Equine anaesthesia and challenges
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
risk factors of horses for anaesthesia
Increasing ASA grade
Increasing age and foals
Surgery type and position
Duration
Time of day, OOH provision
Agents used (premed/TIVA)
Recovery quality ?
Why do horses die during or after anaesthesia?
Fractures in recovery (highest mortality)
Abdominal problems (colic)
Neuro and spinal cord malacia
Intra operative cardiac arrest
Respiratory obstruction
Post anaesthetic myopathy (PAM)
neuropathies
why si there a risk of fractures in recovery
Increased amt of pressure and strain going through limb and still having drugs on board
how can horses be sedated?
standing of recumbent
how are sedatives asnd anagesics and local anaesthetics given?
in combination with each other
why can horses urinate a lot and what needs to be done
alpha 2 agonists make them make more urine
urinary catheters to help keep sterile
GA prep the night before
Admit the night before
Complete physical exam
Murmurs?
Blood sample
isnt routine
Starve
Starve as little as possible (longer starve -> incrs post op ileus -> colic
Remove shoes
Ensure horse is clean
minimal contam into theatre
what should be done on the morning of surgery
IV cannula- ALWAYS
Flush out mouth
So no food, intubate blind to don’t want to push food down trachea
Tail bandage/plait
Cleanliness in theatre. Don’t want to stand on tail in recovery-> scare
Clip if possible
Do before to reduce time if poss
Weigh
Make an anaesthestic plan
Pre-medicate the horse
Can settle, examine them, make sure no worries, tick off things on list
Can tape iv In recovery can hit into themselves so more likely to cause damage. So helps protect horse
Preparation for Anaesthesia
1. prepare monitoring equipement (prime anaesthetic circuit with isoflourane (cap on end))
2. select et tubes
3. change soda lime
4. label and prepare drugs
5. leak test anaesthetic machine and ventilator set tidal volume
6. prepare fluids and table
what type of circuit is used and FGF?
Rebreathing circuit- CIRCLE
fgf= Start 6-8L/min
After 15min reduce to 2-4L/min
premedication for horses
Acepromazine
alpha 2 agonists
opioids
why is acepromazine used as a premed in horses
•Anxiolytic (reduces anxiety, but not a true sedative)
•Reduces anaesthetic gas requirement (MAC)
•Improved recoveries (CEPEF 4)
Historical reduction in mortality (CEPEF2)
when to use acepromazine?
•IM 40minutes before sedation
•IV 20minutes before sedation
what are risks with acepromazine?
•Penile prolapse
•Hypovolaemia
why do we get hypovolemia with acepromazine
Bc vasodilation
Dcrs bp
Fall over
why do we need to discuss with the owner abt using acepromazine if male
Penile prolapse- if breeding stallion need to talk abt this to owner as can affect fertility with it. Is rare tho.
what do alpha 2 agonists do and used for?
•Sedation for induction
•Analgesia
•Vasoconstriction and bradycardia
So need to wait long enough (abt5mins) before giving ket
chose based on how long you need them to last
why are opiods used?
•Analgesia
•Improved sedation quality
•Respiratory depression
chose based on the level of pain you expect them to be in
when to give pre meds?
•In induction box
Give enough time to take effect!
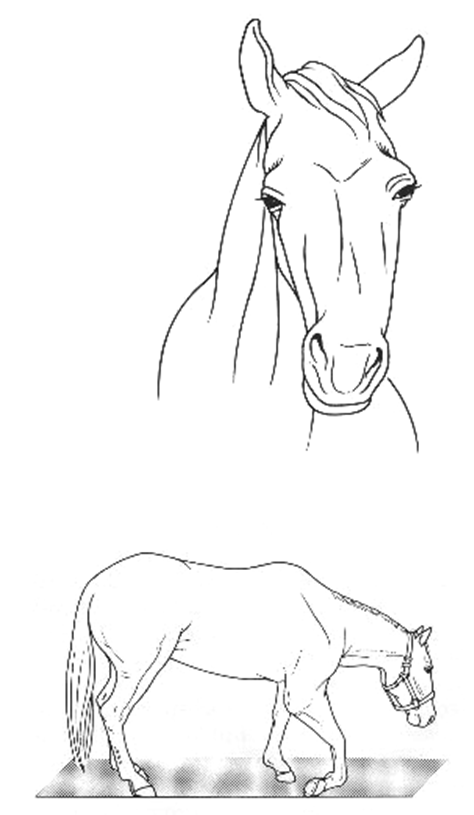
how do we want the horse to present when they are ready for induction?
