Cognition
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
OTs Role
Eval- occupational profile. motor and cognitive assessments, collaborative goal setting
Intervention: modify (compensate, adapt), therapeutic use of occupation, education, advocacy, group interventions
Occupation/Performance Demands: supplies, space, time, number of steps, speed required, position required, sequence, prep work, sensory/perceptual
conditions, functions, and structures
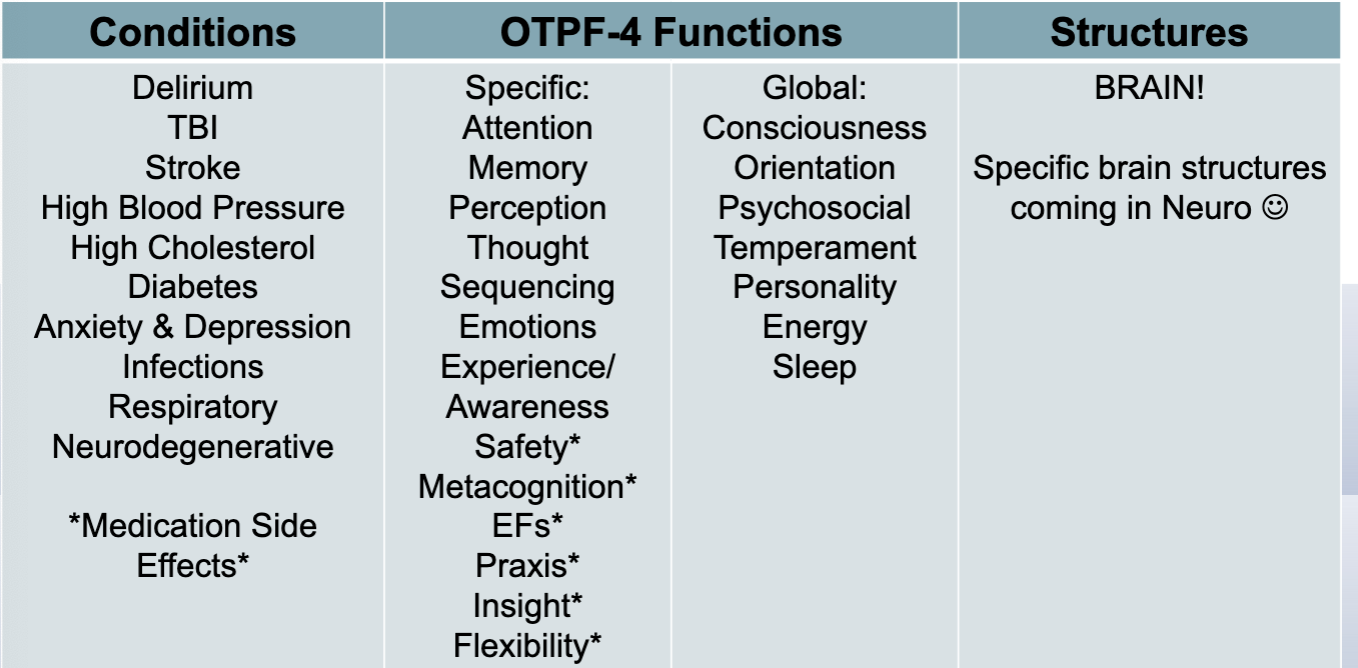
basic cognition skills
attention- alertness and arousal; higher levels involve working memory, sustained concentration, vigilance, divided attention
memory- complex skills consisting of attention, encoding, storage, and retrieval
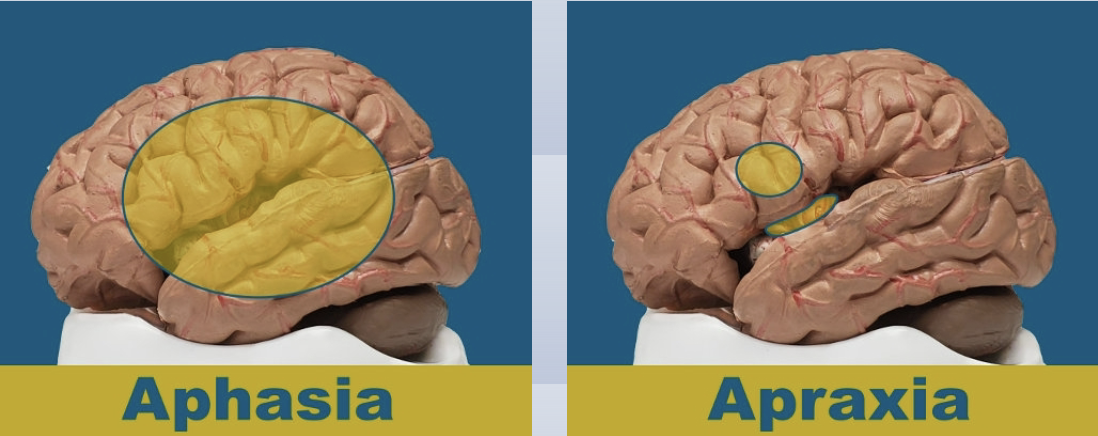
perception- hemispatial neglect, visuospatial organization, apraxia
neglect is an attention issue not vision
