General Sonography II Final Exam
1/147
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
148 Terms
Atherosclerosis → buildup of plaque overtime within artery walls
clinical hx: male, long term smoker, alcohol abuser, DM, cholesterol (LDL), HTN
s/sx: often asymptomatic, can cause chest pain, weakness, leg pain, high BP depending on what arteries are affected
2D US presentation: starts as hypoechoic plaque within lumen → plaque turns echogenic w/ posterior shadowing and gives artery wall irregular lobulated shape
color doppler: twinkle artifact from calcification
DDX: arteriosclerosis (stiff walls, not obstructive), vasculitis (diffuse wall thickening from inflammation, not plaque)
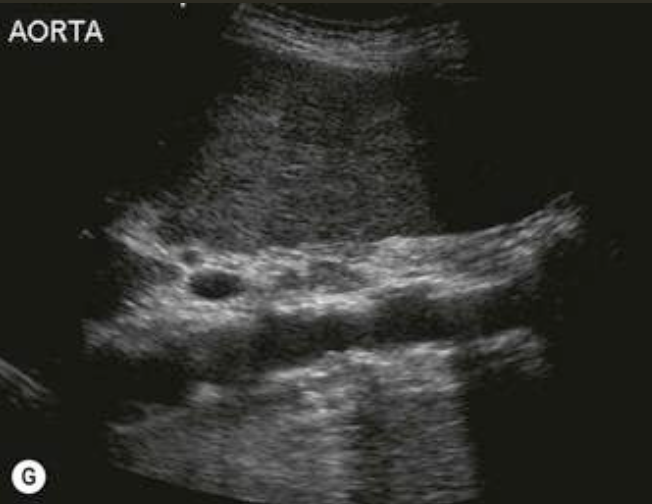
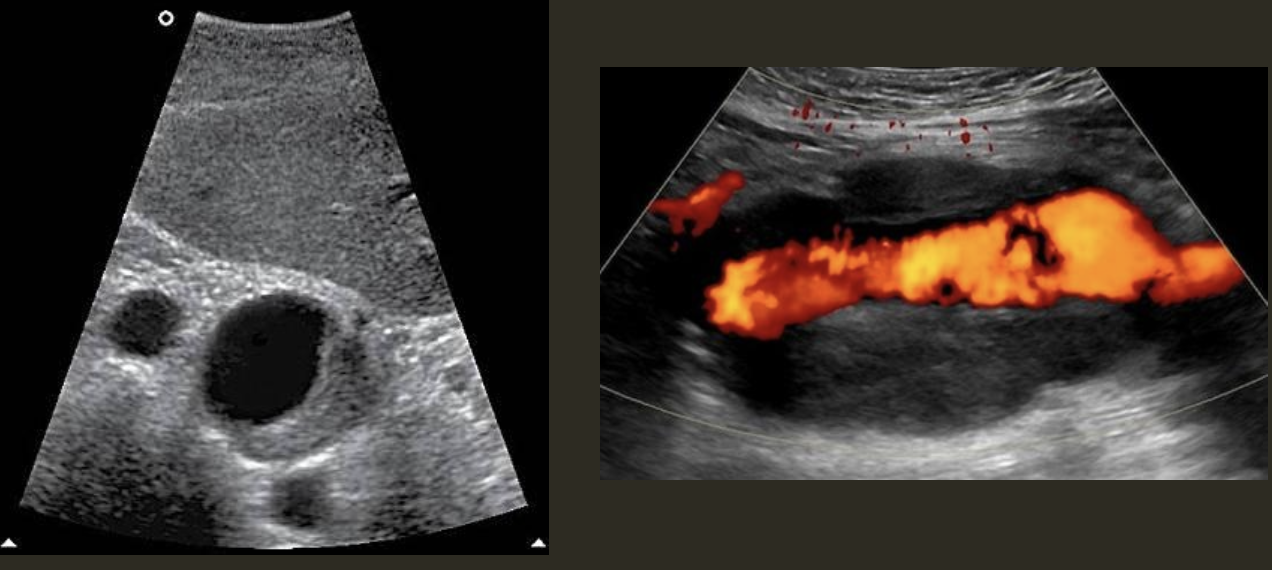
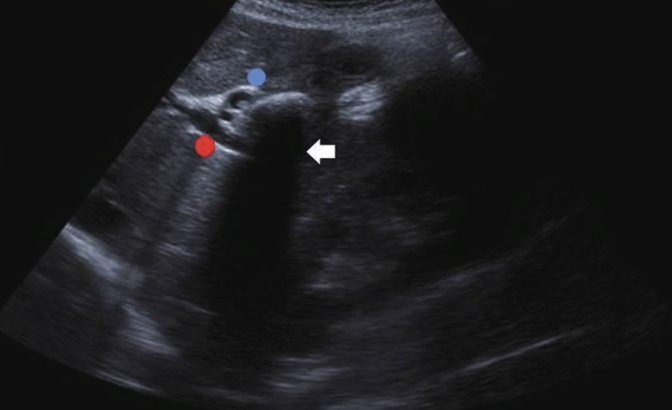
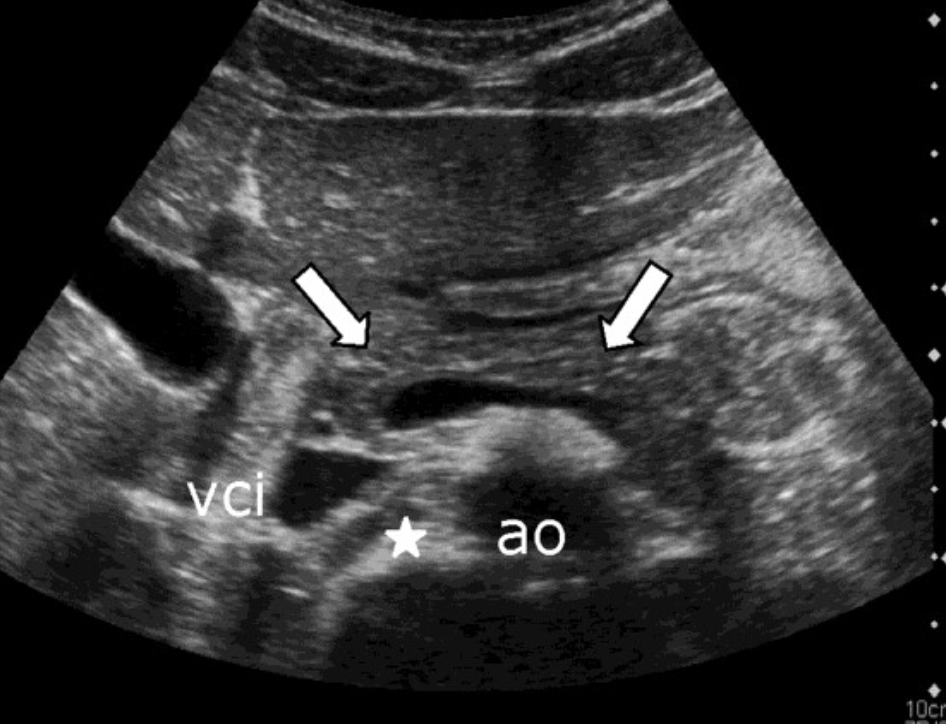
AAA (Abdominal Aortic Aneurysm) → focal dilation of aorta
clinical hx: older (65+) male, smoker, HTN, Marfan syndrome, DM
s/sx: asymptomatic/incidental finding, can have palpable pulsatile mass in midline abdomen, audible bruit (turbulence) → rupture can cause excruciating abdominal pain, back pain, shock, expanding abdominal mass (surgical emergency)
2D US presentation: focally dilated AO (3 cm or greater), mural hypoechoic thrombus, wall calcifications, usually located infrarenal, can be fusiform or saccular
color doppler: turbulent helical flow
DDX: aortic dissection (aorta may be enlarged, but has intimal flap), pseudoaneurysm (focal outpouching w/ narrow neck, but not all 3 layers involved)
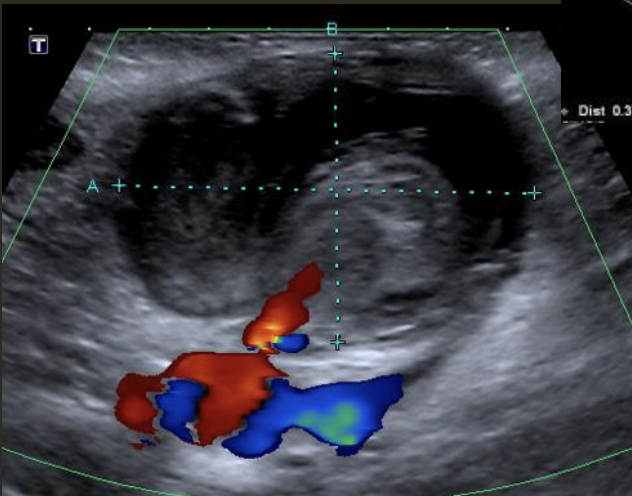
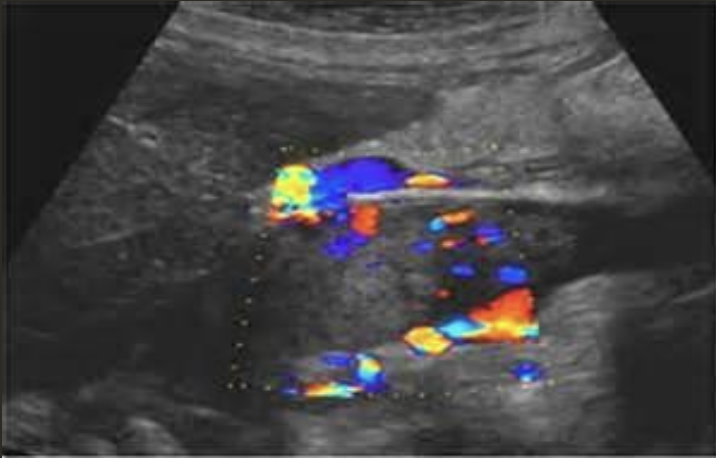
Pseudoaneurysm → rupture from intima layer contained in deeper layers of artery wall
clinical hx: older male, post-catheterization/surgery, trauma
s/sx: acute pulsatile mass, expending mass, pain with bruising, decreased hematocrit, ± increased WBC with mycotic/infected pseudoaneurysm → symptoms appear within hours/days
2D US presentation: heterogenous, pulsating central structure with internal swirling of brighter echogenicity
color doppler: “yin-yang” sign, “to and fro” PW waveform
DDX: hematoma (hypoechoic intraluminal echoes, but not color flow or neck connecting), true aneurysm (wide rather than narrow neck continuous w/ artery, chronic rather than acute)
Aortic Dissection → intimal wall tears and allows blood flow between layers
clinical hx: intimal wall weakness, usually related to surgery, Marfan’s disease, HTN, smoker
s/sx: sudden severe, sharp pain in upper back, tearing/stabbing/ripping feeling
2D US presentation: thin echogenic linear membrane fluttering in lumen creating a true and false lumen
color doppler: fill in both channels → pw shows regular flow in true and weak/no flow in false; asymmetrical kidney perfusion
DDX: AAA (focal dilation, no intimal flap)

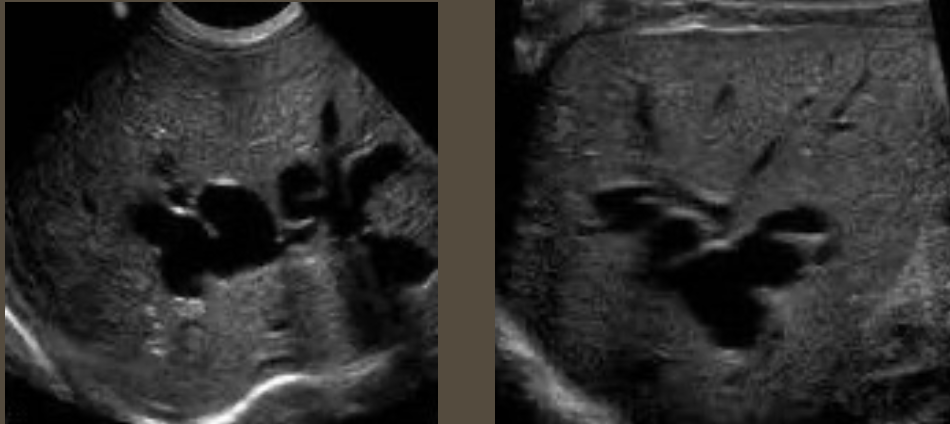
Congestion → increased pressure in IVC and hepatic vein(s) usually by right-sided heart failure
clinical hx: older adults, cardiac issues,
s/sx: epigastric/sternal pain
2D US appearance: dilation of IVC and one or more hepatic veins (IVC greater than 3 cm diameter and hepatic veins greater than 13 mm)
PW: IVC loses “houndstooth” waveform and turns mildly undulating
DDX: budd-chiari (hepatic vein thrombosis/obstruction, but there is no outflow obstruction in congestion)

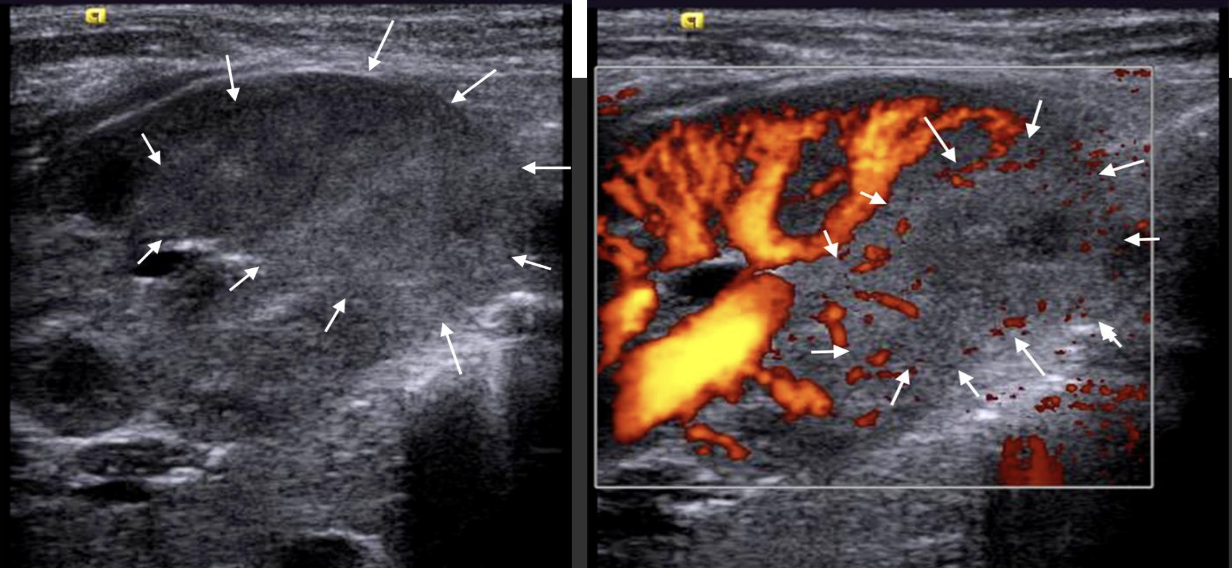
IVC Thrombosis → blood clot in IVC (usually from distal vein or organ)
clinical hx: older, hypercoagulable, immobilized, post trauma or surgery
s/sx: rapid bilateral leg swelling, lower/pelvic pain, ascites, SOB, chest pain
2D US: dilated IVC over 3 cm, intraluminal fill (hypo, echogenic, heterogenous), can be obstruction by IVC tumor
color doppler: lack of fill of affected region, tumor = vessels will be shown feeding tumor in mass
DDX: IVC congestion (dilated IVC, no intraluminal echogenic material), budd-chiari (hepatic vein thrombosis, IVC may be occluded)
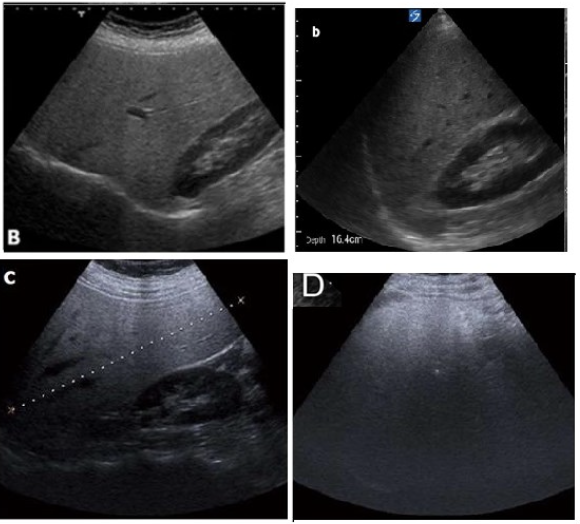
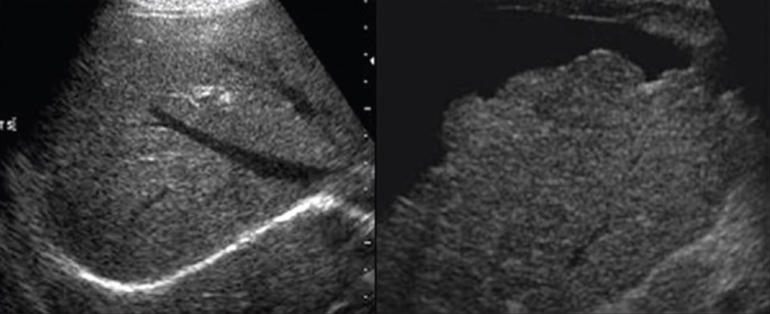
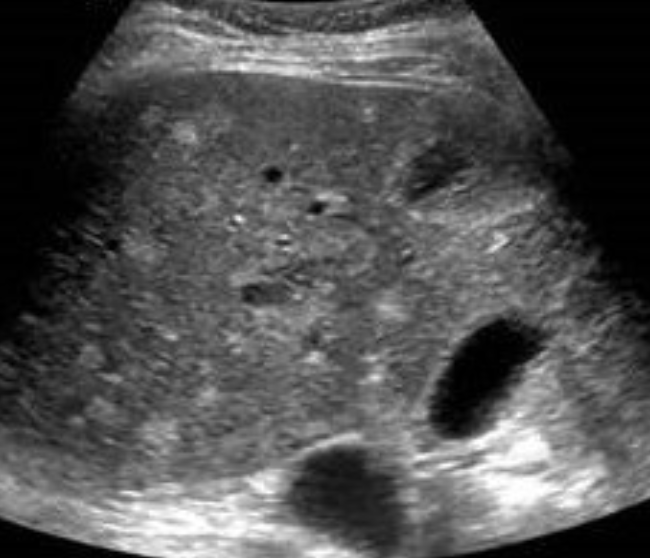
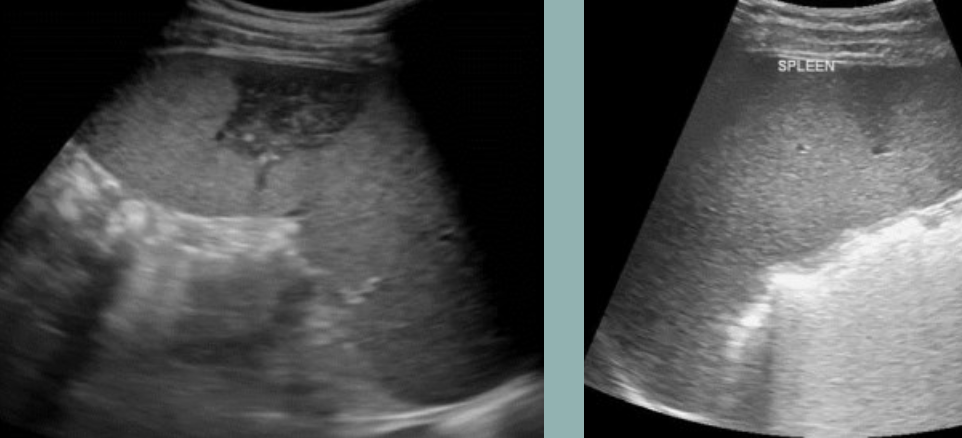
Fatty Infiltration/Fatty Liver Disease → excess fat builds up in liver cells
clinical hx: DM, older male, EtoH abuse, obesity
s/sx: asymptomatic, elevated LFTs, palpable liver
2D US: enlarged liver, diffusely echogenic parenchyma, mild → slightly brighter, can still see periportal fat in veins, moderate → increased echoes, slight impaired diaphragm & vessel borders, severe → significantly brighter, less penetration of posterior right lobe, poor visualization of diaphragm & vessels
DDX: hepatitis (echogenic liver, hepatomegaly, but has bright portal veins), cirrhosis (increased echogenicity, but coarse and nodular)
Glycogen Storage Disease → recessive disease, accumulation of glycogen in liver and kidneys
clinical hx: presents neonatally, recessive
s/sx: asymptomatic, abdominal distention, elevated LFTs (ALT, AST, alk phos)
2D US: echogenic, homogenous liver, hepatomegaly, kidney enlargement, association w/ having hepatic adenomas (adenoma = well-defined, round, homogenous tumor/can be mildly heterogenous if large
DDX: fatty liver (diffusely echogenic & hepatomegaly, but usually adults), hepatitis (hepatomegaly, but hypoechoic not echogenic)
Hemochromatosis & Wilson’s Disease → autosomal recessive, excess iron (HC) and copper (WD) deposits in organs including liver
clinical hx: HC = older adults, WD = young adults/early adulthood
s/sx: abdominal discomfort, fatigue
2D US: echogenic liver, hepatomegaly, can have progressive cirrhotic changes
DDX: fatty liver & glycogen storage disease (echogenic liver, hepatomegaly, but not recessive)

