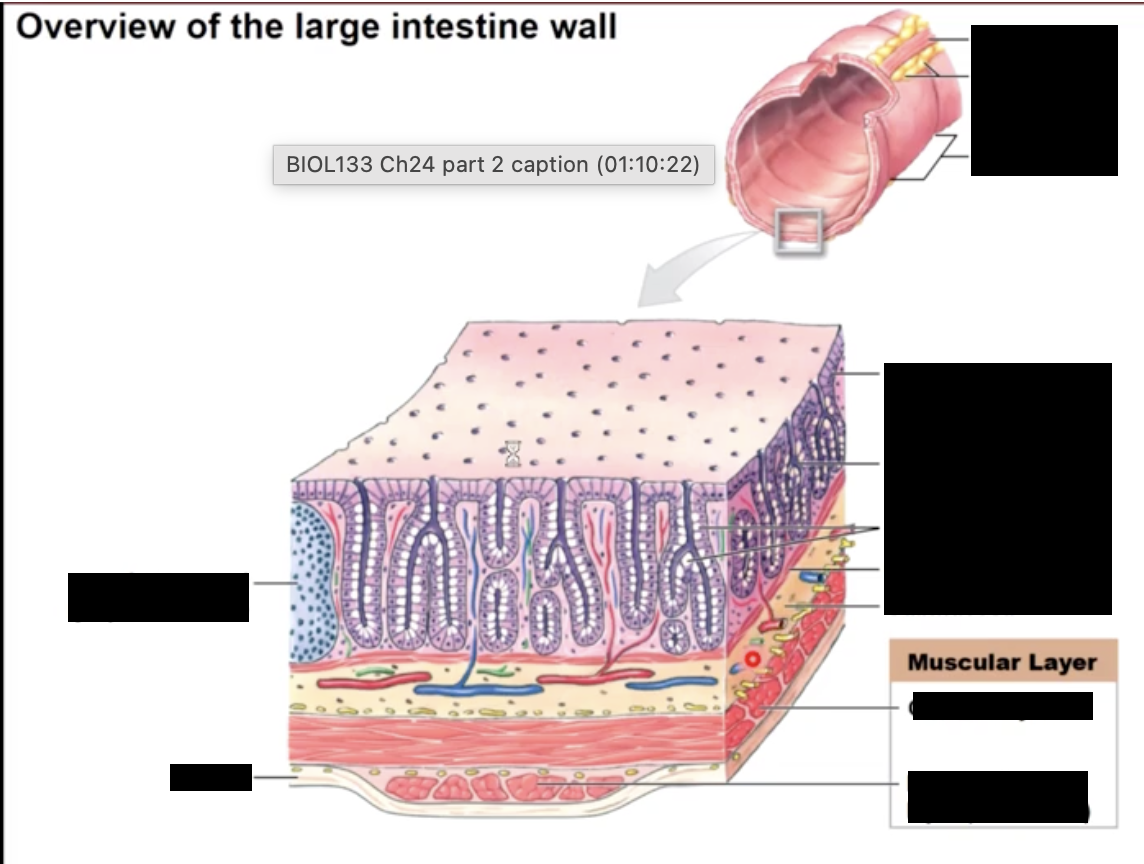
Histology of the GI tract
from the esophagus to the anus the GI tracts consists of 3 layers:
mucosa - epithelial layer which produces mucus
epithelium, laminate propria, muscularis mucosae (embedded with pacesetter cells)
Submucosa - connective tissue layer containing nerves, blood and lymph vessels
Muscularis Externa- smooth muscle layer
longitudinal muscle & circular muscle
Serosa - outer connective tissue layer which forms the visceral peritoneum
** no serosa in oral cavity, pharynx, esophagus and rectum. Has collagen adventina instead
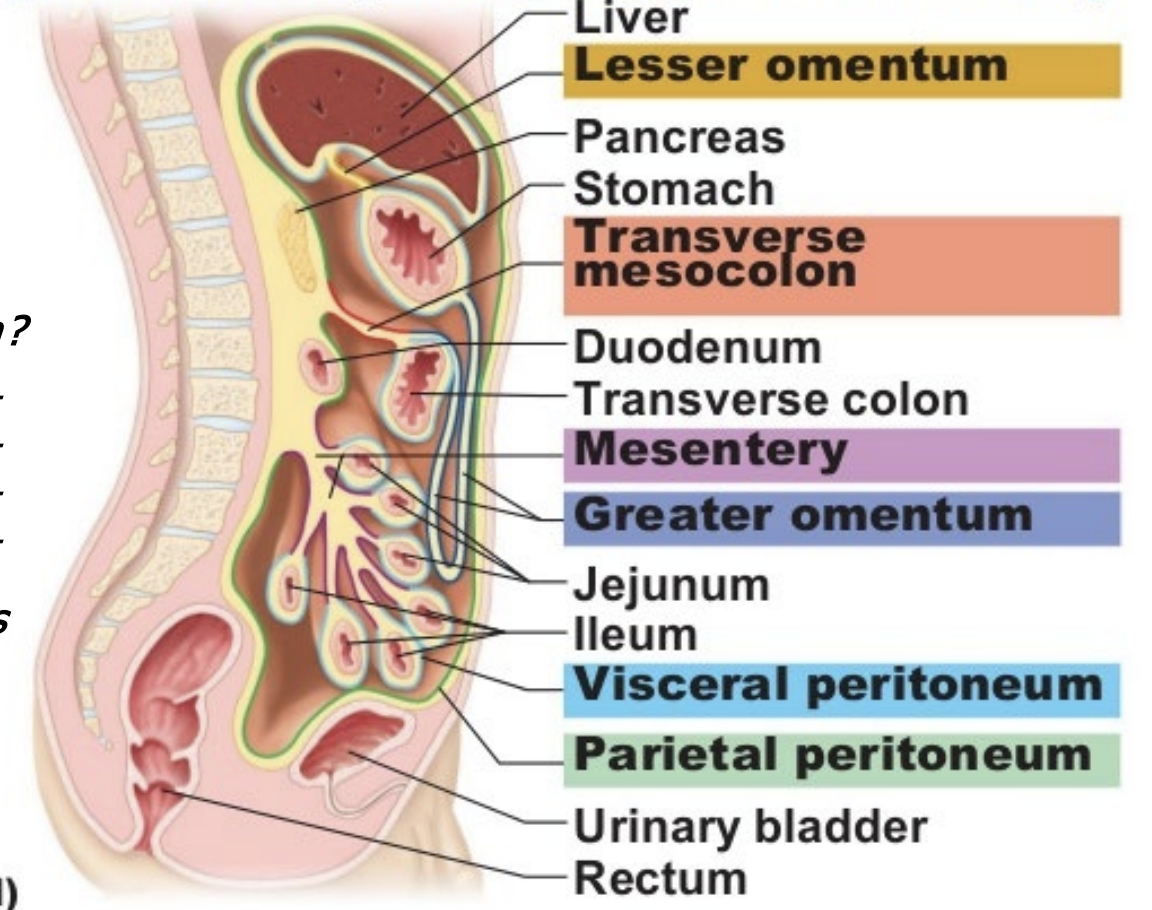
peritoneum
the body’s largest serous membrane (simple squamous epithelium + areolar CT) & it wraps around & stabilizes most abdominopelvic organs
made up of visceral and parietal peritoneum, separated by peritoneal fluid
infiltrated by blood and lymphatic vessels & nerves
insulating layers of fat
5 major peritoneal folds
greater momentum- stomach
falciform ligament - liver- anterior wall of peritoneum
lesser omentum -liver-stomach
