OB Exam 4
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
Diabetes
Most common endocrine disorder associated with pregnancy
General pregnancy findings related to blood glucose
-Glucose levels in the fetus are directly proportional to maternal levels
-Glucose crosses placenta
-Insulin doesn't cross placenta
-Fetus produces its own insulin at 10 weeks gestation
First trimester findings with blood glucose
Rising estrogen and progesterone
-Stimulate insulin production in the pancreas (Promotes increased peripheral use of glucose->Decreased blood glucose, Those with IDDM are prone to hypoglycemia during the first trimester)
Second and third trimester findings with blood glucose
Diabetogenic effect
-Decreased tolerance to glucose
-Increased insulin resistance
-Decreased hepatic glycogen stores
-Increased hepatic production of glucose
Insulin resistance is increased
-Glucose-sparing mechanism that ensures an abundant supply of glucose for the fetus
-Maternal insulin requirements may double or quadruple by the end of the pregnancy
-Maternal insulin requirements gradually increase from 18-24 weeks to 36 weeks
Changes at birth with blood glucose
-Risk of hemorrhage (uterine distension)
-Delivery of the placenta prompts an abrupt decrease in levels of circulating hormones, cortisol and insulinase
-Maternal tissues go back to prepregnancy sensitivities to insulin
-Lactation uses maternal glucose (Mom's insulin requirements remain low)
-ACOG recommends assessing for CHO intolerance with 75-g 2 hour OGTT or fasting at 6-12 weeks postpartum
-Lifelong repeat screening at least every 3 years
Preexisting diabetes in pregnancy
-10% of pregnancies have preexisting DM
-Almost all of these are insulin dependent during pregnancy
-Perinatal mortality is 3 times higher for women with diabetes
Maternal risks/complications with preexisting diabetes
Poor glycemic control in early pregnancy
-Increased miscarriage
Poor glycemic control later in pregnancy
-Increased fetal macrosomia (20-50% of diabetic pregnancies have macrosomic infants, Increased c-section)
Higher rates of preeclampsia and eclampsia
PTL, IUGR, fetal distress, stillbirth, neonatal death
Hydramnios (Polyhydramnios)
-Over 2000 mL of fluid, 10 times more often in diabetic, Associated with PROM, Preterm labor, Postpartum hemorrhage
Increase risk of infection
Hypoglycemia can occur esp. in early pregnancy
-No ill effects on baby
Ketoacidosis
-Diabetic Ketoacidosis occurs at lower blood sugar levels
-DKA can cause fetal death, PTL
Tocolysis increases hyperglycemia
Metabolic acidosis can occur
Fetal/neonatal risks and complications with preexisting diabetes
Congenital malformations
-Most important cause of perinatal loss in pregestational diabetic pregnancy (30-50% of perinatal loss)
Insulin acts as a growth hormone
Macrosomia
-Weight greater than 4500 g, Fractured clavicle Liver or spleen laceration Brachial plexus injury Facial palsy Subdural hemorrhage
Increased risk for RDS
-Hyperglycemia and hyperinsulinemia (Delays pulmonary maturation in fetus)
Neonatal hypoglycemia often occurs within 30-60 minutes after birth
-Interruption of maternal glucose supply
gestational diabetes general
-Any degree of glucose intolerance with the onset or first recognition occurring during pregnancy
-4-7% of all pregnancies in the U.S.
Risk factors for gestational diabetes
Certain ethnic groups
History of GDM
Over age 25
Obesity
Family history of type 2 diabetes
Hx of macrosomic infant
Hydramnios
Unexplained stillbirth
Miscarriage
Hx of infant with congenital anomalies
screening for gestational diabetes
Initial visit if high risk
24-28 weeks is routine
GTT
-1 hour 50-g oral glucose (Lab draw if blood sugar is 130-140 it's a positive screen)
3 hour GTT
-100-g oral glucose
-Lab draw at 1,2, and 3 hours (Diagnosis if two or more values met or exceeded)
Alternative One step screening
-75-g test
Fetal surveillance with gestational diabetes
Twice weekly NST's starting at 32 weeks
Maternal/fetal risk factors with gestational diabetes
Increased risk of developing hypertensive disorders
9.8% if well controlled
18% not well controlled
Cesarean delivery (17-25%)
Type II later in life (up to 70%)
Increased occurrence in future pregnancies
hyperemesis gravidarum general
Excessive prolonged vomiting (10% of women have symptoms that persist throughout pregnancy)
-Concerned if: causing wt loss of 5%, Dehydration, Electrolyte imbalance, Ketosis, Acetonuria
hyperemesis gravidarum risk factors
Nulliparous
BMI(Less than 18.5 or Greater than 25)
Twins
Molar pregnancy
Psychological component
Younger maternal age
Low socioeconomic status
Asthma
Migraines
Preexisting diabetes
Psychiatric illness
Hyperthyroid disorders
Gastrointestinal disorders
Previous pregnancy complicated by hyperemesis
DECREASED RISK of spontaneous abortion
etiology of hyperemesis gravidarum
High estrogen or hCG (having a baby girl)
Transient hyperthyroidism
1.5 increase in female infants
Esophageal reflux
Reduced gastric motility
Decreased secretion of free HCL
Psychosocial
Hyperemesis Gravidarum Treatment
Determine severity
Assessment
-Physical and psychological
IV fluids
Antiemetics
Parenteral nutrition
Supplements
I & O
Hyperthyroidism in pregnancy
Rare in pregnancy (2-17 per 1000 births)
Caused by Graves disease (90-95% of the time)