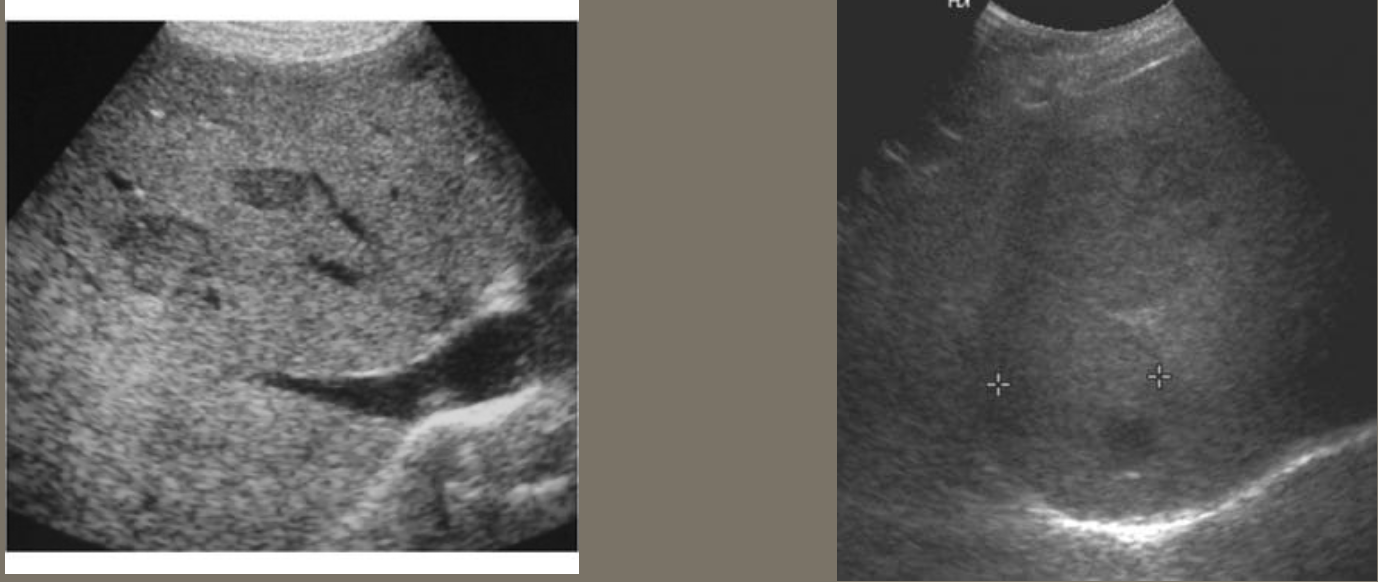
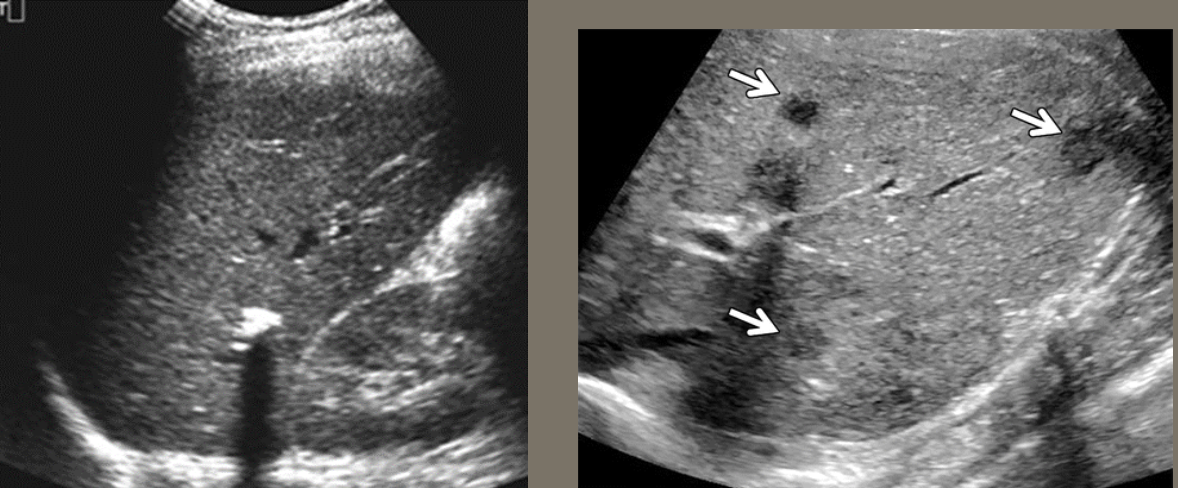
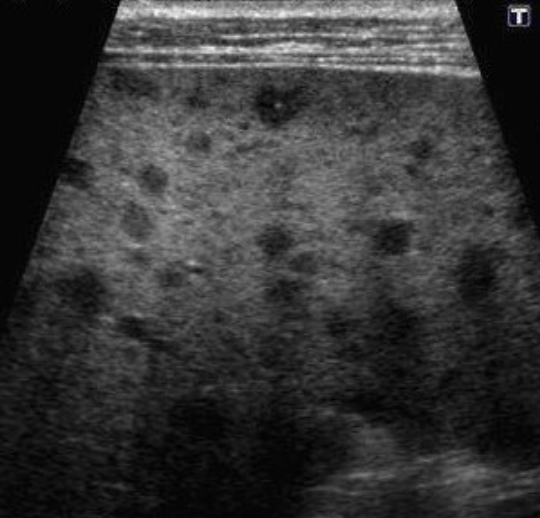
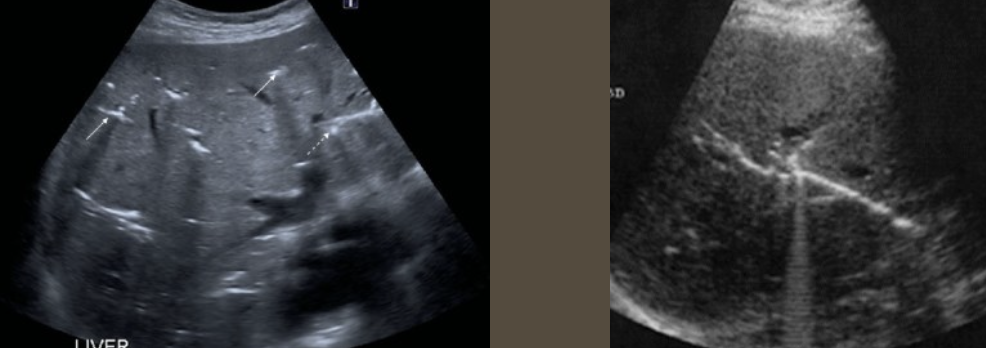
Acute Hepatitis → inflammation of liver
clinical hx: HAV → developing countries, contagious, HBV → needles, healthcare workers, Asia, Africa, HCV → needles (Africa, Europe)
s/sx: asymptomatic initially, can turn to fatigue, GI issues, nausea, and loss of appetite, elevated AST with & ALT x5, jaundice, leukocytosis
2D US: can appear normal, but can be hypoechoic tissue, portal triad edema “cuffing” (starry sky), hepatomegaly, splenomegaly, GB wall thickened w/o distention
DDX: cirrhosis (starry sky appearance can mimic fibrosis, but not acute)
Chronic Hepatitis → continued inflammation of liver (acute hepatitis for 6+ months)
clinical hx: bouts of acute hepatitis, needle users, past HCV
s/sx: asymptomatic, dark urine, jaundice, elevated LFTs, elevated bili
2D US: fibrotic changes, striations in tissue, coarse texture, decrease in portal triad brightness
DDX: cirrhosis (coarse, fibrotic tissue, but has nodular contour)

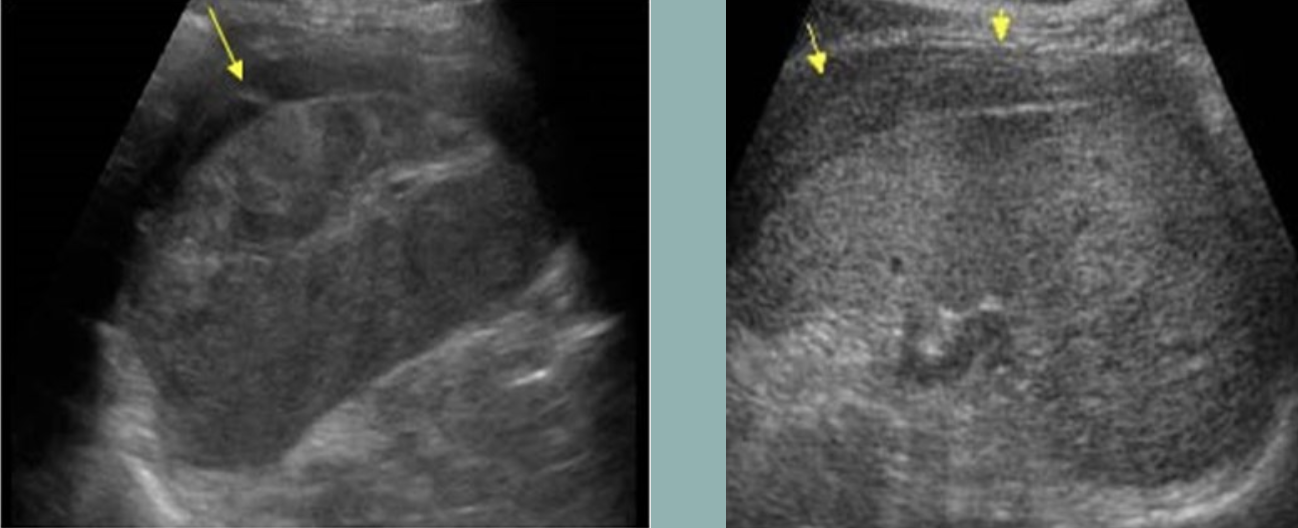
Cirrhosis → chronic liver disease causing fibrosis and scarring
clinical hx: EtoH abuse, older male, obesity, chronic hepatitis
s/sx: asymptomatic, can have abdominal discomfort/distention, anorexia/weight loss, jaundice, dark urine, abnormal AST & ALT, elevated bili
2D US: early stages → hepatomegaly, later/progressive → right ± left lobe atrophy, compensatory caudate lobe hypertrophy, fibrotic heterogenous liver changes, nodular contour, ± hepatic vein compression w/ flattened waveform, PHTN → ascites, splenomegaly, MPV dilation ± reversal of flow
DDX: chronic hepatitis (coarse, fibrotic liver, can turn into cirrhosis if prolonged)
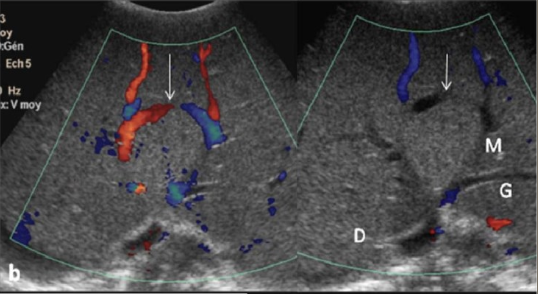
Budd-Chiari Syndrome → rare occlusion of hepatic veins ± IVC
clinical hx: young to middle-aged, hypercoagulable
s/sx: RUQ pain, rapid onset body fluid accumulation, severe elevated LFTs
2D US: intraluminal material isoechoic to liver, hepatomegaly, splenomegaly, ascites, edema
color doppler: no communication between hepatic vein and IVC
DDX: IVC thrombosis (reduced/absent venous flow, but no hepatic vein occlusion), portal vein thrombosis (same secondary findings, but echogenic material in lumen of PV)
HVOD (Hepatic Veno Occlusive Disease) → rare condition where sinusoids are blocked and liver can’t drain properly
clinical hx: stem cell transplant, chemo patients,
s/sx: tender RUQ, rapid weight gain (body fluid accumulation, significant elevated LFTs, elevated bili w/o biliary cause,
2D US: liver swelling, GB wall edema and thickening, dilated MPV, ascites, hepatic artery RI increase
color doppler:
DDX:

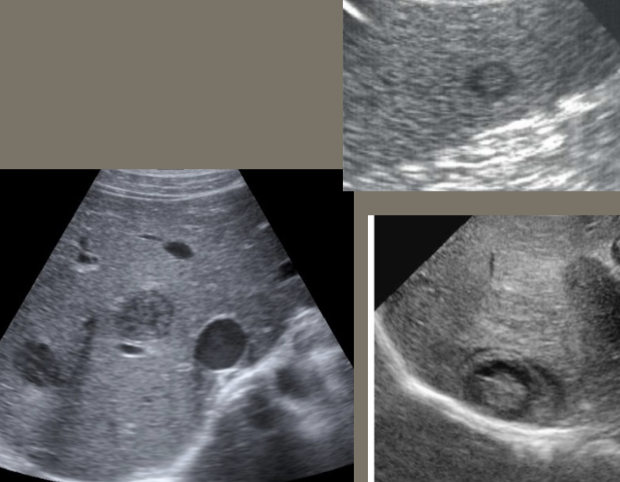
Hepatic Cyst → usually acquired, true cysts are simple cysts
clinical hx: middle-aged or older, women typically
s/sx: asymptomatic, no LFT elevation (if uncomplicated)
2D US: well-defined, thin-walled, anechoic w/ posterior acoustic enhancement, can turn infected or hemorrhagic (internal echoes/septations, thick wall)
color doppler: avascular
DDX: complicated cyst (pyogenic/amebic abscess, hydatid cyst)

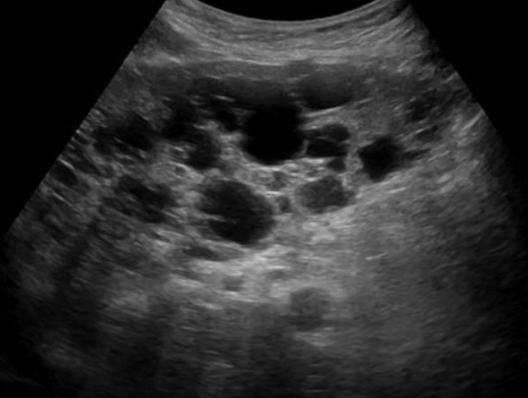
Polycystic Liver Disease → associated with ADPKD
clinical hx: ADPKD, female
s/sx: usually asymptomatic
2D US: varied multiple simple cysts, hepatomegaly from excessive cyst, cysts can become complicated (infected or hemorrhagic)
color doppler: avascular if uncomplicated
DDX: ADPKD, peribiliary cysts, simple cysts
Peribiliary Cysts → rare, fluid-filled sacs forming along bile ducts in liver
clinical hx: *severe liver disease/underlying liver disease
s/sx: asymptomatic
2D US: discrete, clustered, tubular-appearing cysts at the central hilar area of liver
color doppler: avascular
DDX: biliary dilation (mimics appearance of dilated biliary ducts)

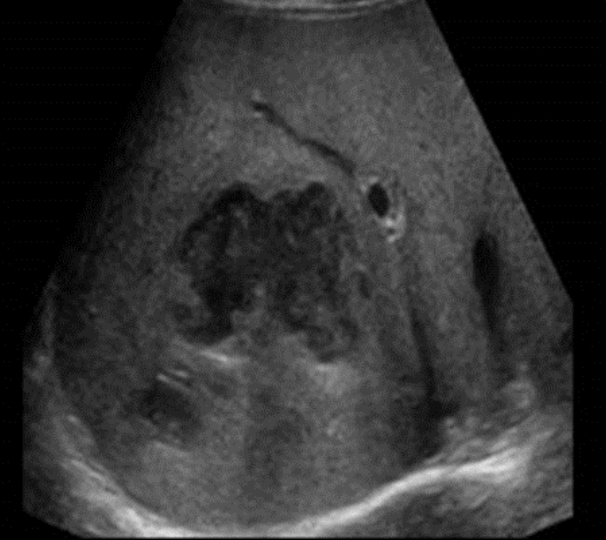
Pyogenic Abscess → pus-filled cyst formed d/t infection
clinical hx: infection (cholangitis, cholecystitis, serious GI infection), iatrogenic
s/sx: fever, increased WBC, anorexia, N&V, RUQ pain
2D US: round, indistinct border, acoustic enhancement, debris filled/can appear solid (echogenic, homogenous, isoechoic heterogenous, septations, altered internal echogenicity), thick echogenic wall
color doppler: no internal vascularity, peripheral vascularity
DDX: amebic abscess, hydatid cyst
Amebic Abscess → parasite reaches liver
clinical hx: recent travel to Central and South America, Africa
s/sx: RUQ pain, persistent diarrhea, leukocytosis
2D US: round/oval, posterior enhancement, uniformly hypoechoic w/ low level internal echoes/debris, ill-defined wall,
color doppler: avascular
DDX: pyogenic/hydatid cyst
Hydatid Disease/Echinococcal Cyst → infectious, parasitic disease (tapeworm) in sheep-herding areas
clinical hx:traveled recently to sheep herding area (
s/sx: may be asymptomatic, RUQ pain, leukocytosis (if it ruptures)
2D US: water lily sign (infolding from collapsed wall), cyst w/ daughter cells, outer wall calcifications,
color doppler: avascular
DDX: amebic abscess, pyogenic abscess