head down, wide based stance. Horses are insensible to surroundings - they are ready for induction...... GIVE KETAMINE
head between knees give ketamine
if a horses head isnt between their knees, can we give ketamine
NO
NEED MORE premed
Start lower dose and give more till you get this
what are typical equine premeds?
ASA 1&2:
+/- Acepromazine (wait 20-40mins) + alpha 2 agonist +/- opioid
Remember NSAID +/- Antibiotic at this time too
what is used for induction?
IV ketamine
A benzodiazepine (midazolam can be combined with the ketamine)
Bc midazolam is licensed
Occasionally guaifenesin IV can be used instead of an alpha 2 agonist
what is guaifenesin
centrally acting m relaxant
give an example of an anaesthetic protocol for horses?
•Acepromazine (sedation) IM, wait approx 30-45 minutes
•Detomidine (alpha 2) IV, wait 5 minutes, adequate sedation must be apparent
•Methadone (opioid) IV, HR>20 bpm, head between knees and non-responsive...
•Midazolam/ketamine IV for induction (or ketamine)
what 3 ways can we get a horse to the ground after induction
free drop
squeeze door
assist → not really done now
how cna we assist a horse down after premed
someone in box with them
guide them down with ropes
not done now
what is a free drop
horse falls down int he padded room by themselves
Safe for humans
But may not be as safe for horses
how is a squeeze door used
it comes out of wall
Can trap the horse between padded gate and wall
Guides the horse down
So is best for horse and humans
But not in most places
what are next steps after induction? (4)
Intubate (ET tubes, cuffs checked, gag, lubricant)
Gag in mouth to keep open
Cant see where going
So if cany food -> can be pushed into lungs -> is why we wash mouth
Attach hobbles and move horse
Place on table and connect to anaesthetic machine
Maintain horse in dorsal or lateral recumbency on oxygen in isoflurane
when intubating what does resistance mean
Should be no resistance in trachea
If in oes will get resistance
what to do once horse is on table?
Monitor as usual, place arterial line for ABP, ECG, Et CO2, pulse oximetry
Catheterise (urinary) and bucket
Connect IV fluids, consider PIVA
what reason on recovery is it better to catheterise patient in surgery
if bladders full more likely to stand up
Also helps them to lie down for longer in recovery so exhale more of the anaesthetic gas before standing
which v is used for venous cannula and IVFT
jugular v
which a is used for arterial cannula
facial a
what is used for maintenance?
Volatile anaesthetic agent (isoflurane or sevoflurane; only isoflurane licensed, isoflurane has a bigger carbon footprint
what is the problem in recovery that hypotension in surgery can lead to
myopathy
what is the problem with the maintenance used in horses?
§Hypotension!
Need lowest dose that ensures anaesthesia
what is the MAC for isoflurane?
1.3-1.6%
what is the MAC for sevoflurane?
2.3-2.8%
what can we use to guide us to know how much volatile agent to give in surgery
Use end tidal isoflurane concentration and monitoring parameters
what do we monitor on the horse
palp pulses
reflexes and eyes
m tone
what machines can we use to monitor
multiparameter
pulse ox
blood gases
how do horses eyes respond differently
Can have palp resp
Track the trends -> didn’t now does this is a difference
If not had one all time that’s ok
if we get nystagmus what could this mean
Nystagmus (horizontal) -> either v deep or getting lighter and waking up -> happens just before the animal starts to move on the table
why do we use m tone and not jaw tone, how do we do this
Jaw tone difficult-> do just the m tone
Palp pectorals or side of neck
Does it feel more tense
Muscles tenses just before they start to move
how can TIVA be achieved?