Types of attention
divided- respond to 2+ events/stimuli at the same time
alternating- shift focus between tasks that demand different behavioral/cognitive skills
selective- process target info selectively and inhibit responding to nontarget info
sustained- ability to maintain attention over time, during continuous or repetitive task
focused- recognize and acknowledge specific sensory info; hear a knock→turn eyes towards noise
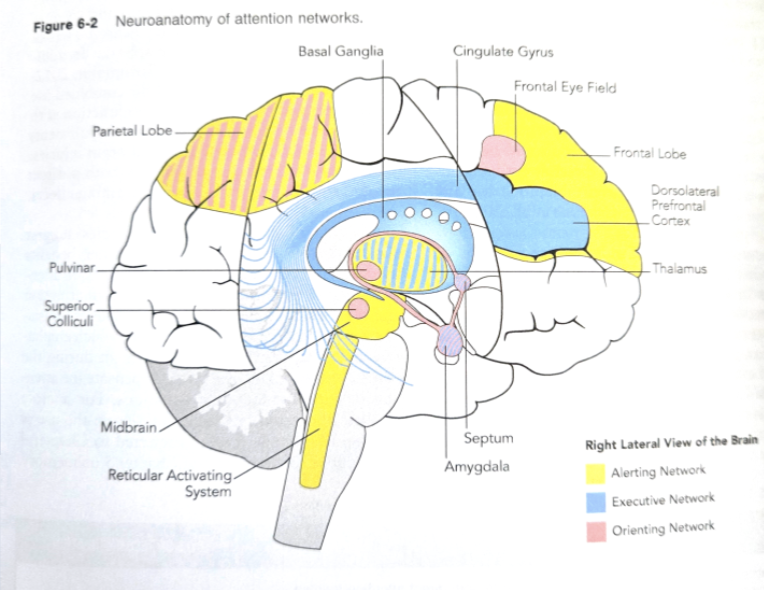
subsystems of attention
alerting: controls sustained attention and vigilance
orienting: responsible for selecting and prioritizing incoming sensory info
executive control: exerting volitional control over attention processes, monitoring, resolving conflict
Attention assessments
Trail making test
test of everyday attention (TEA)
attention treatment
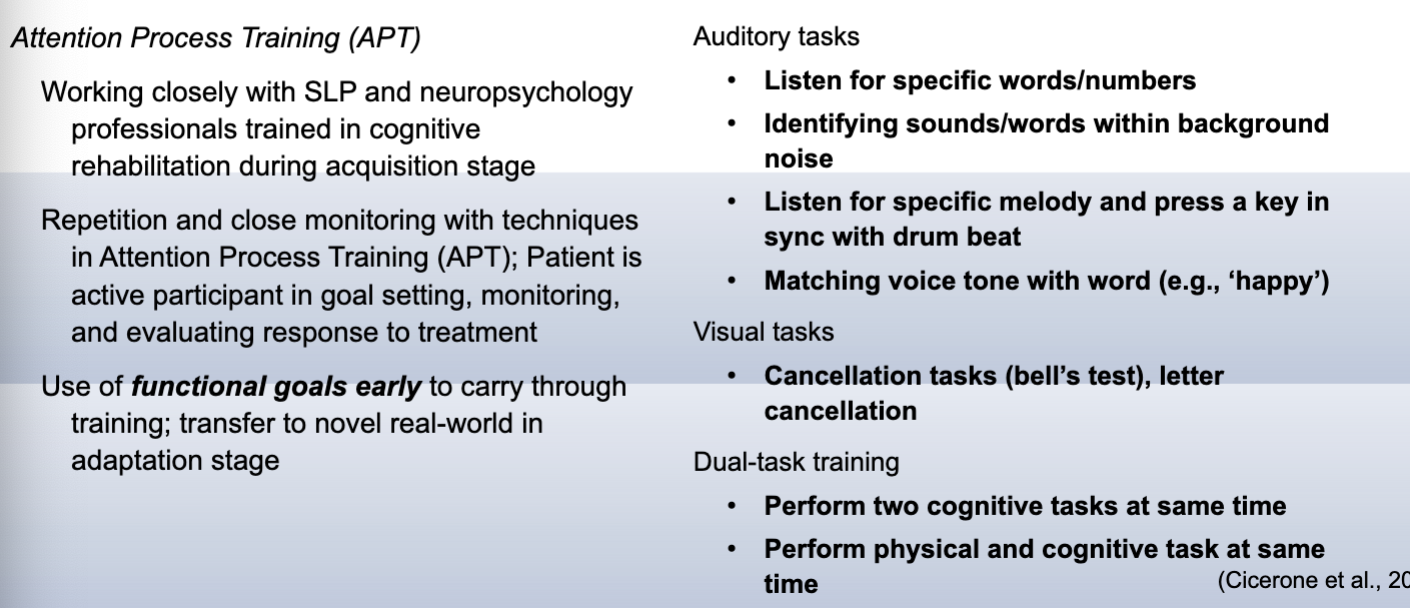
Attention: Time pressure management