Hepatic Candidiasis → rare, fungal infection through bloodstream
clinical hx: chemo, transplant, immunocompromised
s/sx: persistent, low-grade fevers
2D US: multiple small lesions, uniformly hypoechoic, or wheel within wheel/bullseye appearance (hypoechoic rim, echogenic inner wheel, anechoic center)
color doppler: avascular
DDX:
Chronic Granulomatous Disease → congenital defect resulting in increased susceptibility to severe infections
clinical hx: mostly in children, recurrence in girls,
s/sx: recurrent infections
2D US: ill-defined, hypoechoic mass w/ posterior enhancement, ± calcifications present with posterior shadowing,
color doppler: avascular
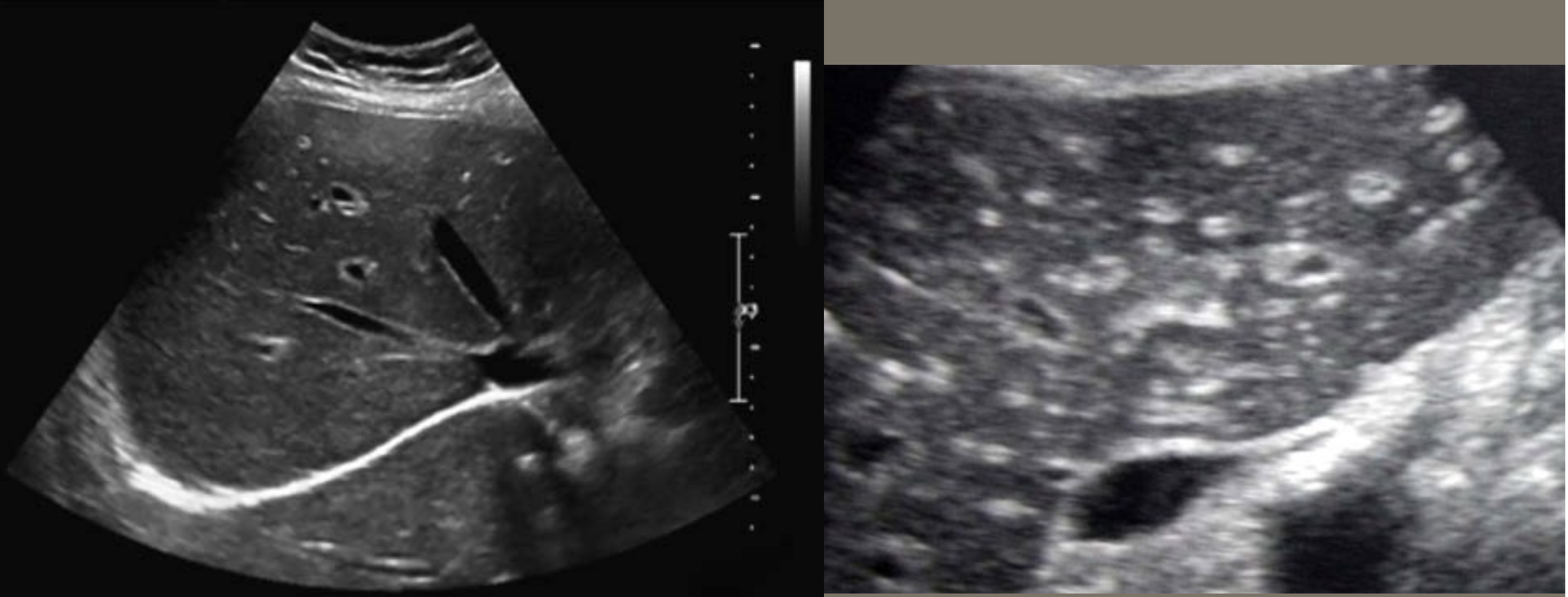
Pneumocystis Carinii → opportunistic infection in immunocompromised
clinical hx: immunocompromised (AIDS)
s/sx: low-grade fever, fatigue
2D US: diffuse, tiny, non-shadowing echogenic foci, replacement of liver parenchyma from echogenic clumps of calcifications (non-shadowing)
color doppler: avascular
DDX: chronic granulomatous disease
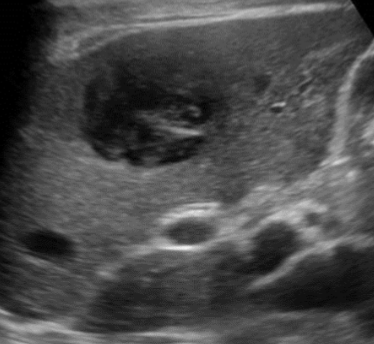
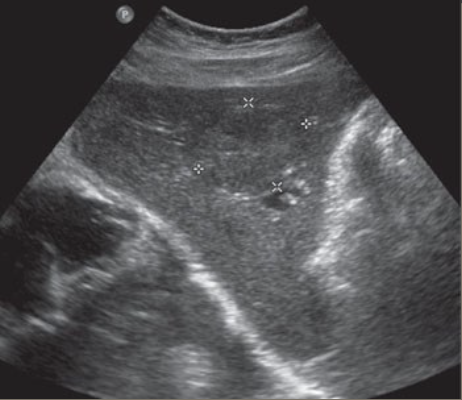
Cavernous Hemangioma → benign tumor of liver
clinical hx: adult female
s/sx: asymptomatic
2D US: typically small (can be large), less than 3 cm, well-defined, homogenous and hyperechoic, scalloped margins or can be heterogenous with hypoechoic center → larger = loses echogenicity w/ hypoechoic center → multiple = hemangiomatosis
color doppler: hypoperfused
DDX: HCC, mets
FNH (Focal Nodular Hyperplasia) → common, benign liver mass
clinical hx: typically women of child-bearing years, long-term birth control
s/sx: asymptomatic
2D US: well-defined, ~5 cm, usually solitary, central hypoechoic scar, isoechoic to hypoechoic to liver
color doppler: central scar → stellate scar doppler pattern (pinwheel)
DDX: hepatic adenoma, hemangioma, HCC
Liver Cell Adenoma → rare, benign liver tumor
clinical hx: oral hormone, glycogen storage disease, typically female
s/sx: palpable abdominal mass, asymptomatic (can have RUQ pain w/ bleeding tumor)
2D US: solitary, up to 15 cm, range of echotexture (echogenic to hypoechoic), calcifications
color doppler: not as vascular, still hard to distinguish from FNH
DDX: HCC, hemangioma, FNH

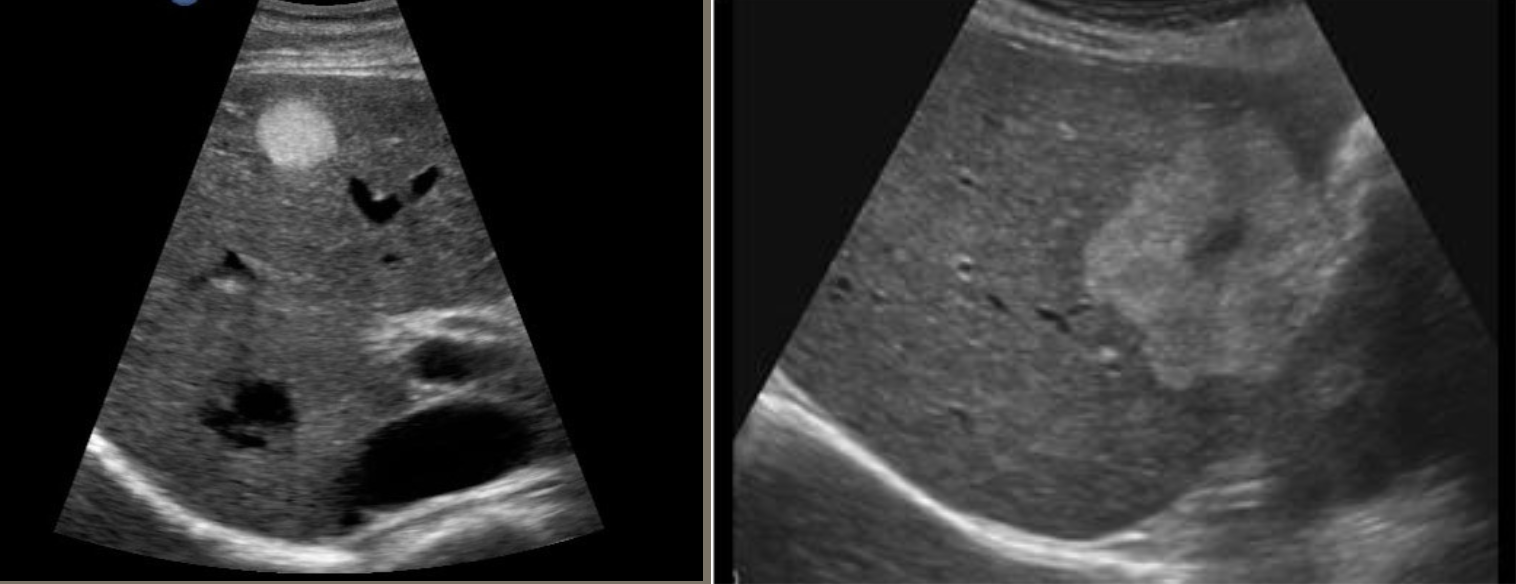
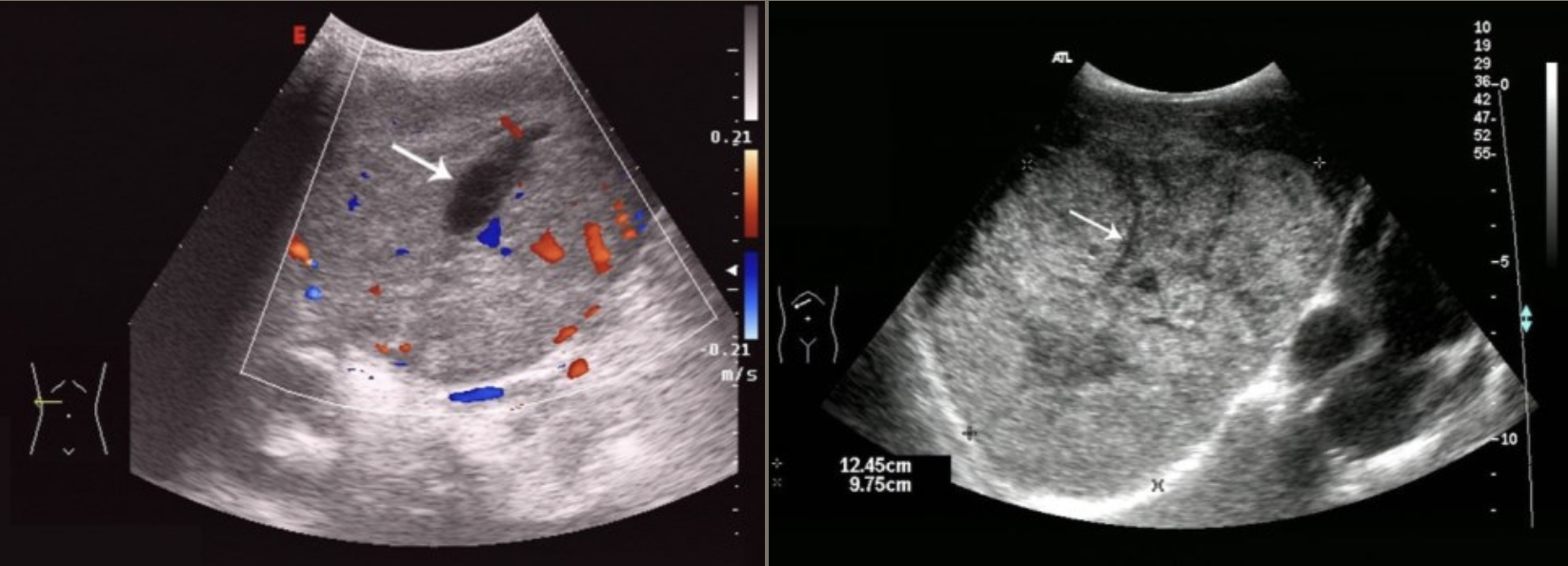
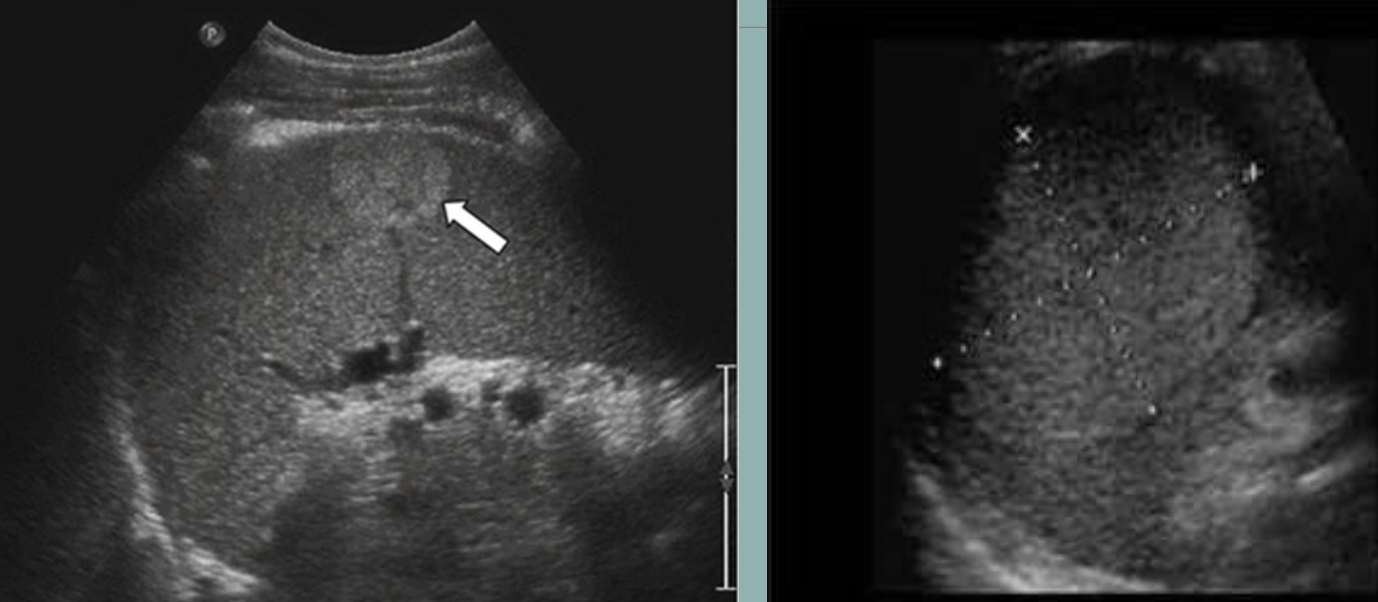
HCC (Hepatocellular Carcinoma) → most common primary malignant neoplasm of the liver
clinical hx: cirrhosis, HBV, HCV, men
s/sx: asymptomatic until invasion, weight loss, abdominal swelling (secondary to ascites), elevated serum AFP
2D US: hypoechoic, echogenic, complex/heterogenous, usually solitary massive tumor, can be multiple nodules throughout the liver, diffuse infiltrative mass, ascites; **fibrolamellar carcinoma has same appearance, but in adolescents
color doppler: very vascular, vascular lumen invasion in both hepatic and portal veins
DDX: liver cell adenoma
Hepatoblastoma → most common primary malignant disease of liver in children under 4
clinical hx: Beckwith-Wiedmann syndrome (overgrowth syndrome), young/child
s/sx: painless, palpable mass, high AFP
2D US: solitary, solid large mass, displacement of vasculature, poorly marginated borders, mixed echotexture (can have areas of hemorrhage, calcifications, necrosis)
color doppler: vascular tumor
DDX: HCC (diff. patient population), Wilm’s Tumor (same presentation as HCC and hepatoblastoma but appears in young adults)
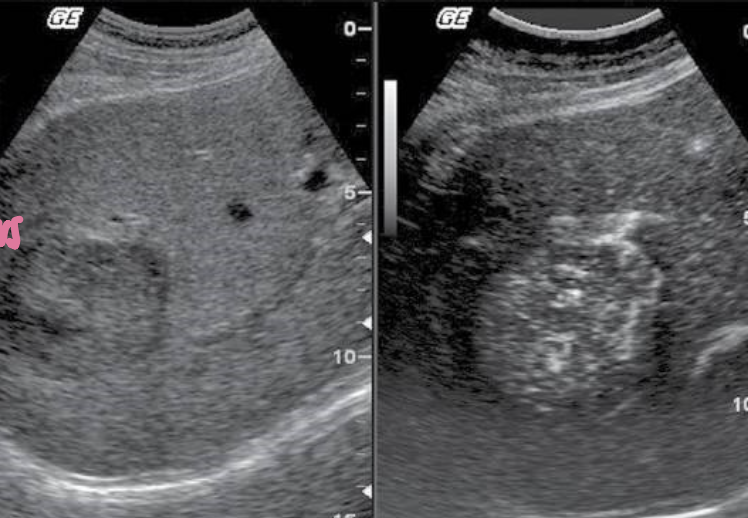
Metastatic Disease (METS) → most common form of neoplastic involvement of the liver
clinical hx: active CA diagnosis or prior remission history
s/sx: can be asymptomatic, abnormal LFTs, jaundice, poor appetite, abdominal distention/bloating & weight loss
2D US: single or multiple solid lesions, varying sizes, can have bullseye appearance, echogenic, or hypoechoic, enlarged liver, can cause pseudo nodularity
color doppler: hypo to hypervascular
DDX: HCC, hemangioma, lymphoma
Lymphoma → lymphocyte proliferation in lymph nodes
clinical hx: known history of lymphoma
s/sx: nontender enlarged lymph nodes, night sweats, weight loss, palpable mass, elevated LFTs and alkphos, jaundice
2D US: multiple hypoechoic masses, lobular, poor margins, encases vasculature, periportal enlarged hypoechoic lymph nodes, splenomegaly
color doppler:
DDX: METS, HCC
Simple Splenic Cysts → secondary cysts from trauma, infection, or infarction (technically pseudocysts, since congenital cysts are rare)
clinical hx: trauma
s/sx: asymptomatic, can have LUQ pain
2D US: round, smooth, well-defined borders, anechoic fluid-filled lumen, no internal echoes (unless complicated, can produce posterior enhancement)
color doppler: avascular
DDX: splenic abscess/infected/complicated cyst
Splenic Abscess → pus-filled sac secondary to infection
clinical hx: underlying infection = endocarditis, septicemia, pancreatitis
s/sx: fever, LUQ tenderness, abdominal pain, left shoulder/flank pain, increased WBC
2D US: simple cyst to mixed echo pattern, hyperechoic nondependent foci representing gas
color doppler:
DDX: pancreatic cyst/infection (if near hilum), simple cyst
Hepatosplenic Candidiasis → severe systemic infection in those w/ weakened immune systems
clinical hx: immunocompromised (AIDS, chemo), fungal infection
s/sx: fever, abdominal pain, splenomegaly, nausea, anorexia
2D US: multiple hypoechoic abscesses, “bulls eye” sign (hypoechoic rim w/ echogenic core), hypoechoic ill-defined nodule, hyperechoic nodule
color doppler: avascular
DDX: splenic abscess (but usually solitary)
Splenic Infarction → blood supply to section of spleen is interrupted, leads to localized necrosis
clinical hx: infection, cardiac conditions
s/sx: acute LUQ pain, fever
2D US: peripheral hypoechoic wedge extending to capsule, normal adjacent parenchyma, later chronic ± fibrotic echogenic changes, ± splenomegaly
color doppler: avascular
DDX: splenic abscess, hematoma
Splenic Trauma → blunt trauma usually resulting in hematoma
clinical hx: usually blunt abdominal trauma, underlying splenomegaly increased risk
s/sx: LUQ pain, low hematocrit from bleeding, abdominal swelling/bloating discomfort
2D US: capsule intact = subcapsular hematoma (conforms to spleen shape), ruptured capsule = free fluid/hematoma may form (check abdominal gutters for free fluid)
color doppler: avascular
DDX: splenic infarction, splenic abscess
Cavernous Hemangioma → most common benign tumor of the spleen
clinical hx: adults, no gender preference
s/sx: asymptomatic
2D US: variable → well-defined echogenic to complex heterogenous pattern w/ hypoechoic regions or isoechoic
color doppler: hypoperfused
DDX: METS, infection
Cystic Lymphangioma → rare benign lymph node collection
clinical hx: usually incidental, manifests in children/young adults
s/sx: asymptomatic, can cause mass effect if large
2D US: mass w/ extensive tissue cystic tissue replacement, when spleen involved multicystic appearance is common
color doppler: avascular
DDX: echinoccocal cyst
Hamartoma → rare benign tumor; overgrowth of normal tissue
clinical hx: adults, no gender preference
s/sx: asymptomatic
2D US: both solid and cystic components, hyperechoic usually, solitary or multiple, well-defined
color doppler: vascular
DDX: hemangioma