SxS: Tachycardia, Fatigue, Heat intolerance, Emotional lability, Weight loss, Severe nausea and vomiting, Exophthalmos, Goiter, Altered lab levels
Treatment is meds
Hypothyroidism in pregnancy
Less common in pregnancy than hyperthyroidism (2-12 per 1000)
Associated with menstrual and fertility problems
Increased risk of miscarriage
SxS: Weight gain, Fatigue, Cold intolerance, Constipation, Cool/dry skin, Coarsened hair, Muscle weakness, Altered lab levels
pregnancy induced hypertension
Multi-organ, vasospastic process of reduced organ perfusion(hypoperfusion), activation of the coagulation cascade
Patho:
-Etiology->Origin unknown
-Is related to->Hypoperfusion, Vasospasm, Endothelial cell damage, Platelet aggregation
hypertensive disorders of pregnancy general
5-10% of pregnancies
Major cause of morbidity and mortality
Infant: uteroplacental insufficiency, preterm birth
Mother: renal failure, coagulopathy, cardiac or liver, abruption, seizure, stroke
50,000 maternal deaths annual in the world
-One woman every 7 minutes
>140/90
-HTN if either is elevated
-6 hours apart
-Positioning
-Appropriate sized cuff
Gestational HTN
HTN after 20 weeks if previously normotensive
No proteinuria, No other systemic findings
Systolic over 140, Diastolic over 90
Resolution
-Usually in first postpartum week
-Must resolve by 12 weeks to meet this classification
Preeclampsia
HTN and proteinuria after week 20 or in the early postpartum period in someone previously normotensive. If no proteinuria new onset HTN with new onset of any of these:
-Thrombocytopenia
-Renal insufficiency
-Impaired liver function
-Pulmonary edema
-Cerebral or visual symptoms
Eclampsia
Convulsions or coma not from other causes in a preeclamptic woman
No history of preexisting seizure-related pathology
1 in 2,000 -1 in 3,448 births
50% develop during the pregnancy
Can occur immediately postpartum
Chronic HTN in pregnancy
HTN in pregnant woman which was present prior to the pregnancy or persists longer than 12 weeks postpartum
superimposed preeclampsia
Women with chronic hypertension may acquire preeclampsia or eclampsia
Can be difficult to diagnose
risk factors for preeclampsia
Primigravida
First pregnancy at age extremes (<19 and >35)
Chronic hypertension
Pre-gestational diabetes
Nephropathy
Family History
Vascular and connective tissue disorders
Preexisting diabetes and/or thrombophilia
Maternal infection/inflammation (UTI, periodontal disease)
Obesity
Race
Multiple gestation
Fetal hydrops (baby has fluid where fluid should not be)
Hydatidiform
Preeclampsia in a previous pregnancy
Recurrence of preeclampsia
preeclampsia causes.....
Placental ischemia
-Endothelial cell dysfunction
Generalized vasospasm
-Poor tissue perfusion in organs (Increased peripheral resistance and BP, Increased endothelial cell permeability)
-Reduced kidney perfusion
-Plasma colloid osmotic pressure decreases
-Decreased liver perfusion
Neurologic complications
-Cerebral edema
-Cerebral hemorrhage
-Central nervous system irritability
Preeclampsia management/assessments
Low dose ASA (81 mg) may help
Accurate BP measurement
Assessment of edema (no longer included in definition of preeclampsia)
Assess for hyperactive reflexes
-DTR's
-Clonus
Proteinuria
-24 hour urine
-Little relationship between degree and outcome
Assess for
-Headache
-Epigastric pain
-RUQ pain
-Visual disturbances
Goals for Gestational HTN and Preeclampsia without severe features
Goals:
-Ensure maternal safety
-Manage outpatient if possible
-Monitor Labs
-Deliver healthy newborn as close to term as possible
-Monitor Fetus
-No bedrest
Goals/Intrapartum care or Gestational HTN and preeclampsia with severe features
Goals:
Ensure maternal safety
Formulate a plan for delivery
Expectant management
-For women less than 37 weeks
-Hospitalization (Antihypertensive meds, Corticosteroids)
Intrapartum Care:
-Continuous FHR and uterine contraction monitoring
-Bed rest with side rails up
-Darkened environment
-Assess for signs of abruption
preeclampsia interventions
Magnesium Sulfate
-Prevents and treats seizure
-IV piggyback on a pump
-Initial loading dose then maintenance
-Little effect on maternal BP
-Unclear mechanism of action
-High alert medications
Control BP
-Antihypertensive medications
preeclampsia postpartum care
Vital signs
DTR's
LOC
Magnesium sulfate x 24 hours
Severe features of preeclampsia
Progressive renal insufficiency
-Serum creatinine concentration >1.1mg/dL or a doubling of serum creatinine concentration in the absence of other renal disease
Pulmonary Edema
Visual disturbances
-flashing lights, auras, light sensitivity, blurry vision, spots in vision
Markedly elevated blood pressure
- > or equal to 160 over > or equal to 110 x 2 (Taken 4 hours apart on bedrest)
Platelet count <100,000
Elevated liver enzymes to twice normal
Severe persistent epigastric or RUQ pain unresponsive to meds
eclampsia causes
Cause of seizure is unknown, could be:
-Cerebral vasospasm
-Hemorrhage
-Ischemia
-Edema
-Platelet and fibrin clots that occlude cerebral vasculature
Eclampsia SxS
Premonitory signs
-Persistent headache and blurred vision
-Epigastric or RUQ pain
-Altered mental status
Seizures can appear without warning
Eclampsia Tx
Ensure patent airway and safety
Note time of onset and duration of seizure
Call for help (remain calm)
Remain at bedside