1)Top-up bolus injections (ketamine e.g. 0.5mg/kg)
shorter
2)Continuous rate infusions ('triple drip' in equine anaesthesia - useful for field anaesthesia)
for Bit longer procedures (45-hr)
what is included in a triple drip in horse anaesthesia?
guaifenesin, ketamine, detomidine
what does TIVA allow for?
Produces a much diminished anaesthesia stress response compared with inhalation agents and is therefore considered as a physiologically superior method of anaesthesia
what can we use for PIVA
Ketamine infusion
Lidocaine CRI
Alpha 2 agonist infusion
what does piva allow for
we use MAC reducing drugs so can reduce the inhalation agent needed
Problems during anaesthesia
•Hypotension
•Hypoxaemia
•Hypercapnia
•Bradycardia
•Tachycardia
•Neuropathy
•Eye problems
what can hypotension lead to?
myopathy on recovery
what is used to improve prevention of hypotension?
Use positive inotrope (dobutamine)
Reduce isoflurane
This is causing the low bp. Get to min level we can
Use PIVA
Increase fluids (if hypovolaemic)
Improve vasc vol
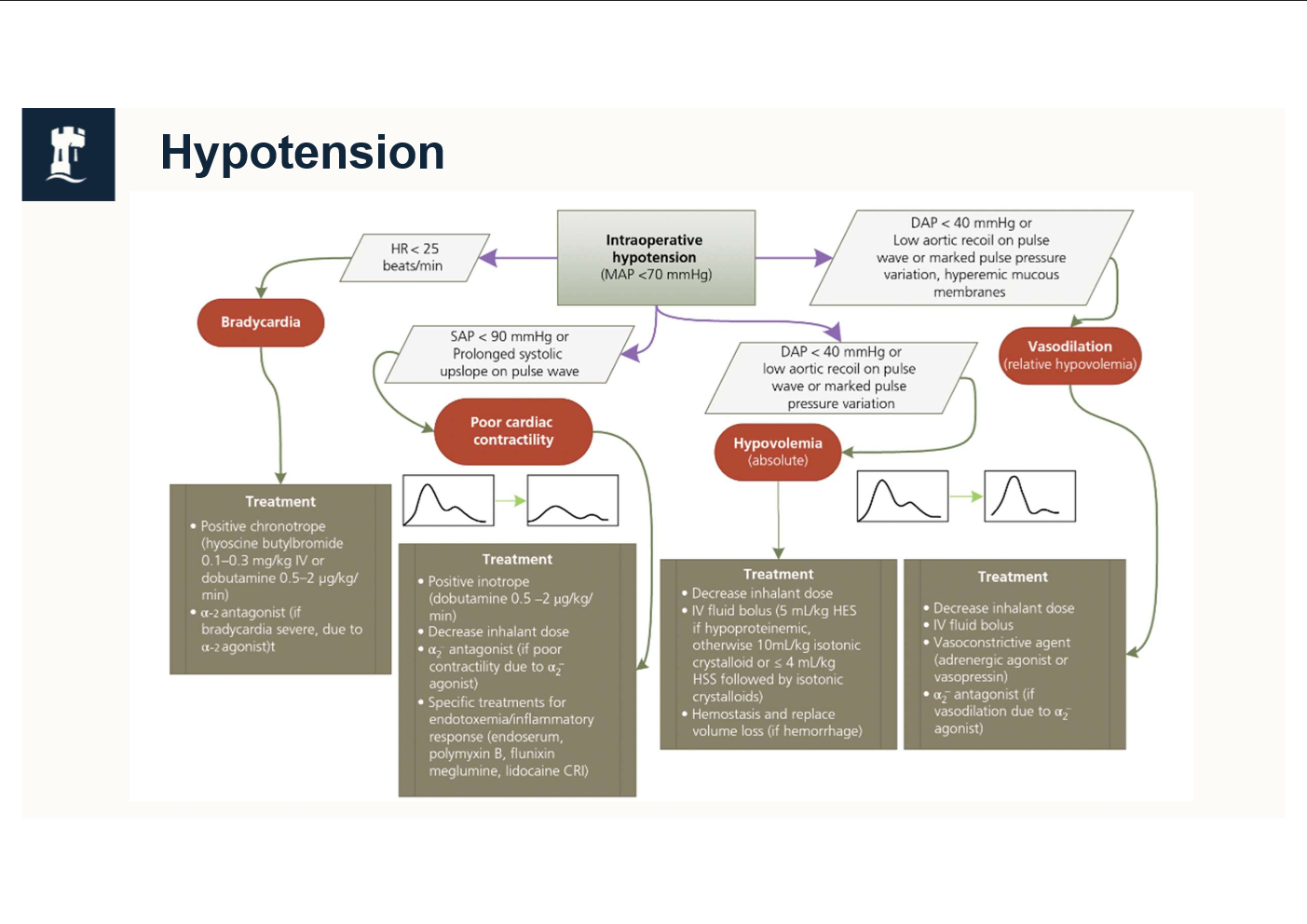
what MAP is considered hypotensive
<70mmHg using invasive arterial monitoring
what does dobutamine (+ve inotrope) do
Incrs contractiltiy of heart
Incrs co
Incrs bp
why does low bp lead to myopathy
Low bp
Dcrs perfusion to m
Not enough o2
Respire anaerobically
Myopathy bc run out of o2 to function and produce lactate which damages muscles
when do we see Spinal cord malacia
•Becomes apparent in recovery period
but occurs in the maintenance
what is Spinal cord malacia
Can use fl but have paralysis of hl
Fatal
what horses get Spinal cord malacia more
•Usually heavy breed horses & young
what is cause of Spinal cord malacia
unknow