Lymphoma → cancer of lymphocytes in spleen
clinical hx: middle-aged/older adults
s/sx: unexplained fevers, night sweats, unintentional weight loss, fatigue
2D US: splenomegaly, hypoechoic lesions, enlarged LUQ lymph nodes, can small/large focal nodular lesions, diffuse or small nodular pattern
color doppler: vascular
DDX:
Metastases → cancer cells metastasized to spleen
clinical hx: current CA (advanced if spread to spleen)
s/sx: can be asymptomatic if microscopic
2D US: varied appearance = hypoechoic, echogenic w/ hypoechoic halo, target or “bulls eye,” well-defined with increase in size
color doppler: vascular
DDX: lymphoma, abscess
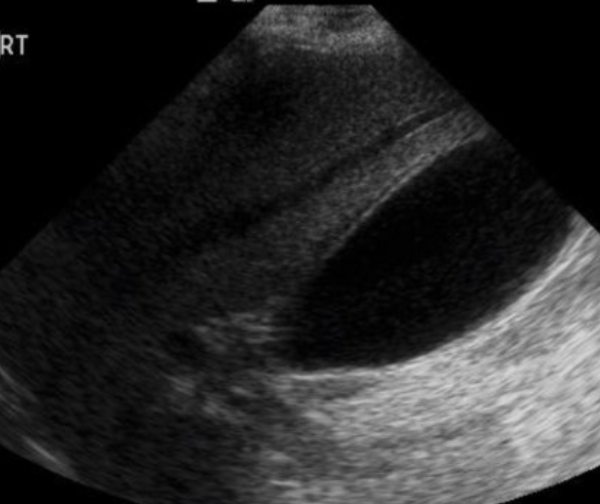
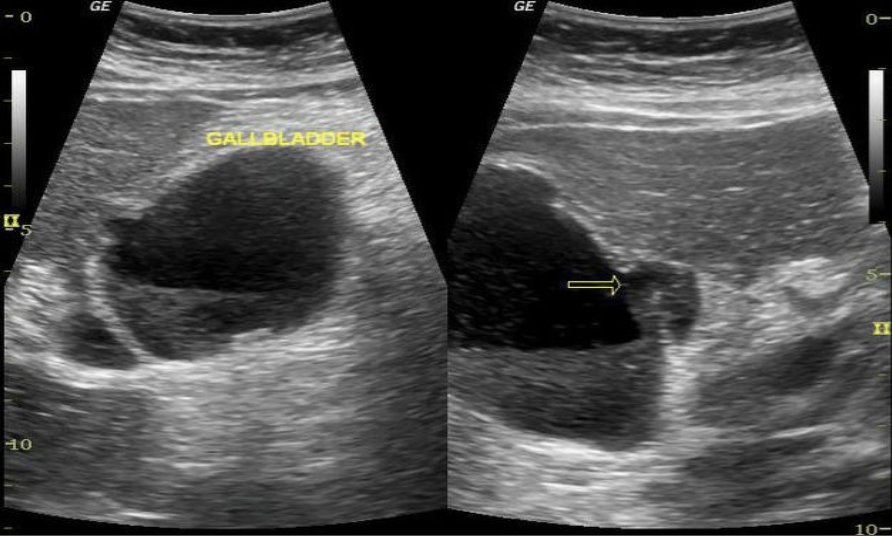
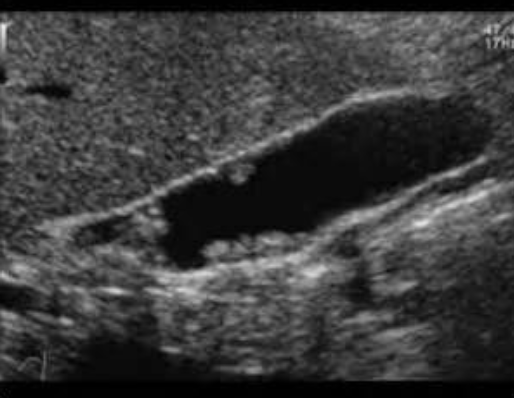
Hydropic Gallbladder → distended GB
clinical hx: middle-aged to older, fasting, post-surgery
s/sx: asymptomatic, if not = RUQ pain, fullness/bloating
2D US: no relaxed curves, rounded/bulbous shape, ± distended cystic duct (check for obstruction), maintained thin wall
color doppler: avascular
DDX: acute cholecystitis, cholelithiasis
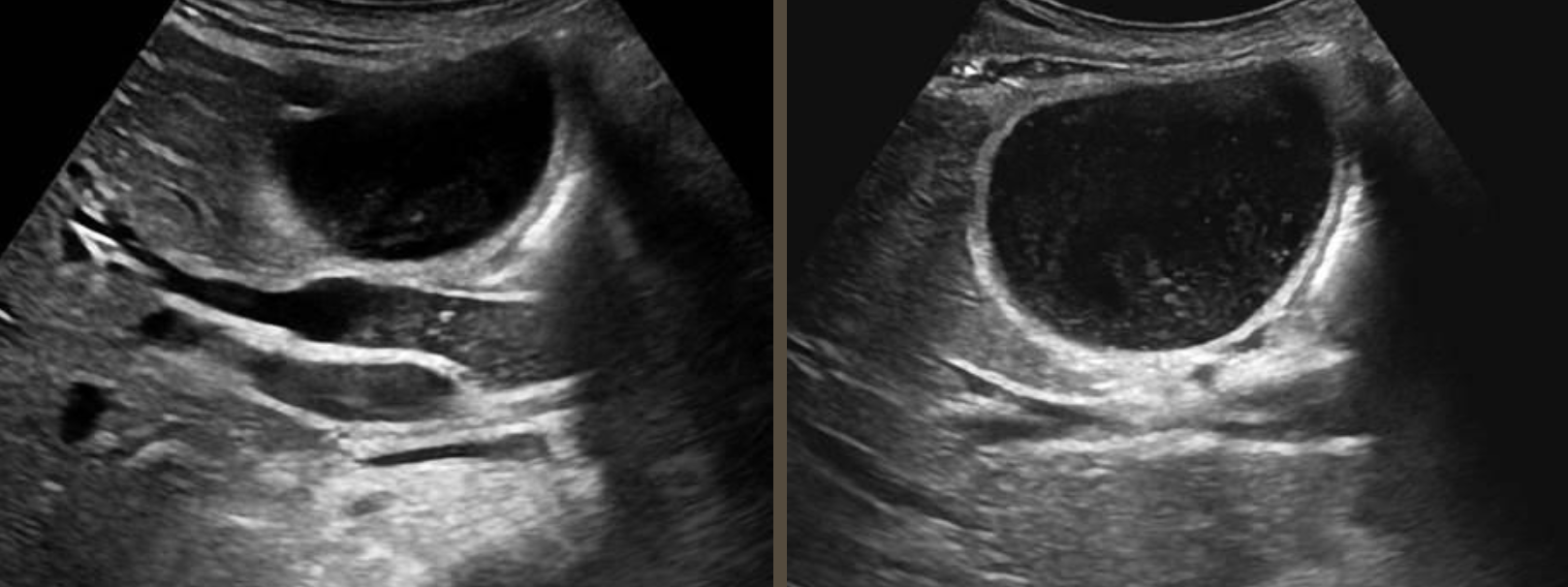
GB Sludge → thickened bile from stasis
clinical hx: pregnant, fasting, critical illness, obstruction of GB
s/sx: asymptomatic, can have RUQ pain/biliary colic
2D US: layered, homogenous milk to moderately echogenic echoes, changes w/ patient mobility, no acoustic shadowing, can be tumefactive = balled up sludge can mimic mass, GB filled w/ sludge = hepatization (isoechoic to liver)
color doppler: avascular
DDX: polyp/tumor, hemobilia
GB Hemobilia → blood in GB
clinical hx: post-procedure, tumor, trauma, infection
s/sx: RUQ pain, anemic (decreased hematocrit)
2D US: lumen fill of mixed echogenicities = cystic regions/heterogenous woven, distended GB >4 cm AP
color doppler: avascular
DDX: GB sludge
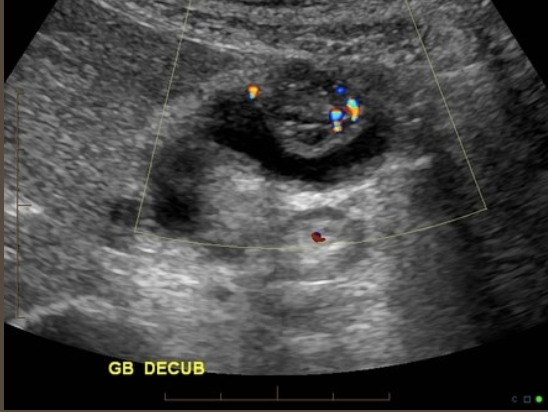
Cholelithiasis → stone in GB
clinical hx: 5 Fs (fat, fourty, female, fertile, fair)
s/sx: commonly asymptomatic, RUQ pain after eating greasy/heavy foods, GB attack/referred pain → right shoulder, back, & sternal chest pain
2D US: well-defined echogenic foci in dependent part of GB producing dark posterior shadowing (stones under 3 mm may not produce shadow), WES sign = wall-echo-shadow sign indicating multiple stones/one large stone, mobile w/ patient positioning
color doppler: avascular
DDX: GB sludge (tumefactive), polyp

Acute Cholecystitis → sudden inflammation of GB
clinical hx: 5 Fs (cholelithiasis common cause of inflammation)
s/sx: constant RUQ pain, positive sonographic Murphy’s sign, N&V, increased WBCs, elevated bilirubin and alk phos if obstruction
2D US: GB wall > 3mm ~6-8 mm, distended lumen (> 4 cm AP and > 10 cm length), gallstones, impacted stone in neck or cystic duct, positive Murphy’s sign, pericholecystic fluid collection
color doppler: increased flow (supportive, not reliable)
DDX: GB sludge
Chronic Cholecystitis → numerous attacks of acute cholecystitis/inflammation causing fibrosis of GB wall
clinical hx: bouts of acute cholecystitis ← also 5 Fs
s/sx: transient RUQ pain, not as reactive to Murphy’s sign
2D US: thickened wall (3.5-4 mm, thickened but not thicker than acute), shrunken, fibrotic GB
color doppler: slightly less flow due to fibrosis
DDX: acute cholecystitis
Gangrenous Cholecystitis → prolonged infection causing GB necrosis
clinical hx: older male, DM (neuropathy can mask pain)
s/sx: fever, hypotension, severe rebound tenderness if abscess leaks, increased WBCs
2D US: usually gallstones and sludge, pericholecystic biloma/rupture of GB wall, sloughed membrane/mucosal layer appearing as intraluminal echo, ± thickened and edematous wall, ulcerations and perforations → pericholecystic biloma/abscess, 80-90% of patients
color doppler: avascular
DDX: acute cholecystitis, chronic cholecystitis
Emphysematous Cholecystitis → rare, air within GB wall
clinical hx: male, DM
s/sx:
2D US: ± gallstones, prominent hyperechoic echo in anterior wall w/ reverbirations & ringdown, can have pericholecystic fluid, loss of defined GB wall layers
color doppler:
DDX: adenomyomatosis
Acalculous Cholecystitis → uncommon, acute cholecystitis w/o stones
clinical hx: critically ill, sepsis patients, HIV, immunocompromised
s/sx: positive Murphy’s sign, increased WBC, can have RUQ pain, fever
2D US: positive Murphy’s sign, distended lumen, GB wall edema
color doppler: wall vascularity
DDX: acute hepatitis, colitis, pancreatitis

Porcelain GB → rare, calcium deposit of GB wall, 25% of patients will develop cancer of the GB wall
clinical hx: association w/ gallstones/chronic cholecystitis, older female
s/sx: asymptomatic
2D US: can appear as mixed speck pattern within wall or more diffuse, clean calcification, posterior shadowing from calcifications
color doppler: avascular
DDX: cholelithaisis, emphysematous GB
Adenomyomatosis → benign, common exaggeration of inner layer of GB wall (mucosal layer)
clinical hx: middle-aged female
s/sx: asymptomatic
2D US: non distended GB, mucosal layer thickening with cystic spaces, focal thickening at fundus more common, produces comet tail artifact, usually on anterior wall, can produce hourglass change of GB shape
color doppler: avascular, can have hypovascular pattern in hypoechoic lesion (adenomyoma)
DDX: emphysematous GB, porcelain GB
Cholesterolosis → benign, polypoid lesions formed in inner wall of GB from cholesterol deposits
clinical hx:
s/sx:
2D US: “strawberry GB”, small, echogenic, well-defined soft-tissue projections connected by stalk to GB wall, no posterior shadow, non mobile, < 10 mm diameter
color doppler: stalk of polyp is vascular
DDX: cholelithasis
Gallbladder Carcinoma → (rare) primary carcinoma of GB
clinical hx: 60+ female, continuous inflammation (chronic cholelithiasis/cholecystitis)
s/sx: weight loss, jaundice, anorexia
2D US: irregular thickening of wall, invasion of liver, intraluminal polypoid mass 10 cm or greater, mass replacing GB fossa, loss of definition between layers, ± increased bili from liver infiltration
color doppler: internal vascular flow
DDX: HCC, cholangiocarcinoma
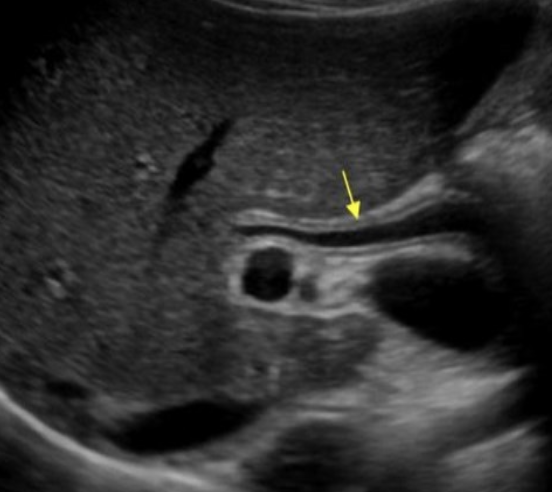
Choledocholithiasis → stones in biliary tree
clinical hx: 5 Fs → same as cholelithiasis since stone can travel
s/sx: jaundice, elevated bili and alk phos, constant RUQ pain, epigastric pain, fever, pancreatitis
2D US: “double barrel” sign, “too many tubes,” stone has rounded surface, highly echogenic, ± posterior shadowing, peripancreatic head edema/fluid → pancreatitis, gallstones, wall edema and distention
color doppler: may see twinkle artifact from stone
DDX: biliary sludge, cholangiocarcinoma

Biliary Sludge → thickened bile in biliary tree
clinical hx: pregnancy, prolonged fasting, critically ill/post surgery
s/sx: asymptomatic, jaundice, RUQ pain, elevated direct bili, alk phos
2D US: duct filled with non calcified, mid level echogenic material (can’t differentiate from blood on US), biliary dilation, can have “double barrel” sign
color doppler: avascular
DDX: choledocholithiasis, cholangiocarcinoma
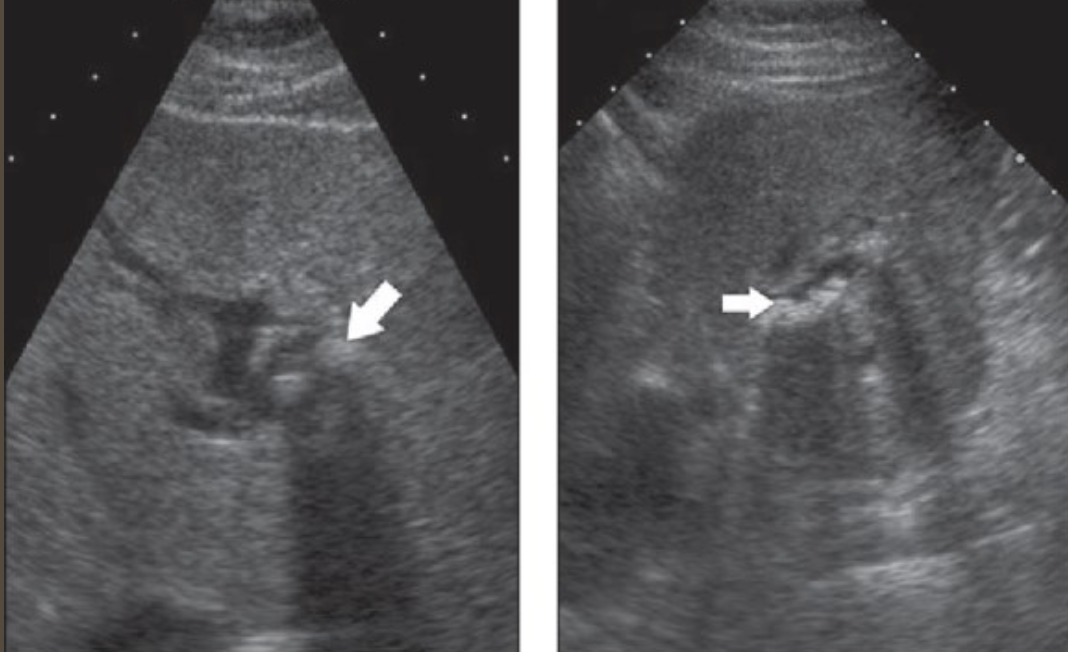
Pneumobilia → air within biliary tree secondary to biliary intervention/procedures, emphysematous cholecystitis, prolonged acute cholecystitis
clinical hx: acute abdomen hx, post biliary procedure, prior emphysematous/acute cholecystitis
s/sx: RUQ pain, N&V, jaundice, fever, abdomen distention
2D US: bright echogenic linear structures following portal triads w/ posterior dirty shadowing and revirberations
color doppler: avascular
DDX: chronic liver disease (i.e. cirrhosis)
Acute Cholangitis → inflammation of bile ducts usually from prolonged obstruction, medical emergency
clinical hx: biliary obstruction hx or current
s/sx: fever, RUQ pain, jaundice, leukocytosis, elevated liv transaminase, elevated bili and alk phos
2D US: biliary dilation, hypoechoic mucosal wall thickening, choledocholithasis or sludge, later → liver abscess
color doppler: avascular
DDX: cholecystitis, choledocholithasis
Pyogenic Cholangitis → more chronic form, seen in individuals from south Asia
clinical hx: south Asia, state of stasis
s/sx: RUQ pain, fever, jaundice
2D US: atrophy of involved segment, stones confined to region w/ associated biliary dilation, stones may or may not shadow
color doppler: avascular
DDX: acute cholangitis, cholecystitis
Sclerosing Cholangitis → chronic inflammation disease affecting entire biliary tree
clinical hx: males
s/sx: abnormal liver transaminase, jaundice if obstructive or underlying liver disease, asymptomatic, underlying autoimmune disease
2D US: irregular, circumferential bile duct wall thickening w/ small diverticuli in intrahepatic ducts (beads on string appearance), pinched off intrahepatic ducts from strictures, choledocholithiasis, biliary sludge
color doppler:
DDX: cholangiocarcinoma, choledocholithiasis