mesentery (proper) - small intestine
mesocolon - large intestine-dorsal wall
retroperitoneal organs: pancreas, duodenum, rectum, ascending & defending colon: kidneys
peristalsis
the coordinated contraction and relaxation of smooth muscle in the muscularis external
it results in the forward movemnet of chrome through the GI tract
segmentation
the mixing of chyme by alternating contraction and relaxation of the GI smooth muscle
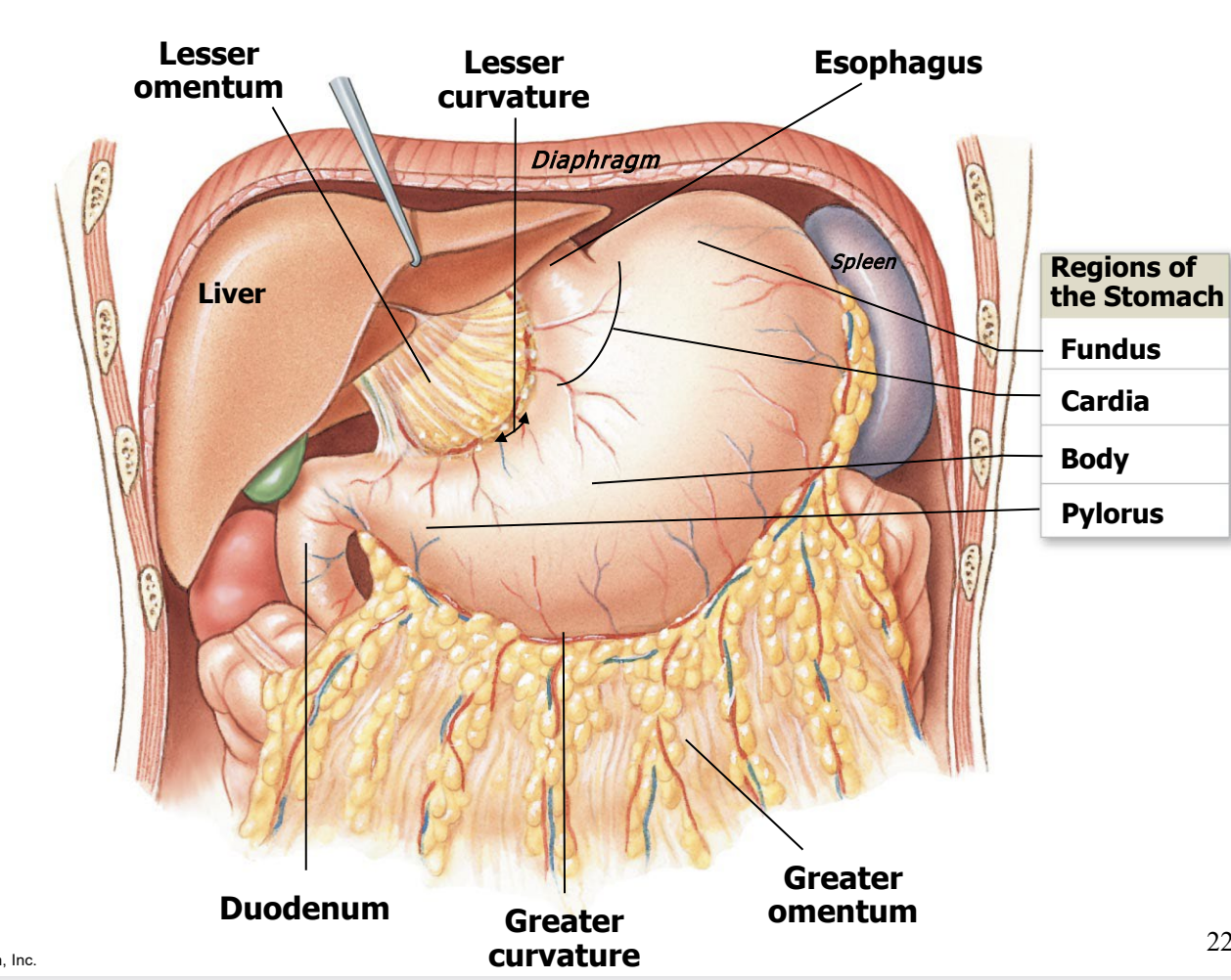
the stomach
primary functions are:
mechanically mix food
begin protein digestion by secreting gastric juice
control flow into the duodenum
food leaving the stomach is called chyme
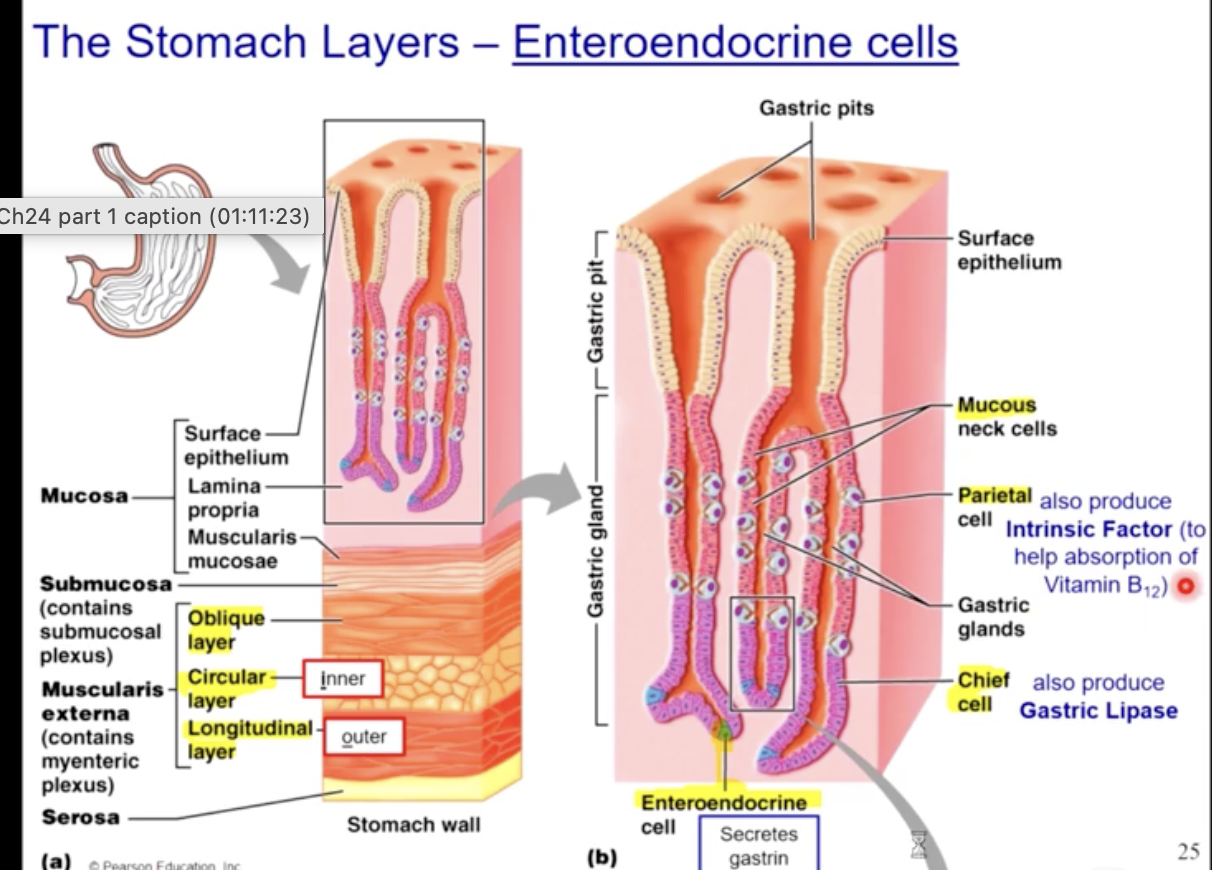
stomach histology
chief cells and parietal cells
the stomach lining contains
mucus secreting goblet cells
gastrin secreting endocrine cells
gastric pits that secret HCL and pepsinogen
when food enters the stomach, gastrin is released in to the blood
Gastrin
released into the blood when food enters the stomach
gastrin activates the gastric pits to secrete pepsinogen and HCL.