eclampsia complications
Periods of hypoxia in mother and fetus
Risk of aspiration
CVA
Cerebral edema
Anoxia
Coma
Maternal death
HELLP Syndrome
Hemolysis
Elevated
Liver enzymes
Lowered
Platelets
HELLP syndrome labs
CBC
CMP
Uric Acid - increases
BUN -increases
24 hour urine for protein and creatinine clearance
Serum creatinine - increase
pathophysiology of HELLP
RBC are destroyed as they travel through constricted vessels
-Hemolytic anemia
-RBC morph
-Reduced oxygen carrying capacity
-Elevated bilirubin and jaundice d/t hemolysis of RBC's
Elevated liver enzymes
-Vasospasm decreases blood flow to the liver
-Serum Liver enzymes become elevated
-Hepatic pain->RUQ, Epigastric, N & V, Tenderness to liver palpation
Platelets gather at site of damaged vascular endothelium causing platelet consumption and thrombocytopenia (possible DIC)
Platelet transfusions may be needed
implications/complications of HELLP
Eclampsia
Abruptio placenta
Disseminated intravascular coagulation
Acute renal failure
Hepatic failure
Pulmonary edema
Acute adult respiratory distress syndrome
Cerebral hemorrhage
Stroke
cerebral hemorrhage
Common cause of maternal death
Watch for
-Progressive decrease in patient's level of consciousness or stupor
-Complaints of flashes of light
Focal neurologic deficits (Nuchal rigidity, seizures, slurring of speech, local or unilateral motor weakness)
-New onset vomiting
-Sudden increase in BP (Sign of intracranial bleeding)
How the cardiac system is affected by HTN during pregnancy
HTN first sign
-d/t elevated systemic vascular resistance
-Left ventricle also working harder
-BP may vary d/t intermittent vasospasm
Edema least valid
Proteinuria may be late in onset
Fluid shifts from intravascular to extravascular
-d/t/ endothelial dysfunction and increased capillary permeability (Hypovolemia, Edema->Inclusive of pulmonary)
-hemoconcentration (Rise in hematocrit)
Leaking of albumin and other plasma proteins
-d/t endothelial dysfunction
-Causes decrease in colloid osmotic pressure (Higher risk for pulmonary edema)
How the renal system is affected by HTN during pregnancy
Endothelial cells in renal system are injured
Vasospasm
-Decreases in renal blood flow and GFR
Glomerular membrane is damaged from vasoconstriction
-Increases permeability to proteins
Severest forms of preeclampsia may have no edema
-Oliguria
-Intravascular fluid volume depletion
-Renal vasospasm
-Decreased cardiac output (d/t vasospasm and increased vascular resistance)
how postpartum is affected by HTN during pregnancy
Auto transfusion and extra vascular to intravascular fluid shifts
-Cause drop in COP (d/t dilution, 6-24 hours postpartum, Greatest risk for pulmonary edema, Lowest cardiac contractility)
How the CNS is affected by HTN during pregnancy
HA in pregnancy
-Question cerebral vasoconstriction (Leads to cerebral ischemia, Seizures, Hemorrhage)
Visual changes
-Retinal arteriolar spasms
-Petechial hemorrhages
-Retinal edema
-Retinal detachment (Can result in permanent blindness)
How the Hematologic system is affected by HTN during pregnancy
Hemoconcentration
Thrombocytopenia
-Platelet consumption
-Platelets adhere to damaged vessel walls
-Hepatic dysfunction contributes
Platelet count usually returns to normal within 72 hours postpartum
-More severe = longer recovery
-Count is o.k. but function may not be normal d/t meds (MgSO4, Aspirin, Steroid therapy)
Higher risk of DVT's ◦ Fibrinogen and blood coagulation
MgSO4 (magnesium sulfate)
Preferred drug for preventing and treating eclamptic seizure
Improves cerebral circulation and perfusion
Interferes with platelet aggregation
-Predisposes to bleeding
Changes serum osmolality
-May increase risk for pulmonary and cerebral edema
BP may decrease
-Relaxant effect on smooth muscle
-Use other medications for direct TX
Contraindicated in those with Myasthenia gravis (respiratory failure)
Contraindicated with heart block, myocardial insufficiency and possibly renal disease
Excreted via kidneys
-Oliguria or elevated serum creatinine levels may lead to high levels
Cardiac monitoring needed if given with IV labetalol
-Dysrhythmias and bradycardia
MgSO4 dosing
IV bolus 4-6 grams over 20-30 minutes
Maintenance infusion of 2-4 grams
-Usually is 2 grams per one hour
-Watch dose r/t renal ability
-Use cautiously with other meds that are CNS depressants (Additive effects/ potentiate->Barbiturates, Narcotics)
MgSO4 therapeutic levels
Normal 1.5-2
Therapeutic 4-7
ECG Changes 5-10
Loss of reflexes 8-12
Respiratory distress 15
Cardiac arrest 25
OVERLAP with therapeutic and ECG changes
MgSO4 side effects
Flushing
Lethargy
Nausea
Diaphoresis
Blurred vision
Hypocalcemia
Depressed reflexes
Depressed platelet aggregation
Cardiac dysrhythmias
Respiratory paralysis
Circulatory collapse
nursing interventions with MgSO4
I & O
Vitals
-Q 5-15" with loading dose
-Q 30-60 depending upon status
Hourly reflexes
Monitor for toxicity
Provide seizure precautions
Assess lung sounds
Antepartal use vs. postpartum use
Monitor for signs of toxicity
Monitor for worsening condition
-Shock
-Respiratory distress
-Arrhythmias
-S/S DIC
safety/antidote with MgSO4
Pre mixed solution, Standard strength, Label lines, Use smart pump, Remove medication completely if finished with it, Double check
Antidote is calcium gluconate or calcium chloride
-Have on unit!
