Mycology Week 2/2
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
59 Terms
pathogenesis of dermatophytes
-which genera infect skin, hair and nails
-they cause superficial fungal infections mostly (so harir, skin nails)
-mostly dermatophytes, some non-dermatophytes
-itchy, red raised patches that may blister and ooze
-usually sharply-defined edges, often times creating a ring with a more normal skin color inside
-can be transmitted person to person, animal to person, etc - YOU NEED TOUCH! to person or to infected object an infected person touched (can live on inanimate objects)
-common in gyms and locker rooms because used and moist places
-highy contagious
-usually clinical diagnosis (just see ringworm shape) but also KOH test/microscopic examination
-wood's lamp is a UV lap that can help tinea capitis since hair sometimes fluoresces when infected with Microsporum and Trichophyton
-in general dermatophytes cause ring worm = tinea and has different names based on the area!
GENERA FOR HAIR/SKIN/NAILS: trichophyton
dermatophytosis
fungal infection of the skin of dermatophytes only
Direct Exam from patient tissue:
-thin, SEPTATE hyaline hyphae ONLY NO CONIDIA JUST HYPHAE FROM DIRECT SPECIMIN!!! maybe arthroconidia
dermatophytes
-filamentous fungi that can digest and obtain nutrients from keratin
-don't usually INVADE HOST TISSUE, they colonize the outermost layer of the skin
Ringworm
-tinea!!
-caused by fungus
-enzymes are released by the fungus during digestion and the physical signs of ringworm are bacause of the hosts' repsponse to these enzymes

other info
-grow slow (4-20 days)
-often used Mycosel, DTM special medias
OLD GENERA!
clinical diseases cauased by dermatophytes
3 genera of fungi that are dermatophytes
MICROSPORUM
-hair and skin (many macro and many micro conidia)
TRICHOPHYTON
-hair and skin and nails (TRi = 3)
-rare macroconidia but many microconidia
EPIDERMOPHYTON
-skin and nailsf
-numerous macroconidia, no microconidia
keratinophilic
geophilic
zoophilic
anthropophilic
tinea unguium
ringworm of the nails caused by A DERMATOPHYTE
-onchomycosis is just caused by any fungi
tinea pedis
foot disease caused by dermatophytes
ATHLETE'S FOOT
tinea barae
bearded area of face and neck infection by dermatophytes
tinea manuum
hand disease
tinea cruris
groin, perineum, perianal region disease caused by dermatophytes
JOCK ITCH
tinea corporis
skin on body/trunk disease caused by dermatophytes
onchomycosis
Tinea unguium --> only dermatophytes
-nail infection caused by any fungus (not just dermatophytes like candida, aspergillus, scopulariopsis)
tinea capitis
scalp and hair shaft disease caused by dermatophytes
principle of the KOH smear for examining specimens from skin, hair nails
-drop of 10% KOH on slide and a small quantity of specimen
-gently heat the smear
-coverslip and examine microscopically
KOH breaks apart the keratin and skin layers makes hypae easier to see if present
diagram and describe
-epidermophyton
-produces only macroconidia that are smooth-walled, club shaped, multi-septate)
diagram and describe
-microsporum
Microsporum canis
-common cause of ringworm in children
-commonly from infected dogs/cats
-reverse side can be yellow/orange
-cottony/floccose colonies that are white and turn brown in the center
-hyphae are hyaline and septate
-numerous thick-walled, SPINDLE SHAPED, multi-celled macroconidia
-some macroconidia have curbed knob at the end (dog's tooth, looks pointed on both ends kinda with a curved end which is the dog's tooth)
-usually >6 compartments inside macroconidia
-a few microconidia may be made that are club-shaped (RARE)
-Microsporum gypseum (nanizzia gypsea)
*fringed colonies that are like cinnamon-powder with white border
-from dogs, cats, rodents
-causes scalp/skin infections in humans
-macroconidia are rough-walled and often clustered
-cylindrical to fusiform shaped with NO MORE than 6 comparments
-ends are ROUNDED not pointy
-small club-shaped microconidia may be seen along hypae
-symmetric, rough, thin-walled with ROUNDED ends
Microsporum audouinii (if not in lab, just put bold)
-tinea capitus in children
-sub-Saharan Africa
-gray/white colony with salmon reverse
-produces pectinate aka comb-like hyphae
-sometimes can produce odd shaped conidia that look like M. canis but hyphae have termina chlamydoconidia

Microsporum gypseum (nanizzia gypsea)

Microsporum audouinii
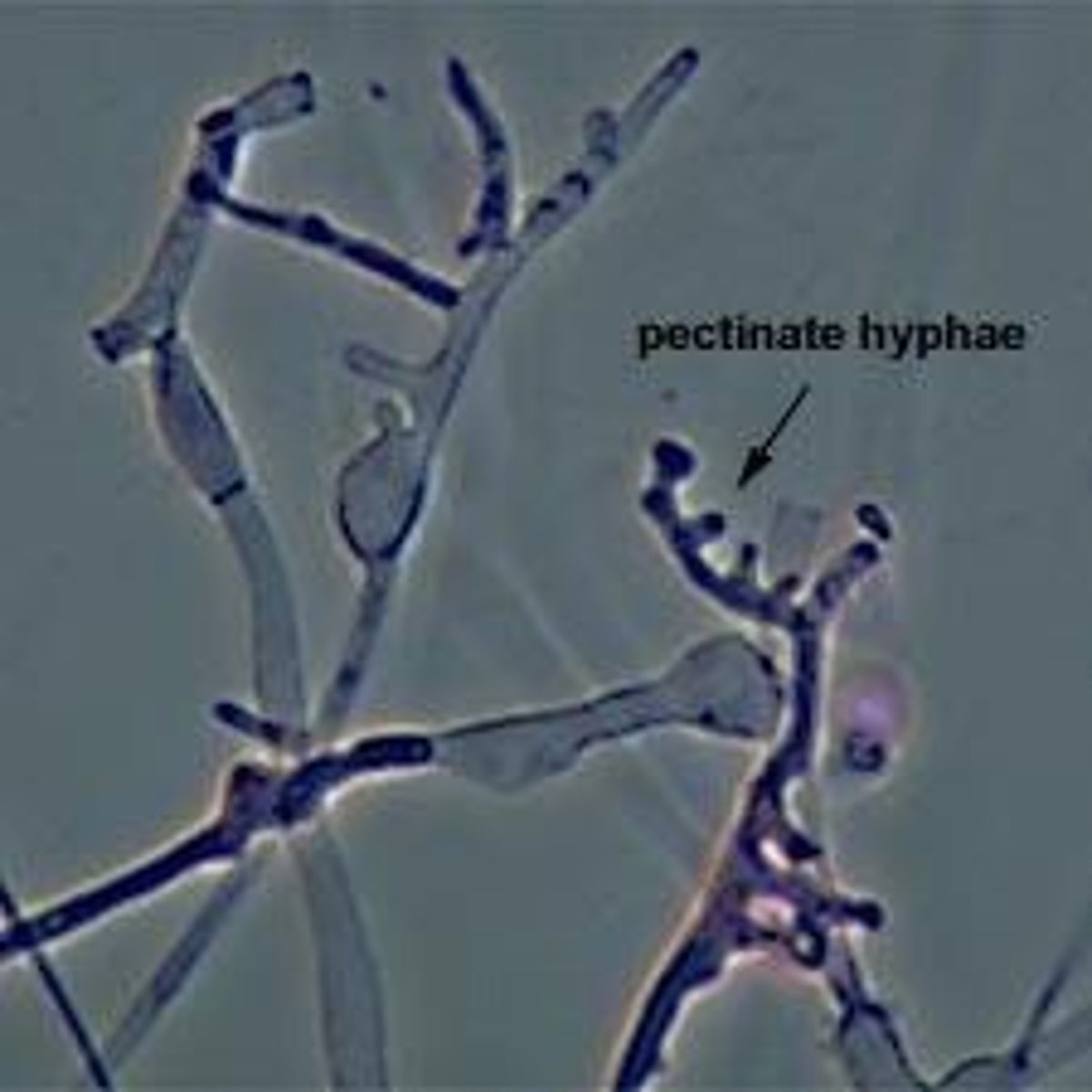
diagram and describe
-trichophyton
-mainly microconidia arranged singly or in clusters
-rare macroconidia that are elongated, pencil to cigar shaped, smooth walled, thin walled, multiseptated
RUBRUM:
-most frequently isolated dermatophytes causing infection worldwide (ringworm, athlete's foot)
-fluffy white colonies with reverse side being red (rubrum) being produced when older
-hyphae are small, septate, hyaline
-pyriform (tear-drop shaped) microconidia along hyphae (not clustered, look like birds on a wire)
-macroconidia can be there and are pencil-shaped, multi-cellular, attached to hypae by thick attachements (RARE)
-TEAR shaped microconidia!!!