Intrahepatic Cholangiocarcinoma → common primary malignancy of liver (least likely location for cholangiocarcinoma
clinical hx: HCV, cirrhosis
s/sx: painless jaundice, dark urine, increased bili & alk phos
2D US: solid mass w/ variable appearance, large hepatic mass, heterogenous, ill-defined, ± biliary dilation
color doppler: hypovascular
DDX: HCC, mets

Hilar Cholangiocarcinoma/Klatskin’s Tumor → tumor at hilar level of liver
clinical hx: HCV, cirrhosis, male
s/sx: abnormal bili & alk phos, jaundice
2D US: dilation of higher order ducts w/ no connection between R & L ducts to CHD, ill-defined tumors with poor borders, isoechoic tumor, portal vein stricture/compression
color doppler:
DDX: HCC, distal cholangiocarcinoma
Distal Cholangiocarcinoma → bile duct cancer outside of liver
clinical hx: older, hx of sclerosing cholangitis
s/sx: jaundice
2D US: well-defined polypoid tumor found in ducts, extends along extrahepatic ducts towards hilum, nodular, intrahepatic dilation, invasion of adjacent structures
color doppler: hypovascular
DDX: pancreatic head tumor, ampullary duodenal tumor

Mirizzi Syndrome → obstruction of CHD by secondary inflammation due to stone impacted in cystic duct
clinical hx: cholecystectomy w/ residual stone or cholecystitis
s/sx: RUQ pain, fever, jaundice
2D US: cholecystitis with large stone in cystic duct, cystic duct stump with large calcified stone, intrahepatic dilation, normal CBD
color doppler:
DDX: cholangiocarcinoma, choledocholithiasis/cholelithiasis
Caroli’s Disease → rare, recessive found in peds, communicating ectasia of intrahepatic ducts
clinical hx: young, peds, renal disease/congenital hepatic fibrosis association, strong association with medullary sponge kidney
s/sx: cramplike upper abdominal pain from stasis
2D US: multiple cystic structures toward porta hepatis, localized masses or scattered cysts communicating with bile ducts, ± sludge & calculi
color doppler: avascular
DDX: sclerosing cholangitis, polycystic liver disease, hepatic cysts
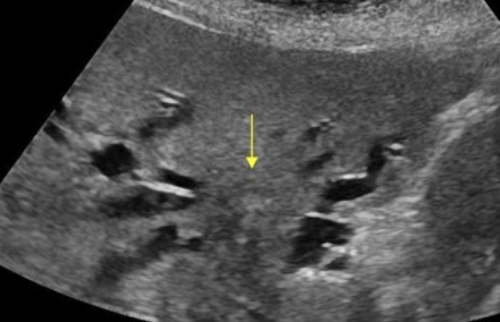
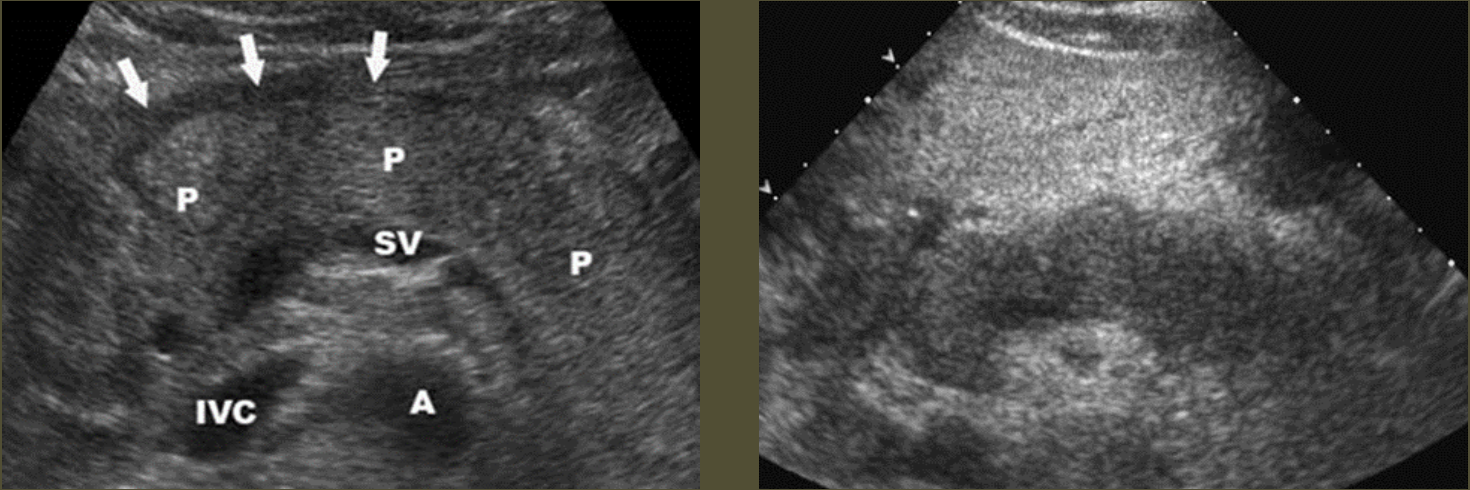
Acute Pancreatitis → sudden inflammation of pancreas from blockage of ducts and increased secretions
clinical hx: gallstones in bile duct, alcohol abuse, obstruction/mass, endoscopy, trauma, drugs, transplant
s/sx: increased amylase (not as useful), increased lipase (more specific), sudden severe epigastric pain, pain radiating to mid back, LUQ pain, N&V, fever, increased WBCs, jaundice (if biliary obstruction)
2D US: pancreas enlargement, hypoechoic parenchyma from edema, irregular ill-defined borders, peripancreatic free fluid, peripancreatic echogenic inflammatory fat, can have focal areas of inflammation/hypoechoic tissue
color doppler: can have hyperemia
DDX: chronic pancreatitis
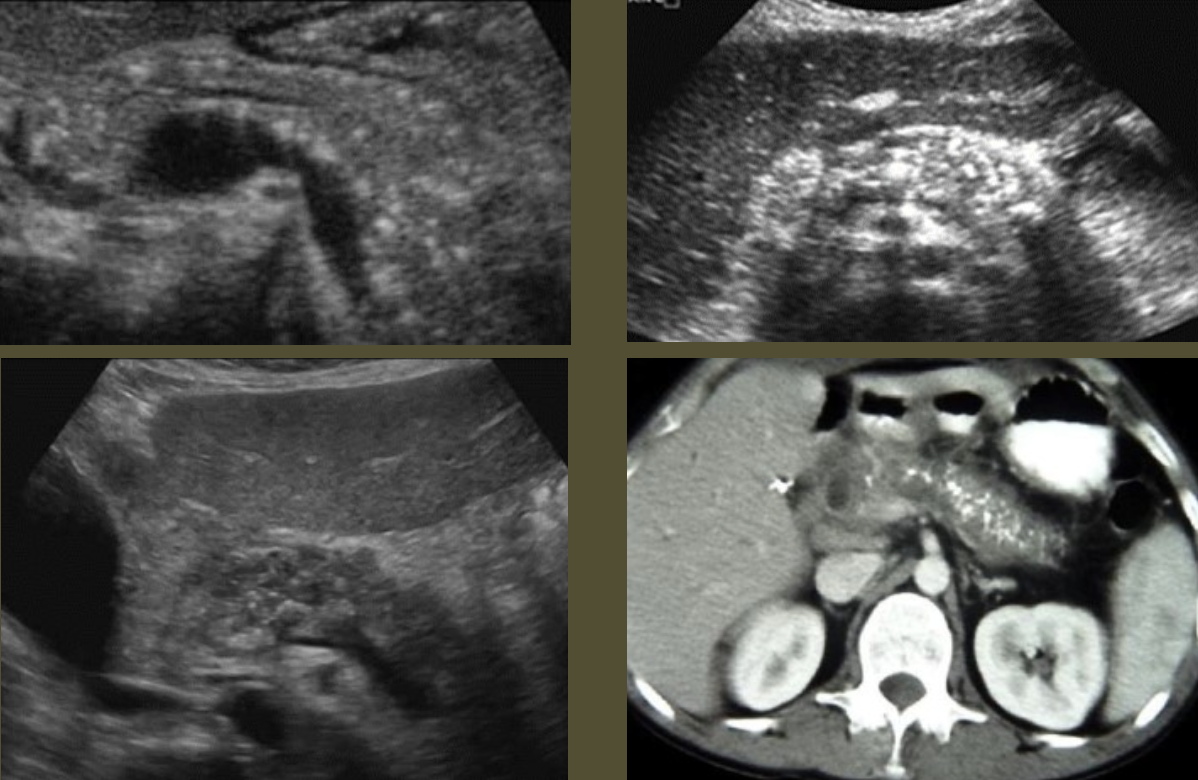
Chronic Pancreatitis → recurrent attacks of acute pancreatitis, progressive destruction of pancreatic tissue
clinical hx: association w/ chronic alcoholism/biliary disease, increased risk of developing pancreatic cancer
s/sx: asymptomatic, pancreatic insufficiency (digestion issues & glucose intolerance), jaundice if biliary obstruction, lipase can be elevated (more likely than amylase)
2D US: mixed pattern of echogenicity (hyperechoic from fibrosis to hypoechoic from inflammation), calcifications, normal to atrophic size, nodular surface, dilated/calcified pancreatic duct (> 3 mm), solid mass, thrombosis of splenic and portal vein
color doppler:
DDX: acute pancreatitis
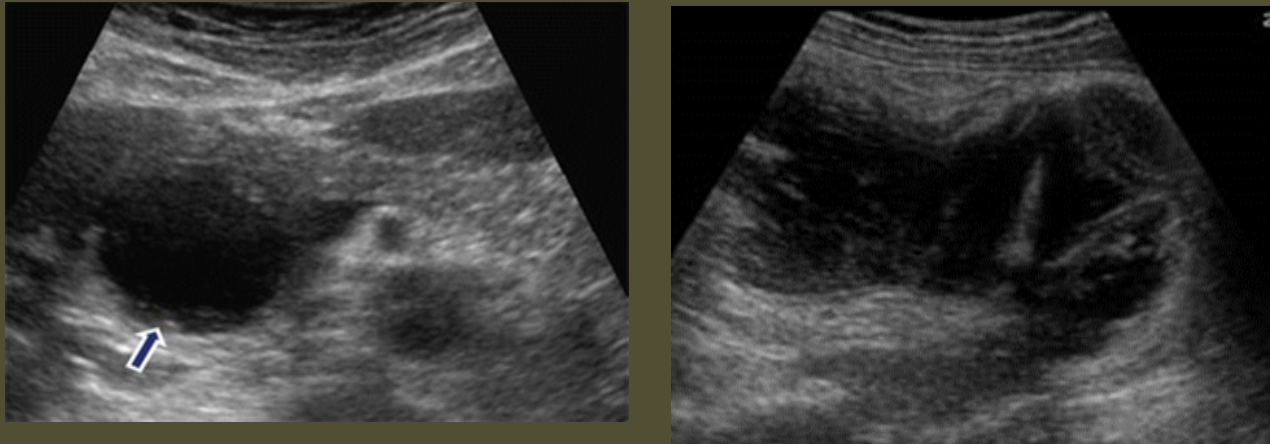
Pancreatic Pseudocyst → peripancreatic fluid collection from trauma or pancreatitis (4-6 week onset after pancreatitis)
clinical hx: trauma, hx of pancreatitis
s/sx: patient will feel better because of walled off inflammation, rupture → sudden shock and peritonitis, ascites if ruptures into abdomen
2D US: not always spherical, usually located in lesser sac (anterior to pancreas and posterior to stomach)
color doppler: avascular
DDX: true cyst
Cystic FIbrosis in Pancreas → mucus from CF plugs ducts
clinical hx: pancreatic lipomatosis (fatty replacement of pancreas → obesity, DM, older age), younger patient with respiratory issues (CF)
s/sx: abdominal distention/bloating
2D US: small pancreatic cysts (1-3 mm) → can be seen on ultrasound if bigger than 3 mm, increased pancreas echogenicity
color doppler: avascular
DDX: chronic pancreatitis, pancreatic lipomatosis, autosomal dominant polycystic disease (can rarely manifest in pancreas)
Microcystic Adenoma (Serous Cystadenoma) → rare, benign tumor
clinical hx: female, older
s/sx: asymptomatic
2D US: well-defined tumor, large mass with multiple tiny cysts, no ductal obstruction
color doppler: vascular
DDX: malignant tumor
Macrocystic Adenoma (mucinous cystadenoma) → malignant or benign with malignant potential
clinical hx: female
s/sx: nonspecific abdominal symptoms, weight loss, abdominal mass, jaundice
2D US: usually found in body or tail, well-defined cysts with thick mucinous fluid, internal septations, or solid mural nodules, larger than 2 cm cysts, calcifications → more solid components = more chance for malignancy
color doppler: hypovascular
DDX: pseudocyst
IPMT (Intraductal Papillary Mucinous Tumor) → slow-growing lesion, form of mucinous cystic neoplasm
clinical hx: 60-70 years, no gender preference, recurrent pancreatitis
s/sx: asymptomatic
2D US: originates from main duct
color doppler: hypovascular
DDX: macrocystic adenoma
Adenocarcinoma → most common primary neoplasm of pancreas
clinical hx: usually 60+ y/o, rarely found as hereditary association in male patients
s/sx: head → obstruction of CBD w/ jaundice and hydropic GB, courvoisier sign (palpable non-tender w/ jaundice in GB), body and tail (tail is least common) → weight loss, pain, jaundice, vomiting
2D US: usually found in head, larger and invade adjacent organs, poorly defined mass, isoechoic or hypoechoic, enlargement of involved region, dilated panc duct over 3 mm, dilated CBD at head, displacement and compression of adjacent vessels
color doppler: vascular
DDX: chronic pancreatitis
Insulinoma → most common functioning islet cell tumor of pancreas, usually benign
clinical hx: 40-60 y/o, obese
s/sx: hypoglycemic symptoms, palpitations, headache, confusion, pallor, sweating, slurred speech, coma
2D US: small, well-encapsulated hypoechoic tumor usually in body or tail
color doppler: vascular
DDX: adenocarcinoma, focal pancreatitis
Gastrinoma → second most common functioning islet cell tumor of pancreas from non-insulin secreting panc tumors secreting excessive amounts of gastrin, malignant
clinical hx: 50 y/o,
s/sx: N&V, abdominal pain, weight loss
2D US: typically tumor found in head, peptic and duodenal ulcers present, usually multiple, can be extrapancreatic
color doppler: vascular
DDX:

Pancreatic Lymphoma → malignant neoplasm, usually parapancreatic
clinical hx:
s/sx: abdominal pain, weight loss, palpable mass, jaundice, N&V
2D US: cystic mass in pancreas, multiple nodes along pancreas, duodenum, porta hepatis, and SMV and SMA
color doppler: hypovascular
DDX: adenocarcinoma
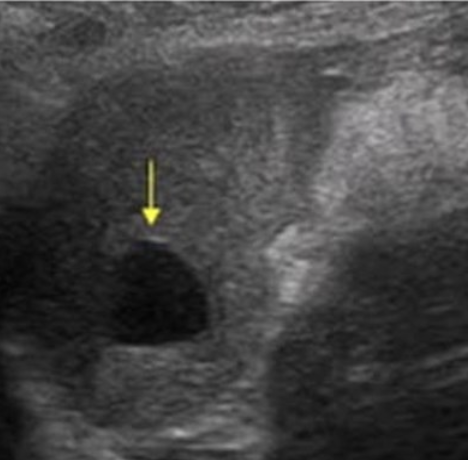
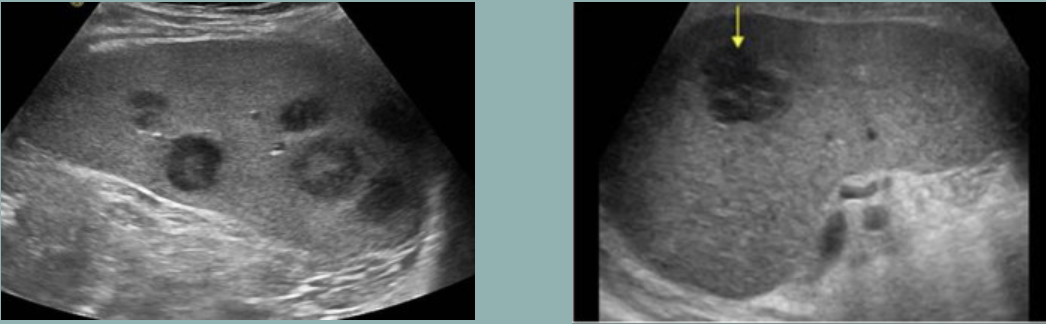
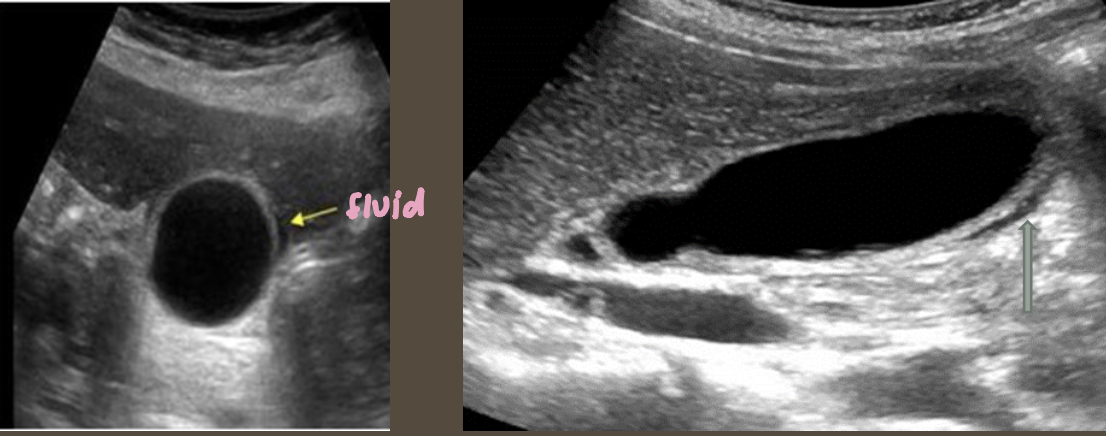
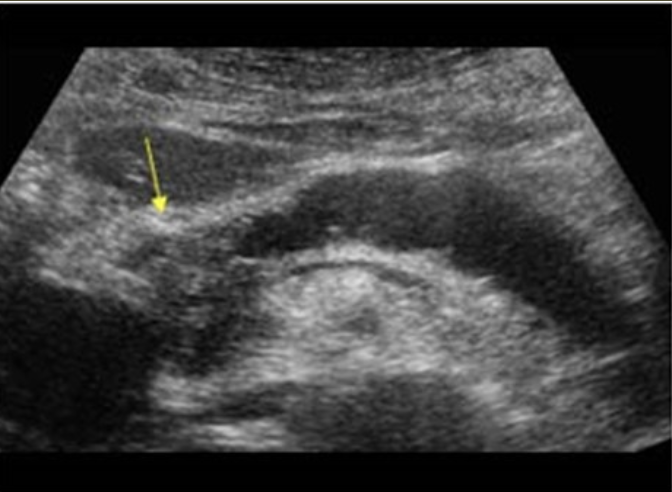
Simple Renal Cyst → common lesion of kidney, fluid-filled sac (benign, Bozniak 1)
clinical hx: incidence increases with age (50+), uncommon in children
s/sx: asymptomatic
2D US: anechoic, well-defined smooth, thin wall, round or ovoid, posterior enhancement
color doppler: avascular
DDX: complex cyst