protective changes in pregnancy against blood loss
Hypervolemia
Increased vascular resistance
Plasma volume increases
RBC mass increases
-Meets metabolic demands of mother and baby
-Protects against the potentially deleterious impairment in venous return caused by pressure of enlarging uterus
-Safeguards against blood loss at birth
Antepartal Hemorrhage
Leading cause of maternal death
-Highest incidence of maternal mortality (Ruptured ectopic, Abruption)
Miscarriage general
Pregnancy that ends as a result of natural causes before 20 weeks gestation
Fetal weight less than 500 g may be used as definition
10-20% of all confirmed pregnancies end in miscarriage
Early miscarriage
-Before 12 weeks gestation
-90% before 8 weeks
50% of early miscarriages
-Chromosomal abnormalities
causes of early miscarriage
Endocrine imbalance
-uncontrolled diabetes, hypothyroidism, etc.
Immunologic factors
-E.g. antiphospholipid antibody syndrome: maternal immune system attacks the placenta, leading to clot formation and pregnancy loss, etc.
Infections
-TORCHES, listeria, etc.
Systemic disorders
-Uncontrolled hypertension, renal disease, etc.
Genetic factors
-Chromosomal abnormality e.g. trisomy 16, etc.
late miscarriage
12-20 weeks
Usually maternal causes:
-Advanced maternal age and parity
-Chronic infection (PID, bacterial vaginosis, syphilis)
-Premature dilation of cervix
-Anomalies of reproductive tract
-Chronic debilitating disease (Diabetes, HTN, etc.)
-Inadequate nutrition
-Recreation drug use
prevention of miscarriage
Immunization
Early prenatal care
Treatment of pregnancy complications
Types of miscarriage
-Threatened: Spotting, os closed, mild uterine cramping present
-Inevitable: Moderate to heavy bleeding with open os, tissue may be present, mild to severe cramping
-Incomplete: Same symptoms as inevitable. Fetus is expelled and placenta is retained
-Complete: All fetal tissue is passed, cervix is closed, slight bleeding, mild uterine cramping
-Missed: Fetus has died but products are retained in utero. No bleeding or cramping. Os is closed
Habitual miscarriage
Recurrent spontaneous abortion
-3 or more consecutive pregnancy losses before 20 weeks gestation
Unclear etiology
-multifactorial
Increased risk for:
-preterm birth, previa, fetal anomalies
Septic miscarriage
Fever
Abdominal tenderness
Vaginal bleeding is malodorous
Requires surgical intervention
monitoring/management/home care for miscarriage
Monitoring
-Lab results :hCG
-Ultrasound
-HgB: Blood loss
-WBC: Infection
Management
-Depends upon the type of miscarriage
-Bed rest and supportive care
-D & C
-D & E (After 16 weeks)
-Outpatient vs. inpatient
-Misoprostol, pitocin, laminaria -
-Rhogam
-Control bleeding
-Psychologic care
Home care
-Discharge teaching
-Follow up
incompetent cervix general
Recurrent premature dilation of the cervix
Passive and painless dilation during the second trimester
Acquired or Congenital
Cervical Length
-Less than 25mm
Etiology of incompetent cervix
History of:
-Cervical lacerations
-Excessive dilation for curettage or biopsy
-DES from pt's mother: diethylstilbestrol->Synthetic estrogen to prevent miscarriage and preterm labor, Discontinued 1971->Reproductive tract anomalies
-Short cervix: Cervical funneling, Effacement of internal os
Management of incompetent cervix
Bed Rest
Hydration
Tocolysis
Cerclage
-Inserted at 10-14 weeks
-Removed at 37 weeks for vaginal delivery or c-section
Cerclage
Treatment of choice for cervical insufficiency
80-90% of pregnancies treated with cerclage result in live viable birth
Suture around the cervix to constrict the os
Abdominal cerclage->Suture (Mersilene tape) is placed at the junction of the lower uterine segment and the cervix
Risks: ROM, Preterm, Chorioamniotis
ectopic pregnancy general/risk factors
Gestational sac is implanted outside the uterine cavity
-fallopian tube (95% of cases), abdominal cavity, ovary, cervix
Responsible for 3% of maternal mortality, Leading pregnancy related cause of first trimester maternal mortality, Leading cause of infertility, Higher risk of future ectopic pregnancies
risk factors: Sexually Transmitted Infection(PID), Reversal of tubal ligation
Sxs of ectopic pregnancy
Missed period
Adnexal fullness and tenderness
Pain
-Unilateral, bilateral or diffuse: Blood irritates peritoneal cavity, Pain increases with rupture, Referred shoulder pain (Diaphragmatic irritation by blood in peritoneal cavity)
Bleeding (50-80% of the time)
Dx of ectopic pregnancy
Screen for if
-Abdominal pain
-Vaginal spotting or bleeding
-Positive pregnancy test
hCG
Ultrasound (transvaginal)
ectopic pregnancy tx
Surgical
Treatment of hypovolemia if applicable
Methotrexate
-Folic acid analog
-Destroys rapidly dividing cells
-Similar results to surgery
-High success, Low complications
-Good reproductive potential
molar pregnancy
Benign proliferative growth of the placental trophoblast in which the chorionic villi develop into edematous cystic transparent vesicles that hang in a grapelike cluster
1 in 1000 pregnancies in U.S.