TONSURANS
-most common cause of SCALP RINGWORM in the US
-velvet/suede like colonies
-reverse reddish-brown
-hyphae are small, septate, and hyaline
-pleomorphic microconidia usually tear-dropped shape or club shaped, could also be round aka balloon like
-rubrum is more organized, these tend to cluster more on the hyphae
-macroconidia are rare
-could have chlamydoconidia
SCHOELEINII
-severe, chronic favus (scarring scalp) infection resulting in permanent hair loos
-growth often submerged in medium and appear yeast like
-knobby, irregular hyphae
-subsurface hyphae from antler-like branches called favic chandeliers with slowell tips like nail heads
-micro and macro conidia are ABSENT

Trichophyton Agars
-differential media to identify Trichophyton based on nutritional requirements
-incubate up to 2 weeks
-T agars
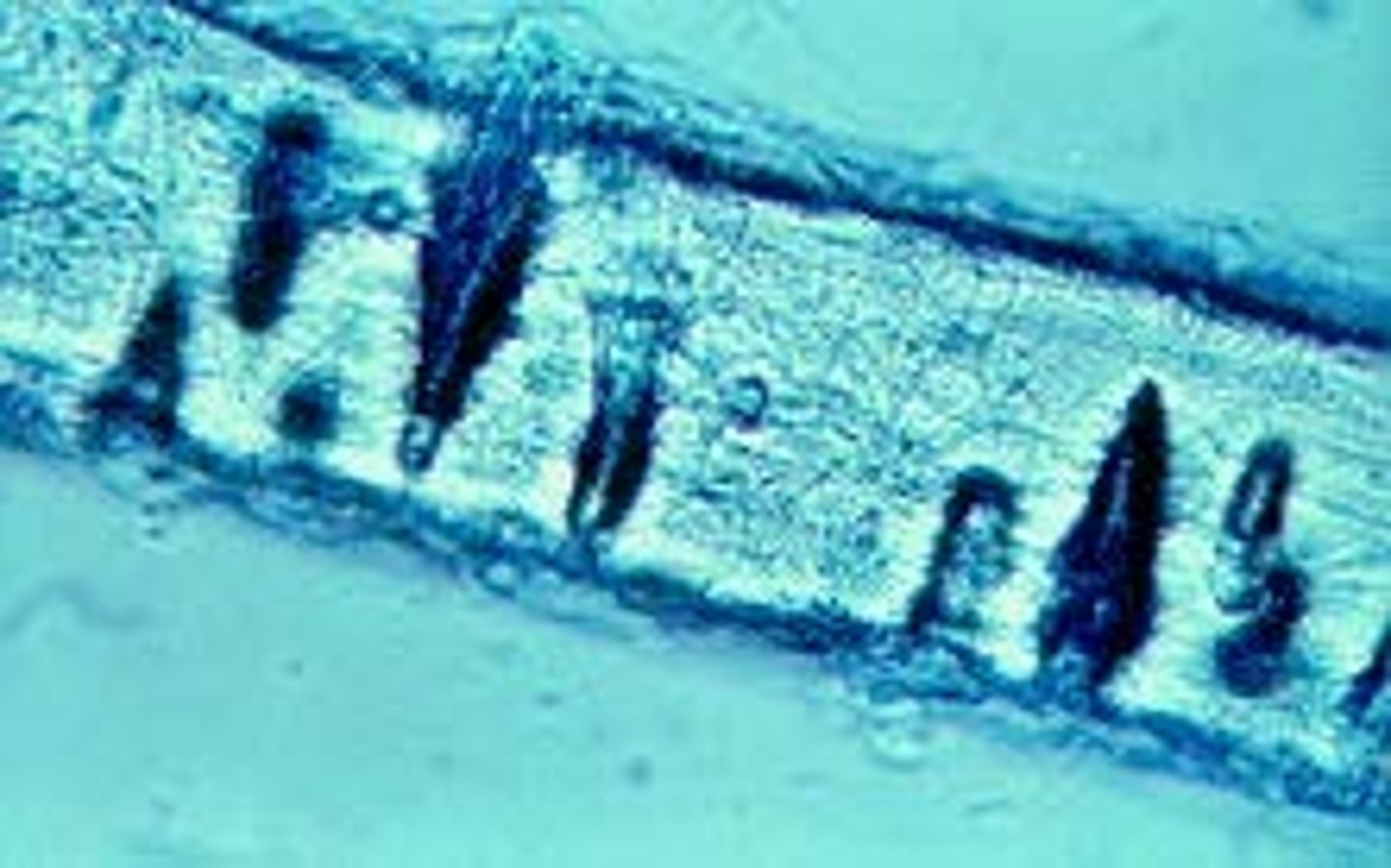
Hair Perforation Test
-Trichophyton mentagrophytes (+) vs T. rubrum (-think)
-take hair, autoclave it, and then place fungus in tube
-incubate at room temp for 4 weeks and look weekly for + reaction
MENTA: can have macroconidia but tonsurans can never have macroconidia
TONSURANS is more balloon-shaped and tear dropped. I think menta is more round conidia!
+ = endothrix (wedge, shaped performations cuased by hyphae penetrating hair)
- = ectothrix (fungal hyphae remain outside the hair shaft)
how to identify: Epidermophyton floccosum
-causes jock itch, athlete's foot, nail infections
-macroconidia are blunt, club-shaped, multicelled (2-6) and singly or in groups of 2-3 attached
-macroconidia transform into chlamydoconidia with age
-arthroconidia are common with age
-may see sterile hyphae with older age
-no microconidia
-hot dog shaped to me!!!! or poo lol
-form chalmydoconidia on lots of pictures they had for us

dermatomycosis are the
-most common fungal infections worldwide
-more common in tropical environments = warm and wet
-tinea pedis is the most common
-tinea capitis very common in children
how to identify: Microsporum canis
ABOVE Already
how to identify: Trichophyton rubrum
+ urea results
positive? from internet
how to identify: T. mentagrophytes
+ urea results
urea +, the rest is above
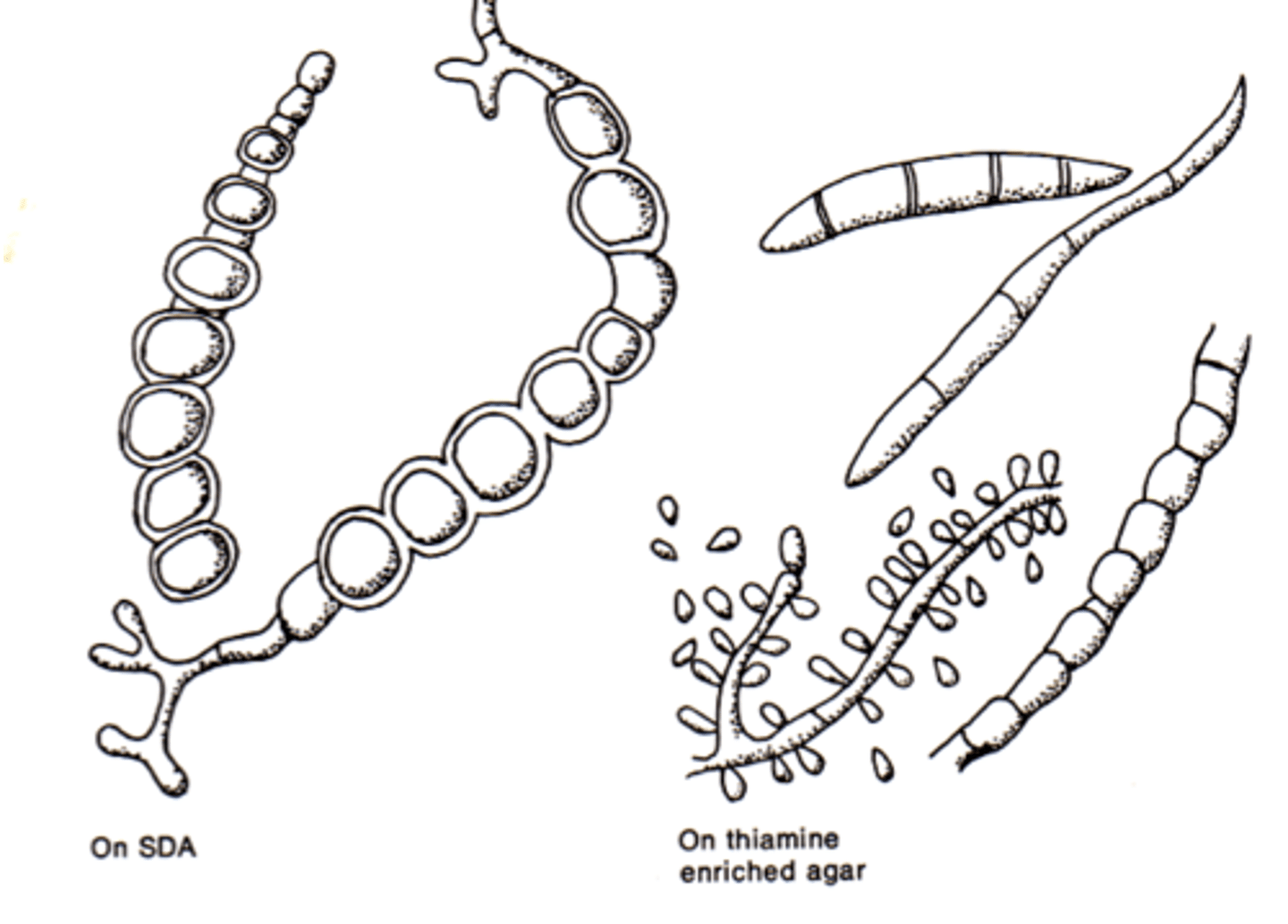
how to identify: Trichophyton verrucosum
+ growth requires for thiamine and inositol
-t. verrucosum requires casein + thiamine
skin-like, WAXY dimpling the agar, sand$ looking colonies
macroconidia look like rate tails
tests used to identify species within Trichophyton
-urea
-hair perforation test
-growth requirements for casein, thiamine, inositol
-historically, trichophyton species were differentiated by their requirements for casein, thiamine, and inositol
-T. tonsurans requires thiamine for grwoth or thiamine + inositol
-t. verrucosum requires casein + thiamine
-urease test helps differentiate T. rubum (-) from T. mentagrophytes (+)
-hair perforation test also differentiates T. rubum (-) from T. mentagrophytes (+), can invade the hair shape and can be seen microscopically)
Pneumocytsis jiroveci