the lowered pH created by HCL converts pepsinogen to pepsin, which initiates protein catabolism (PSNS also activates gastric juice secretion)
HCL aslo: kills microbes, denatures proteins, breaks plant cell walls & connective tissue of meat
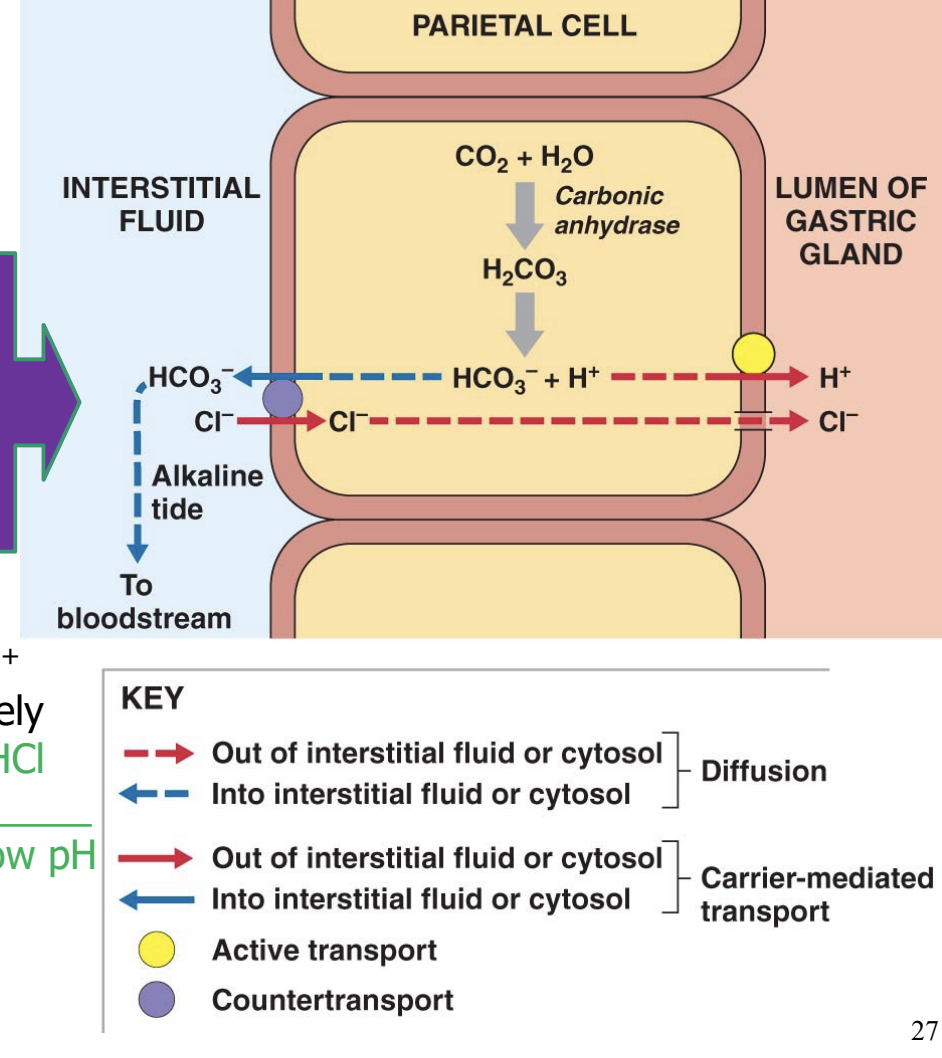
HCL secretion by parietal cells
pH 1.5-2
HCL is formed by moving H+ ion into the lumen separately from Cl- ion.
HCL does not build up in the parietal cell which would mean low pH within that cell
a counter transport mechanism ejects the bicarbonate ions into the interstitial fluid and imports chloride ions into the cell
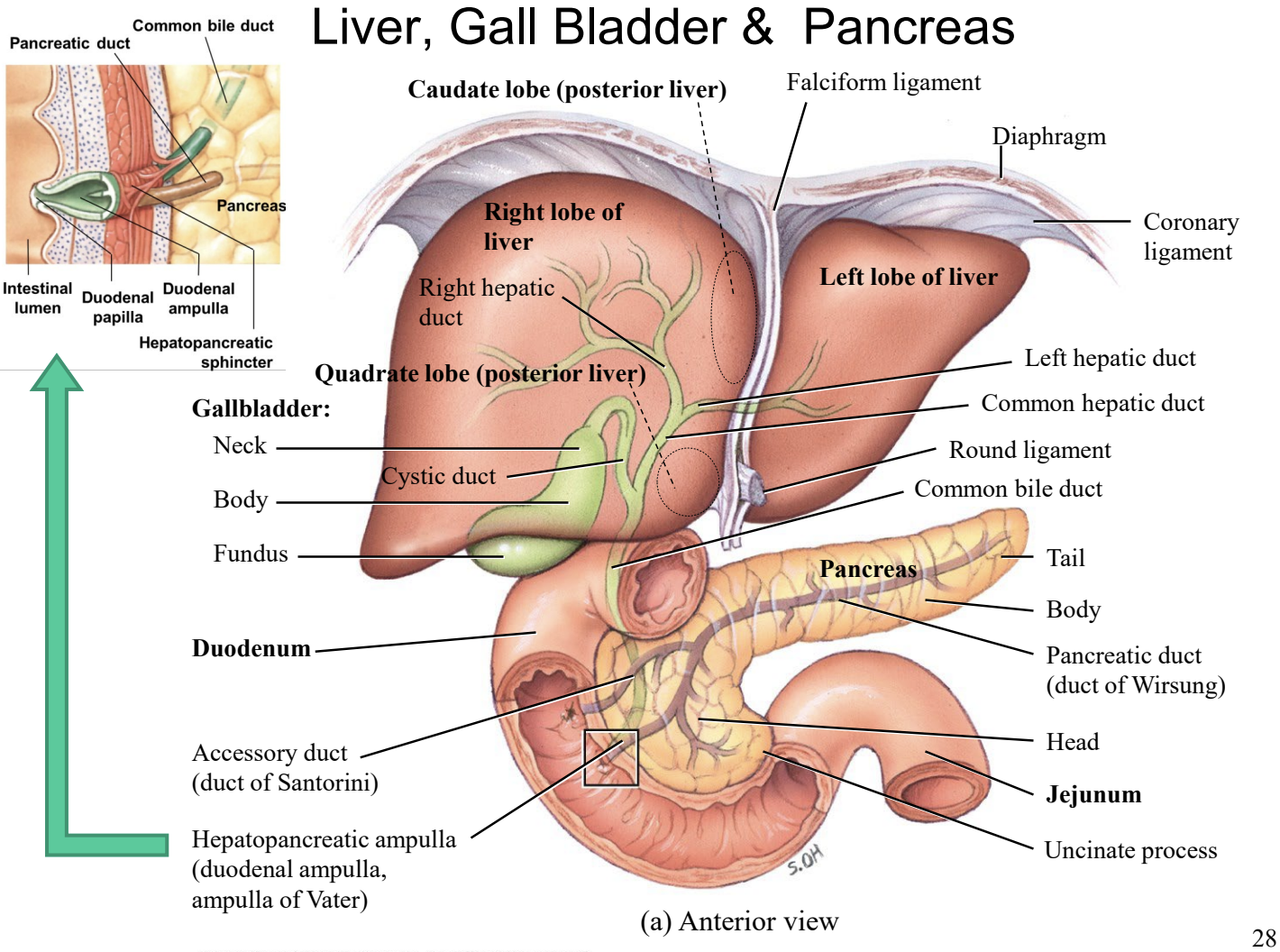
Bile
Bile : you produce 1 L/ day
bile is produced in the liver and stored in the gall bladder. When chyme enters the duodenum, the gall bladder contracts releasing bile into the duodenum through the bile duct
bile is composed of
bile salts: made from cholesterol, these salts emulsify large drops of fat into smaller droplets → micelles = small lipid bile salt complexes
bilirubin - a metabolite formed during heme degradation, this yellow pigment is converted into urobilinogen and stercobilin which gives faces it’s brown colour
cholesterol
pancreatic juice
produced by the pancreas
consists of bicarbonate (HCO3) and digestive enzyme (trypsin, chymotrypsin, carboxypeptidase, amylase, lipase, and nuclease) produced by the pancreas and released by the pancreatic duct into the duodenum
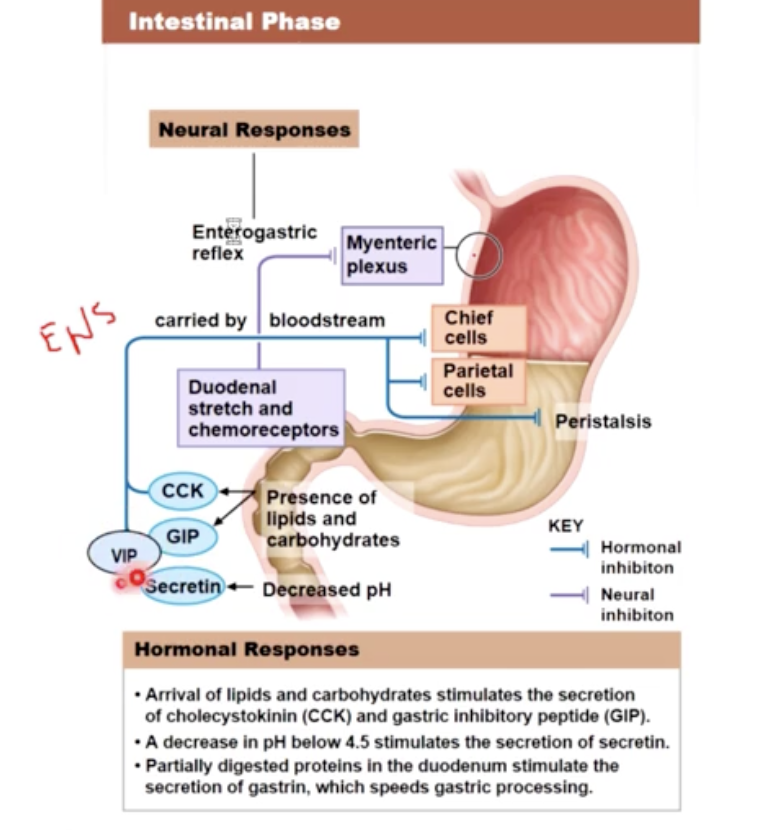
6 Hormones involved in regulation of digestive enzymes
Gastrin
Secretin
Gastric Inhibitory peptide
Cholecystokinin
vasoactive Intestinal Peptide
enterocrinin
Garstrin
secreted by G cells in pyloric antrum when stimulated by th vagus nerve or when food arrives in the stomach
and enteroendocrine cells in the duodenum release gastrin when they are exposed to large quantities of undigested proteins
gastrin increases stomach motility and stimulating gastric acid and enzyme production
stimulates gastric motility and juices
Secretin
released when chyme enters the duodenum
Secretin’s main effects is to increase the secretion of buffers by the pancreas, increasing the pH of the chyme
secretin also stimulates secretion of bile by the liver and reduces gastric motility and gastric sensory rates
secretion of buffer and bile
Gastric Inhibitory Peptide
secreted when fats and carbohydrates (especially glucose) enters the small intestine
the inhibition of gastric activity stimulates insulin release at the pancreatic islets.