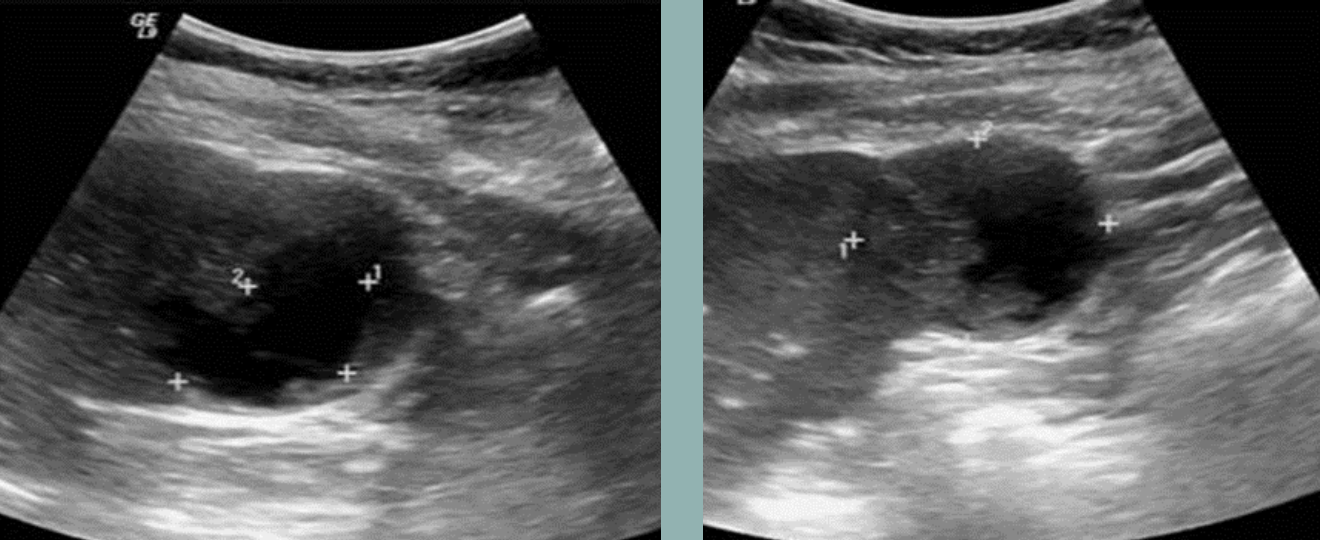
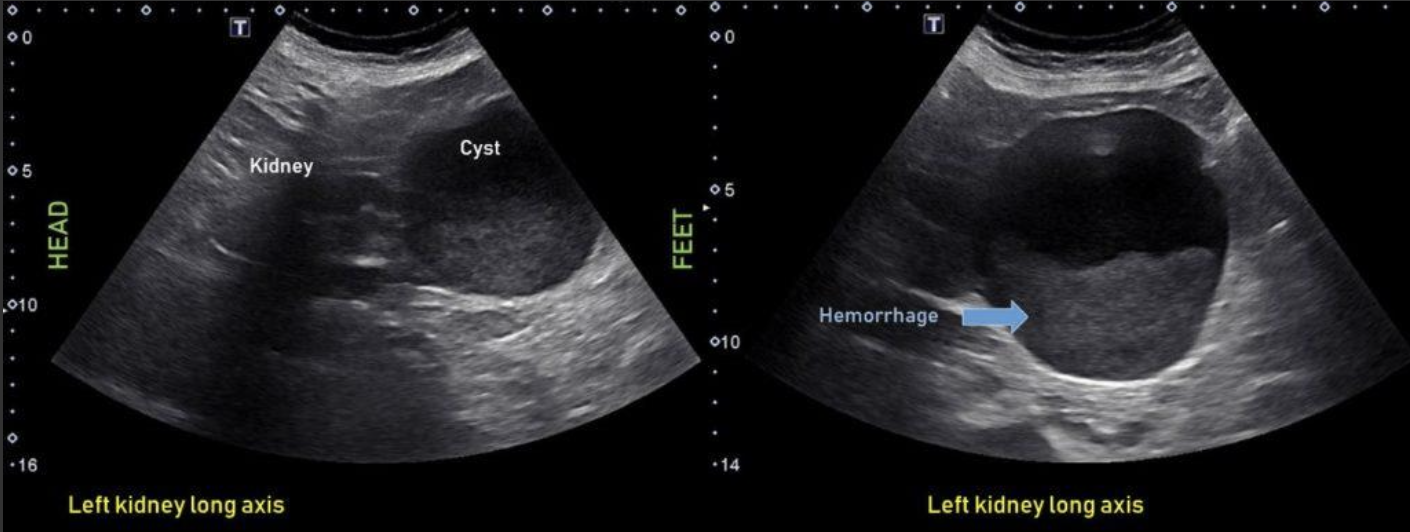
Complex Renal Cyst → any cyst that is not a simple cyst
clinical hx: post-surgery, trauma
s/sx: flank pain, fever, hematuria, WBC increase, can be asymptomatic
2D US: well-defined cystic structure, internal echoes or anechoic, septations, focal hypoechoic inner mural extension, can be hemorrhagic
color doppler: if solid can have vascularity
DDX: malignant tumor, RCC
Milk of Calcium Cyst → calcium buildup in cortex
clinical hx: older, stasis, metabolic issues
s/sx: asymptomatic
2D US: echogenic layering/sediment, posterior revirberations
color doppler: twinkle artifact
DDX: renal calculi
Parapelvic Cysts → renal cysts adjacent to sinus
clinical hx: older age
s/sx: asymptomatic
2D US: no communication w/ collecting system, well-defined anechoic renal sinus cysts, can be multiple, does not follow kidney shape, random distribution, varying size
color doppler: avascular
DDX: hydronephrosis
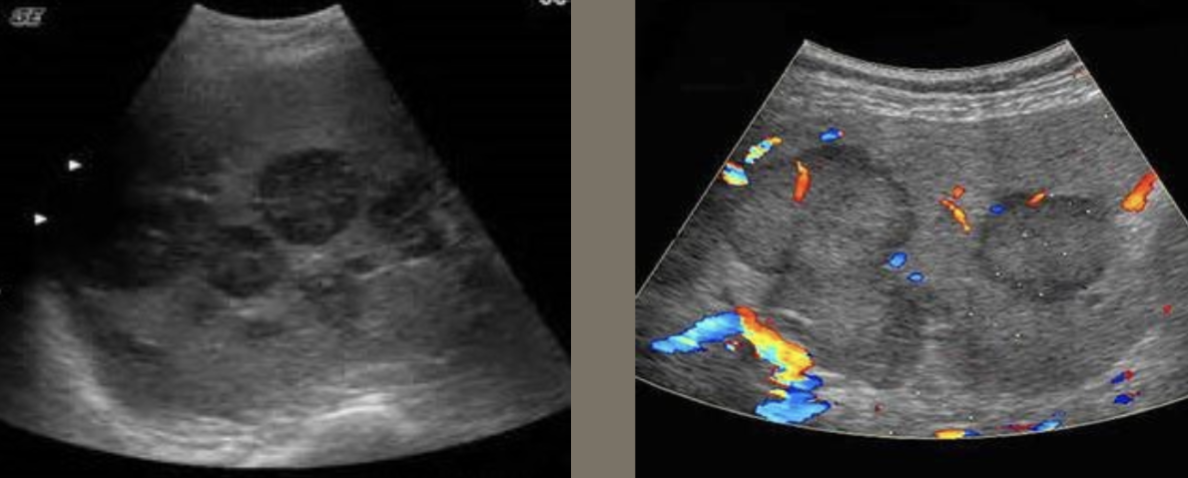
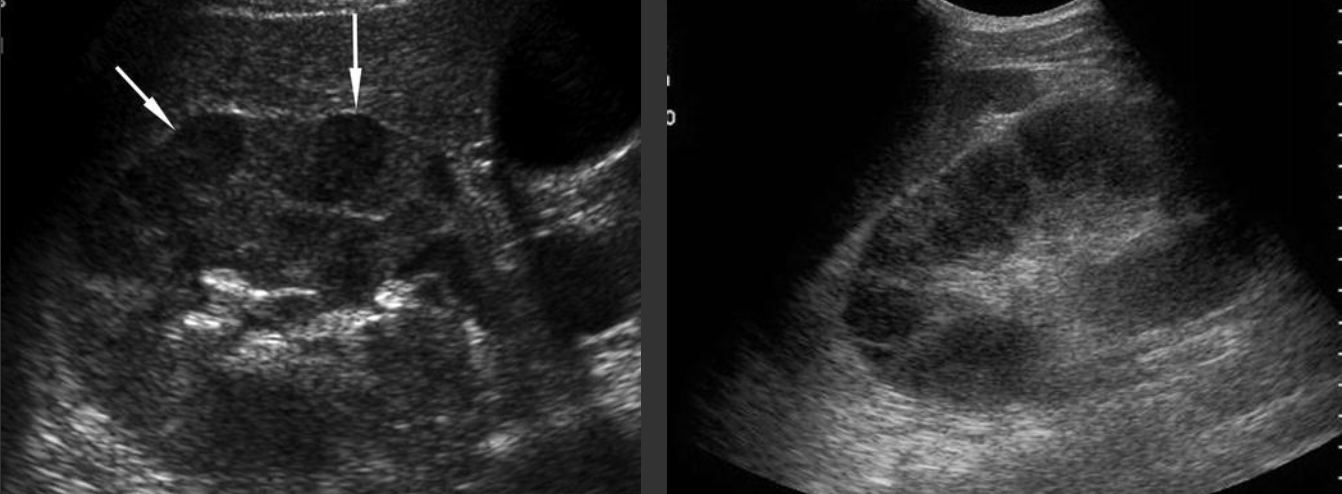
ADPKD (Autosomal Dominant Polycystic Kidney Disease ) → most common hereditary kidney disorder
clinical hx: 30 y/o develops, associated with polycystic liver disease
s/sx: HTN, palpable masses, swollen abdomen, pain w/ rupture, bouts with kidney stones
2D US: bilateral cortical/medullary cysts, varying sizes, simple/hemorrhagic, enlarged bilateral kidneys, normal tissue replaced with cysts,
color doppler: focal echogenic vascular lesion in background of PKD
DDX: parapelvic cysts, hydronephrosis
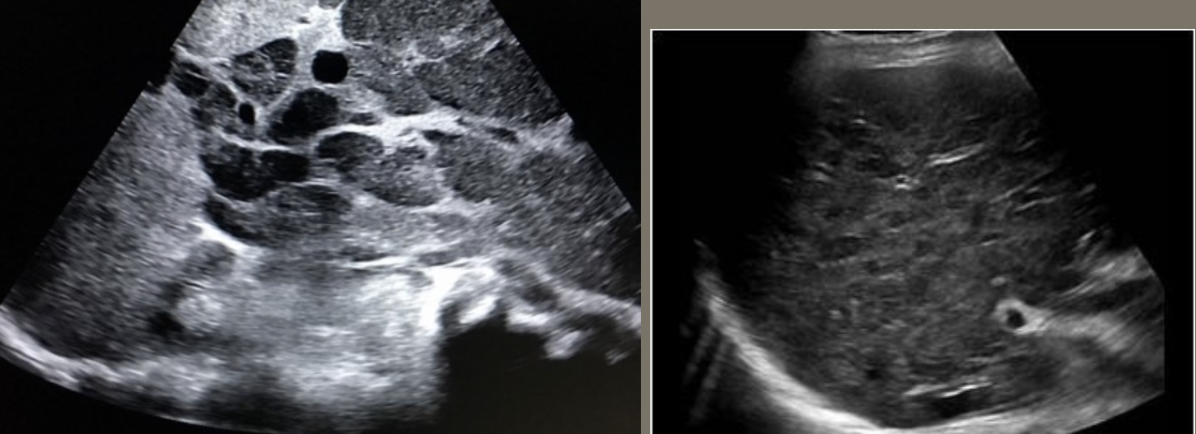
ARPKD (Autosomal Recessive Polycystic Kidney Disease) → dilated renal collecting tubes
clinical hx: presents in newborns
s/sx: failure to thrive (newbors)
2D US: bilateral enlarged kidneys, echogenic, small cystic changes (1-2 mm)
color doppler: loss of cortical medullary interface
DDX: MCDK
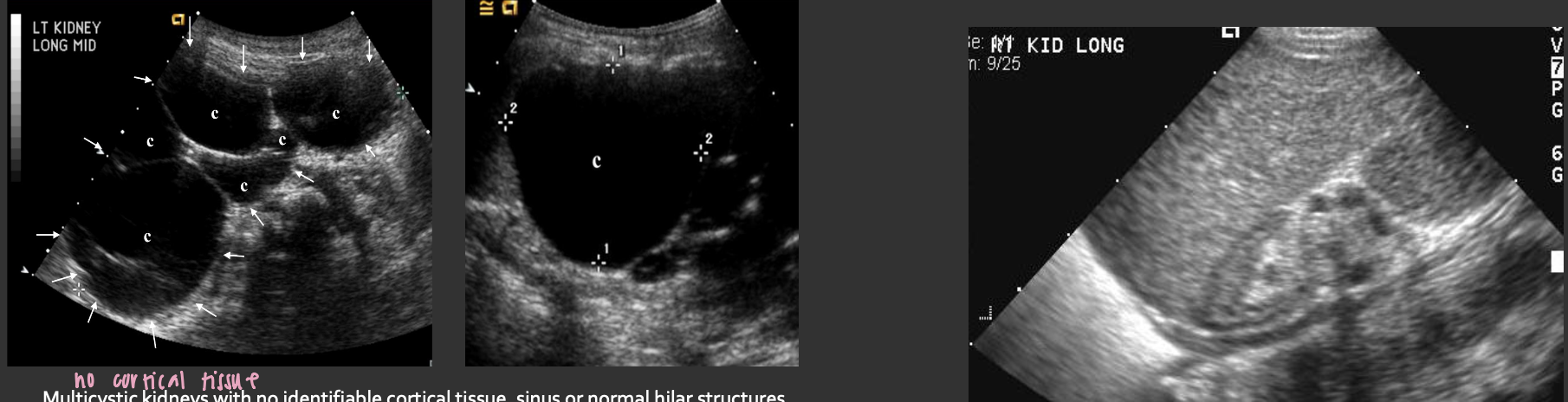
MCDK (Multicystic Dysplastic Kidney) → common acquired renal dysplasia
clinical hx: male
s/sx: asymptomatic
2D US: unilateral (bilateral incompatible with life), multiple non communicating cysts, absence of normal cortex and sinus, initially → enlarged kidney, in adults → atrophic kidney that may become calcified
color doppler: avascular
DDX: ADPKD
Acquired Cystic Kidney Disease → due to chronic renal failure
clinical hx: dialysis, chronic renal failure risk for RCC
s/sx: asymptomatic
2D US: 3-5 small cysts in each kidney, atrophied, echogenic kidneys, ± internal echoes fro hemorrhage
color doppler: solid vascular tumor
DDX: ADPKD

Retroperitoneal Hematoma → bleeding from trauma or surgery
clinical hx:
s/sx: hematuria, sudden constant flank pain, AKI
2D US: poor differentiation from cortex, hematoma variable appearance, can have mass effect on kidney
color doppler: avascular
DDX: renal abscess, infected cyst

