Acute and Emergency Dermatology
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
consequences of failure of mechanical barrier to infection
sepsis
consequences of failure of temperature regulation
hypo and hyperthermia
consequences of failure of fluid and electrolyte balance
protein and fluid loss
renal impairment
peripheral vasodilation
causes of erythroderma
•“Any inflammatory skin disease affecting >90% of total skin surface”
causes of erythroderma
–Psoriasis
–Eczema
–Drugs
–Cutaneous Lymphoma
–Hereditary disorders
–Unknown
principles of management of erythroderma
•Appropriate setting - ITU or burns unit
•Remove any offending drugs
•Careful fluid balance
•Good nutrition
•Temperature regulation
•Emollients – 50:50
•Oral and eye care
•Anticipate and treat infection
•Manage itch - antihistimine
•Disease specific therapy; treat underlying cause
drug reactions
•Can occur to any drug
•Commonly 1-2 weeks after drug
–Within 72 hours if re-challenged
mild drug reaction
–Morbilliform exanthem
macular rash

severe drug reaction
Erythroderma
Stevens Johnson Syndrome/Toxic epidermal necrolysis,
DRESS
which drugs commonly cause Stevens Johnson Syndrome/Toxic epidermal necrolysis
–Antibiotics
–Anticonvulsants
–Allopurinol
–NSAIDs
Stevens Johnson Syndrome
•Fever, malaise, arthralgia
•Rash
–Maculopapular, target lesions, blisters
–Erosions covering <10% of skin surface
•Mouth ulceration
–Greyish white membrane
–Haemorrhagic crusting
•Ulceration of other mucous membranes
Toxic epidermal necrolysis
•presents with prodromal febrile illness
•Ulceration of mucous membranes
•Rash
–May start as macular, purpuric or blistering
–Rapidly becomes confluent
–Sloughing off of large areas of epidermis – ‘desquamation’ > 30% BSA
–Nikolsky’s sign may be positive
management of Stevens Johnson Syndrome/Toxic epidermal necrolysis
•Identify and stop culprit drug as soon as possible
•Supportive therapy
long term complications of Stevens Johnson Syndrome/Toxic epidermal necrolysis
–Pigmentary skin changes
–Scarring
–Eye disease and blindness
–Nail and hair loss
–Joint contactures
erythema multiforme
presentation + management
•Hypersensitivity reaction usually triggered by infection
–Most commonly HSV, then Mycoplasma pneumonia
•Abrupt onset of up to 100s of lesions over 24 hours
–Distal proximal
–Palms and soles
–Mucosal surfaces (EM major)
–Evolve over 72 hours
•Pink macules, become elevated and may blister in centre
•“Target” lesions
•Self limiting and resolves over 2 weeks
•Symptomatic and treat underlying cause
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
•Onset 2-8 weeks after drug exposure
•Fever and widespread rash
•Eosinophilia and deranged liver function
•Lymphadenopathy
•+/- other organ involvement
management of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
•Stop causative drug
•Symptomatic and supportive
•Systemic steroids
•+/- Immunosuppression or immunoglobulins
pemphigus
•Antibodies targeted at desmosomes
•Skin – flaccid blisters, rupture very easily
•Intact blisters may not be seen
•Common sites – face, axillae, groins
•Nikolsky’s sign may be +ve
•Commonly affects mucous membranes
•Ill defined erosions in mouth
•Can also affect eyes, nose and genital areas

pemphigoid
•Antibodies directed at dermo-epidermal junction
•Intact epidermis forms roof of blister
•Blisters are usually tense and intact