GIP has secondary effects, stimulating submucosal duodenal gland activity, stimulating lipid synthesis in adipose tissue, and increasing glucose use by skeletal muscles
gastric inhibit - insulin stimulant
cholecystokinin
CCK
secreted when chyme arrives in the duodenum, especially when chyme contains lipids and partially digested proteins
the net effects of CCK are to increase the secretion of pancreatic enzymes and push pancreatic secretions and bile into the duodenum
The presence of CCK has two additional effects, it inhibits gastric activity and it appears to have CNS effects that reduce hunger
*gastric and hunger inhibit - enzyme & bile release
Vasoactive Intestinal Peptide
VIP
stimulates the secretion of intestinal glands, dilates regional cappilliares and inhibits acid production in the stomach
the dilation of capliallries in active areas of the intestinal tract, VIP provides an efficient mechanism for removing absorbed nutrients
gastric inhibit - intestinal vasodilation
Enterocrinin
released by enteroendorine cells of the duodenum in response to stimulation by the vagus nerves before chyme reaches the pyloric sphincter and also when chyme enters the duodenum
It stimulates production of alkaline mucus by the duodenal submucosal glands, which protects the intestine from acidic chyme
vagus - enterocrinin - alkiline mucus
regulation of bile production
when acid chyme enters the duodenum it stimulates the release of CCK and secretin into the blood stream
secretin - increase bile production in liver
CCK - causes contraction of the gallbladder and opens the hepatopancreatic sphincter so bile enters the duodenum
Vagal stimulation (PSNS) - further controls the gallbladder
regulation of pancreatic juice secretion
as acid chyme enters the duodenum, it stimulates the release of secretion and cholecystokinin into the blood stream
secretin - increase the production HCO3 buffer in the pancreas
CCK - increase the digestive enzyme production from the pancreas and open sphincter
