Ant Seg L1: DISORDERS AND SURGERIES OF THE ORBIT
1/137
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
138 Terms
what are the cranial sutures?
coronal, lambdoidal, metopic, sagittal
What is Craniosynostosis?
the premature fusion of cranial vault suture
According to Virchow's Law, the premature fusion of the cranial vault suture inhibits normal skull growth ____________ to the fused suture, and a compensatory growth occurs at the open sutures.
perpendicular
According to Virchow's Law, the general direction of growth after the craniosynostosis is __________ to the fused suture.
parallel
In Craniosynostosis, _________________ can be elevated due to brain growth in a confined space
Intracranial pressure
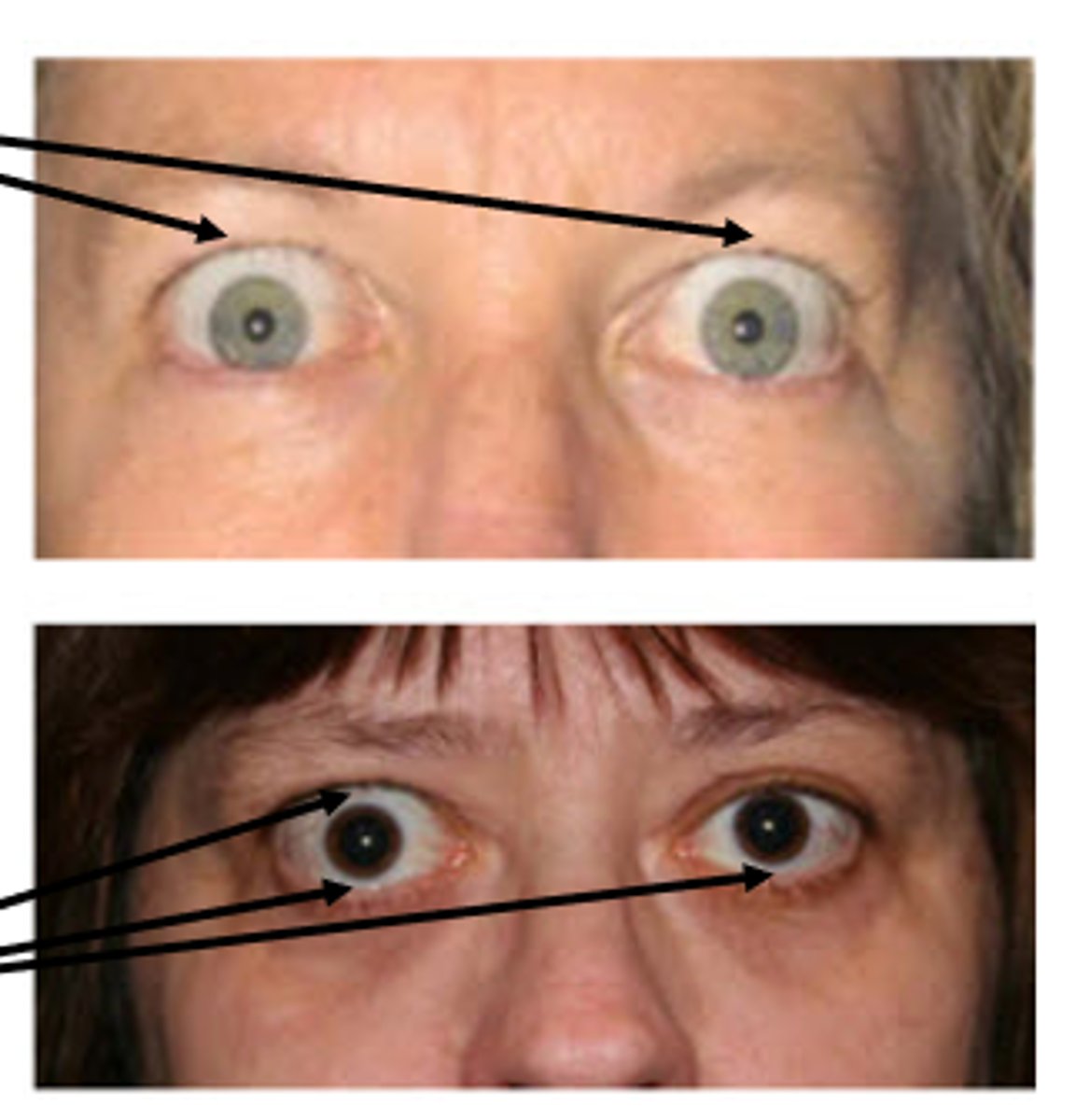
what are the Ocular manifestations/sequelae of Craniosynostosis?