decision making ordered in 3 levels based on time pressure present
operational: immediate decisions and actions to prevent failure
tactical: anticipate and adapt behaviors to reduce or prevent problems when time pressure is present but manageable
strategic: decisions made well ahead of time with no pressure
Memory
depending on location of injury, different types of memory are impacted
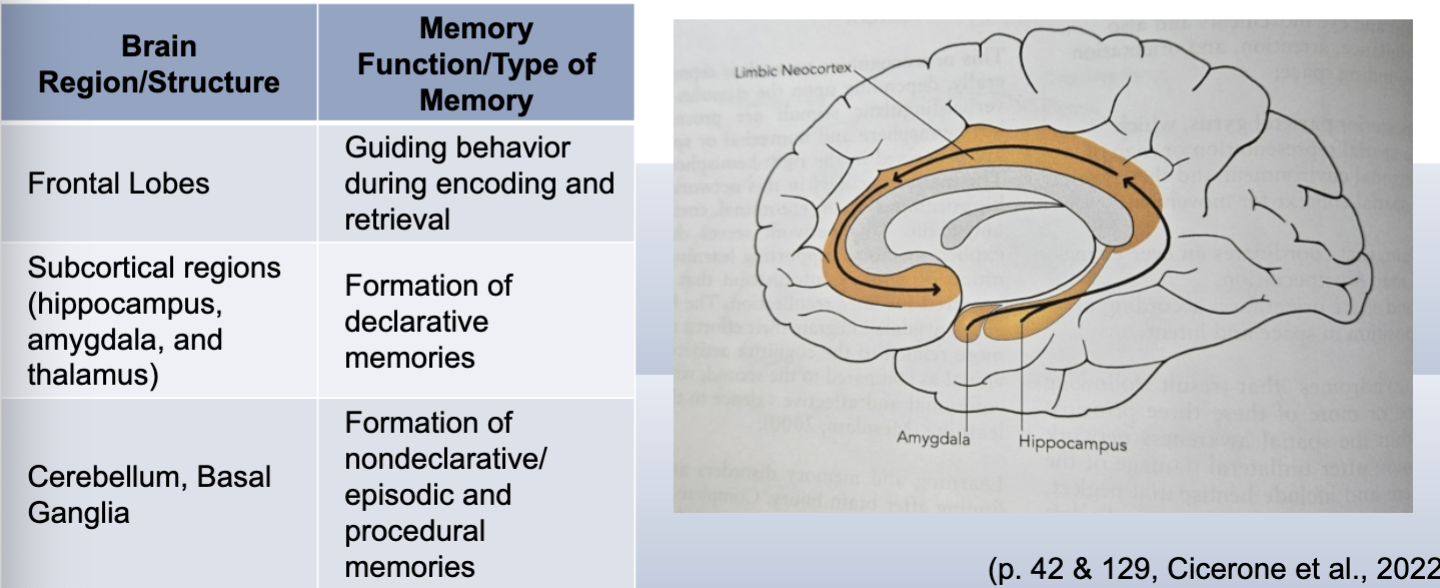
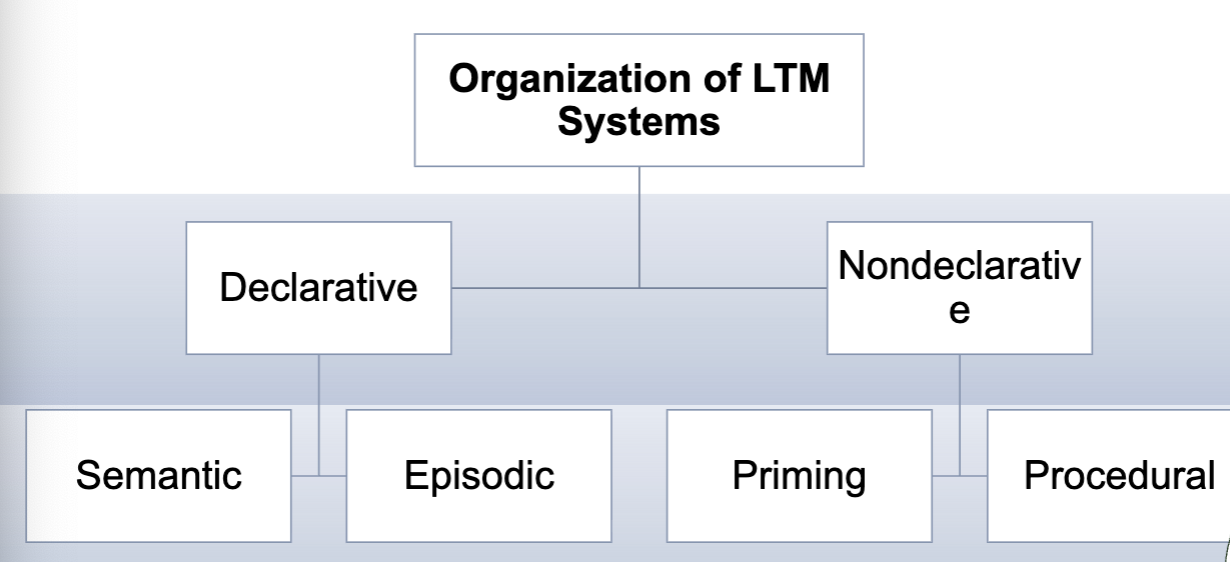
Long term memory hierarchy
declarative- explicit memory, conscious recall of what you did this weekend
semantic- knowledge, definitions, facts, concepts
episodic- context specific, personal experiences; tap into episodic to remember semantic (where did I write that fact in my notes, where was I when I studied this)
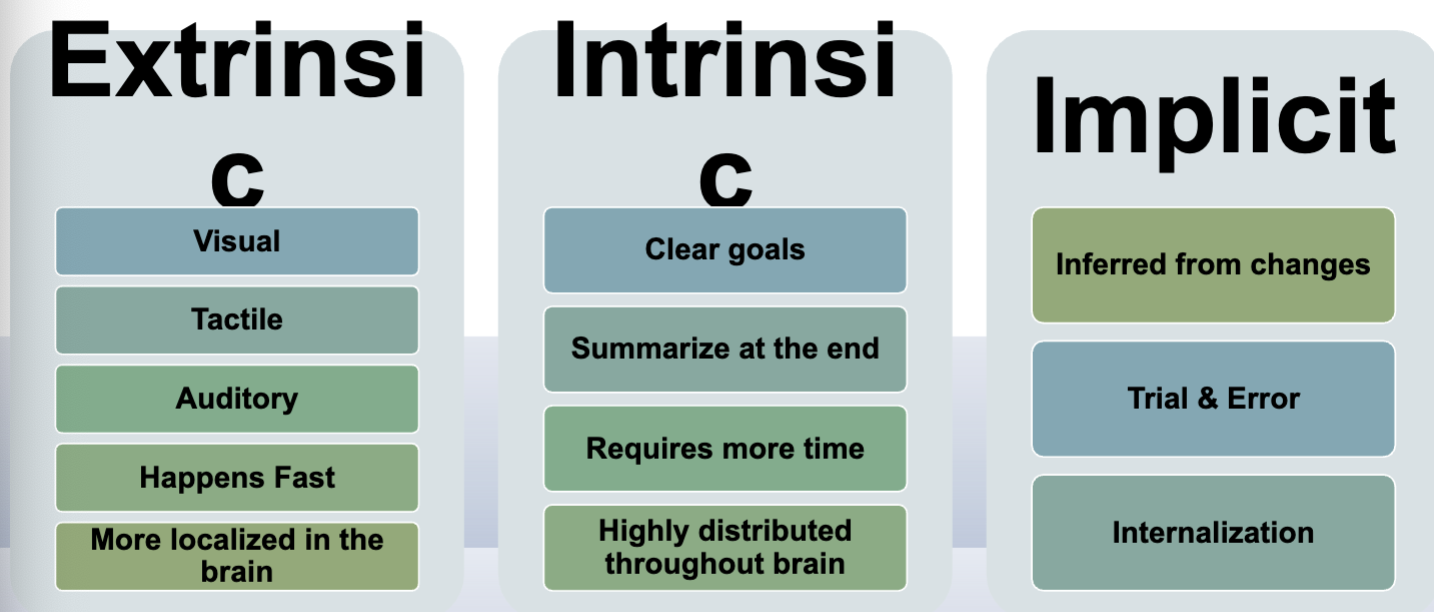
non-declaritive- does not require conscious thought to retrieve, automatic behaviors