vagal stimulation (PSNS) enhances pancreatic stimulation
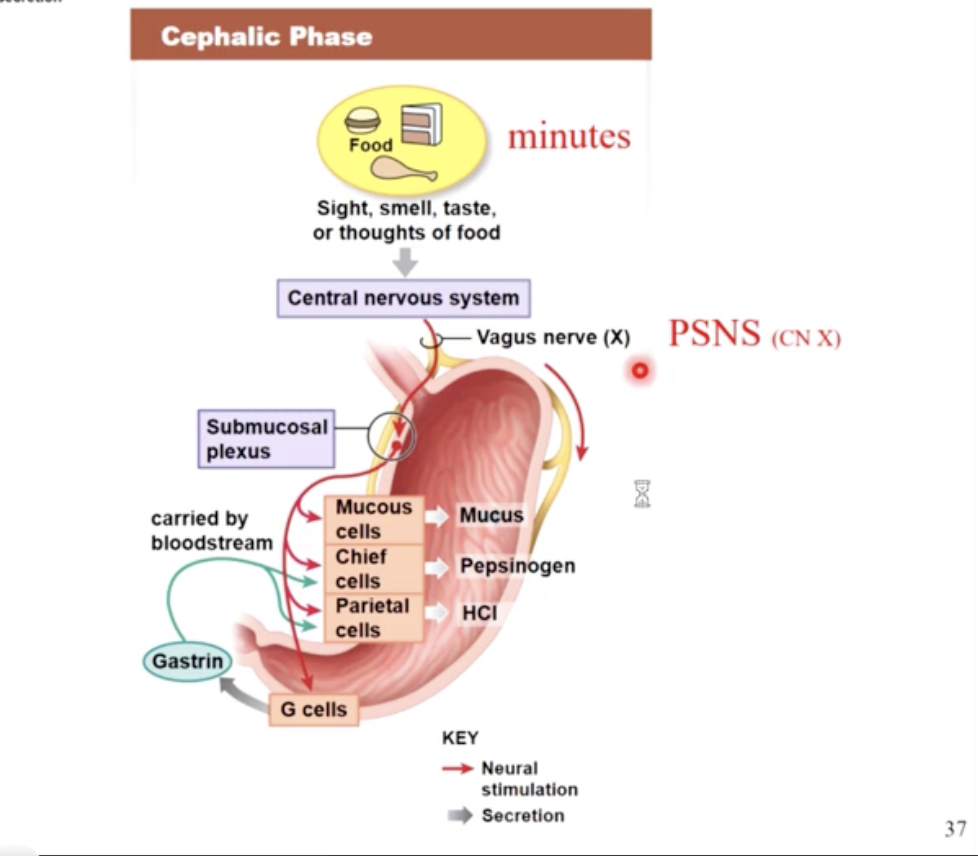
3 phases of digestive activities
digestive activities of the gastrointestinal tract occur in 3 over lapping phases:
the cephalic phase
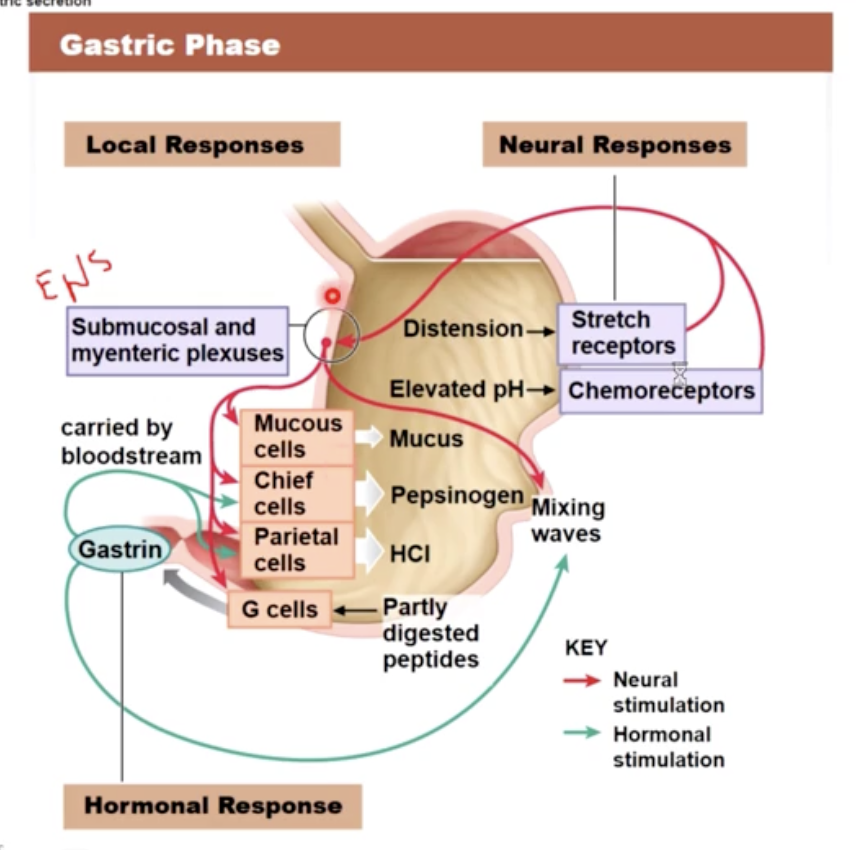
the gastric phase
the intestinal phase
insulin
allows your cells to take up glucose & amino acids from the blood stream
two gastric reflexes
gastroenteritis reflex: stimulates motility and secretion along the entire small intestine
gastroileal reflex: triggers the opening of the ileocecal valve, allowing materials to pass from the small intestine into the large
both reflexes accelerate movement along the small intestine
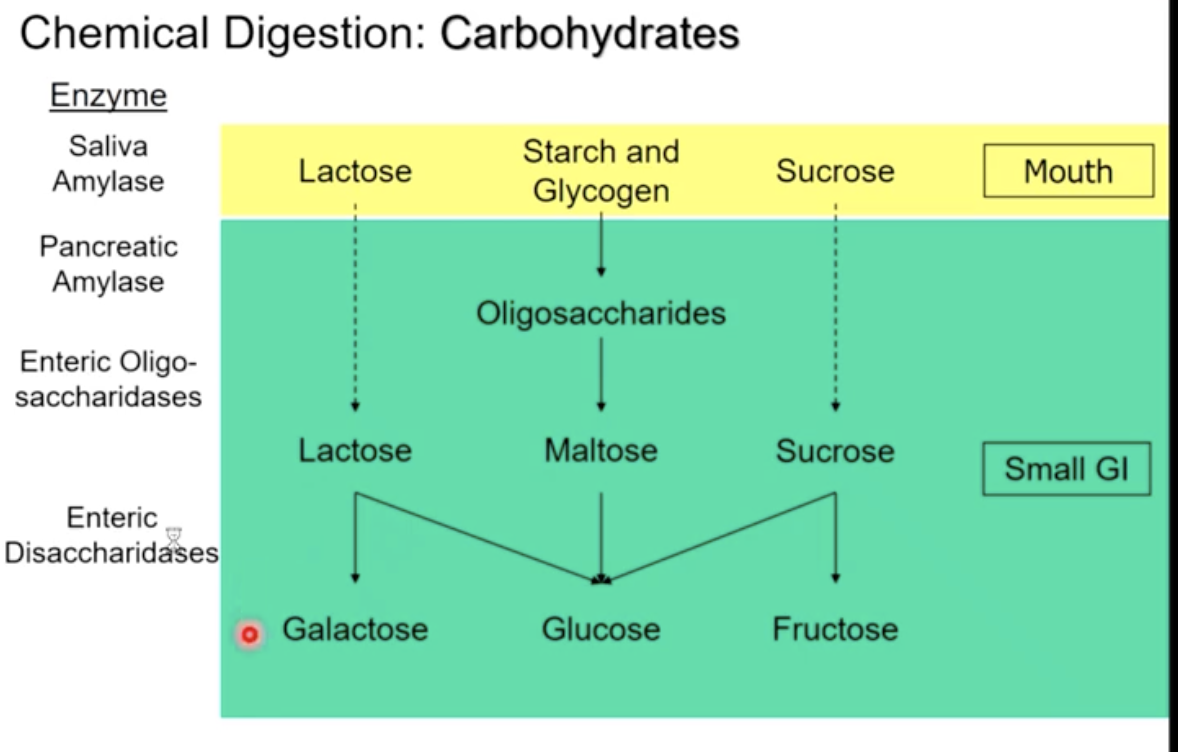
chemical digestion of carbohydrates
salivary amylase begins break down in mouth
pancreatic amylase begins breaking oligosaccharides down in duodenum
polysaccharides → smaller saccharides (oligosaccharides) → pancreatic amylase (breaks down oligosaccharides) with enteric oligosaccharides, into disaccharides (lactose, maltose, sucrose) → enteric disaccharides break disaccharides into monosaccharides (glucose fructose, galactose)
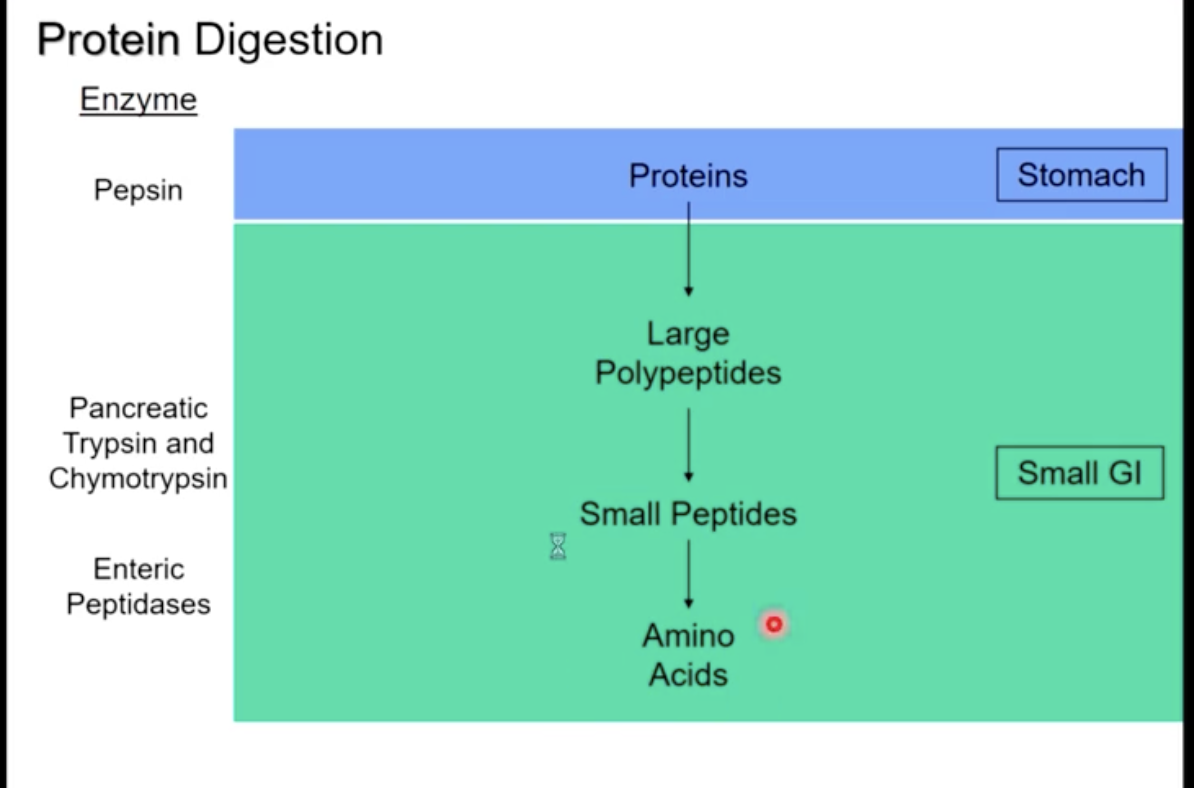
Protein Digestion
protein digestion begins in the stomach with the enzyme pepsin
the release of pancreatic trypsin and chymotrypsin in the duodenum (converting proteins into large polypeptides)
enteric peptidases break large polypeptides into small polypeptides, then amino acids
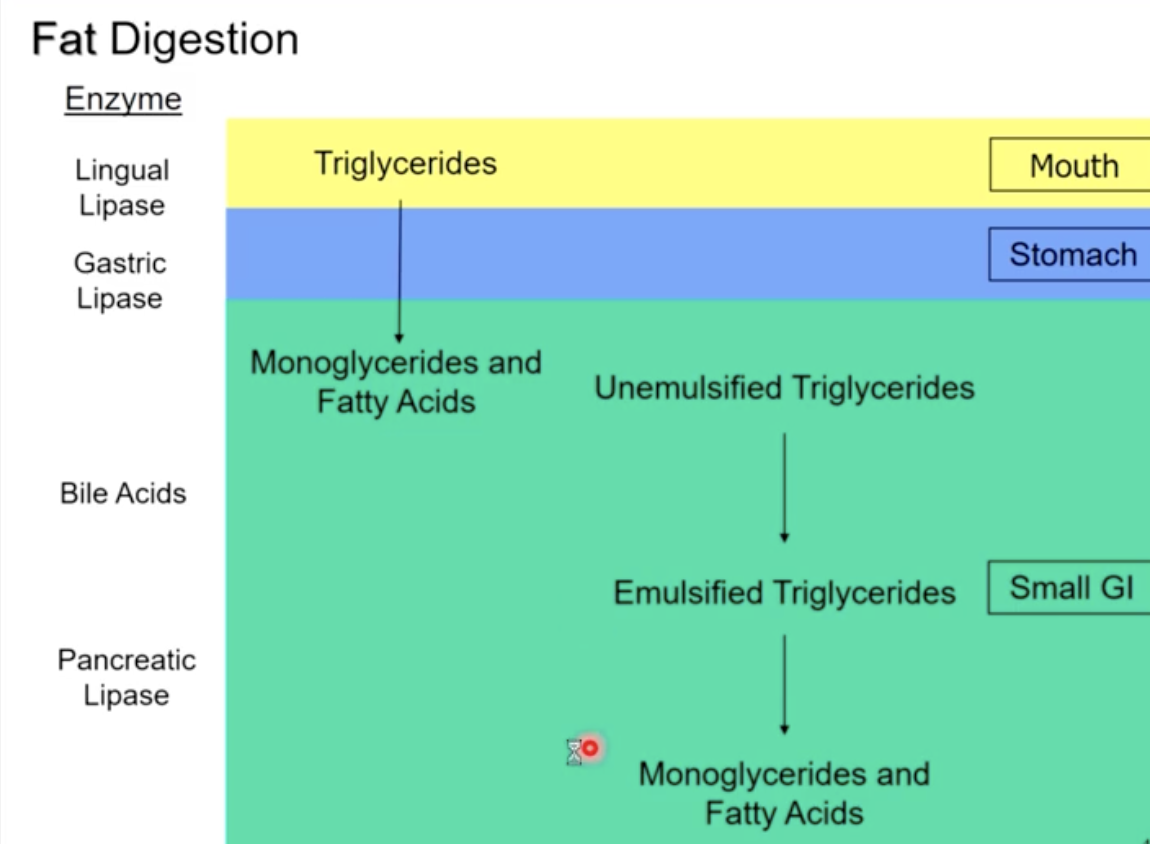
Fat digestion
lingual lipase in the mouth and gastric lipase in the stomach break triglycerides into monoglycerides and fatty acids
bile acids in the small intestine begin to emulsify the fat droplets (unemulsified)
Pancreatic Lipase can then break emulsified triglycerides into monoglycerides and fatty acids
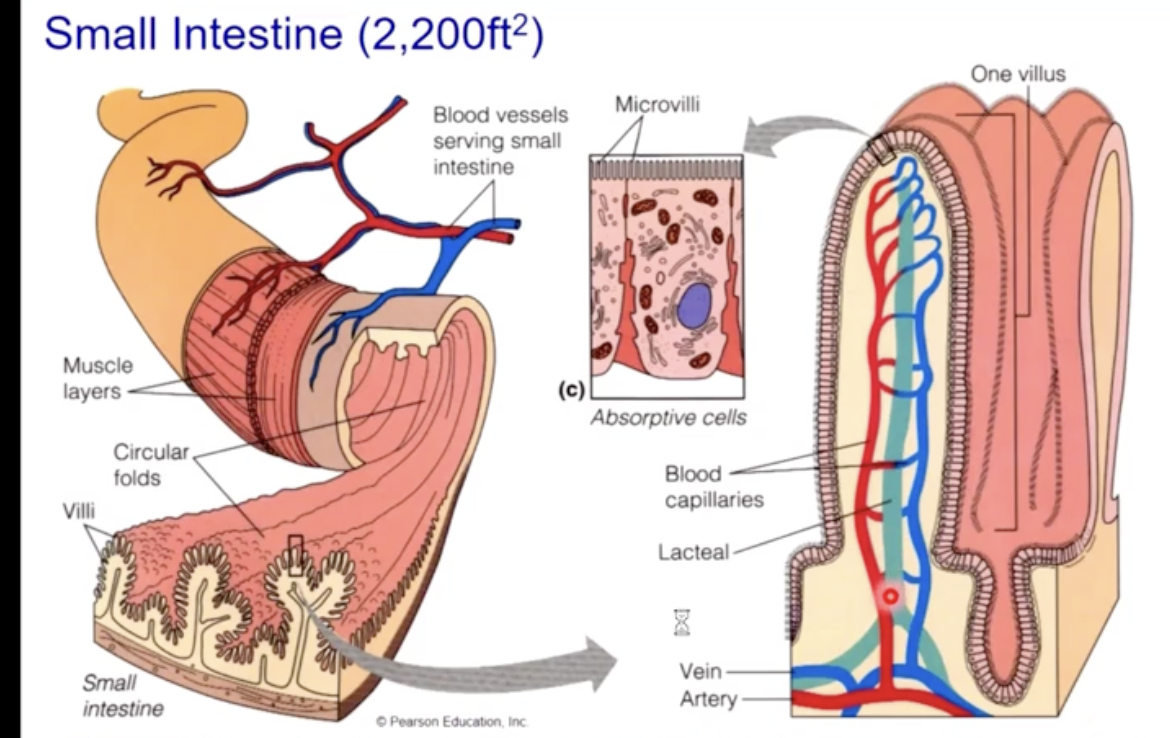
The small intestine