•Proptosis- protrusion of the eyes
•Papilledema- bilateral optic nerve head swelling due to increased intracranial pressure
•Optic nerve head atrophy
•EOM paresis
what are the Non-Syndromic Craniosynostosis?
1. Scaphelocephaly
2. Trigonocephaly
3. Brachycephaly
4. Oxycephaly
5. Positional Plagiocephaly (not a true Craniosynostosis)
Scaphelocephaly is premature fusion of the ____________
sagittal suture
Scaphelocephaly results in __________ elongation of the cranium
anterior-posterior
scaphelocephaly resembles ___________
an inverted boat or a football-head
Trigonocephaly is premature fusion of the ____________
metopic suture
__________ results in a high retreating forhead, V-shaped, (triangle shaped head)
Trigonocephaly
Brachycephaly is premature fusion of:
both coronal sutures
Can have fusion of one coronal suture (unicoronal craniosynostosis)
____________ results in shortened front-to-back diameter of the skull, head disproportionately wide.
Brachycephaly
Oxycephaly is premature fusion of the:
coronal and sagittal and/or lambdoid sutures
___________ results in tower skull or "high-head" syndrome
Oxycephaly
what is the most common cause of misshapen head during infancy?
Positional Plagiocephaly
what causes Positional Plagiocephaly?
Back of the head is often flatter on one side due to position in womb during pregnancy
•More common in twins, triplets, etc.
•Infants have poor control of head and often will rest on flatter side
what is the treatment for Positional Plagiocephaly?
Treatment: none (sometimes helmets)the
Once infant has better control of their head, the deformity decreases naturally
what bones make up the roof of the orbit?
1. Lesser wing of the Sphenoid
2. Frontal
"Front-less"
what bones make up the floor of the orbit?
1. Maxillary
2. Palatine
3. Zygomatic
"My pal Z"
what bones make up the medial wall of the orbit?
1. Sphenoid
2. Lacrimal
3. Ethmoid
4. Maxillary
"SLEM"
•The ____________________________________ is weak- may be involved in a blow out fracture
posteromedial portion of the maxillary bone
The floor of the orbit is also the roof of the ____________ sinus
maxillary
The _______________________________________ is the thinnest bone and can erode in ethmoid sinusitis infections
lamina papyracea of the ethmoid
what bones make up the lateral wall of the orbit?
1. Greater wing of the sphenoid
2. Zygomatic
"Greater-Z"