priming- exposure to stimulus influences later response without conscious awareness
read the word coffee, more likely to later identify soda rather than bread because you’ve been primed for beverages
procedural- skill memory, implicit, know how to ride a bike without “thinking about it”
prospective (future)- I need to remember I have a Dr appointment tmrw
retrospective (past)- I had a Dr appointment last week
Memory assessments and interventions
contextual memory test
rivermead behavioral memory test 3rd edition
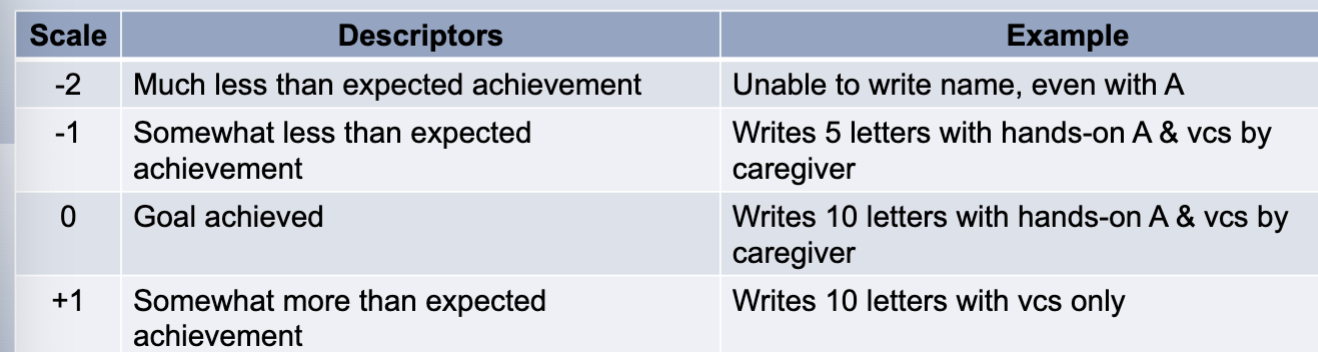
goal attainment scaling
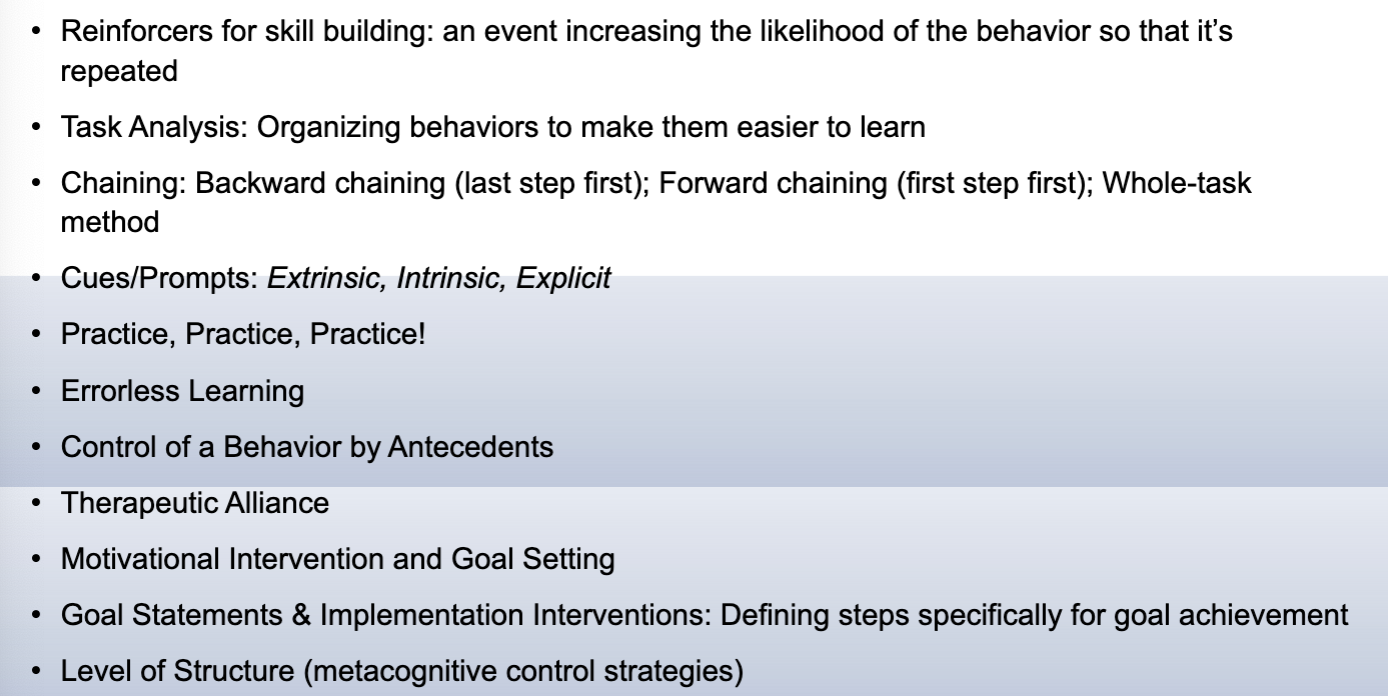
interventions: external help (orientation notebook, visual cues, electronic devices); memory strategy training (association techniques, organizational, and elaboration)
Perception
guides decisions and actions, shapes beliefs
hemispatial neglect: most associated with right parietal lobe injury; many improve but chronic neglect impacts many occupations
can be neglect of visual, auditory, tactile, and proprioception contralateral to injury
assessments: bells test, behavioral inattention test, test of visual neglect
training: visual scanning training (gold standard), stimulus location, anchoring, pacing, density, lighthouse strategy (help cue to visually scan the whole environment)
visuospatial and visual organizational skills
assessment: line bisection test, figure-ground visual perception test, body midline test, conditional visual target cancellations
training: pattern recognition (word locus, dot configurations, sequential analysis); 30-40 min, 3x /week
Apraxia
Injury to premotor strip; if someone has Broca’s aphasia also assess for apraxia because Broca’s injury often spans the area affecting praxis
know their not right, but can’t figure out how to fix it→ frustration
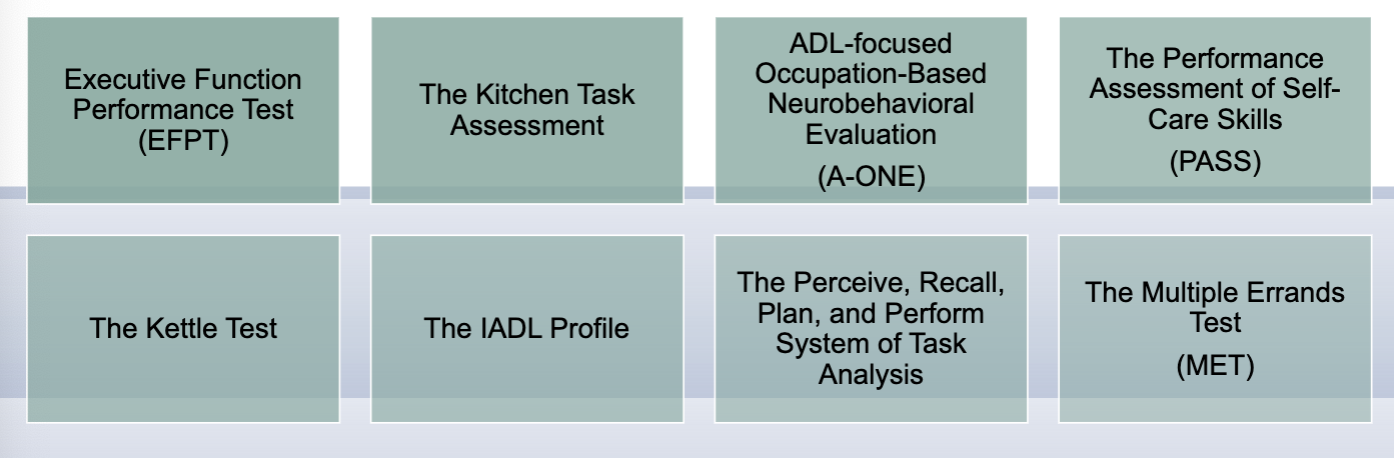
assessment- Arnadottir OT-ADL neurobehavioral evaluation (A-ONE), apraxia screen of TULIA (AST)
treatment: specific gestural or strategy training is recommended for apraxia during acute rehab for L hem. stroke
gestural: transitive to intransitive to instransitive-nonsymbolic gesture; use personally relevant stimuli
strategy training: initiating with proper plan of action and selection of objects to activity execution to controlling own performance
grading instructions, assistance, and feedback
Higher level cog skills
knowing about knowing and knowing how to know, metacognition , monitoring, awareness of executive functions
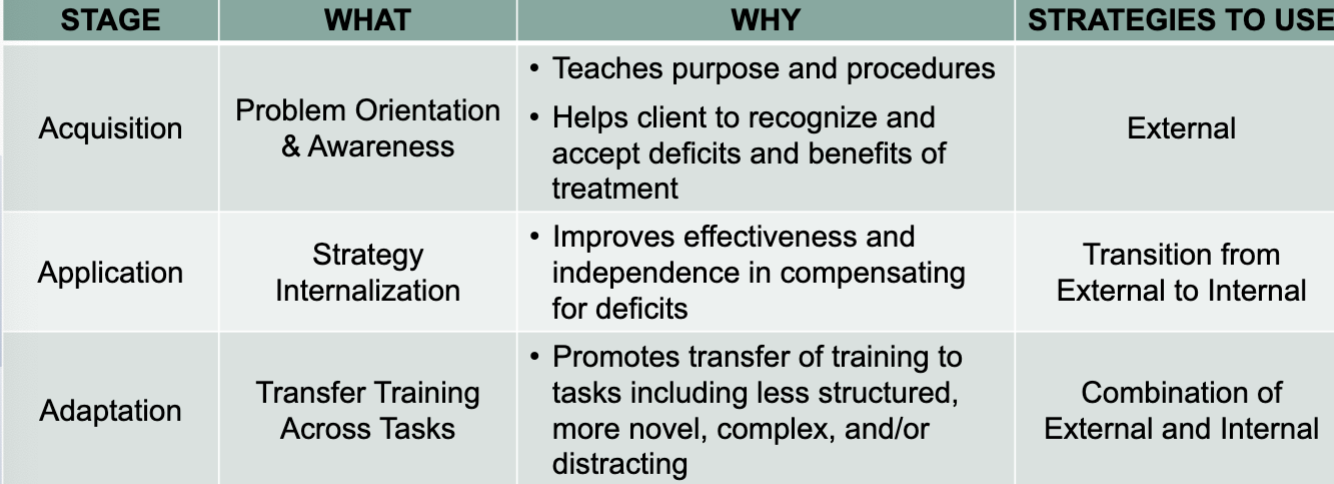
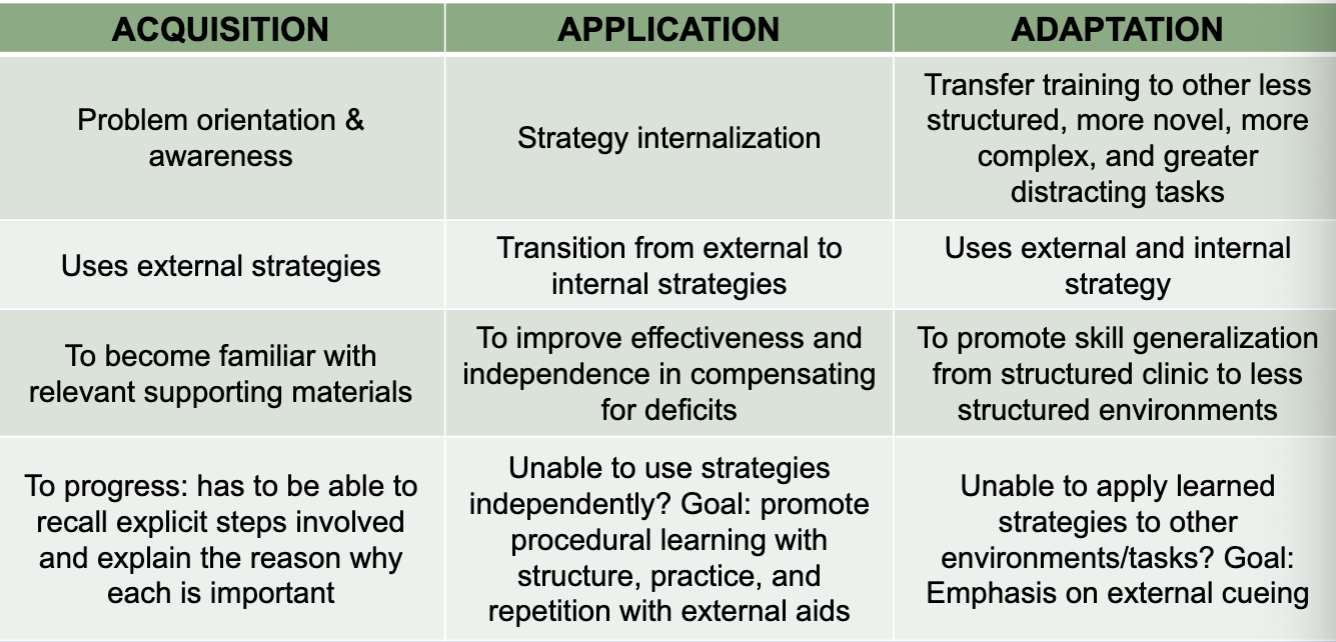
Stages of Treatment for Cognition:
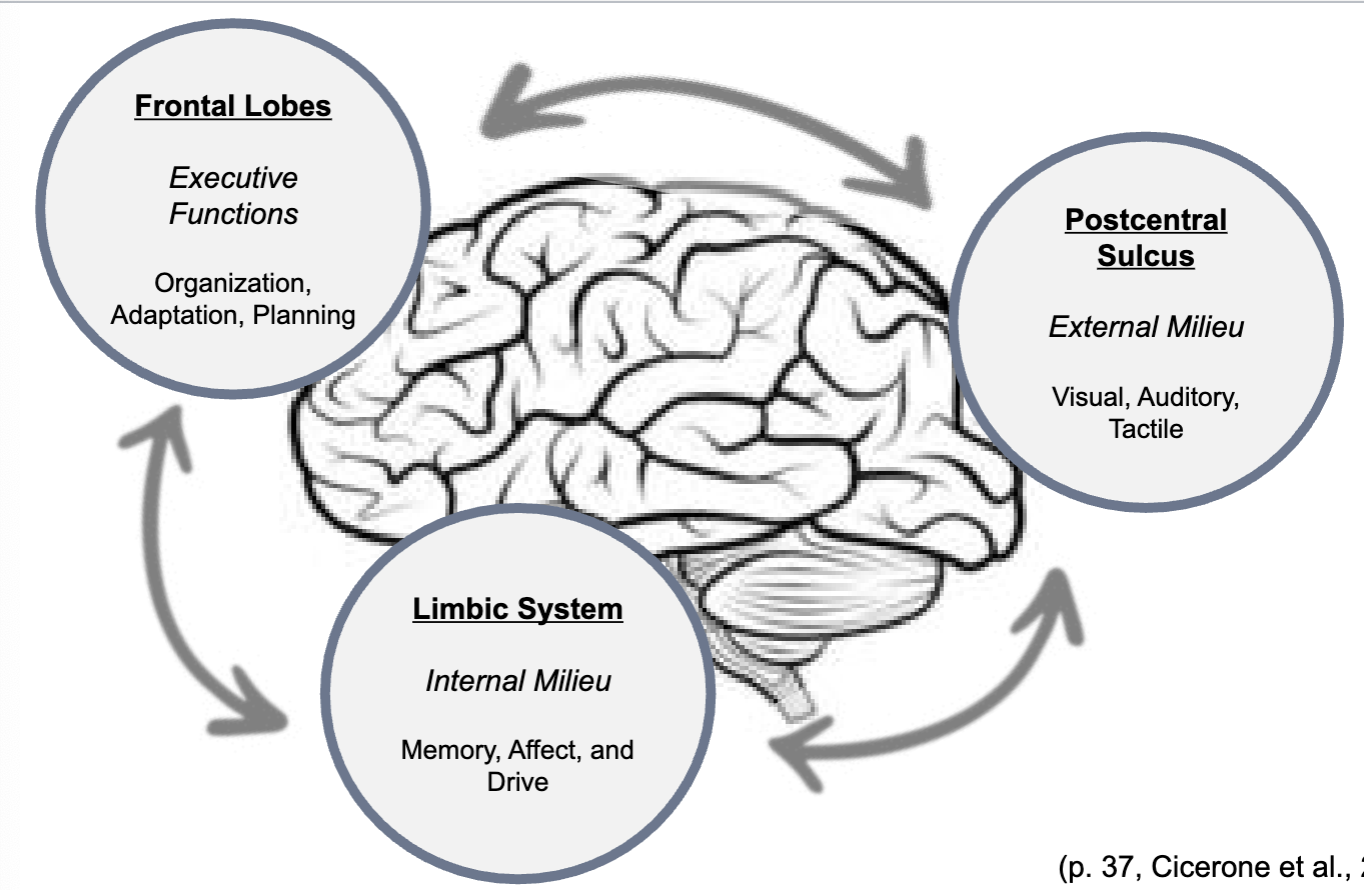