THIS IS NOT A DERMATOPHYTE (subcut)
-until 1980 thought to be a parasite
-only fungus to lack chitin in cell wall
-lacks ergosterol too in cell membrane, has cholesterol
-not susceptible to amphotericin B
-susceptible to antiparasitic agents
-more fragile cell wall that other fungi
-CAN'T GROW IN CULTURE
-CAN ONLY INFECT THE LUNG (could be commensal there)
-AIDS defining illness
-trophozoites form vs cyst form
-this species is unique to humans
-carinii is unique to rats
-causes severe pneumonia in immunocompromised
PCP = pneumoncytsis pneumonia
-seen cysts and intracystic bodies (double comma or parenthesis like) in stain preps from bronchoscopy with lavage
microsporidia
NOT A DERMPAH -- caused subcut infection
-unicellular eukaryotes
-obligate intracellular fungi (was though to be a parasite too)
-the most common ones end in zoon
-acquired through ingestion or inhalation
-chronic water diarrhea
-AIDS patients another defining illness
-usually take fecal, urine, and respiratory secretions
-injects a polar tubule into the cell and released sporagispores
-might say white belt across the spore
subcutaneous fungal infections
-deeper layers of the skin
-from traumatic implanation
-soil saprophytes and can vary by geographic region
-many already discussed
-sporotrichosis (sporothrix spp)
-chromoblastomycosis (mainly Fonsecaea, Phialophora, Cladophialophora, etc.)
-phaehyphomycosis (mainly cladophialophora, exophiala, bipolaris)
**Cladophialophora bantiana is a long chain of metal chains it looks like to me; they say kinda looks like cladosporium, i Disagree lol
***C. carrionii looks like penicillium. she gonna tell me tmr how to differentiate; pen has green colonies, carrionni will have dark colonies bc dematiatious
-mycotic mycetoma (scedosporium, madruella, acremonium, exophiala)
-lobomycosis (loboa loboi)
*Lacazia loboi or above name is older
*only in the Americas in humans and dolphins
*verrucoid to nodular lesions and crusty plaques, and tumors
*surgical excision is first treatment but often reoccurs
*does not grow in culture
*often found causing LOBEY ears and grow in chains of fungi globules
*fungus seen as globulose cells connected by a narrow neck
-rhinosporidosis (rhinosporidium seeberi)
*doesn't grow in culture, now a parasite, though to be a yeast before
*reddish mucosal poly in the nasal cavity that bleeds profusely on touch
*EWW!!
*endemic to India and Sri Lanka
*large round sporangia containing sporagiospores
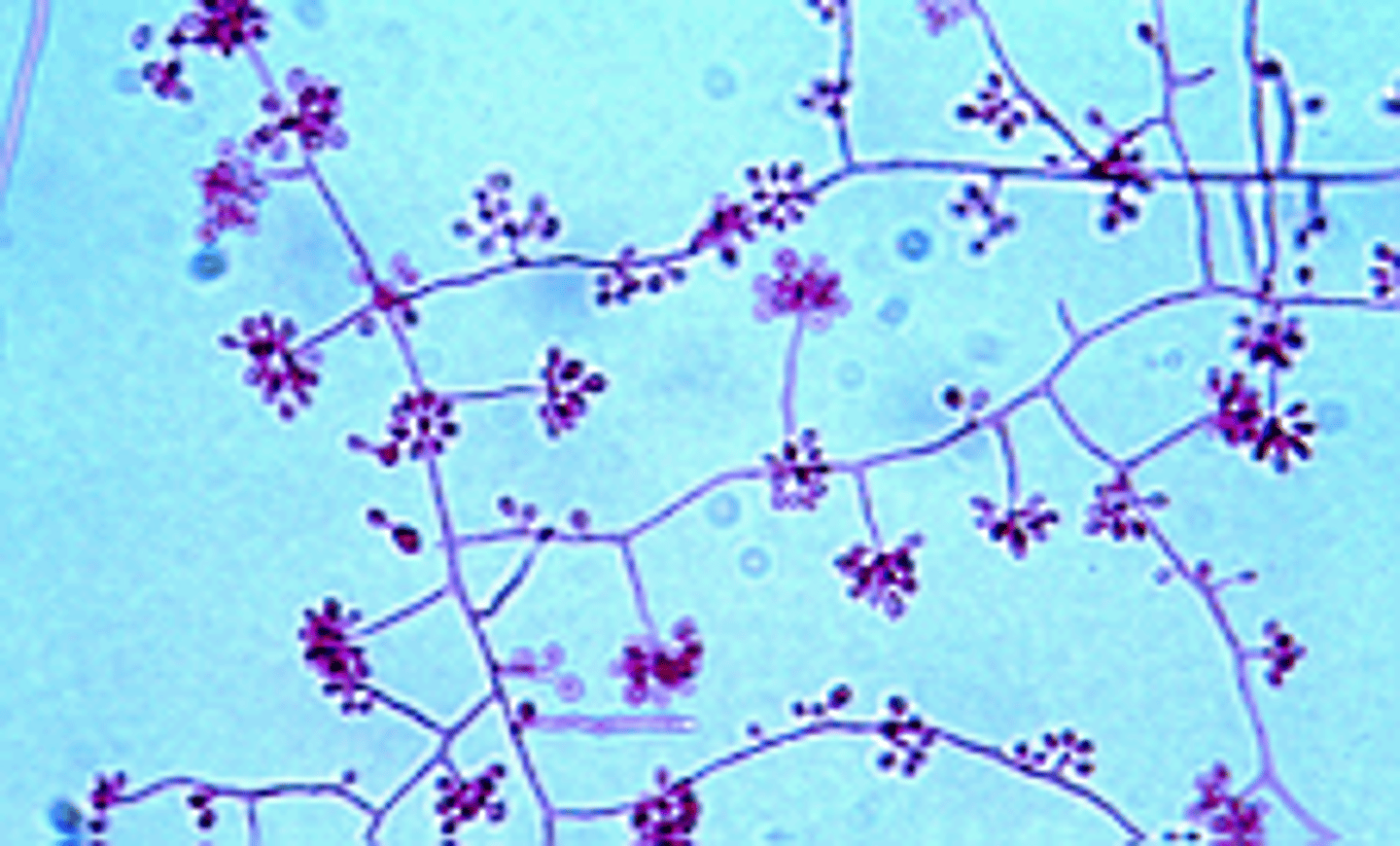
sporotrichosis (about, etiology, agent)
-Sporothrix schenckii complex
-Rose Gardener's Disease
-world wide but common in warm places
-florists, gardeners, outdoor enthusiasts, farmers
-DIMORPHIC FUNGI that is mold in the soil, yeast in the body
-most often found in rose bushes, wood splinters, thorns, etc
-aerosolization is possible but rare
-first sign is small, painless nodule that can look like insect bite occuring 1week - 3 months after
-then the one nodule forms another nearby and in a line they move up the arm!!!