potentially hypotension → but Can still have a good bp and get this
•More common in dorsal recumbency
•Not related to duration of anaesthesia
how does hypoxaemia present on machines?
•Shown by low sats on SPO2% and low SaO2 on arterial blood gases
•PaO2 <60mmHg
why does hypoxamia happen?
•O2 failure→ so not getting enough o2
•V/Q mismatch...
The animal is turned on its back, RR is reduced (by drugs), CO is reduced (by drugs) = low O2 delivery
Parts of lungs ventilated and parts are perfused, don’t match up, poor gas exchange, not enough o2, co2 incrs
Get resp acidosis too
What is hypoxemia?
Low O2 tension in blood
what to do in case of hypoxamia? (7 steps)
1.Check the SPO2% reading - some pulse oximeter probes don’t work well on horse tongues’, so check it first
2.Take blood gas - if PaO2 is much lower than it should be (remember is should be 4-5 x FIO2%) – act
3.Switch down the isoflurane/sevoflurane
4.Ventilate/IPPV… increase resp/tidal volume
5.Ensure adequate circulating blood volume (IVFT)
6.Tilt table (head up) slightly if possible
7.Give beta agonist (down the ETT) eg salbutamol (is bronchodilator)
and hurry up and finish and get horse back into sternal!
what is hypercapnia?
excess carbon dioxide in the blood
why does hypercapnia happen?
•The animal is turned on its back, RR is reduced (by drugs and position), so CO2 rises in the body
how to reduce co2 in cases of hypercapnia?
•Reduce the volatile agent (isoflurane)
•Instigate ventilation
why do we tolerate a bit of hypercapnia
•Spontaneous breathing in recovery
•Increased oxygen dissociation in tissues
If slightly acidic, Hb releases o2 better, so get more oxygen to tissues -> reduce myopathy
what to do in cases of bradycardia?