pemphigus vs pemphigoid
•Pemphigus.
–Uncommon
–Middle aged patients
–Blisters very fragile – may not be seen intact
–Mucous membranes usually affected
–Patients may be very unwell if extensive
–Treat with systemic steroids. Dress erosions. Supportive therapies
•Pemphigoid
–Common
–Elderly patients
–Blisters often intact and tense
–Even if extensive, patients are fairly well systemically
–Topical steroids may be sufficient if localised; systemic usually required if diffuse
common causes of Erythrodermic psoriasis and Pustular Psoriasis
–Infection
–Sudden withdrawal of oral steroids or potent topical steroid
Erythrodermic psoriasis and Pustular Psoriasis
•Can occur without previous history of psoriasis
•Rapid development of generalised erythema, +/- clusters of pustules
•Fever, elevated WCC
•Exclude underlying infection, bland emollient, avoid steroids
•Often require initiation of systemic therapy
Eczema Herpeticum
•Disseminated herpes virus infection on a background of poorly controlled eczema
•Monomorphic blisters and “punched out” erosions
–Generally painful, not itchy
•Fever and lethargy
•In adults consider underlying immunocompromise
treatment of Eczema Herpeticum
•Treatment dose Aciclovir
•Mild topical steroid if required to treat eczema
•Treat secondary infection
•Ophthalmology input if peri-ocular disease
Staphylococcal Scalded Skin Syndrome
•Initial Staph. infection
–May be subclinical
•Diffuse erythematous rash with skin tenderness
•More prominent in flexures
•Blistering and desquamation follows
–Staphylococcus produces toxin which targets Desmoglein 1
•Fever and irritability
who is Staphylococcal Scalded Skin Syndrome seen in
•Common in children, can occur in immunocompromised adults
treatment of staphylococcal scalded skin syndrome
•Require admission for IV antibiotics initially and supportive care
•Generally resolves over 5-7 days with treatment
urticaria
•Weal, wheal or Hive:
–Central swelling of variable size, surrounded by erythema. Dermal oedema
–itching, sometimes burning
•Histamine release into dermis
–fleeting nature, duration: 1- 24 hours
•Angioedema
–Deeper swelling of the skin or mucous membranes

acute urticaria
<6 week history
•Idiopathic
–50%
•Infection, usually viral
–40%
•Drugs, IgE mediated
–9%
•Food, IgE mediated
–1%
treatment of acute urticaria
•Oral antihistamine
–Taken continuously
–Up to 4 x dose
•Short course of oral steroid may be of benefit if clear cause and this is removed
why avoid opiates and NSAIDs in urticaria
exacerbate urticaria
chronic urticaria
> 6 week history
•Autoimmune/Idiopathic
–60%
•Physical
–35%
•Vasculitic
–5%
•Rarely a Type 1 hypersensitivity reaction
management of chronic urticaria
(the image)
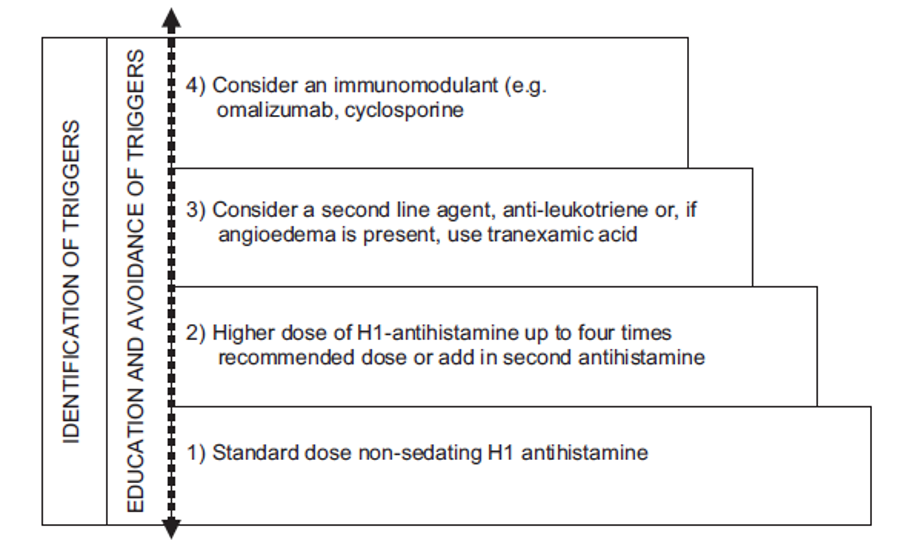
use of omalizumab
•Monoclonal antibody to IgE, mechanism of action unknown
•Licensed for use in chronic spontaneous urticaria
•300mg S/C ever 4 weeks