The ___________ half of the globe is vulnerable to trauma because the lateral wall only protects the ___________ half of the the globe.
anterior, posterior
what are the 5 Syndromic Craniosynostosis?
1. Saethre-Chotzen syndrome
2. Muenke syndrome
3. Apert syndrome
4. Pfeiffer syndrome
5. Crouzon syndrome
"Snack-choosing monkey apes prefer croutons."
what is the Craniosynostosis of apert syndrome?
brachycephaly and/or oxycephaly
what is the inheritance pattern of the 5 Syndromic Craniosynostosis?
Autosomal dominant inheritance
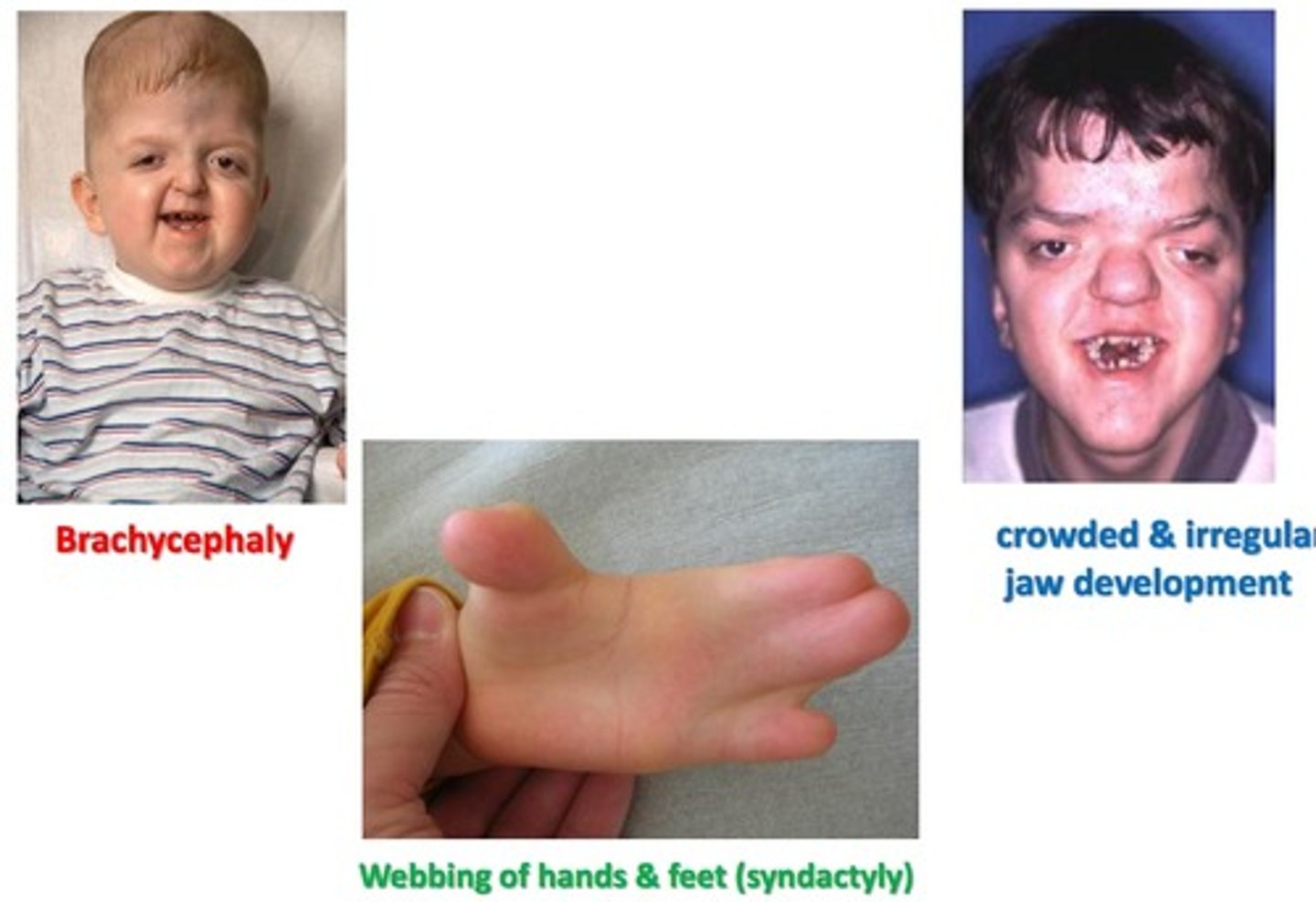
what is the presentation of apert syndrome?
Flat, elongated forehead
Proptosis
Underdeveloped midface
Fusion of the digits (2-3 fingers per hand)
what causes Crouzon Syndrome?
Premature closure of cranial base sutures, orbit and maxillary complex
Usually brachycephaly
what is the presentation of Crouzon Syndrome?
•Wide set proptotic eyes, beaked nose, underdeveloped jaw
•Dental issues, possible cleft lip and palate
•No associated hand/feet anomalies3

what is the cause of Muenke syndrome?
•Premature closure of coronal sutures (brachycephaly)
what is the presentation of muenke syndrome?
•Abnormally shaped head
•Wide set eyes
•Flattened cheek bones
•Mild hand/feet abnormalities
•Most have normal intellect

what is the presentation of pfeiffer syndrome?
•Abnormally shaped head
•Wide set eyes
•Beaked nose
•Underdeveloped upper jaw
•Thumbs and big toe point away from other digits, may have webbing or fusion
Hearing issues

what is the cause of Saethre-Chotzen syndrome?
•Premature closure of coronal sutures (brachycephaly)
what is the presentation of Saethre-Chotzen Syndrome?
•Abnormally shaped head
•Low frontal hairline
•Ptosis
•Wide spaced eyes
•Broad nasal bridge
•Facial asymmetry
•Small ears
•Fusion of 2nd and 3rd fingers
•Usually normal intelligence

Most, if not all Craniosynostosis present with ______________.
proptosis
Proptosis causes increased exposure to the environment which can desiccate the ocular surface/cornea. How should we treat this?
•Artificial tears
•Preservative-free if dosing more than 4x a day (QID)
•Gel or ointment (ung) at bedtime (QHS)
•Possible lid taping QHS
what innervates the eyelid skin?
CNV-sensory supplied by V1 upper eyelid, V2 lower eyelids and motor to muscles of mastication
what innervates the Orbicular oculi (orbital and palpebral portions)?