-nodule gets larger and looks like open sore/ulcer that is slow to heal
-can spread to bones, joints, and CNS in immunocompromised
YEAST/direct exam: elongated yeast cells that look like cigars with buds (Cigar bodies)
MOLD: white to cream, later become wrinkled brown or black with white border, grows within 7 days (kinda fast) (mold is pictured here)
-mold is called small tear-shaped conidia in clusters like rosettes!
mycetoma (about, etiology, agent)
-bacterial
-fungal
chromoblastomycosis (about, etiology, agent)
Sporothrix schenckii in tissue specimens
-microscopic morphology
already above!
key microscopic characteristics of mold phase of S. scheckii when incubated at 25-30C
investigate etiological agents of mycetoma
-actinomycotic vs eumycotic mycetoma
-clinically significant bacteria in each category
- chronic infection usually of the lower extremeties (feet)
- tumor like deformities that drain pus with granules
FUNGI:
-many fungi that have septate hyphae
-usually dermatiaceous fungi
-Pseduoallescheria boydii (sexual state with cleistothecia)
-Scedosporium apiospermum (asexual state)
**lollipop on a stick; septated hyphae, simple conidiophores, truncate base conidia technicallly but hard to see
-ALSO could be acremonium, exophiala, curvularia, and madurella mycetomatis though
BACTERIA (aerobic actinomycetes including...)
-Nocardia
-Streptomyces
-Actinomadura
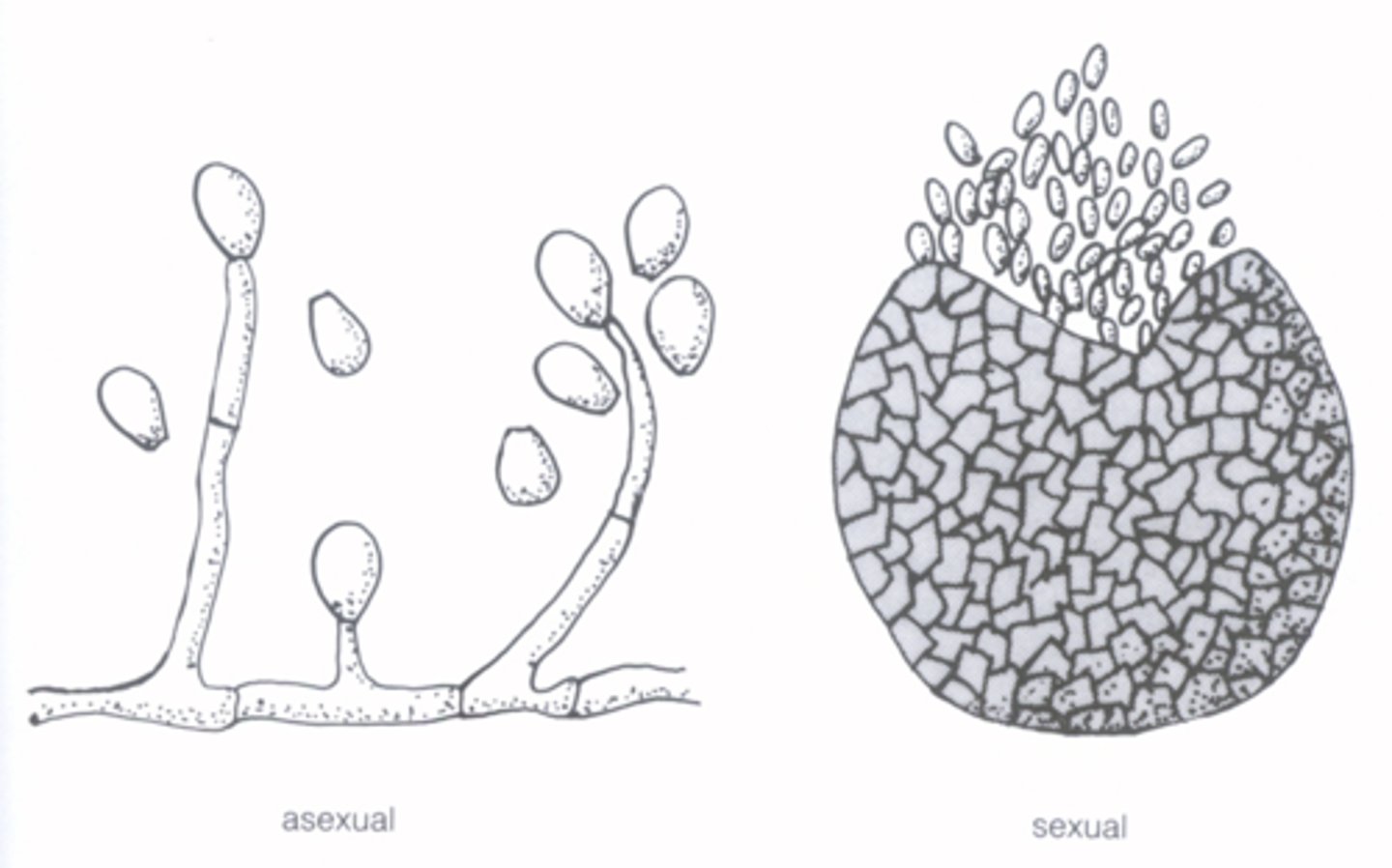
microscopic features of pseudoallescheria boydii/Scedosporium boydii COMPLEX
-study guide has lots of good pictures for these and some things above too!!
PBoydii:
-sexual state
-large brown cleistothecia
-elliptical ascospores inside
SBodyii:
-asexual state
-septate hyphae with simple, conidiophores
-conidia are unicellular, oval, and truncate (cut off at the base)
biochemical characteristics of the Nocardia species
-aerobic, branching G+ rods
-partially acid-fast
-3-6 days in culture (so often done in mycology lab)
-streptomyces similar in all ways except partially acid-fast negative
list dematiaceous fungi associated with chromoblastomycosis and the fungus MOST FREQUENTLY implicated
-muriform bodies?
-other names for muriform bodies?
-chromoblastomycosis: wart-like tumors via traumatic implantation; cauliflower
-most common in tropical and subtropical areas
-sclerotic bodies, muriform bodies, copper-penny bodies
-Phialophora verrucosa, Fonsecaea pedrosoi, Fonsecaea compacta, and cladophialophora carrionii
Phialophora (lab only)
-lots of microconidia
-dematiaceous hyphae
-causes subcutaneous infections (chromoblastomycosis, maybe phaeohyphomycosis)
-flared cup-like collarettes; look like a vase of flowers??
what is a dimorphic fungus
-list ALL the clinically significant fungi in this category that are agents of systemic mycoses (systemic fungal infections)
-thermally dimorphic (yeast in the beast, mold in the cold)
-dirmophic system mycoses of these are usually multiple tissues and organs that overcome cellular defenses of the host by changing their form
-THEY CAUSE SYSTEMIC DISEASES and many have geographic locations they are found in!! sporo is the only superficial one, the rest are systemic.