•Consider cause... Volatile agent, vagal tone, opioid, alpha 2, toxaemia, hypoxia - address those first
•THEN, if HR still low use drug.... Hyoscine N-butylbromide (BUSCOPAN!) →incrs hr
•Other drugs include atropine or glycopyrrolate
what do you need to consider with bradycardia
§Breed/fitness of horse and their HR prior to anaesthesia
§If blood pressure or oxygen delivery is compromised too – you need to act
what do you need to consider with tachycardia
Breed/fitness of horse and their HR prior to anaesthesia
Evaluate ABP and reflexes too, especially nystagmus and palpebral reflex, may need to act fast if horse moves
what to do with tachycardia?
Consider the causes... sympathetic stimulation (nociception is most likely), but can be CO2, acid base disturbance, drug reaction, cardiac issue, hypotension...
•Depth not adequate... Administer ketamine (or thiopentone) bolus IV and consider the % volatile agent - may need to increase too (increase FGF too to speed this rate of change up, remember the horse is on a circle)
•More analgesia?
•Check arterial blood gas... hypercapnia?
BP Low.... Treat as for hypotension
why does neuropathy occur?
Poor positioning +/- hypotension
Pressure placed onto nerve so get problems post op and recovery
when does neuropathy become evident?
when horse wakes up, may cause poor recovery
but happens in the maintenance
what is the most common neuropathy?
Radial nerve, facial nerve (headcollar left on during sx)
what has happened here
neuropathy
Radial n -> dropped elbow
Cant weight bare
From being in lateral
what does neuropathy resemble
myopathy → not as painful as myopathy tho
when are eye problems seen?
when horse has been in lateral recumbency
so Eye rubbed against something
how to prevent eye problems?
Must protect lowermost eye with padding
Lubrication for eye at start of surgery
what occurs in the recovery period: part 1
•Volatile agent switched off
•Reconnected to hoist
•Head supported
•Positioned in RLR in recovery box (if dorsal or RLR on table), LLR if LLR on table
Flipping can make them stop breathing due to the lungs
•Pull dependent limb forwards
Reduce risk of radial n neuopathy
•Demand valve can be used to stimulate breathing
•Nasal tubes (obligate nasal breather)
•Extubate when swallowing or just before
•Exit recovery box, watch, can recover with ropes outside
Ropes don’t pull them up, and doesn’t support weight but just gives them some support/ stabiliser
What are the characteristics of an optimum recovery environment?
Quiet, Dark
What should be ensured regarding the bladder in an optimum recovery environment?
Empty bladder
What is important for pain management in the recovery environment?
Analgesia
What should be allowed time for in the recovery environment?
Anaesthetic drug elimination
What type of sedation can be used in recovery?
Low dose alpha 2 agonists or acepromazine
When should romifidine be administered in recovery?
Once in recovery and breathing spontaneously
When should xylazine be administered in recovery?
Once signs of reduced anaesthetic depth occur
what are the optimal timings in recovery
•Lateral: 30 minutes
•Sternal: 10-15minutes
•Standing: 15 minutes then taken back to stable
what are some complications in recovery?
UAO, Laryngeal obstruction, nasal oedema
what are signs of upper airway obstruction
Stridor or stertor following tracheal extubation
Nostril flaring on inspiration
Abdominal respiratory effort
Exaggerated thoracic excursion
Absence of airflow at the nostrils
where can upper airway obstruction occur
Obstruction tends to occur within the nasal passages or at the level of the larynx
what can cause laryngeal obstruction
Dorsal displacement of soft palate
Epiglottic retroversion
what can be done to reduce laryngeal obstruction
Select appropriate ET tube size and insert gently
Following laryngeal surgery may leave ET tube in place for recovery (secured)
what can be done if laryngeal obstruction occurs
would need to pass another endotracheal tube to fix this
or
Emergency tracheostomy
how can we reduce nasal oedema
Common usually resolves as horse stands
Use nasopharyngeal tubes, or phenylephrine or both
Can recover horse to standing with ET tube in place

what has happened here

very occasionally they can throw their heads around with the nasal tubes in place and you can get bleeding
but as long as that horse can breathe, that's fine, the bleeding will stop