the small intestine has specialized features for absorption
long length (2200 ft (squared))
800 circular folds (plicae circulares)
villi - each villus has both blood and lymph supply for absorption
microvilli
characteristics of the 3 segments of the duodenum
duodenum (10" inches) - duodenal glands secrete bicarbonate rich mucus
neutralize chyme, get pH up to 7-8
Jejunum (8 feet)
extensive villi and microvilli because of the large amounts of food absorption
Ileum (11 feet)
contains aggregated lymphoid nodules (lymphocytes “hangout” and screen for pathogens)
How do the regional specializations of the small intestine change along it’s length
the duodenum has small villi & numerous mucous glands
the jejunum has numerous villi for absorption. Most chemical digestion & absorption takes place here
The ilium contains aggregated lymphoid nodules
*90% of nutrient absorption takes place in the small intestine
(10% in the large)
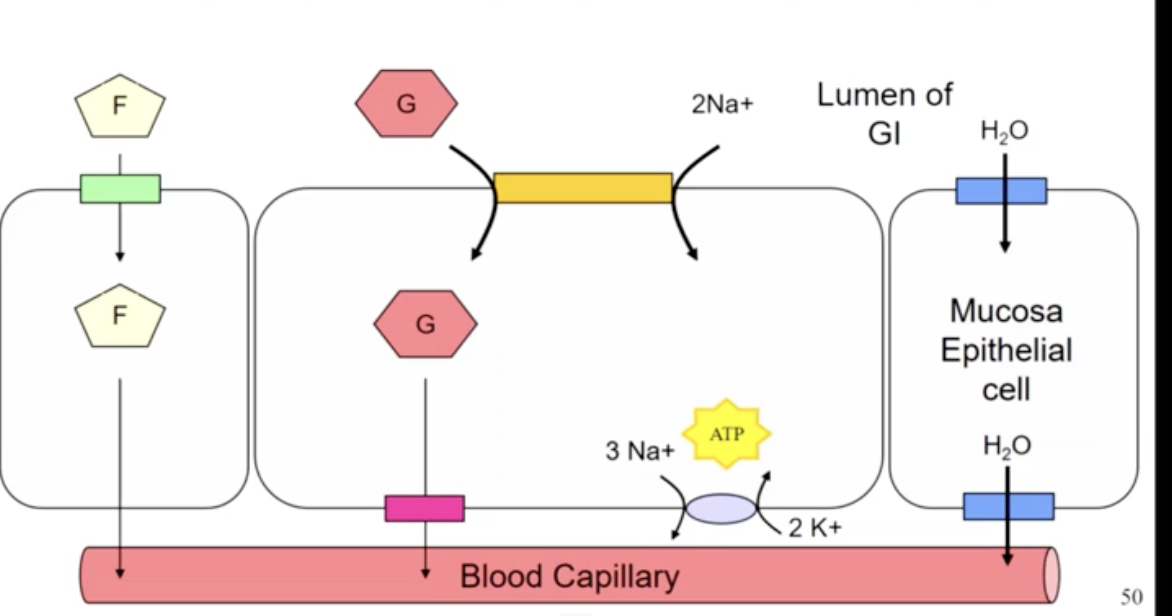
Absorption into the small intestine
most nutrients are absorbed actively into the mucosa of the GI tract eg. by a Na cotransporter (and H2O follows Na)
glucose, galactose amino acids and most water soluble vitamins are absorbed this way (sodium dependent glucose transport)
water and fructose are absorbed by facilitated diffusion
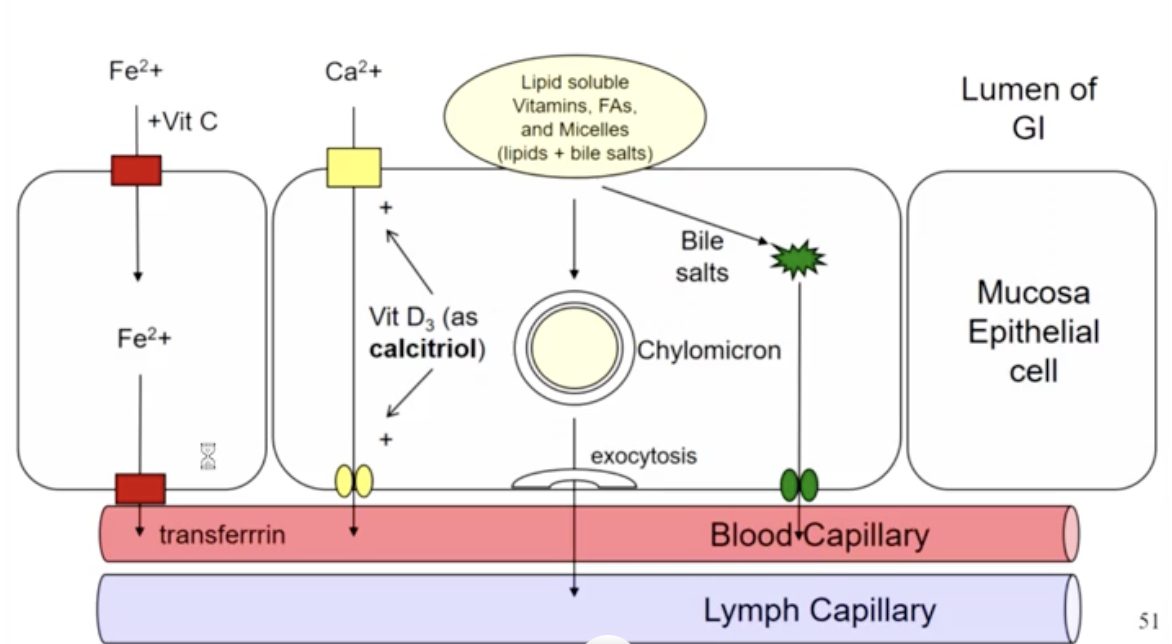
absorption of lipid soluble substances
fatty acids are absorbed by direst or facilitated diffusion & enter lymph
fat soluble vitamins A,D & E are absorbed similarly to FA
vitamin B12 is absorbed with the help of intrinsic factor, which is secreted in th gastric juice (by parietal cells). Vitamin B12 is required for erythropoiesis
lacteals
lymphatic capillaries that absorb dietary fats through the villi of the small intestine. This fluid is called chyle
lacteals merge with larger lymphatic vessels to transport the chlme to the thoracic duct
once the fat (in chylomicrons) travels to the liver, it is converted to lipoproteins (HDL or LDL) and can enter the bloodstream to be carried to tissue