CNVII- motor to muscles of facial expression, taste to anterior 2/3 of tongue and lacrimation
what innervates the muscle of Mueller?
sympathetics
what innervates the levator?
CN III
what does the Lateral palpebral artery branch from?
lacrimal artery
what does the medial palpebral artery branch from?
Ophthalmic artery
what do the eyelid veins drain into?
palpebral and ophthalmic veins
ALL RECTI MUSCLES ORIGINATE AT _____________
COMMON TENDONOUS RING
mnemonic for orbital apex
LF STUNALI
L acrimal nerve (V1)
F rontal nerve (V1)
S uperior ophthalmic vein
T rochlear nerve (CNIV)
U pper division of CNIII (SR,
Levator)
N asociliary nerve (V1)
A bducens nerve (CNVI)
L ower divison of CNIII
I nferior ophthalmic vein
what is the presentation for orbital cellulitis?
•Eyelid edema, erythema, warmth and tenderness
•Conjunctival injection, chemosis
•Proptosis
•Febrile and malaise
•Restricted extraocular motilities/pain
with eye movement
what are the symptoms for orbital cellulitis?
•Red eye
•Pain
•Blurred vision
•Double vision
•Eyelid swelling
•Nasal congestion/discharge
•Sinus headache, congestion, pressure
•Tooth pain
•Infra/supraorbital pain
what is the etiology of orbital cellulitis?
•Direct extension from a paranasal sinus infection (especially ethmoiditis)
•Focal periorbital infection: Dacryoadenitis, Dacryocystitis
•Dental infections
•Sequela of orbital trauma
•Sequela of orbital surgery or paranasal sinus surgery
•Vascular extension (seeding from a systemic bacteremia)
•Secondary to orbital venous stasis and inflammation from a septic cavernous sinus thrombosis
•Infection by Staphylococcus (adults), Streptococcus (adults), H. influenzae (children)
•Fungal infection in immunocompromised patients (diabetics, HIV, chemotherapy patients): Mucormycosis/zygomycosis, Aspergillus
what is the clinical examination for orbital cellulitis?
•Ask about trauma, surgeries, ear/nose/throat infections, tooth pain/abscess, stiff neck or mental changes
•Palpation of the affected lid assessing for warmth and tenderness
•Visual acuity: look for reduced in affected eye
•APD: Indicates compressive optic neuropathy
•Extraocular motilities/restrictions
•Proptosis: Resistance to retropulsion
•Conjunctival congestion/chemosis
•Dilated fundus exam: swollen optic nerve head
•Check for febrile status
what is the treatment for Orbital Cellulitis?
Emergency department will perform a CT scan of the orbits and paranasal sinuses (axial and coronal with contrast) to confirm diagnosis
Admit/refer to ED/hospital for IV antibiotics stat
(Concern for infection of the CNS and meningitis- refer immediately to emergency department)
what are the 4 types of Idiopathic Orbital Inflammation (IOI)?
•Dacryoadenitis
•Myositis
•Dacryoadenitis + Myositis
•Orbital Apex syndrome
IOI is a diagnosis of _________
exclusion
what are the differentials for IOI
•Thyroid related ophthalmopathy
•Orbital cellulitis
•Orbital tumor
•Lacrimal gland tumor
•Orbital vasculitis
•Trauma
•Cavernous sinus thrombosis
•Cranial nerve palsy
•Herpes Zoster Ophthalmicus
what is the presentation of IOI?
•Usually unilateral, although bilateral more common in children
•Marked tenderness of the involved region
•Lid edema, erythema
•Lacrimal gland enlargement (dacryoadenitis)
•Limitation of and pain with EOM (myositis)
•Proptosis
•Decreased orbital retropulsion
•Conjunctival chemosis
•Reduced corneal sensation
•Increased IOP
what are the symptoms of IOI?
•Acute onset of orbital pain
•Decreased vision
•Binocular diplopia
•Red eye
•Headaches
•Fever, nausea, vomiting
what is the Clinical Examination for IOI?