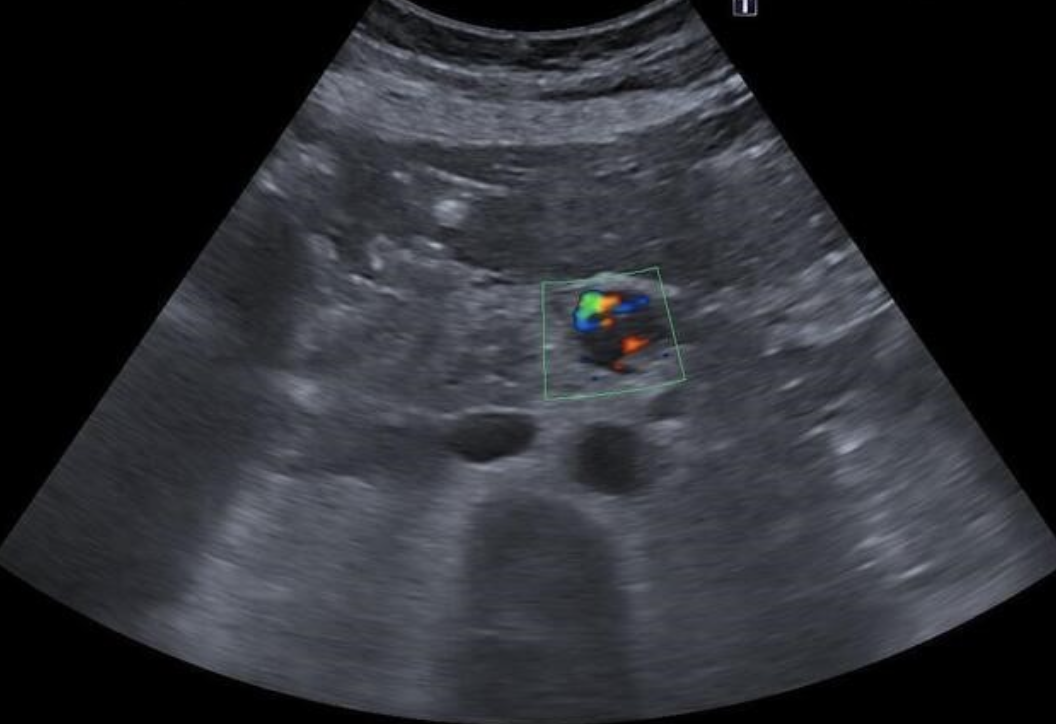
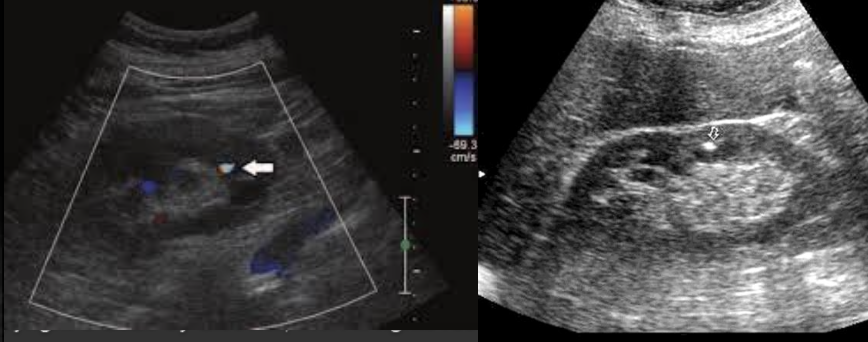
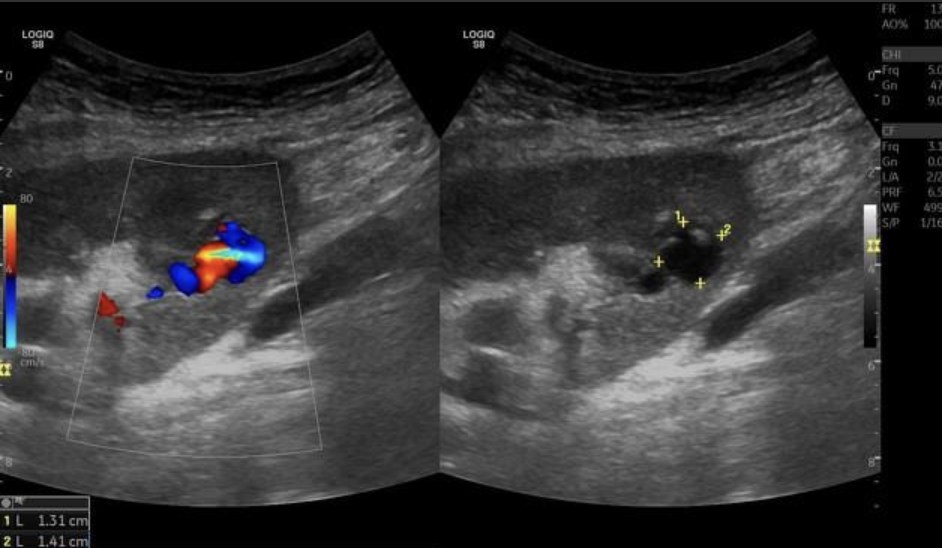
AVF (Arteriovenous Fistula) → abnormal connection between artery and vein in kidney
clinical hx: congenital, iatrogenic, spontaneous
s/sx: hematuria, flank pain, abdominal bruit
2D US: cystic space
color doppler: focal aliasing
DDX: aneurysm
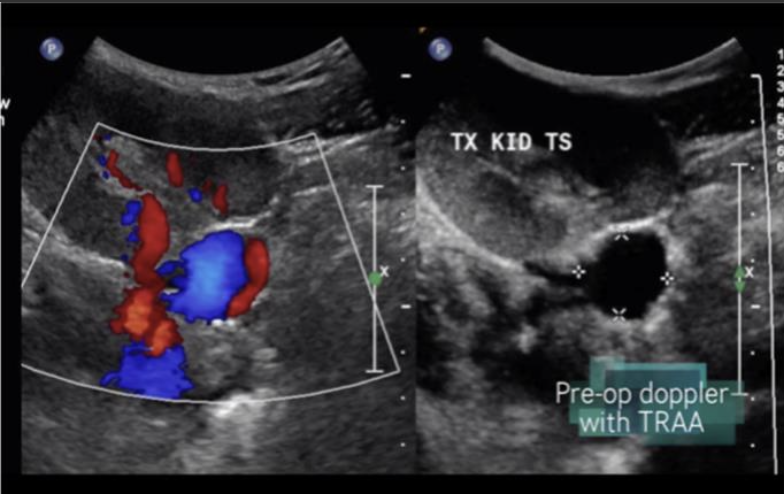
Renal Artery Aneurysm → focal dilation of renal artery
clinical hx: congenital, inflammatory disease
s/sx: asymptomatic
2D US: cystic mass medial to renal hilum, connection to main artery
color doppler: helical flow
DDX: AVF
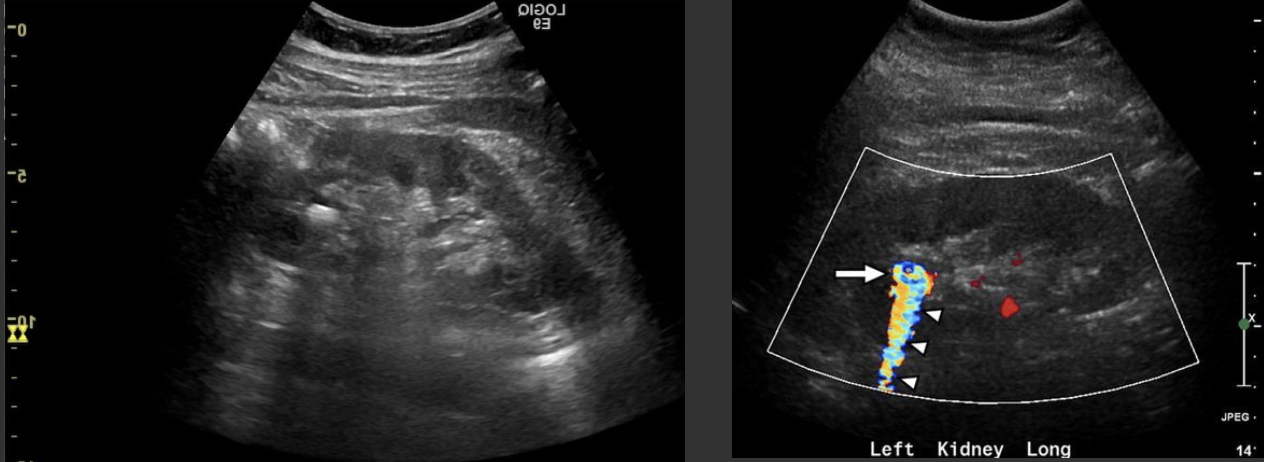
Renal Artery Stenosis → narrowing of renal artery
clinical hx: older adults, smoking, DM
s/sx: HTN that doesn’t respond to normal medical treatment
2D US: usually unilateral, compare affected kidney to unaffected, kidney is significantly smaller than contralateral kidney
color doppler: increased velocity in artery
DDX: atherosclerosis renal artery aneurysm

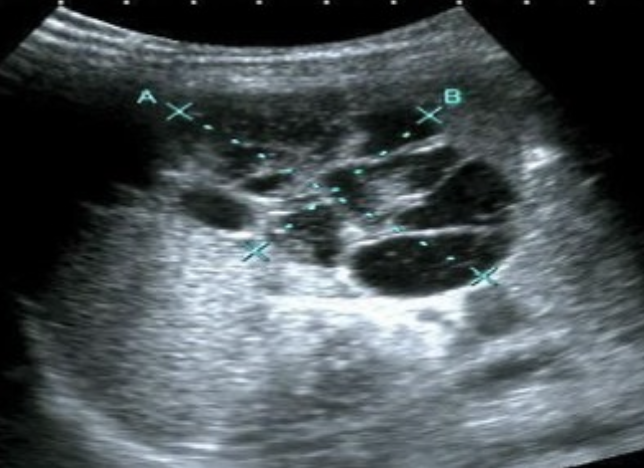
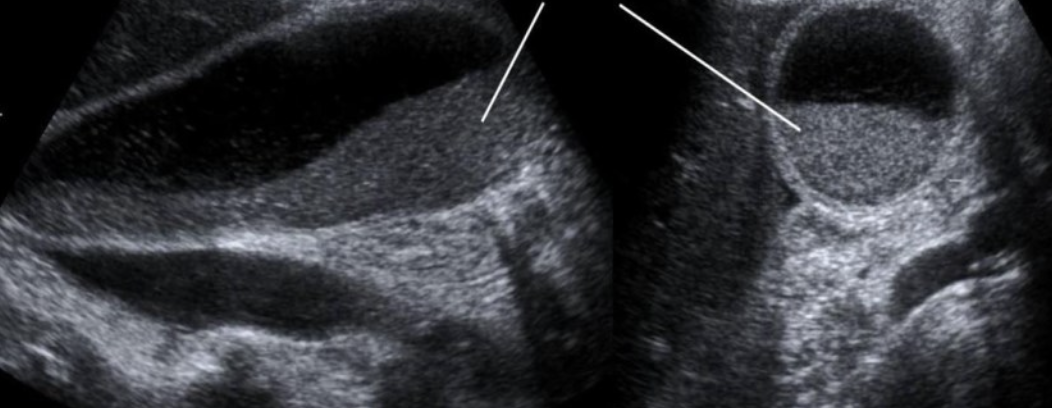
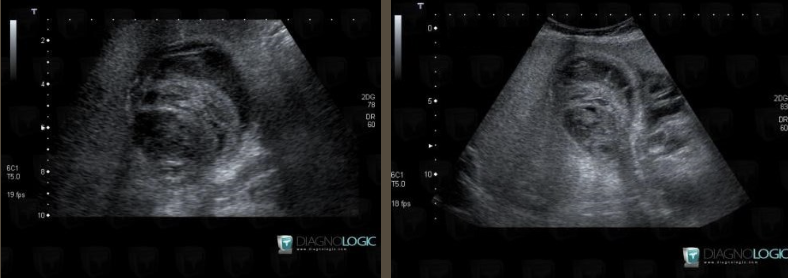
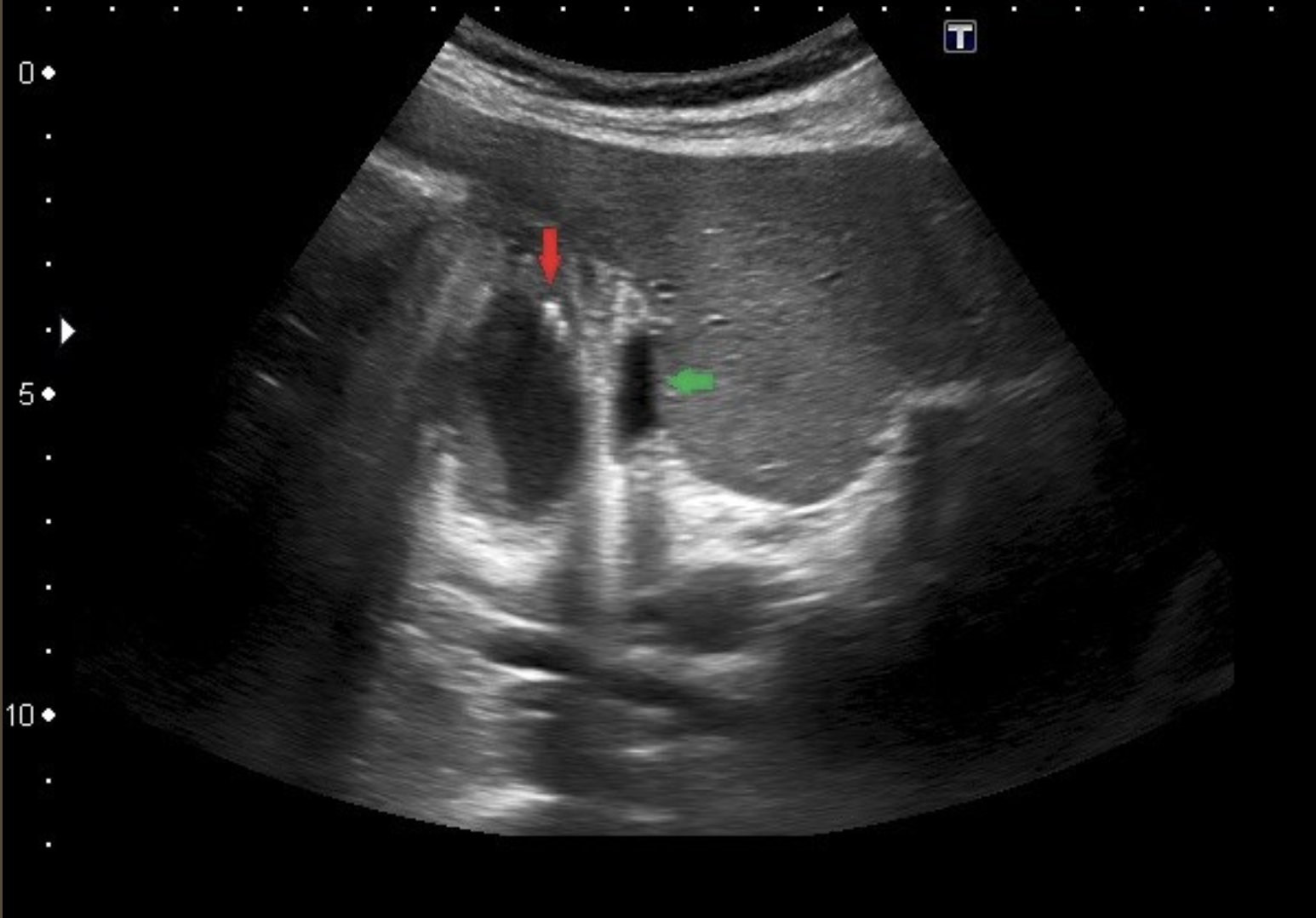
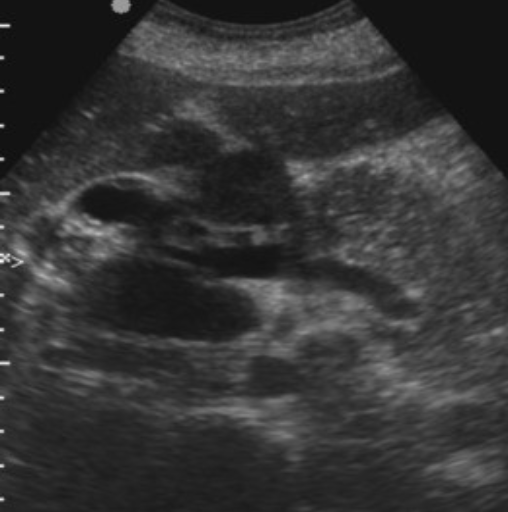
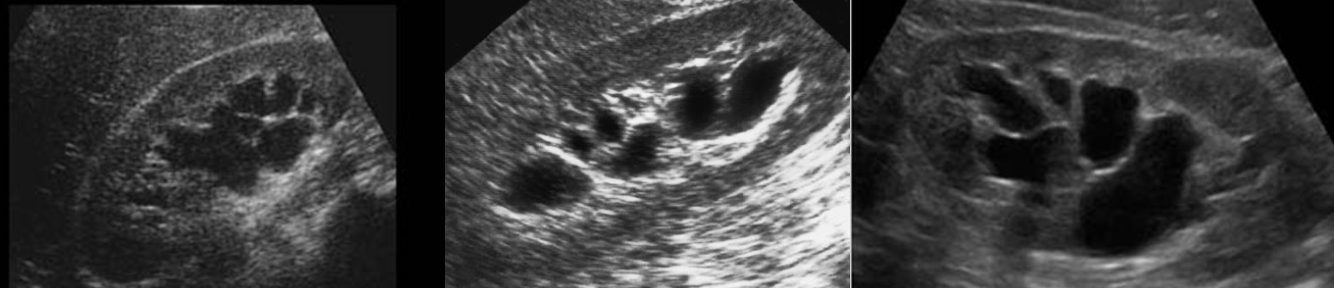
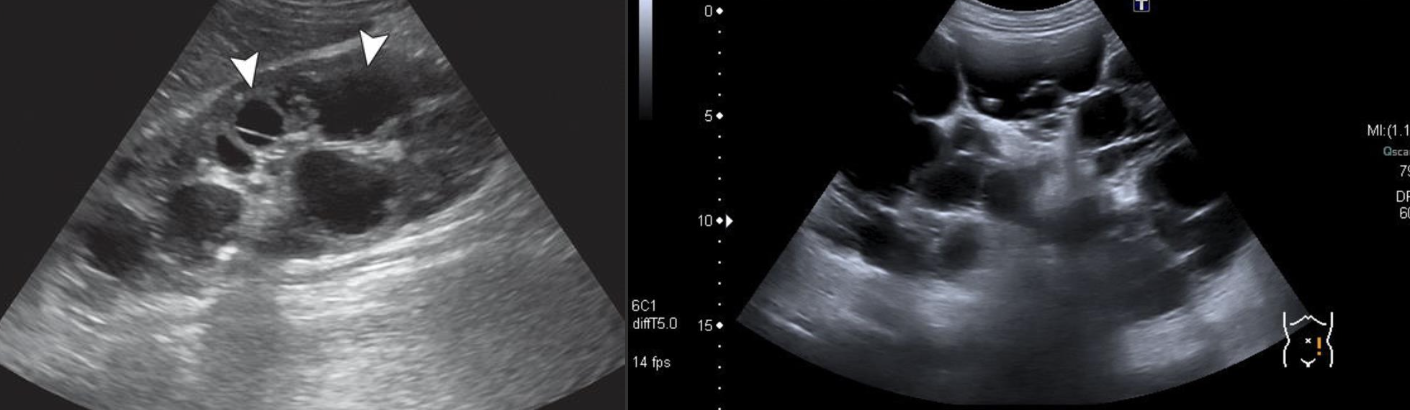
Hydronephrosis → dilation of renal collecting system from mechanical obstruction or functional dysfunction (calculi, mass, trauma, pregnancy)
clinical hx: prone to stones (stasis, pregnancy)
s/sx: if stone → renal colic, N&V, hematuria, frequency/urgency
2D US: grade 1 (mild) → pelviectasis, cortex preserved, grade 2 (mild to moderate) → expands into major calyces, cortex preserved, grade 3 (moderate) → expand all calyces, entire pelvis dilated, cortex preserved, grade 4 (severe) → cortical thinning, AKI to CKD, creatinine >1.2
color doppler: avascular
DDX: parapelvic cysts

Nephrolithiasis → very common, calculi
clinical hx: increase incidence with age, associated with underlying kidney anomalies, diet, steroids, medication , family hx
s/sx: renal colic when stone moves down ureter, hematuria, WBC increase from stone passing
2D US: echogenic foci, rounded surface, posterior shadowing
color doppler: twinkle artifact
DDX: milk of calcium cyst (location differs)
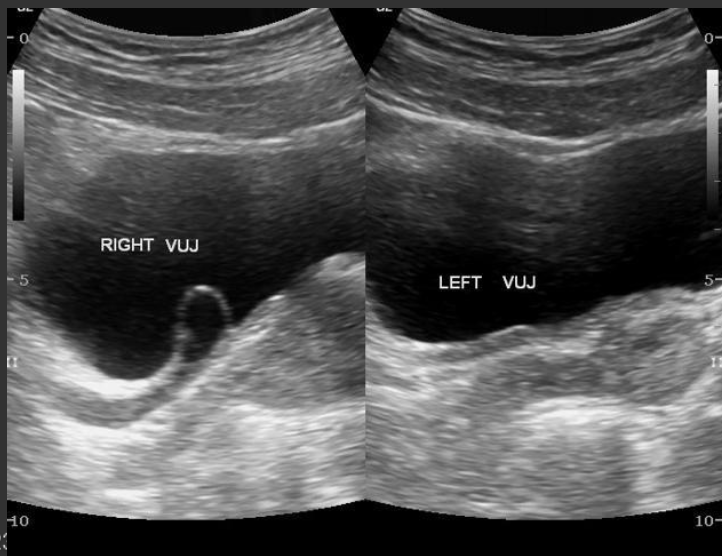
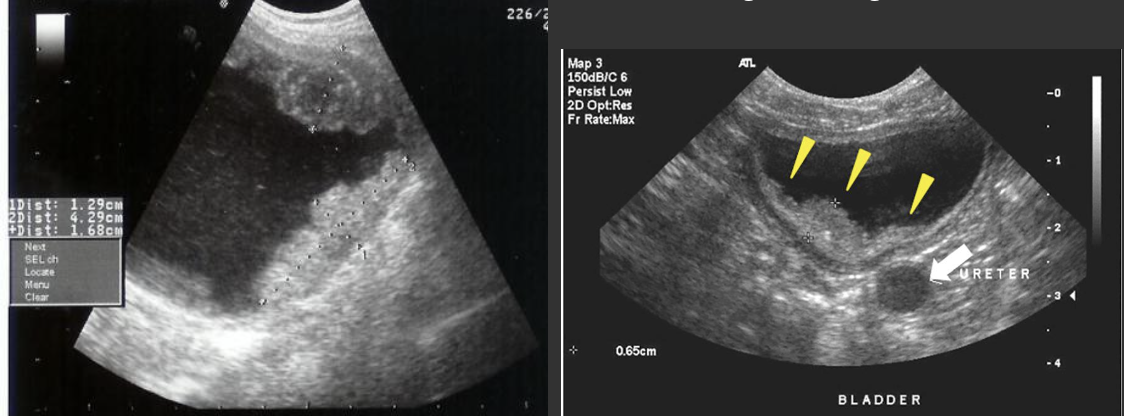
Hydroureter → dilation of the ureter from BOO, ureter mass, gravida uterus, uterine fibroid compression
clinical hx: pregnancy, BPH (older males), nephrolithiasis prone (pregnancy, stasis)
s/sx: renal colic, symptoms mimic UTI (frequency, urgency)
2D US: dilated ureter at UVJ
color doppler: avascular
DDX:

VUR (Vesicoureteral Reflex) → common, non-obstructive cause of hydronephrosis (reflux of urine from bladder back up ureters into kidney)
clinical hx: history of recurrent infections, young children
s/sx: dysuria, frequency, urgency, fever, abdominal pain
2D US: hydronephrosis, intermittent dilations of collecting system (post-void changes), displaced ureteral jet in bladder, ureterocele (ballooning of lining of ureter into bladder)
color doppler: avascular
DDX:
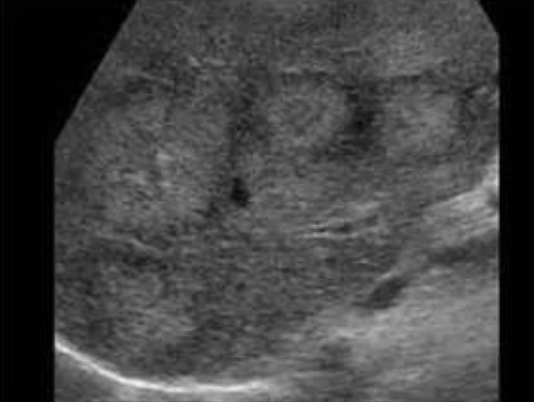
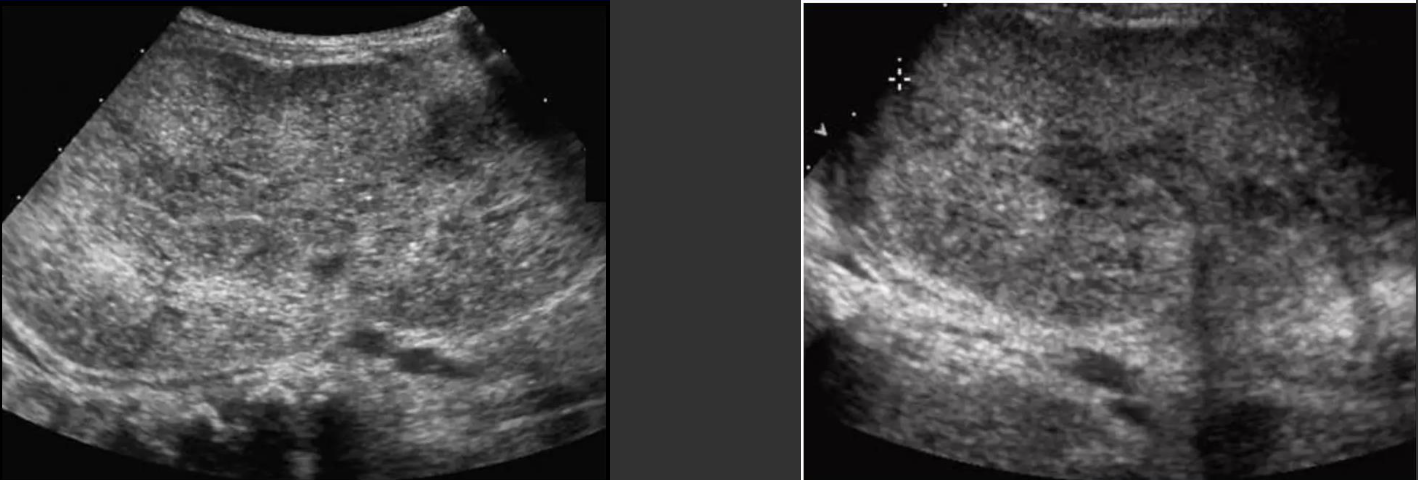
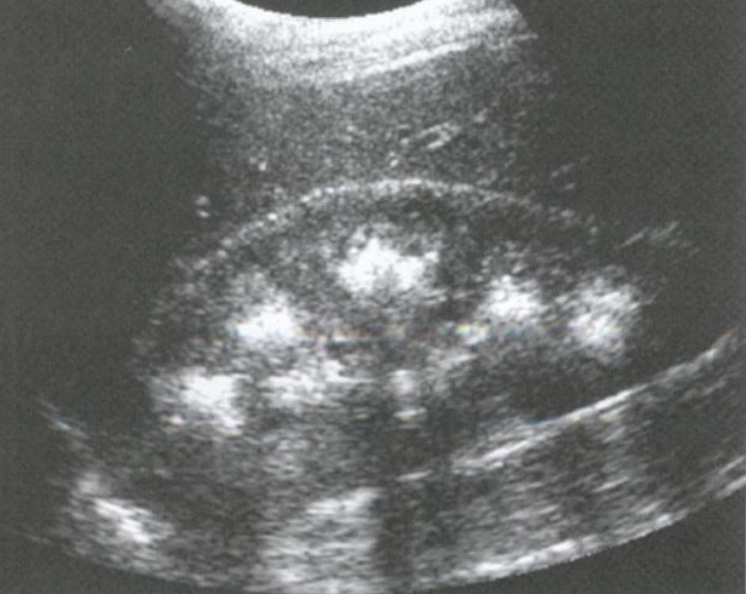
Nephrocalcinosis → calcium deposits in kidney parenchyma
clinical hx: chronic glomerulonephritis (cortex), hyperparathyroidism (medullary, more common)
s/sx: asymptomatic
2D US: pyramids more echogenic than cortex, echogenic halo around pyramids
color doppler: avascular
DDX:
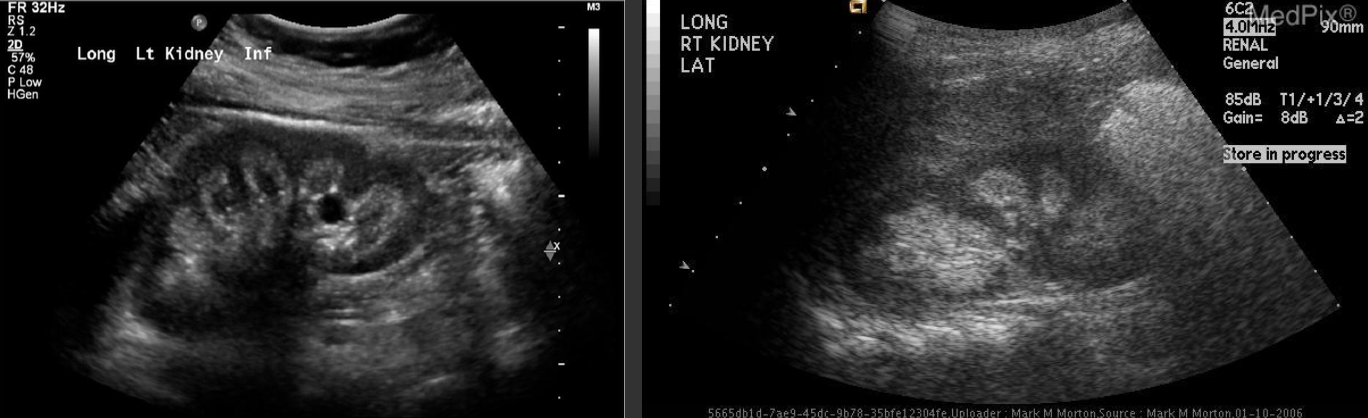
MSK (Medullary Sponge Kidney) → congenital, rare dilated collecting tubes, causes recurrent stones
clinical hx: recurrent nephrolithiasis, hematuria, flank pain, renal colic
s/sx:
2D US: unilateral, small anechoic dilations in papillary zone, multiple diffuse hyperechoic calcifications, nephrocalcinosis, focal clusters of echogenic foci with shadowing in pyramids
color doppler: avascular
DDX: Nephrocalcinosis
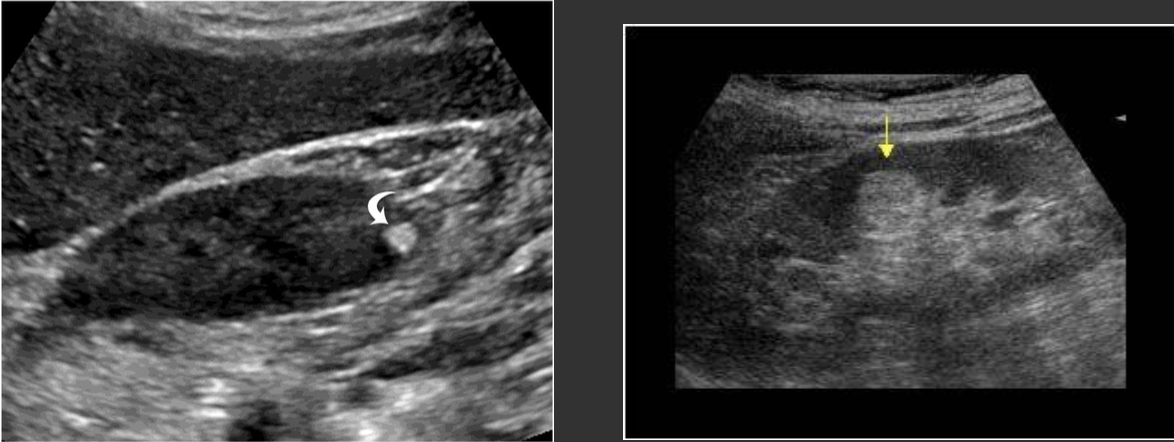
AML (Angiomyolipoma) → most common benign tumor of kidney
clinical hx: more common in females, right side more common, associated with tuberous sclerosis
s/sx:
2D US: well-defined, hyperechoic spherical lesion, typically echogenic but can be more hypoechoic if hemorrhage
color doppler:
DDX: RCC, renal lipoma
Sinus Lipomatosis → excessive renal fat proliferation
clinical hx: aging, obesity, steroids
s/sx: mild flank pain
2D US: highly echogenic enlarged sinus
color doppler: avascular
DDX:

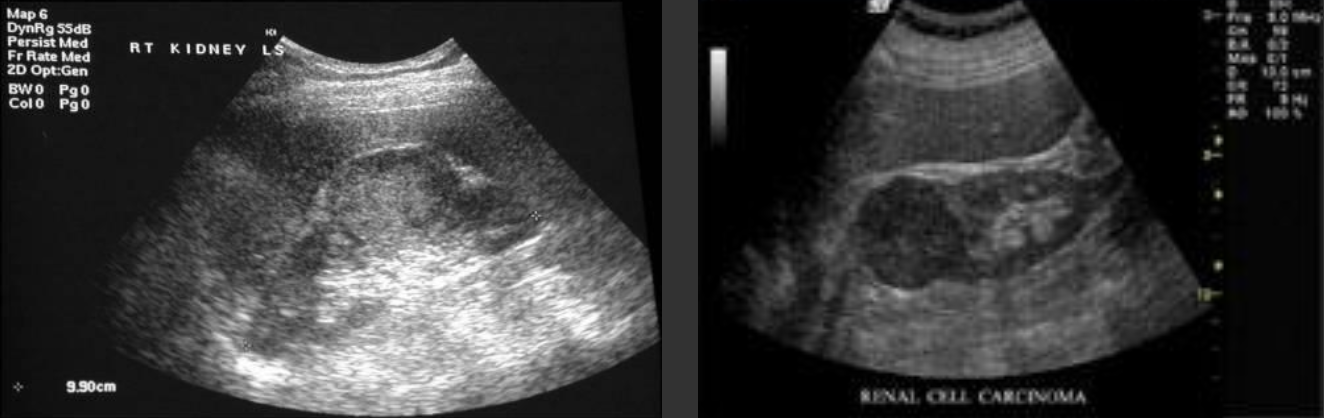
RCC (Renal Cell Carcinoma) → most common primary malignant tumor of the kidney
clinical hx: male, late middle age, smoking, ACDK, von Hippel Lindau, Tuberous sclerosis
s/sx: microscopic hematuria
2D US: solid, usually isoechoic but can vary, renal vein and IVC involvement, typically solitary and invades into surrounding vasculature
color doppler: vascular
DDX: AML, TCC
TCC (Transitional Cell Carcinoma) → usually in bladder, 90% of collecting system renal tumors
clinical hx: heavy smoking, men, 65+
s/sx: gross hematuria, flank pain if obstructive
2D US: renal sinus hypoechoic mass, irregular bladder wall, collecting system dilation if trigone involved
color doppler: vascular in renal tumor
DDX:
Lymphoma → renal involvement, usually bilateral
clinical hx: AIDS
s/sx: ± flank pain
2D US: kidney may be enlarged, loss of renal sinus pattern, perirenal hypoechoic lobular mass, small hypoechoic parenchymal lesions
color doppler:
DDX:
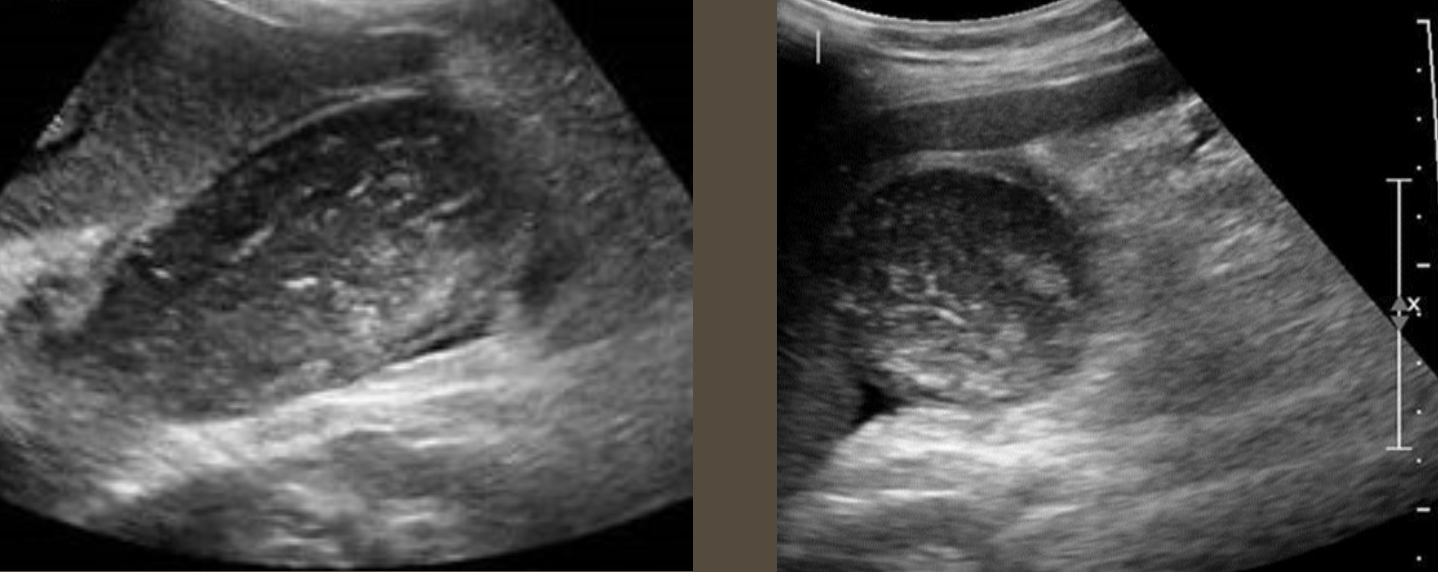
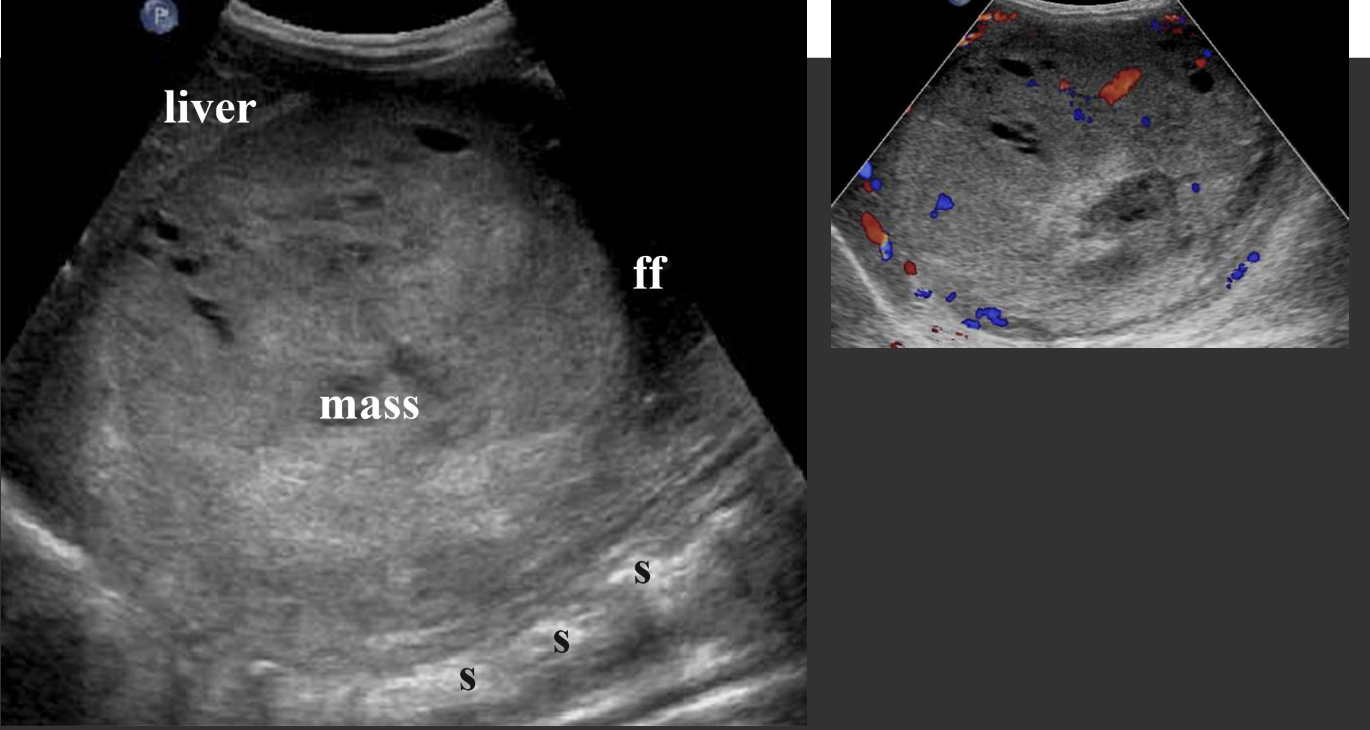
Nephroblastoma (Wilm’s Tumor) → 2nd most common peds abdominal cancer
clinical hx: 2-5 years, unilateral, Beckwidth-Wiedmann
s/sx: abdominal swelling, abdominal pain
2D US: vascular involvement, large solid mass, distorts renal cortex, sinus, pyramids and contour, hydronephrosis, extension into renal vein, IVC, contralateral kidney, homogenous to complex, calcifications, well-defined
color doppler: hypovascular/vascular
DDX: neuroblastoma, hepatoblastoma
Acute Pyelonephritis → acute infection of urinary tract, usually begins in bladder and ascends ureters
clinical hx: stones, tumors, E. coli, female
s/sx: UTI symptoms, fever, persistent flank pain, leukocytosis
2D US: thickening of renal pelvis, cortex appearance varies (normal, hypoechoic, patchy), as abscess develops → mixed echogenic pattern in parenchyma
color doppler: avascular in region of involvement
DDX: