maternity chpt 12-14
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
physiologic changes in breasts
after delivery, estrogen and progesterone decrease and prolactin increases
prolacitn stims breast milk production
hen infant suckles, the posterior pituitary releases oxytocin, resulting in the milk ejection reflex (let down reflex)
post partum assessment of breasts
examine whether or not mother is breastfeeding
observe size, symmetry, and shape
assess for flat or retracted nipples
assess for signs of nipple trauma if breastfeeding
palpate for firmness or tenderness
expected findings of PP breast assessment
breast fullness is normal immediately after delivery
it is soft and nontender
~3rd PP day, both breastfeeding and nonbreastfeedign pts experience some degree of primary breast engorgement
incr vascular and lymphatic system of the breasts recedes milk production
breasts become larger, firm, warm, and tender, she may feel throbbing pain in breasts
primary engorgement subsides eithin 24-48 hrs
deviations from normal PP breast assessments
signs of irritation and tissue breakdown are cracked, blistered, r reddened areas
skin breakdown of nipples is often associated with an improper infant latch
nipple soreness is a rimary reason that women stop breastfeeding, so this complaint should b addressed
skin breakdown allows entery for bacteria
nursing action of breasts: for nonreastfeeding pt education
avoid stimulating breast
ice packs to breasts (lettuce cold)
analgesics for pain management
subsides within 48-72 hrs
“how are you breastfeeding the baby”
nursing action of breasts: for breastfeeding pt education
frequent feedings to empty the breatss and to prevent milk stasis
warm compresses to breast and breast massage to facilitate the flow of milk before feeding sessions
express milk by breast pump or manually if the infant is unable to nurse (i.e. preterm infant)
ice packs after feedings to reduce inflammation and discomfort
analgesics for pain man.
when does masitis occur
incidence: occurs most often 3 months after birth, 2-10% of women are affected
etiology of mastitis/how is it caused
caused by staphylococcus aureus
engorgement and stasis of milk
contrisction of breatss by a bra that is too tight
fatigued mother or has health problems that lower immune system
assessment findings of mastitis
breast tenderness or warmth to the touch
generally feeling ill (malaise) or muscle ache
breast swelling and hardness
pain or a burning sensation continuously or while breastfeeding
skin redness, often in a wedge shaped pattern
fever of 101 or greater
med management of mastitis
oral antibiotics x10-14 days
culture expressed milk from affected breasted if infection does not resolve
untreated mastitis may progress to abcess
pt teaching on risk reduction of mastitis
complete emptying breast and good breastfeeding techniques
postpartum nurse must teach breastfeeding techniques
encouraged to avoid missed feedings
wash hands before feeding
decreased nipple irritation and tissue breakfwon
use more than one breatsfeeding position
air dry nipples after feeding
feed on unaffected side first, then on affected so then you have lactation let down from affected side
physiologic changes in cardiovascular system
average blood loss from vaginal birth: 200-500 mL
increased flow of blood back to the heart
decreased pressure from pregnant uterus on the bessels
mobilization of excess extracellular fluid into the vascular compartment
cardiac output is elevated for 24-48 hours after delivery and returns to prepregnant levels within 10 days
what is diuresis and diaphoresis
increasd excretion of irome
urinary output increased in pp period of up to 3,000 mL/day
nursing consideration
diaphoresis (pofuse perspiration)
phys changes: cardiovascular - what are 2 hematologic system changes
leukocytosis
hemoglobin and hematocrit
what is leukocytosis
incr. WBC as high as 30,000/mm3 during labor and immediately pp
return to normal within 6 days after birth
what is hemoglobin and hematorcit and wy is it difficult to interpret
decr in Hgb bc of blood loss
low Hct due to plasma that dilutes the concentration of blood cells
return to normal within 4-6 wks
phys changes: cardio - hypercoagulable state
pt is still in a hypercoagulable state during the postpartum period
new mothers are increased risk for thrombus formation
elevations in clotting factors cause continued risk of thrombus formation
hemostasis returns in 4-6 wks
pp assessment for cardiovascular
q15 mins for first hour of delivery
q30 mins for second hour of delivery
q4 hrs for next 22 hrs
every shift sfter the first 24 hours or as stated in hospital or unity protocols
expected findings of pp assessment cardio
P& BP within normal ranges, after delivery systolic and diastolic BP may show a transient 5% elevation
bradycardia may occur postdelivery and in the early PP period, and is considered normal
pp assessment of cardio, assess temp and prescence of chills: expected
expected findings:
offered warm blanket and reassure it is normal
pp assessment of cardio, assess temp and prescence of chills: deviations from normal
women with elevated temp should be eval. further for possible infection, and the physician or midwife needs to be notified
pp assessment for cardiovascular
assess lower extremities for venous thrombosis
assess calves and groin area for tenderness, edema, and sensation of warmth each shift
compare pulses in both extremiies
measure the calf width if thromboembolism is suspected
expected cardiovascular findings during PP assessment
no tenderness or feelin of warmth
deviatons fro normal findings in cardiovascular PP assessment
symptoms of deepvein thrombosis include:
muscle pain
tenderness
redness or incr. warmth to touch
palpatin of a hard, cord like vessel
swellin of veins
edema
decreased blood circulatin to the affeced area
complications of venous thromboembolic disease
VTE a blood clot that starts in a vein; risk highest during pregnancy but extends though the 12th week pp
2 types of venous thromboembolic disease
deep vein thrombosis - clot deep in vein, in the leg, sometimes in arm or other veins
pulmonary embolism - DVT clot break free from a vein wall, travels to lungs, blocks blood supply
risk factors of venous thromboembolic disease unrelated to pregnancy
personal history of VTE
thrombophilia
obesity
cancer
smoking
immobility
trauma
infection
how does venous thromboembolic disease present in pregnancy
5x moe than nonpregnant women d/t:
venous stasis inlower extremiies
incr. blood volume
compression of inferior vena cava and pelvic veins with advancing gestation
nursing action to prevent thrombus formation
decreased risk with early ambulation
sequential compression device
anti-embolism stockins
nursing care of thrombophlebitis (cardiovascular)
apply supportive bandage or antiembolic stockings
apply a warm pack to the affected area
slightly elevated involved leg
perform serial measurements of circumference of calves; a circumference difference of more than 2 cm is classified as leg swelling
monitor vitals signs every 4 hours; there may be a slight increase in temperature
heparin anticoagulation therapy may be ordered
physiologic: respiratory - how to assess
Assess respiratory rate:
q15 mins for first hour
q30 mins for second hour
q4 hrs for the next 22 hours
every shift after the first 24 hours or as stated in hospital or unit protocols
Assess breath sounds
who is at risik for pulmonary edema
women who received oxytocin, large amounts of IV fluids, tocolytics such as magnesium, sulfate or terbutaline, had multiple birth, or PEC, or on bed rest
phys. changes in respiratory: expected findings
the respiratory rate inthe postpartum perid is typically in the range of 12 to 20 breaths per minute
the PaO2 should be 95% or higher
breath sounds clear
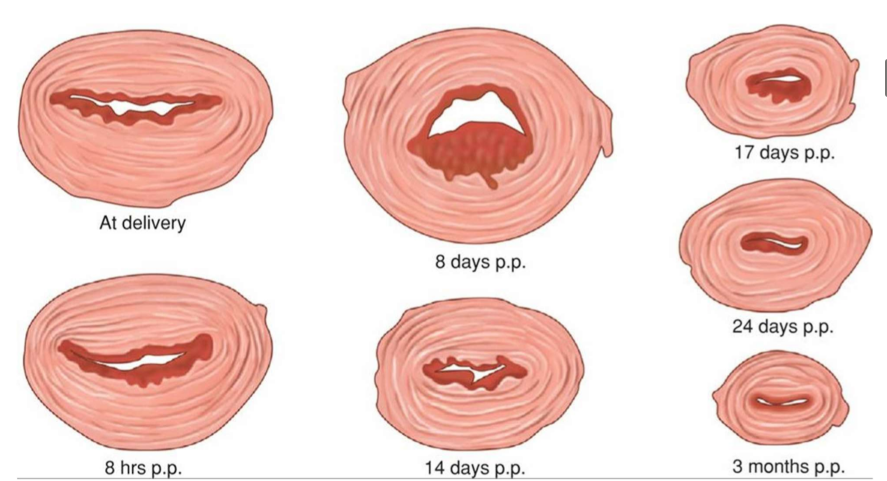
physiologic changes in cervix
dilated, edematous, and bruised
small tears or lacerations may be present
rapid healing takes place
physiologic changes in vagina
greatly stretched
walls appear edematous
may have multiple small lacerations
few vaginal rugae (folds) are present
rugae begin to reappear by 3-4 wks
vaginal epithelium restored 6-20 wks
vaginal wall regains thickness
dyspareunia (discomfort durin inercourse)
phys. changes in vagina: estrogen
estrogen is key for vaginal walls to regain thickness
without estrogen, vagina becomes atrophic
estrogen is produced by ovaries and during lactation, decr. inestrogen contributes to vaginal dryness which may lead to dyspareunia
phys. changes in perineum
pelvic floor muscle stretch and thin
may be edematous and bruised
laceration and episiotomy - episiotomy may not completely heal for another 6 months
phys changes of uterus: involution
return to pre-pregnant state; usually takes 6-8 wks postpartum
phys. changes of uterus: afterpains
caused by strong intermitent uterine contraction