•Ask about trauma, surgeries, ear/nose/throat infections, tooth pain/abscess, stiff neck or mental changes
•Palpation of the affected lid assessing for warmth and tenderness
•May need to open eye to assess for:
•Visual acuity: Reduced in affected eye
•(+) APD: Indicates compressive optic neuropathy
•Extraocular motilities/restrictions
•Proptosis: Resistance to retropulsion
•Conjunctival congestion/chemosis
•Dilated fundus exam: Swollen optic nerve head
•Check for febrile status
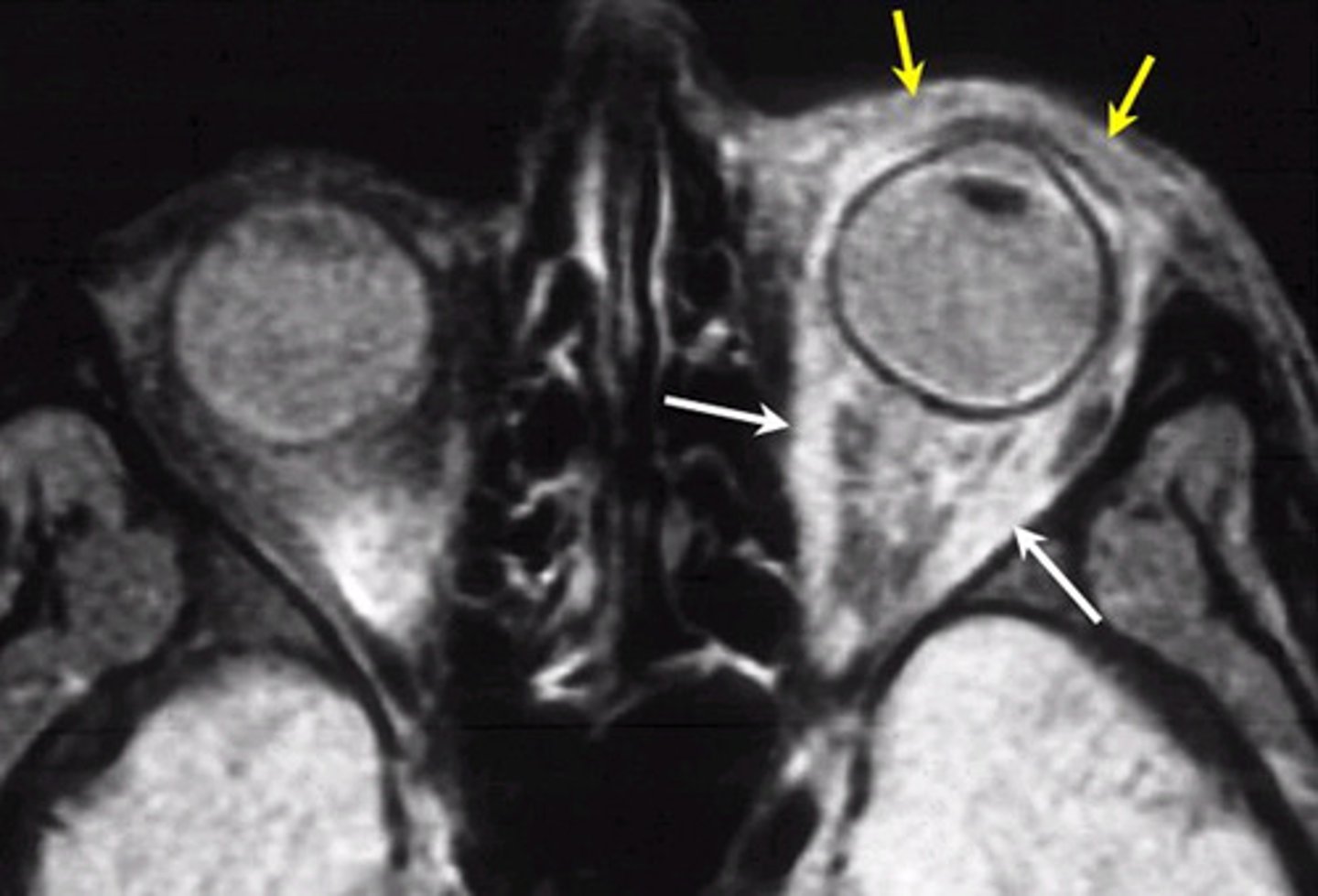
CT of Dacryoadenitis and myositis
the tendons & extraocular muscles are enlarged

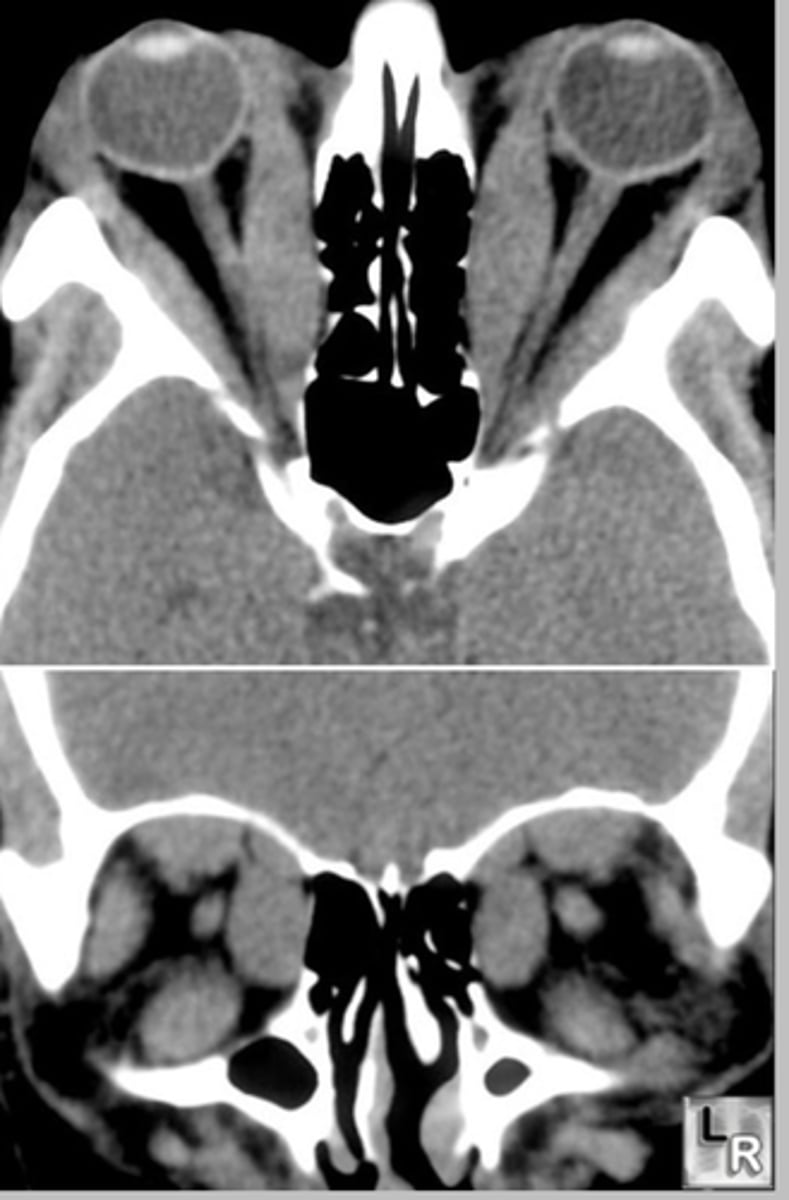
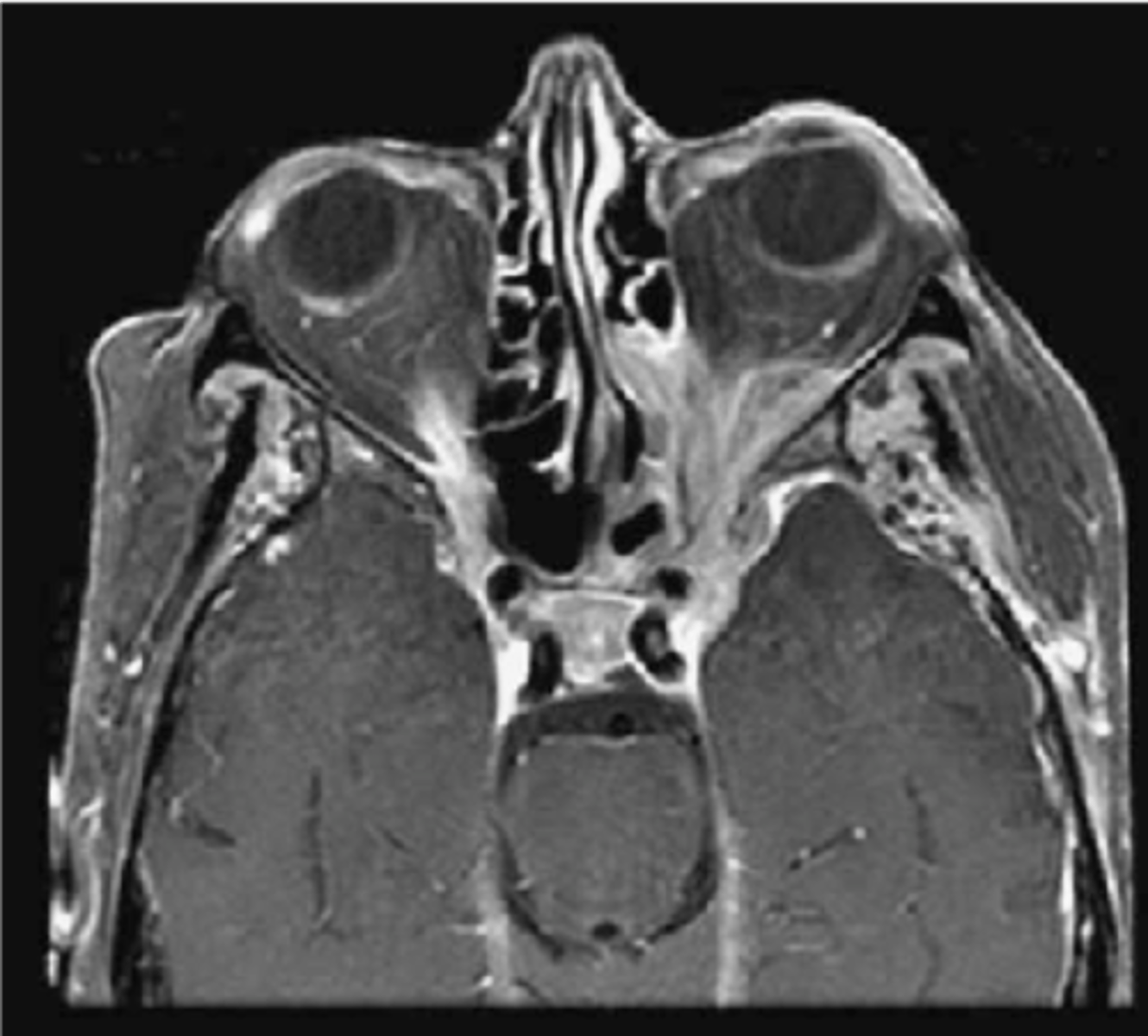
CT of of Thyroid Ophthalmopathy
only the muscle belly is enlarged.(coke bottle appearance of EOM)
what is the treatment/management of IOI?
Admit/refer to ED/hospital for orbital CT scan STAT
•ED to initiate systemic steroids once all other conditions have been ruled out
•ED will run hematology to rule out presence of vasculitis in adults •(i.e. Wegner's granulomatosis, Polyarteritis nodosa)