the absorption state
insulin stimulates:
glucose uptake and glycogenesis
amino acid intake and protein synthesis
triglyceride synthesis
Androgens, estrogens and growth hormone also stimulate protein synthesis
Glycolysis and aerobic respiration provide the ATP needed to power cellular activities aswell as the synthesis of lipids and proteins
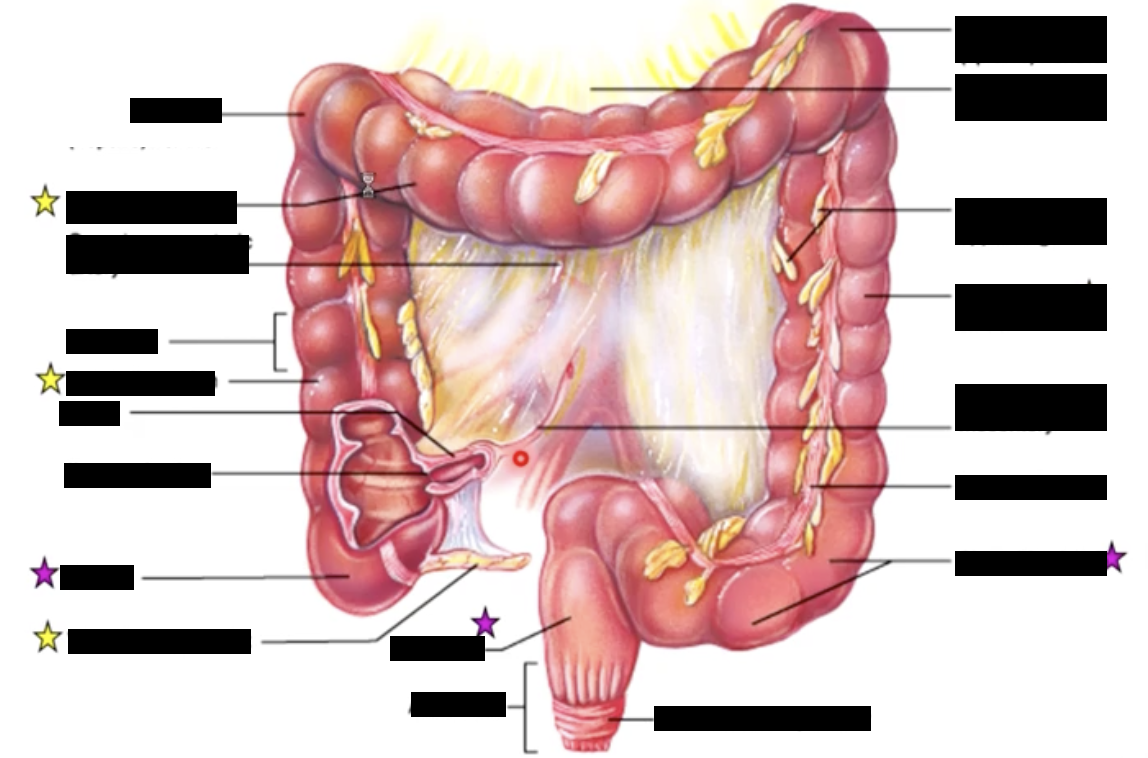
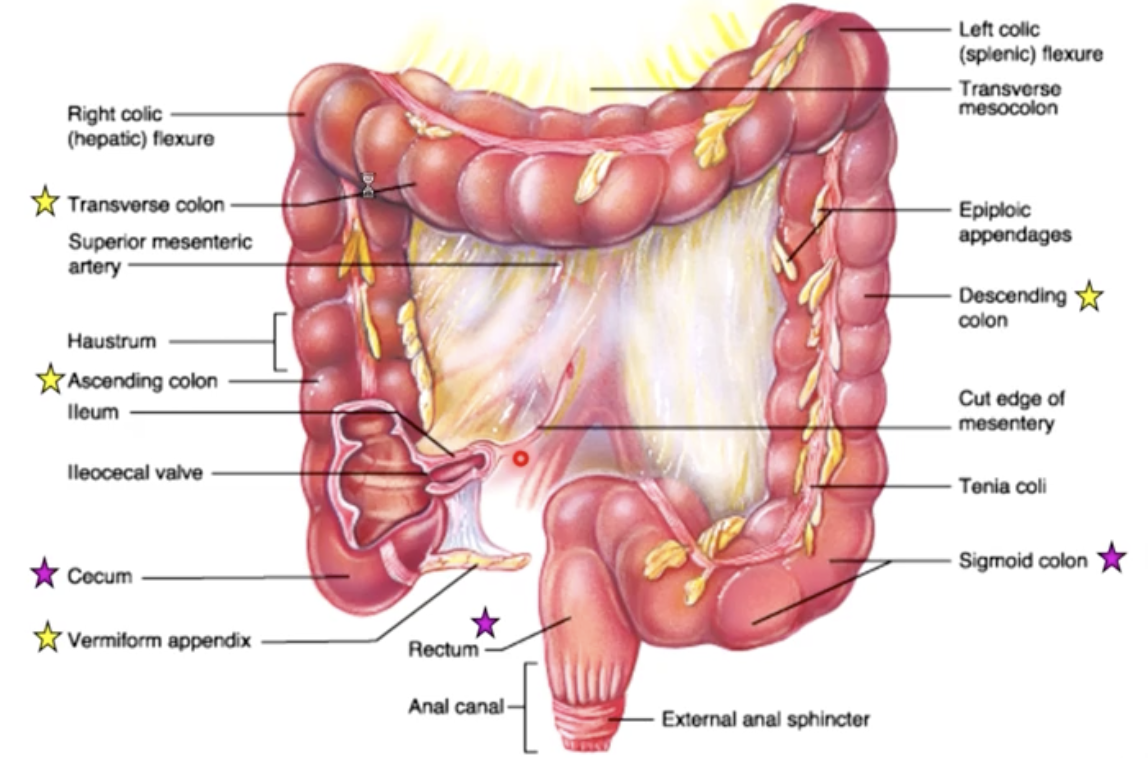
tenia coli
3 bands of longitudinal smooth muscle of the muscularis externa
Verniform appendix
vestigial organ or “bacterial safe house”
vermiform - “wormlike”
the appendix, when infected can cause death. Those who have had it are perfectly healthy afterwards
the appendix used to be seen as vestigial (no longer needed), but research has recently suggested that the appendix serves as a safe house for useful bacteria when illness flushes these bacteria from the rest of the intestines
this function is expected to be useful in a culture lacking modern sanitation, where diarrhea may be prevalent
this function would explain the health of individuals without appendixes in developed countries, and the worm like shape of the appendix, with copious amounts of immune tissue
regardless of the appendix’s function it is extremely important to have it removed immediately the event of appendicitis
large intestine (chyme mixes with bacteria)
the large intestine’s primary role is water absorption from the undigested material and aid in elimination of feces
also absorbs Na and other electrolytes, vitamin K, small amounts of vitamin B9 (folic acid), vitamin B7 (biotin), and vitamin B5 (pantothenic acid) produced by enteric bacteria
unlike the small intestine the large intestine does not continuously move the fecal bulk toward the anus. The large intestine uses “mass" movements” occurring only periodically push the fecal bulk toward the rectum (3-4 times a day)
defecation