-geographically restricted
-primary site of infection is pulmonary bc of conidia inhalation
*Blastomyces species
*coccidiodes immitis/posadasii
*histoplasma
*paracoccidiodes
*talaromyces marneffei (before was penicillium marneffei)
*Sporothrix schenckii
discuss geographic distribution and ecology of the dimorphic fungi
pathogenesis and clinical infection associated with the dimorphic fungi
systemic infections
TISSUE and MOLD phase microscopic: Histoplasma capsulatum
-little suns!
-RIGHT half of the US lol, pretty common in MN
-endemic to Ohio and Mississippi river valleys
-small budding yeast
-old buildings, bat guano in caves
-old chicken coops, spreading fertilizer rich in chicken shit
-anything with old bird droppings
-inhaling MICROconidia!!! bc macro too big to get to alveoli
-intracellular, can live inside macrophages
-95% asymptomatic but could be pulmonary infection
-once inside alveoli, turns to yeast
-can live inside the macrophage like TB
-most infections are self-limiting
-culture specimens are lower respiratory tract and blood, maybe bone marrow or brain
-NARROW BASED BUDS IN YEAST FORM; can look like toxoplasma protozoa
-stain could look to have a capsule which is where it got it's name from but it doesn't have a capusle
-tuburculate macroconidia are diagnostic for this!!!
-MOLD FORM: TUBURCULATE MACROCONIDIA!!!!!!!!! SUNS!!
white daisy's or cotton looking on plate
-tuberculate macroconidia is pictured in mold form
-small pear, shaped microconidia in mold form
-antigen detection, serology, PCR could identify too, or MALDI
TISSUE and MOLD phase microscopic: Blastomyces dermatitidis
Blastomyces in general stuff:
-fungus endemic to Ohio and Mississippi River valleys, Great Lakes
-soil, decaying wood, rivers, lakes, recreational water
-inhalation of conidia
-could by asymptomatic, acute pneumonia, chronic pnuemia, or acute respiratory distress syndrome (ARDS)
-usually go systemic to skin, soft tissue, bone, etc
-cough, fever, SOB, night sweats, weight loss, non-healing skin lesions
-diagnose with bacterial pneumonia first but antibacterial agents don't work and then a fungal infection is considered
-50% asymptomatic and resolve without tx
-macro and micrscopic morphology used the most
DERM STUFF
-37C so LARGE yeast form they have thick, refractile, double-countoured cell walls, single broad based bud, they can even fold in on themselves a little bit. don't tend to break off until they are the size of the parent cell
-Mold form: in culture plate, filamentous mold with septated hyphae, short or long conidiophores, round/pear shaped conidia at the apex of conidiophore (lollipop), or directly from hyphae, need to differentiate from scedosporium (also lollipop)
-classic eastern 1/2 of the US
-very common in DOGS becuase they love to sniff the ground and then they spreada it to us.
COLONY MORPH: prickly and spiky usually means dimorphic.
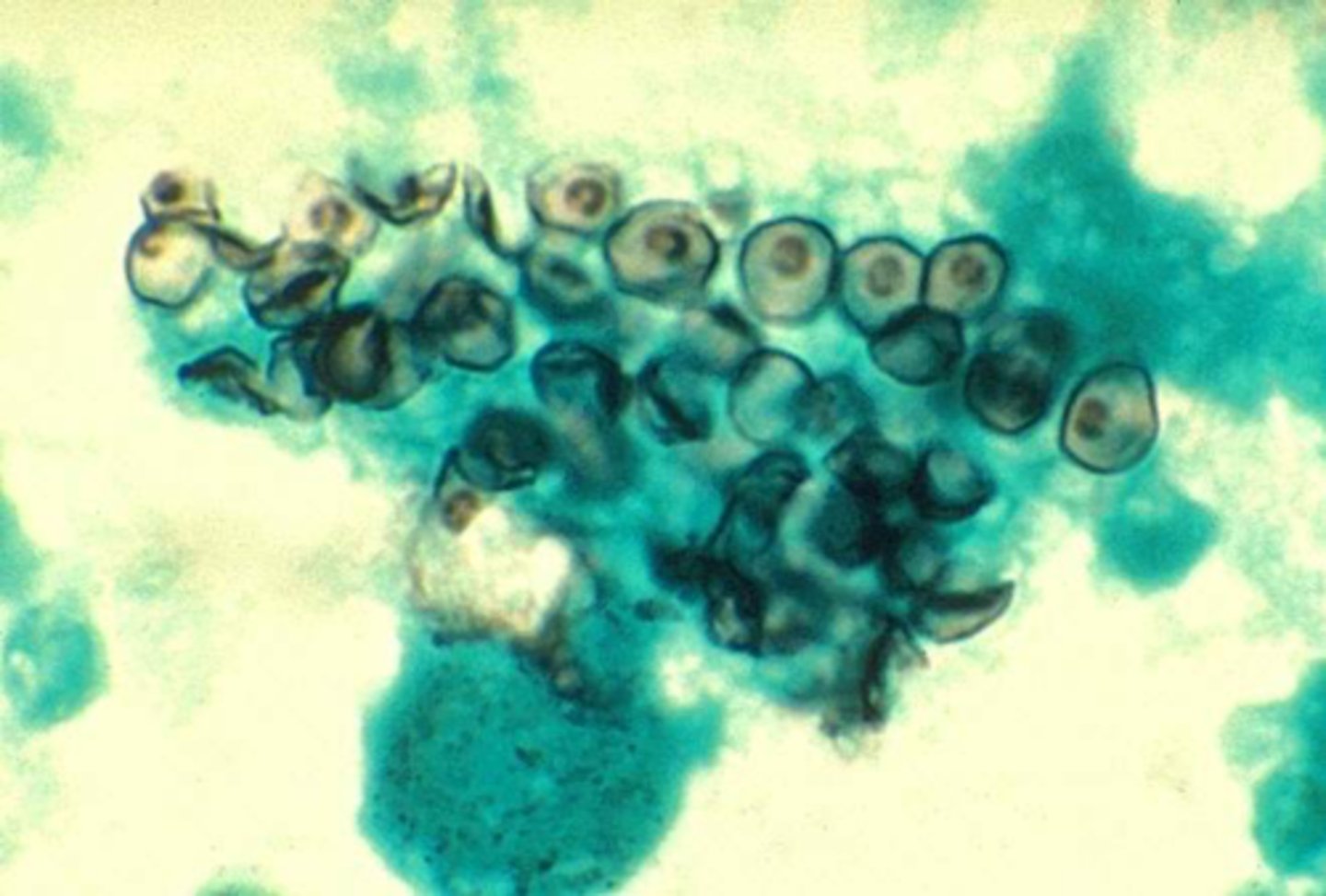
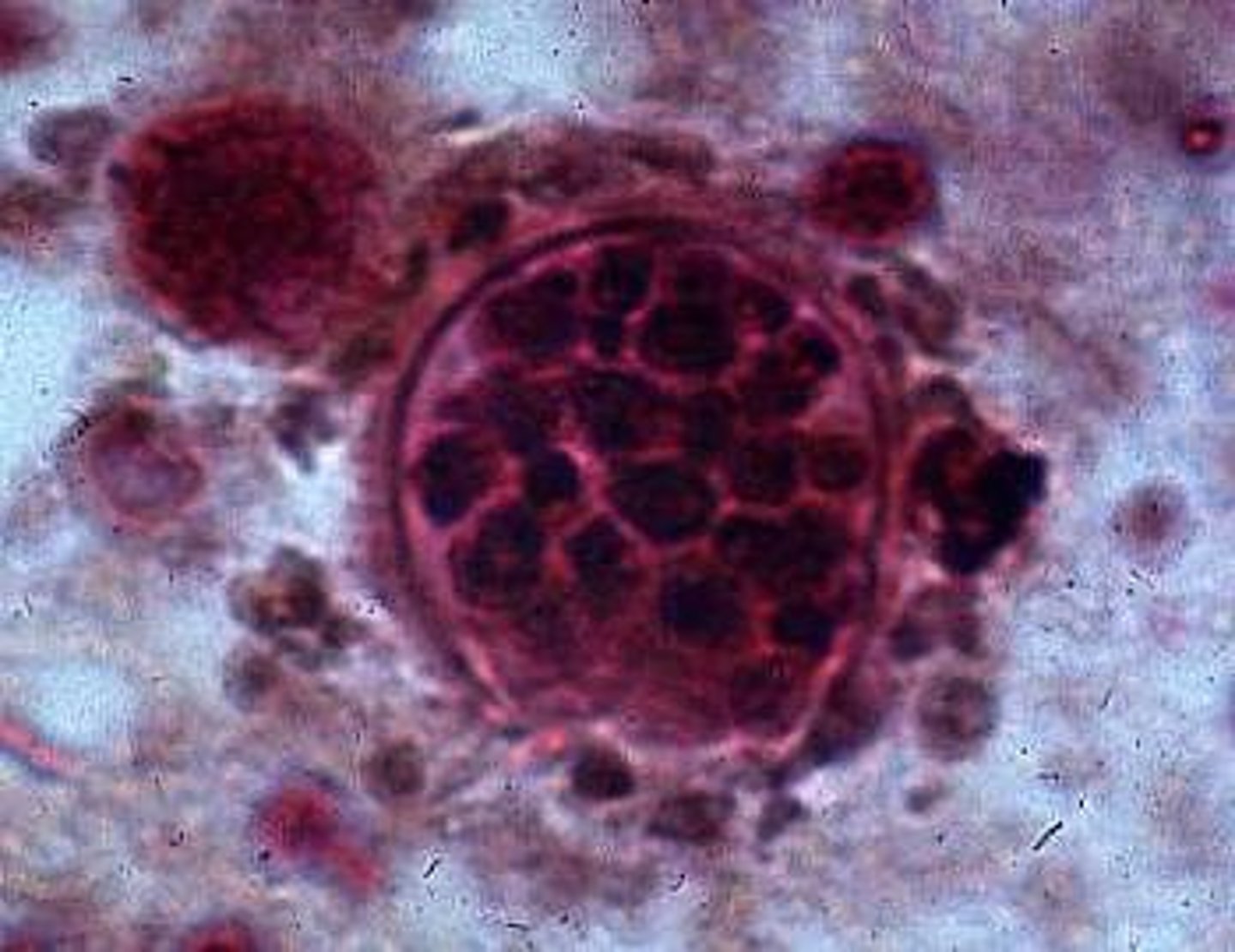
TISSUE and MOLD phase microscopic: Coccidiodes immitis
COCCIDIODES
-valley fever!