what is the presentation of orbital apex syndrome?
•Unilateral vision loss with ophthalmoplegia involving multiple cranial nerves
•Vision loss is due to CN II being affected. Optic atrophy can occur weeks to months after initial presentation if not remedied
•Ophthalmoplegia due to involvement of: CN III, IV, VI
•Periorbital facial pain and forehead hypoesthesia due to CNV1 involvement: Decreased corneal sensitivity
•Mydriasis and ptosis: Due to CN III involvement
•Proptosis
•Injection/chemosis
what are the symptoms of orbital apex syndrome?
•Poor vision in affected eye
•Binocular diplopia
•Orbital pain
what is the etiology of orbital apex syndrome?
•Inflammatory
•Infectious
•Neoplastic
•Iatrogenic/Traumatic
•Vasculopathic
what is the Differential Diagnosis of orbital apex syndrome?
Cavernous sinus syndromes- no optic nerve involvement with these conditions
what is the examination of orbital apex syndrome?
•Ask about trauma, surgeries, ear/nose/throat infections, tooth pain/abscess, stiff neck or mental changes
•Palpation of the affected lid assessing for warmth and tenderness
•May need to open eye to assess for:
•Visual acuity:Reduced in affected eye
•(+) APD: Indicates CN II involvement
•Extraocular ophthalmoplegia
•Proptosis: Resistance to retropulsion
•Conjunctival congestion/chemosis
•Dilated fundus exam: Swollen optic nerve head
•Check for febrile status
what is the Treatment/Management: of orbital apex syndrome?
•Admit/refer to ED/hospital for orbital CT and MRI scan STAT
•ED to initiate systemic steroids once all other conditions have been ruled out
Orbital Apex Syndrome CT appearance
expanding lesions at the orbital apex
What is the presentation of orbital varix?
•Intermittent proptosis of one or both eyes which is non-pulsatile and NOT associated with a bruit
•Proptosis is precipitated by valsalva manuever or compression of the jugular veins
What are the symptoms of orbital varix?
•Intermittent bulging of eyes on command or with valsalva maneuver
what is the Differential Diagnosis of orbital varix?
•Carotid cavernous fistula
what is the Diagnosis, Treatment, Management of orbital varix?
•X-ray of orbit to rule out mass
•Patient education
What is the presentation of carotid cavernous fistula?