Unknown etiology
-Ovular defect
-Nutritional deficiency
Risk factors
-Ovulation stimulation
-Early teens or over 40
-History of miscarriage
complete molar pregnancy
Fertilization of an egg with lost or inactivated nucleus
Resembles bunch of grapes
Fluid filled vesicles grow rapidly
-Uterus is bigger than expected
Usually has no fetus, placenta, amniotic membranes or fluid
Hemorrhage into uterine cavity and vaginal may occur
-No placenta to receive blood
20% progression towards choriocarcinoma
partial molar pregnancy
Two sperm fertilizes a normal ovum
Have embryonic or fetal parts and an amniotic sac
Congenital anomalies are usually present
6% malignant transformation
Sxs of molar pregnancy
Normal pregnancy symptoms
Vaginal bleeding later 95%
-Prune juice discharge or bright red
-Larger than expected uterus (25% have smaller)
management of molar pregnancy
Most abort spontaneously
Suction curettage
No induction
-Increased risk of embolization
Rhogam if needed
Ultrasound
hCG
Chemotherapy
placenta previa types
Four types
1)Total
2)Partial: Incomplete coverage
3)Marginal: An edge of placenta extends to the margin of internal os
4)Low lying: Lower uterine segment, but doesn't touch the os
placenta previa risk factors
History of previa
Hx of c-section
Endometrial scarring
Multiple gestation
Closely spaced pregnancies
Maternal age older than 35
African or Asian ethnicity
Smoking
Cocaine use
Multiparity
History of suction curettage
Living at higher altitude
placental previa SxS/Dx
70% painless vaginal bleeding
Suspect if bleeding after 24 weeks
Bright red bleeding
Pregnant women can lose 40% of their blood volume without signs of shock
Usually diagnosed with ultrasound before bleeding
vasa previa
Unprotected fetal vessels pass across the cervical os in front of the presenting part of the fetus