when the mass movements of the large intestine move faces to the sigmoid colon, this activated the sensory neurons in the GI wall
the PSNS relaxes the internal sphincter of the anus & somatic impulses contract the external sphincter (skeletal muscle)
we have conscious control over the external sphincter
during dedication mass movements push faces toward the anus and is aided by conscious contraction of the abdominal wall and diaphragm (valsava maneuver)
portal stimulation
the superior and inferior mesenteric veins drain the blood from the GI tract that contains the absorbed nutrients
these veins drain hepatic portal vain leading into the liver
this allows the liver to control the amount of nutrients entering the general circulation
the hepatic portal vein delivers 2/3 of the blood entering the liver
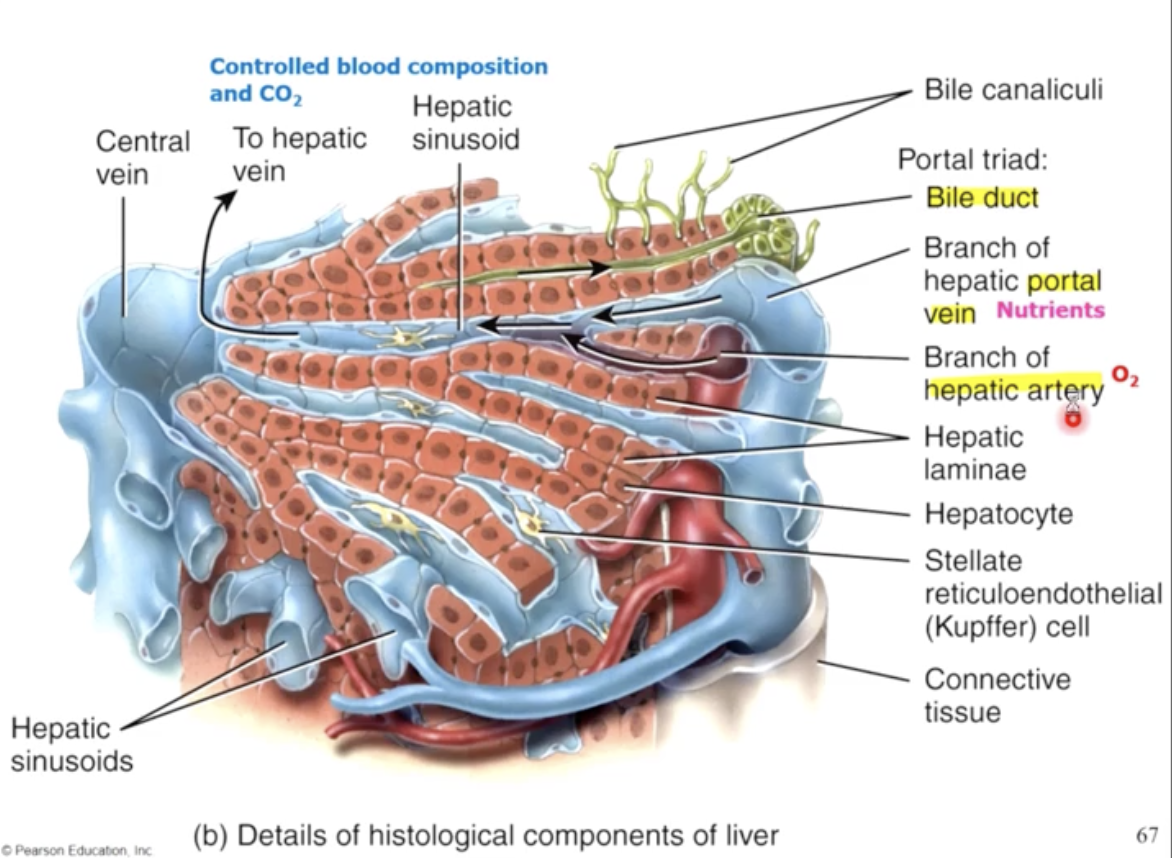
The livers role in digestion and metabolism
in addition to it’s role in bile production, the liver aids in digestion by:
1) storage of glycogen, Lipid, fat soluble vitamins and iron resevoirs
2) destroying dissolved bacteria by filtering portal blood through sinusoids containing macrophages called Kupffer Cells
3) Maintaining glucose, amino acids & fatty acid levels in blood (at times through interconverting nutrient types e.g. conversion of carbohydrates to lipids)
4) catabolism of amino acids and producing urea
5)) production of fat acids, triglycerides, cholesterol, and lipoproteins (ie. HDL and LDL)
6) metabolism of drugs, hormones (E,NE, sex hormones, steroid hormones), and toxins in the ER (endoplasmic reticulum)
7) breakdown of hormones, antibodies and old RBC’s
8) synthesis of clotting factors an plasma proteins
Fluid Turnover in the GI tract
in order to mechanically and chemically digest food, the GI tract secretes about 7 litres of fluid, including bile, enzymes and mucus
therefor failure of absorption can rapidly cause dehydration through losses of ingestion and secreted fluid (up to 9 litres per day)