Frontal lobe regulation of internal and external milieu
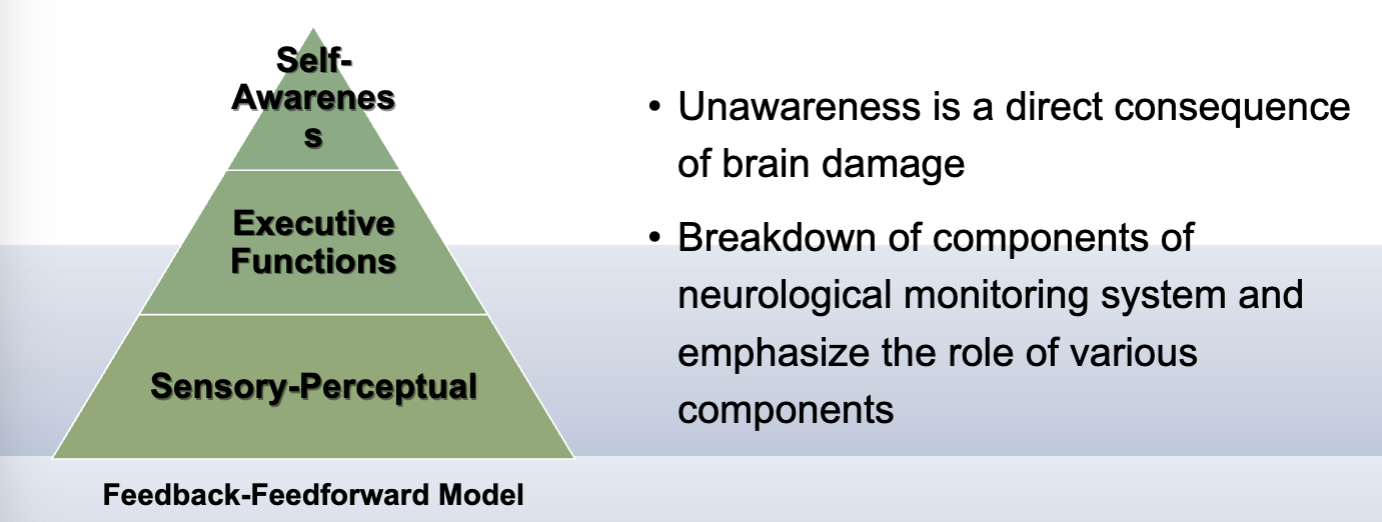
awareness
lack of knowledge/recognition of disease/injury, consequential deficits, functional disabilities
unawareness = anosognosia
Awareness Levels
anticipatory: anticipating any potential impact of deficits prior to situation
emergent: recognizing deficits are occurring in functional engagement; able to use compensations once recognized
executive functions- actual doing (and anticipatory)
intellectual: key for compensation implementation (able to set a reminder)
knowledge about + how to compensate
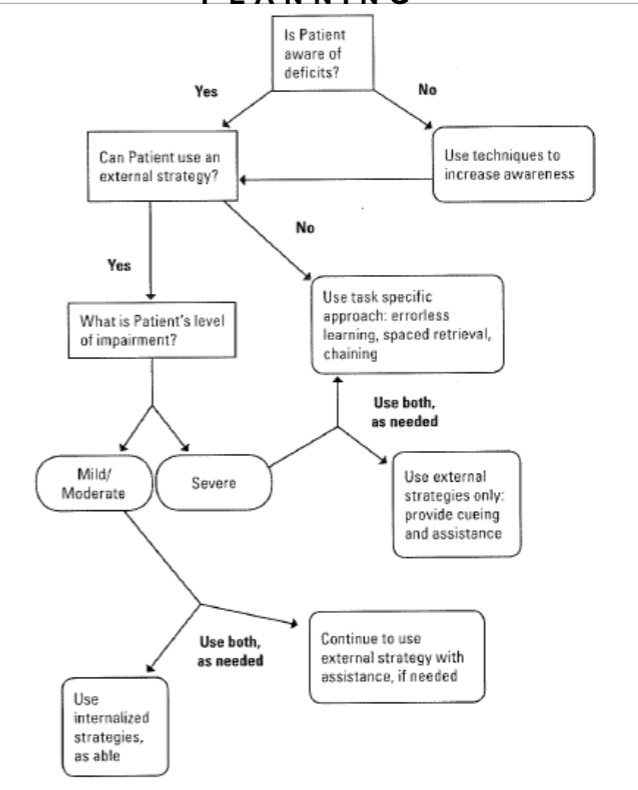
Awareness treatment guidelines
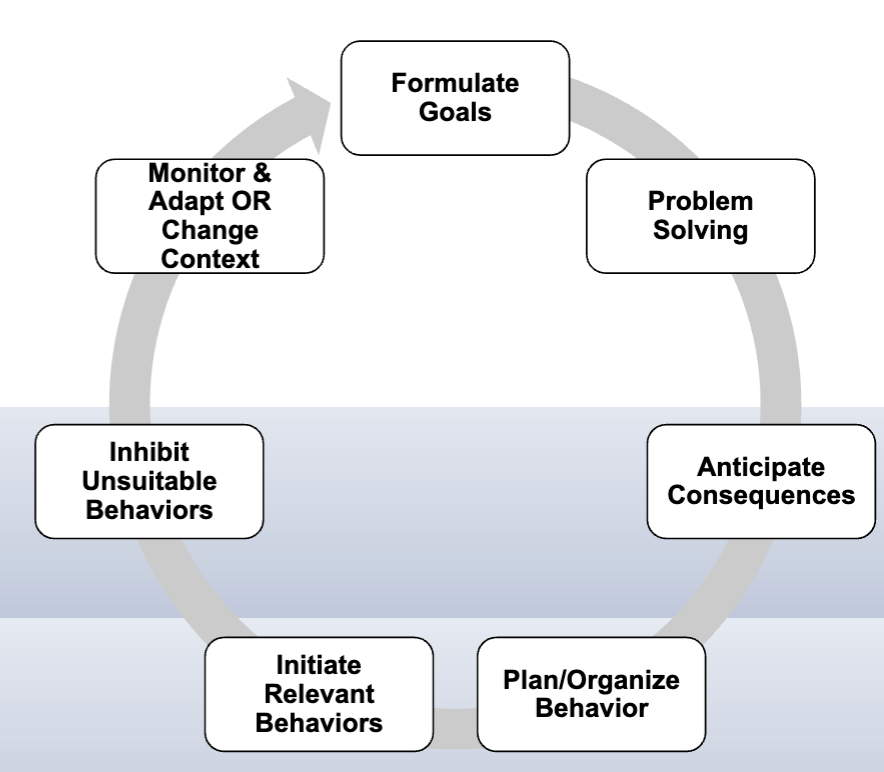
Executive functions
integrative cognitive processes that manage goal-directed, purposeful, and adaptive behavior; higher-order functions in non-routine situations (novel, conflicting, complex)
oversees basic processes: attention, memory, behavior, emotion
development of metacognition processes (self-monitoring, error awareness, insight)
common issues: fail to comprehend goal, plan, oversimplify task, recognize errors, poor execution, reject complexity of task
Goal setting for executive function
GOAL-PLAN-DO-CHECK
Goal attainment scale
patient reported outcome that involves goal selection and standardize means to measure the extent goals are met
planning
anticipation and step-by-step sequence to meet activity demands
check traffic, get in car, drive to campus
monitoring is a common deficit in neuro- can you monitor yourself when carrying out plan and make appropriate responses
self-eval- evaluate yourself and receiving feedback, make changes as needed
assessments and intervention for executive functioning
Stages of Treatment: Executive Functioning
feedback