Vessels surrounded only by the amnion and are not covered with Wharton's jelly
Risk of laceration->Esp during ROM
Associated with higher fetal morbidity and mortality
Examiner may feel a pulsing vessel
Velamentous insertion of the cord
Rare
Associated with previa and multiple gestation
-Cord vessels branch at membranes and then into placenta
Rupture of membranes or traction
-Can tear the vessels->Fetus bleeds to death
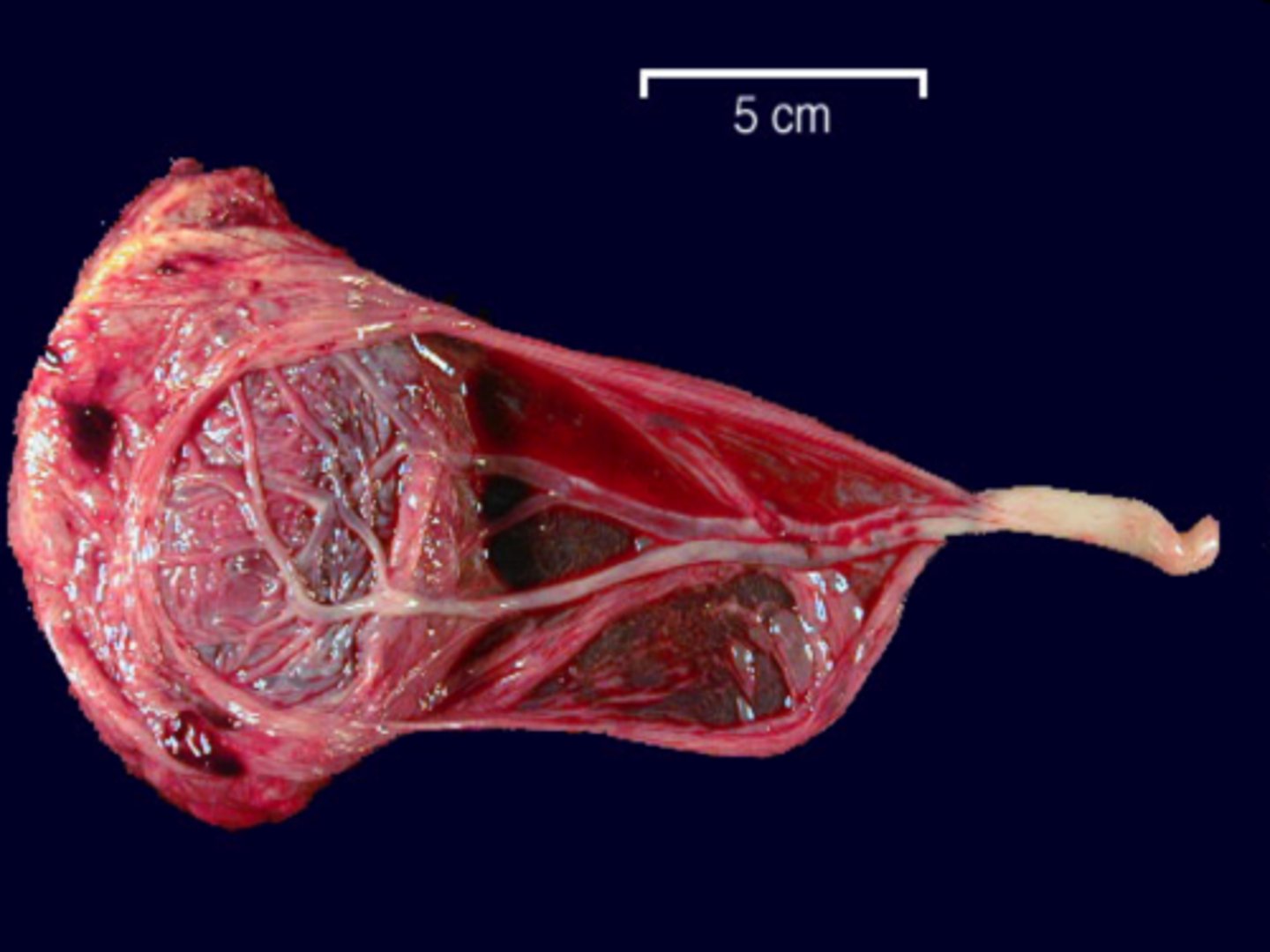
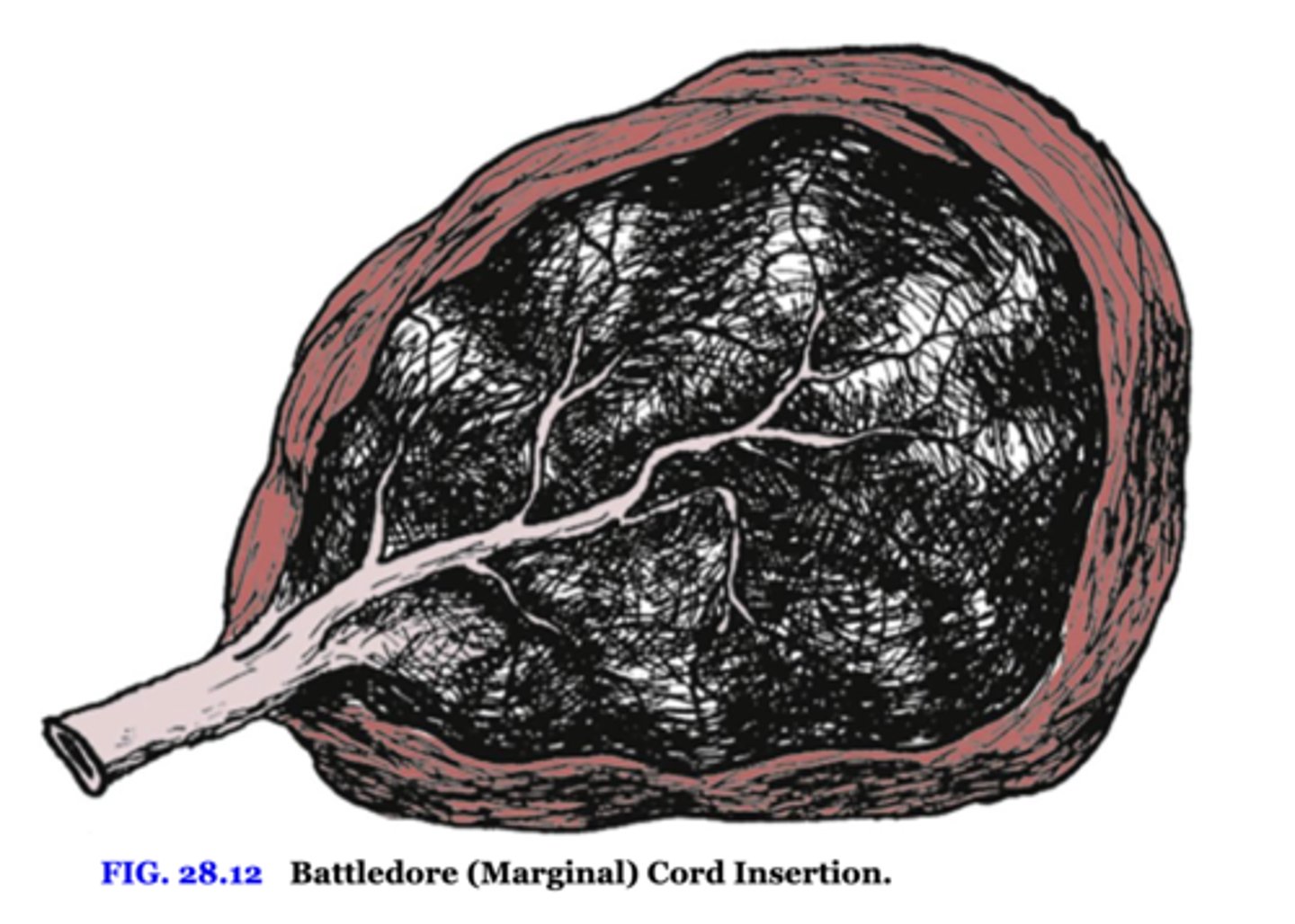
Battledore (marginal) insertion of the cord
cord inserts at edge of placenta
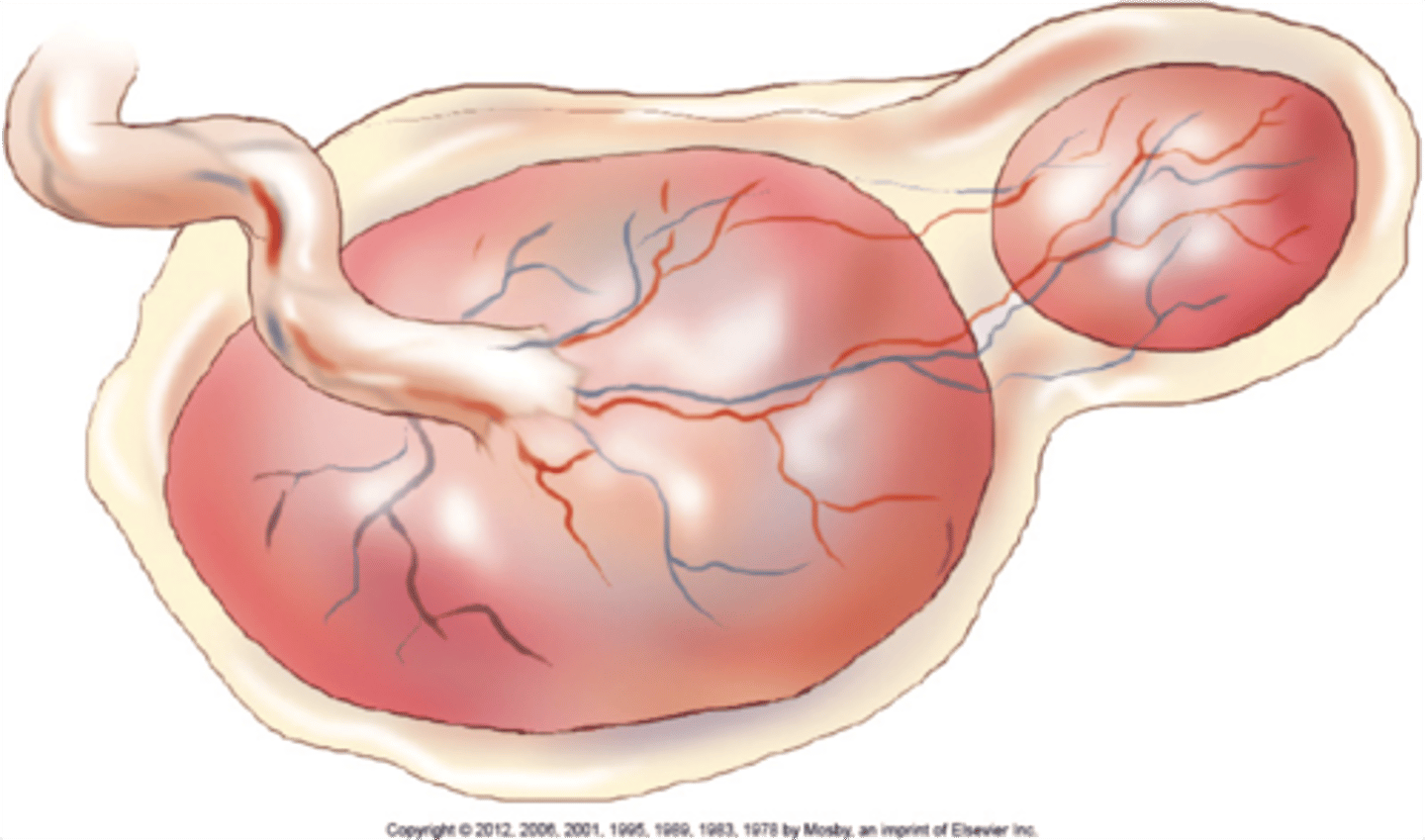
succenturiate placenta
Lobed placenta
Retained fragments likely
Placental abruption and risk factors
Premature separation of placenta
Risk Factors
-Maternal hypertension
-Cocaine use (Causing hypertension)
-Abdominal trauma (Motor Vehicle Accident, Abuse)
-History of abruption (25% recurrence rate)
-Smoking
-Preterm Pre-labor Rupture Of Membranes
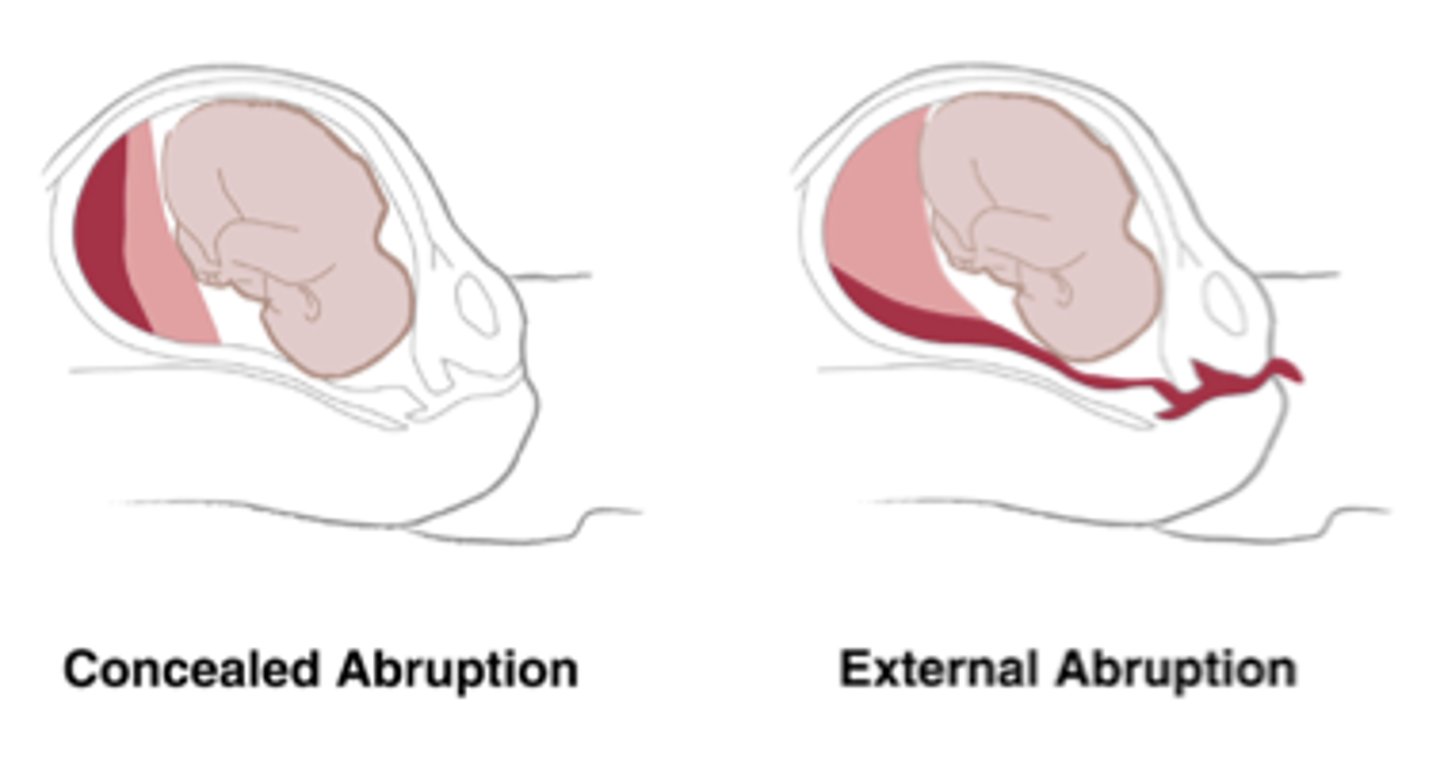
SxS of placental abruption
Vaginal bleeding
Uterine tenderness
Contractions
s/s hypovolemia
Board like abdomen
(couvelaire uterus)
Placental abruption morbidity/mortality
Mortality rate
-1%
-Leading cause of maternal death
Prognosis depends upon
-degree of placental detachment
-Blood loss
-DIC
-Time between placental detachment and birth
Perinatal mortality rates (15-30%)
Mortality
-fetal hypoxia
-preterm birth
-status as SGA
Morbidity
-neurologic defects
Non reassuring FHT's
-60% of the time (Decreased variability, Late decels)
Hyper stim and increased resting tone may be noted
Abnormal clotting factors
placental abruption Tx
Expectant Management
Delivery: Vaginal or Cesarean
DIC def/risk factors
Consumptive coagulapathy
-Diffused clotting
-Consumes clotting factors
Blood cells are destroyed as they pass through fibrin-choked vessels