•Typically, unilateral presentation
•Red eye
•Chemosis and injection from backup of venous blood
•Pulsatile proptosis: beating at rhythm of heart
•Orbital bruit
•Decreased visual acuity
What are the symptoms of carotid cavernous fistula?
•Pulsations of the globe
•Irritated red eye
•Eyelid edema
What is the differential diagnosis of carotid cavernous fistula?
•Orbital varix
what type of fistula is Characterized by direct connection of internal carotid artery to the cavernous sinus?
"High-flow" or direct fistula
What type of fistula is 80% of lesions and often secondary to closed head trauma?
"High-flow" or direct fistula
What type of fistula is characterized by a connection of the sinus with any of the meningeal branches of the internal carotid?
"Low-flow" or dural fistula
What type of fistula is often associated with systemic disease (i.e. HTN, connective tissue disorders, atherosclerosis)?
"Low-flow" or dural fistula
what is the Diagnosis, Treatment, Management of carotid cavernous fistula?
•Orbital CT or MRI: enlargement of the superior ophthalmic vein
•Arteriography usually required to identify fistula
•High-flow fistula are closed by surgical repair of the lesion, if possible or embolization with balloon occlusion
•Low-flow fistulas are closed by endovascular balloon occlusion, if possible. May have conservative monitoring with low-flow fistula as some spontaneously resolve.
what Palliative Care is Provided by the Optometrist for carotid cavernous fistula?
•Appropriate identification of abnormality and timed referral
•Patient will need to be referred for emergent imaging and initiation of systemic antibiotics/steroids/immunomodulators
•Proptosis: Prescribe heavy lubrication to the eyes to prevent exposure keratitis
•Gel-based artificial tears (preservative-free) q1hr- PRN
•Ointment with lid-taping QHS
•Elevated IOP: Prescribe topical anti-hypertensive agent (i.e. Alphagan 1gtt TID in affected eye)
what is the MOST COMMON CAUSE of hypothyroidism?
Hashimoto's Thyroiditis- autoimmune-mediated attack of the thyroid gland, Iodine-deficiency in developing countries
what are the SIGNS/SYMPTOMS of hypothyroidism?
cold intolerance, fatigue, weight gain, dry skin, course hair
what is the DIAGNOSTIC TESTING for hypothyroidism?
Increased TSH, decreased T4 , T3, Anti-thyroid antibodies
what is the MOST COMMON CAUSE of hyperthyroidism?
Grave's disease-autoimmune disease of TSH autoantibodies constantly stimulating thyroid gland
•FEMALE predilection
what are the SIGNS/SYMPTOMS of hyperthyroidism?
heart palpations, weight loss, heat intolerance, hair loss
what is the DIAGNOSTIC TESTING for hyperthyroidism?
Decreased TSH, increased T4 , T3, Anti-thyroid antibodies
what are other names for TED?
thyroid ophthalmopathy, thyroid-associated orbitopathy
what is the most common demographic for TED?
middle aged women
•4-8:1, female to male gender ratio
•When males develop TED, more severe form
what is the Most common cause of unilateral or bilateral proptosis in adults?
TED
TED has a Severe presentation in ________.
smokers
what is the pathophysiology of TED?
•Autoimmune process affecting fibroblasts of the orbit found on orbital fat and EOMs
•Orbital fibroblasts trigger inflammation in the interstitial spaces of the EOM and connective tissue of the orbit
•Stimulation of T and B lymphocytes
•Production of pro-inflammatory cytokines
•Accumulation of glycoaminoglycans (GAGs)
orbital fat expansion, EOM enlargement, proptosis/diplopia
Mnemonic for the progression of the TED: NOSPECS
•N- No ocular signs/symptoms
•O- Only signs, no symptoms (lids)
•S- Soft tissue swelling
•P- Proptosis
•E- EOM involvement
•C- Corneal involvement
•S- Sight loss from optic nerve head involvement
what are the eyelid disorders of TED?
•Eyelid retraction
•Eyelid edema
•Reduced blinking
•Lid lag (Von Graefe's sign)
what are the ocular surface disorders of TED?
•Superficial keratopathy
•Conjunctival injection
•Superior limbic keratoconjuncitivitis (SLK)
•Proptosis
what are the EOM disorders of TED?
•EOM restriction
•Resistance to retropulsion of the globe
what are the ONH disorders of TED?
•Decreased visual acuity
•Decrease color vision
•Positive RAPD
•Visual field defects
what is Dalrymples' sign?
retraction of of upper lid on primary gaze