-filamentous fungi in culture
-no YEAST like colonies in direct, instead spherules in tissue
-C immitis is Valley Fever, Cali San Joaquin valley
-C posadasii: SW US and mexico
-winds dissemintate the arthroconidia for many miles and inhaled
-athroconidia inhaled into lungs then transform in multinucleated spherical structures containing hundreds of endospores
-most are asymptomatic but some have rash + pneumonia
-if spreads it goes to lymph nodes, joints/bone, skin
-identify by spherules in smear with endospores inside
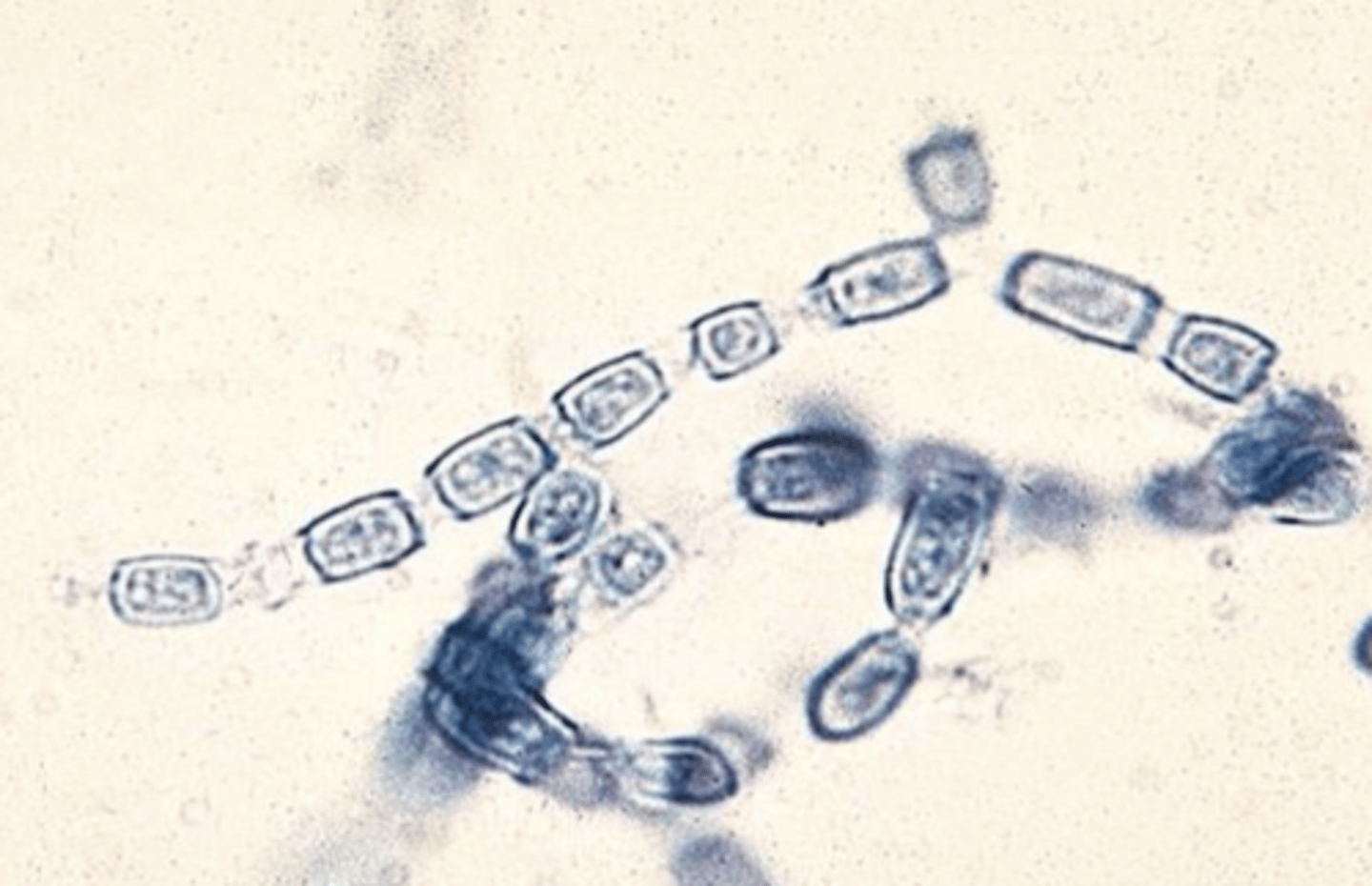
Coccidiodomycosis (Valley Fever)
-cottonly white mold form in culture
-high risk for labs cause arthroconidia aerosolize easily
-identify with MALDI
-used to be a potential bioterrorism agent
YEAST: spherules with many endospores inside
-MOLD: barrel-shaped arthroconidia and alternate between disjunctor cells that fracture easily
CULTURE: cottonly mold that can grow on SBA
-was a bioterrorism agent until 2012 when they said easier to just go to AZ and get soil than steal from our lab LOL
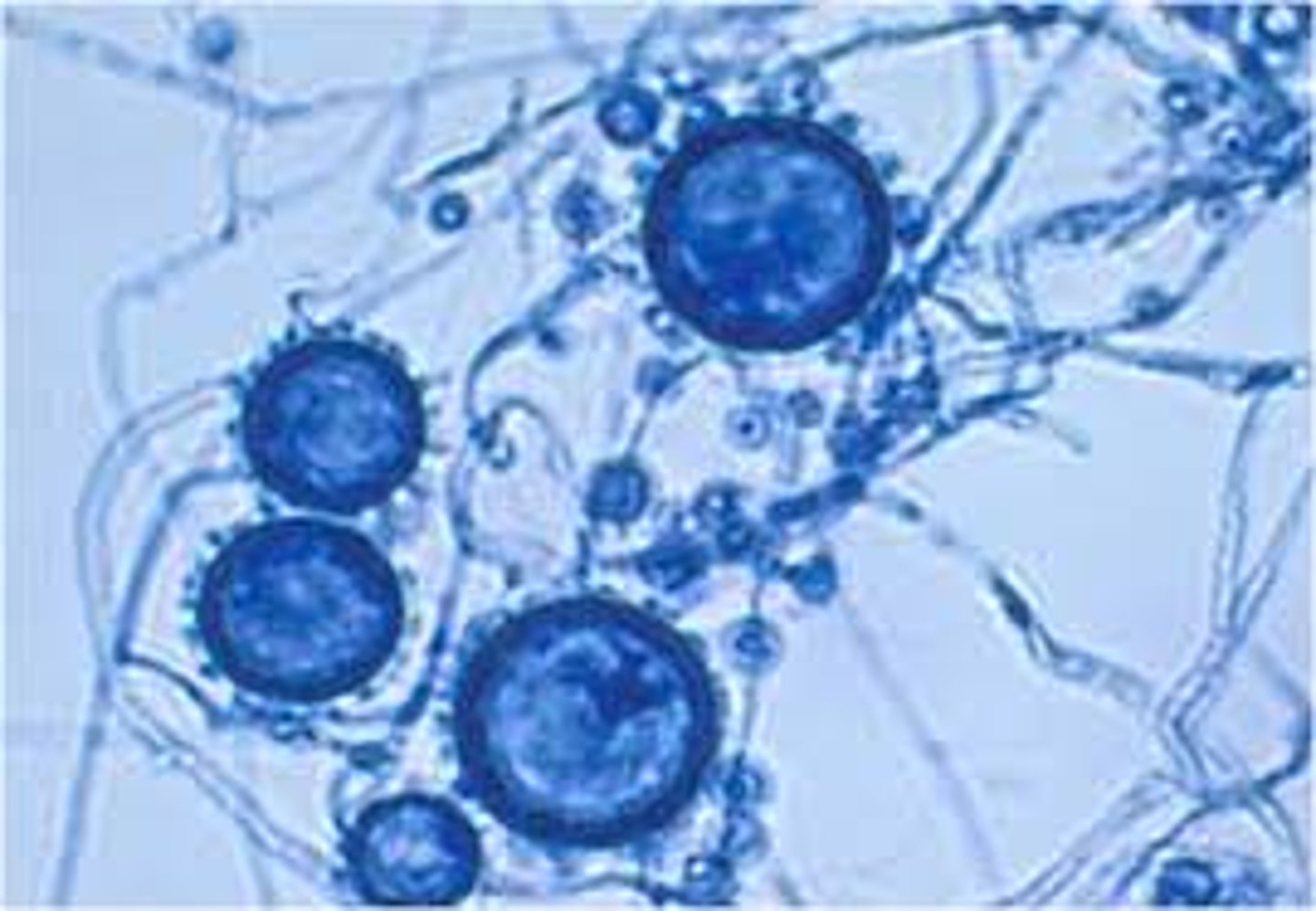
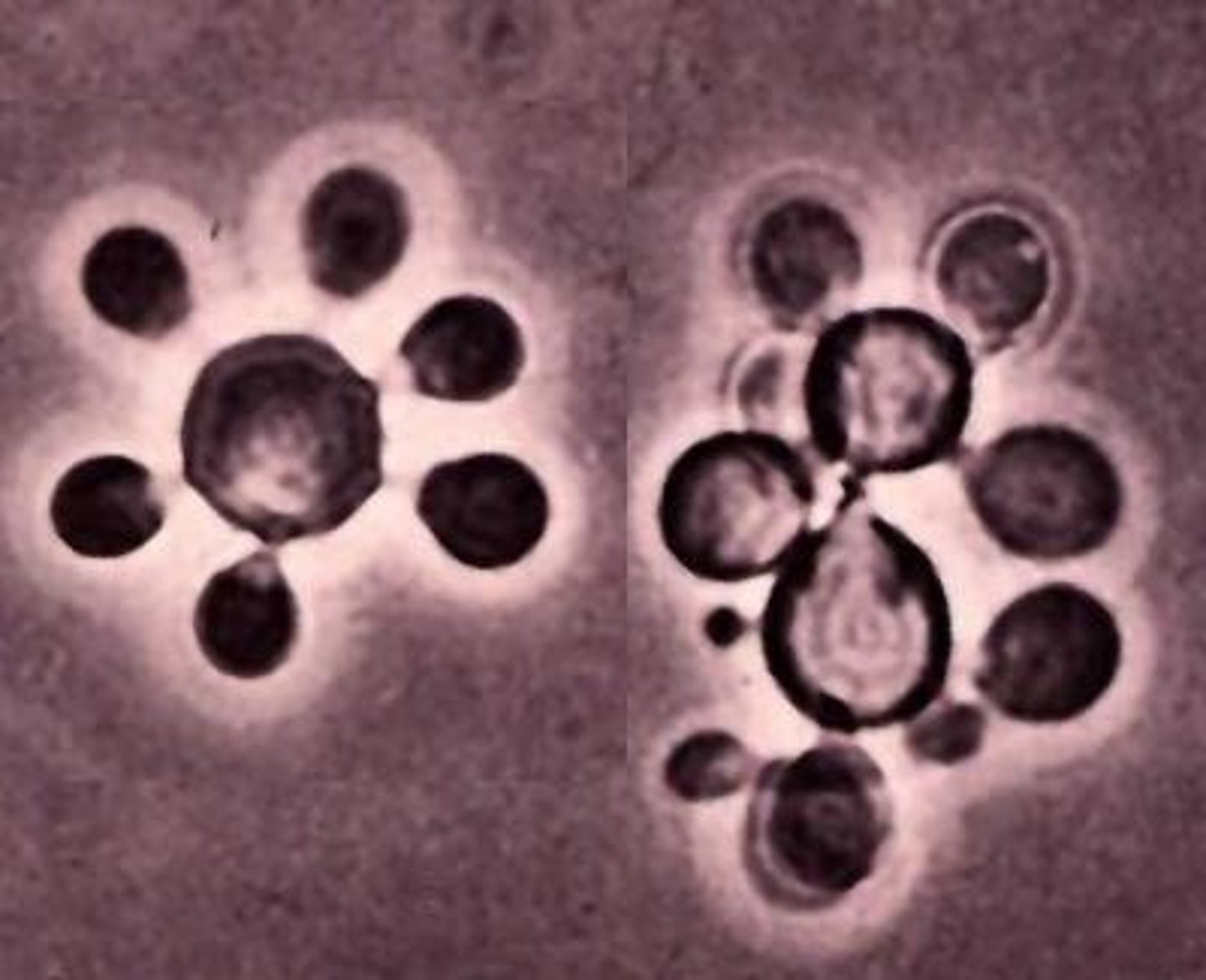
TISSUE and MOLD phase microscopic: Paracoccidiodes brasiliensis
-central mexico, central america, south american just not chile (weird!)
-80% in brazil
-ecology is unknown but in areas with high humidity usually
-inhalation on CONIDIA
-spreads from lungs to lymph nodes and then to skin
-slowly progressive disease (months to >30 years)
-ulcerative mucocutaneous lesions of face, mouth, nose is most obvious sign
-culture takes 6-8 weeks to grow so serology can be done
MOLD: -septate, branched hyphae with a few chlamydospores
YEAST: -large yeast with multiple buds around mother cells (Mickey Mouse :)) (yeast is pictured)
**Histoplasm mold form can look similar to this but its the mold form THIS IS HOW IT GROWS IN HUMANS/DIRECT SPECIMEN
based on a description of the organism in a direct exam, identify the most probable pathogen:
-a gram stain from sputum was + for large, round oval yeast with broad-based buds. What is this organism?
Blastomyces dermatitidis
alternate molecular tests for identifying dimorphic fungi in the lab and their significance
PCR, MALDI, lol idk the usual
Phaehyphomycosis
-what is it
-which organisms most associated with it
above i think!