Always a secondary diagnosis
Risk factors:
-Abruption
-Retained dead fetus
-Amniotic fluid embolus
-Severe preeclampsia
-HELLP syndrome
-Gram-negative sepsis
perinatal loss/grief
Ectopic pregnancy or fetal death, miscarriage and induced abortion
-Hidden or silent
Stillbirth
-Usually later term
-Parents are planning on welcoming a healthy newborn (End of life decisions)
Difficult with perinatal loss
-Society belief that there are no barriers to getting pregnant
-Expectation that pregnancy will result in a healthy live baby
-Society minimizes perinatal loss
-Lacks understanding of associated pain (May not get the support that they need)
Lack of identifiable cause
-Complicates grief
-Women feel responsible (Repeated loss)
Parental Grief Box
Acute distress
-Shock, numbness, intense crying, and depression
Intense Grief
-Loneliness, emptiness, and yearning, guilt, anger, resentment, bitterness, irritability, fear and anxiety (esp. about getting pregnant again)
-Disorganization, difficulties with cognitive processing, sadness and depression, and physical symptoms
Reorganization
-Search for meaning, reduction of distress, reentering normal life activities with more enthusiasm, can make future plans, including another pregnancy
family grief of baby
Grandparents
-Sadness for their own child as well
-Survivor guilt (Infant deal is out of order)
Siblings
-Depends upon age and stage (Understanding, response and grief)
actualizing the loss of a baby
Tell honestly
Use the term miscarriage, dead and died
-Avoid (Lost or gone)
Let them recount, and listen
See, hold, name
-Acquaint and separate
-Offers closure
important decision making with infant loss
Autopsy
Organ donation
Baptism
Burial
Cremation
what/what not to say with infant loss
What to say:
-I'm sad for you
-How are you doing with all of this