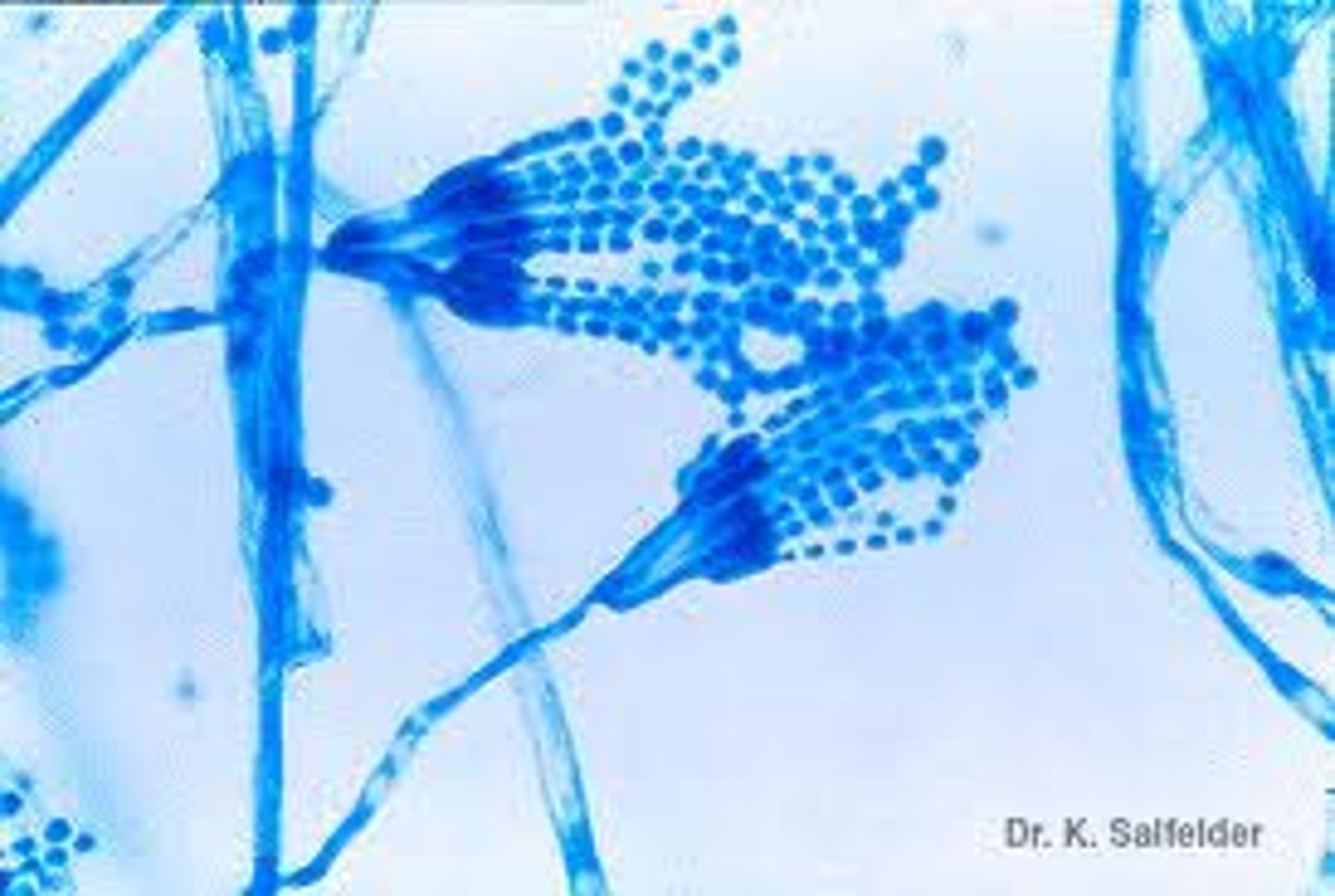
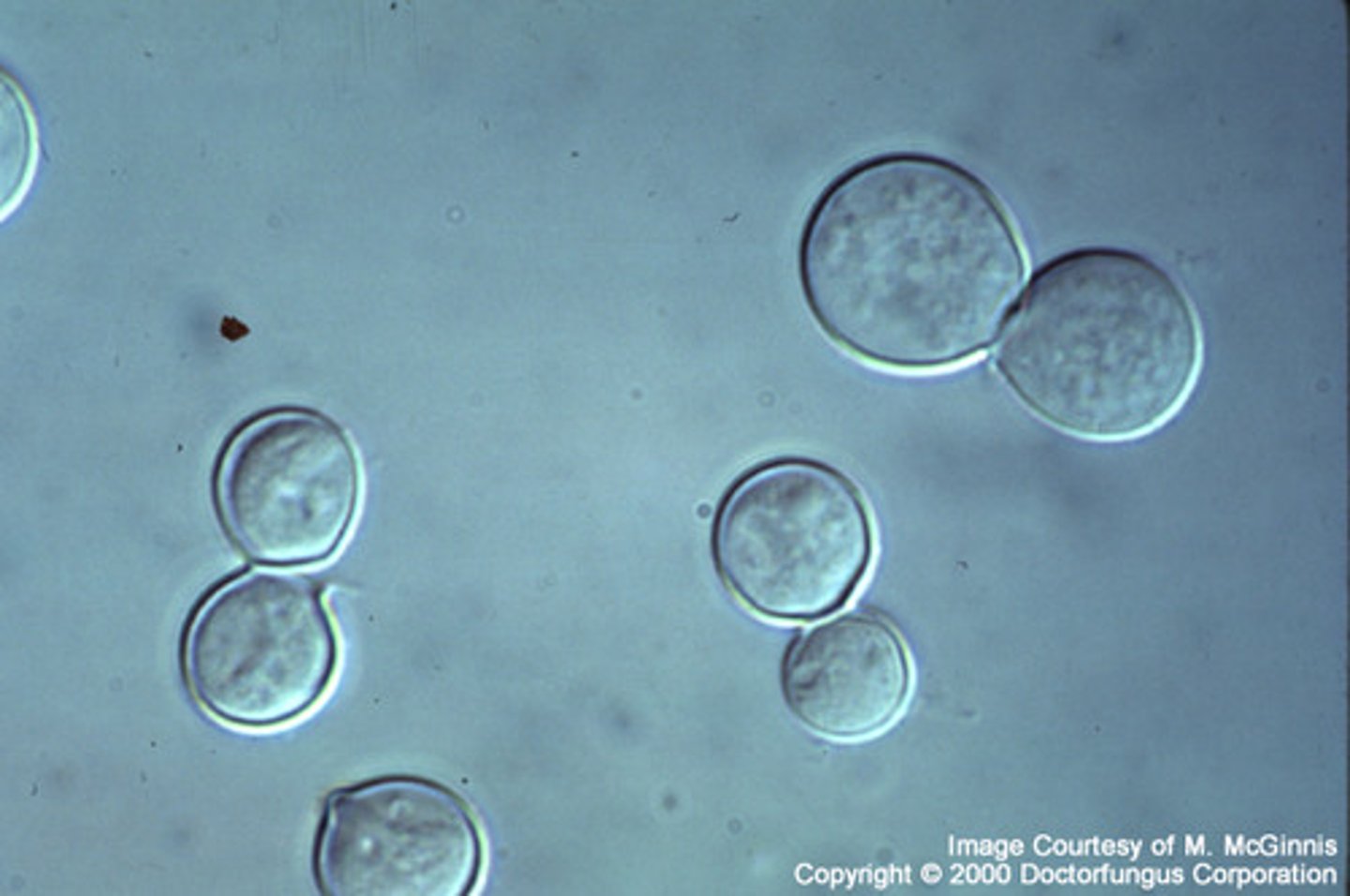
clinical significance of: penicillium marneffei
-AKA TALAROMYCES MARNEFFEI
-dimorphic
-common cause of systemic infections in immunocompromised patients
-small, elongated yeast-like cells seen in skin lesions
-mold form: colony produces a diffuse red pigment, microscopic morphology looks like other penicillium species (paintbrush, green colonies)
REPRODUCE BY FISSION NOT BY BUDDING!!!!!!!!!!!! can see a septation between 2 yeast cells from direct culture
SE ASIA = bamboo rat
-it's a pen looking organism but it IS THE ONLY DIMORPHIC PEN looking one!
*talaromyces marneffei
-used to be penicillium marneffei
-SE asia like Thailand
-AIDS-defining illness
-unclear mode of transmission but first found in bamboo rat
-inhalation of conidia is route of infection
-red pigment diffusable on culture which is different than penicilliums but looks like it under microscope
-could be found in blood
-yeast form divides by fission