-This must be hard for you
-What can I do for you
-I'm sorry
-I'm here and I want to listen
What not to say:
-God had a purpose for her
-Be thankful you have another child
-The living must go on
-I know how you feel
-It's God Will
-You have to keep on going for her sake
-You're young. You can have another
-We'll see you back here next year and you'll be happier
-Now you have an angel in heaven
-This happened for the best
-Better for this to happen now, before you knew the baby
-There was something wrong with the baby anyway
perinatal mood disorders
Set of disorders that can occur anytime during pregnancy as well as in the first year postpartum and can include:
-Depression (postpartum depression)
-Bipolar disorder
-Postpartum psychosis
1 in 7 women affected by perinatal mood disorders
Postpartum depression
-Negative effects on child development
Maternal suicide
-20% of postpartum deaths in depressed women
Dx of perinatal mood disorders
Rule out:
-Thyroid
-Anemia
Signs and Symptoms of major depression
Edinburgh Postnatal Depression Scale
perinatal mood disorders care management/nursing interventions
Care management
-Antidepressants
-Cognitive-behavioral Therapy or interpersonal psychotherapy
nursing interventions
-Educate (Depression as an illness, Plan of care, Medications)
-Discuss alternative treatments respect refusal of meds
Dx of depression
5 of the following nearly every day:
-Depressed mood
-Spontaneous crying
-Diminished interest in all activities
-Insomnia or hypersomnia
-Weight changes
-Psychomotor retardation or agitation
-Fatigue or loss of energy
-Feelings of worthlessness or inappropriate guilt
-Diminished ability to concentrate
-Suicidal ideation
risk factors for depression during pregnancy
Prior history
-Self
-Family
Lack of social support
Stressful life events
Partner discord
History of PMS