HEENT Nasal and Sinus Disorders
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
70 Terms
Normal respiratory functions of the nose
Warms air (conchea, septum)
Humidifies air completely before it passes beyond the nose
Partially filters via turbinate, septum, and pharyngeal wall, traps in mucus coating and transports via cilia
Nose function raises air temp to within
1 degree F of body temp
Keisslebach’s plexus is a common area for
epistaxis = arteries or veins get dry or brittle, bleed easily
Nose function is very effective at filtration; nothing larger than
6 micrometers will enter the lungs
“Coal miner’s lung” can come from
particles greater than 5 micrometers entering the lungs; cigarette smoke particles 0.3 micrometer and can get to alveoli
Anterior vs Posterior epistaxis
Anterior Epistaxis = Kiesselbach venous plexus MC source
Posterior Epistaxis = Sphenopalatine artery branches and Woodruff’s plexus MC site (may cause bleeding in both nares & the posterior pharynx)
Epistaxis etiology
Nasal trauma, rhinitis, alcohol/cocaine use, antiplatelet meds, HTN may prolong
Epistaxis risk factors
HTN, nasal neoplasms
Epistaxis presentation
Bleeding out of one or both nostrils, bleeding into oropharynx
Epistaxis dx
Assess location of bleeding, anterior vs posterior
Epistaxis tx - anterior
Local pressure for 10 min.
Review Meds: ASA, Warfarin, Dabigatran- possible instigators
Oxymetazoline NS
Premarin cream for recurrent anterior bleeds
Epistaxis tx - posterior
Immediate ENT Referral, nasal packing
Other instigators of epistaxis may be
local trauma
HTN
extreme dryness
atrophic rhinitis
foreign body
Nasal fracture etio
fracture of nasal bones, septum, or turbinates
etio: trauma
Nasal fracture presentation
Swelling, tenderness, black eyes, nasal bleeding, nasal congestion
Nasal fracture dx
x-rays, CT
Nasal fracture tx
Splinting and realignment by hand or surgery
Surgery right away or after edema goes down
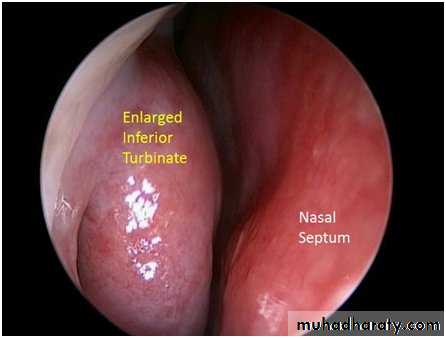
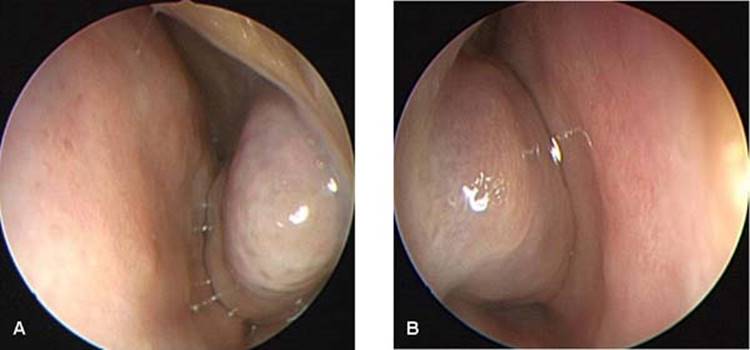
Nasal septum deviation etio
congenital, trauma, can get worse w/ age
Nasal septum deviation presentation/symptoms
Obstruction of one or both nostrils
Nosebleeds
Snoring, preference for sleeping on a certain side
Awareness of nasal cycle
Nasal septum deviation dx

speculum/endoscopy
Nasal septum deviation tx
Septoplasty
Decongestants
Antihistamines
Corticosteroid NS
Complications:
compensatory turbinate hypertrophy on non occluded side;
predispose to secondary disorders like rhinitis, sinusitis; nasal septal
hematoma
Nasal foreign body etio
Most common in children
Button batteries- if suspected/known = urgent referral, radiographs might be helpful if suspected but not visualized
Nasal oreign body presentation
Classically presents with epistaxis associated with unilateral, mucopurulent and foul smelling discharge, nasal obstruction
-mouth breathing
can also be largely asymptomatic
Nasal foreign body dx
Direct visualization with otoscope or endoscopy
Nasal foreign body tx
Remove via positive pressure technique or instrumentation
Positive pressure technique: having patient blow nose while occluding nose opposite of foreign body
Instrumentation: hemostat, forceps
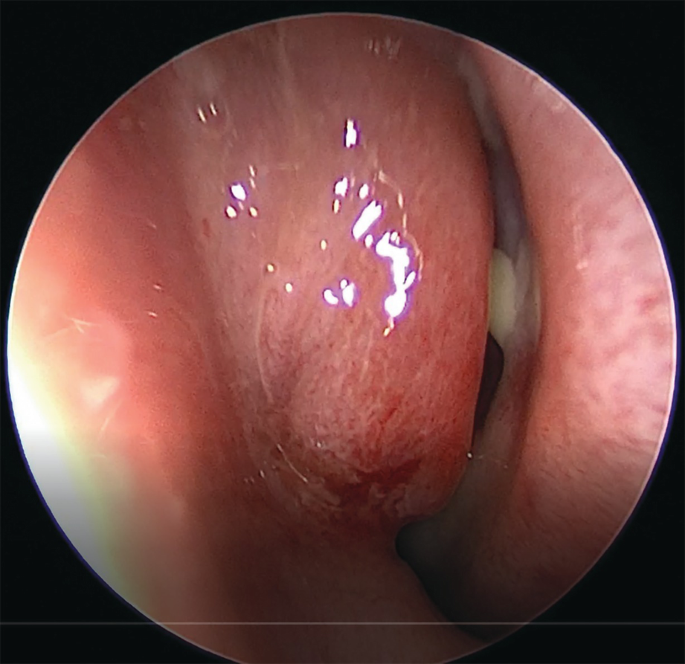
Nasal polyps etio
Allergic rhinitis most common cause, may be seen with CF
Nasal polyps presentation
Pale, boggy mass on the nasal mucosa. May have findings associated with allergic rhinitis
Nasal polyps dx
Most are incidental findings but if large, they can cause obstruction or anosmia
Nasal polyps tx
Intranasal corticosteroids are most effective
Surgical removal may be needed if medical therapy unsuccessful
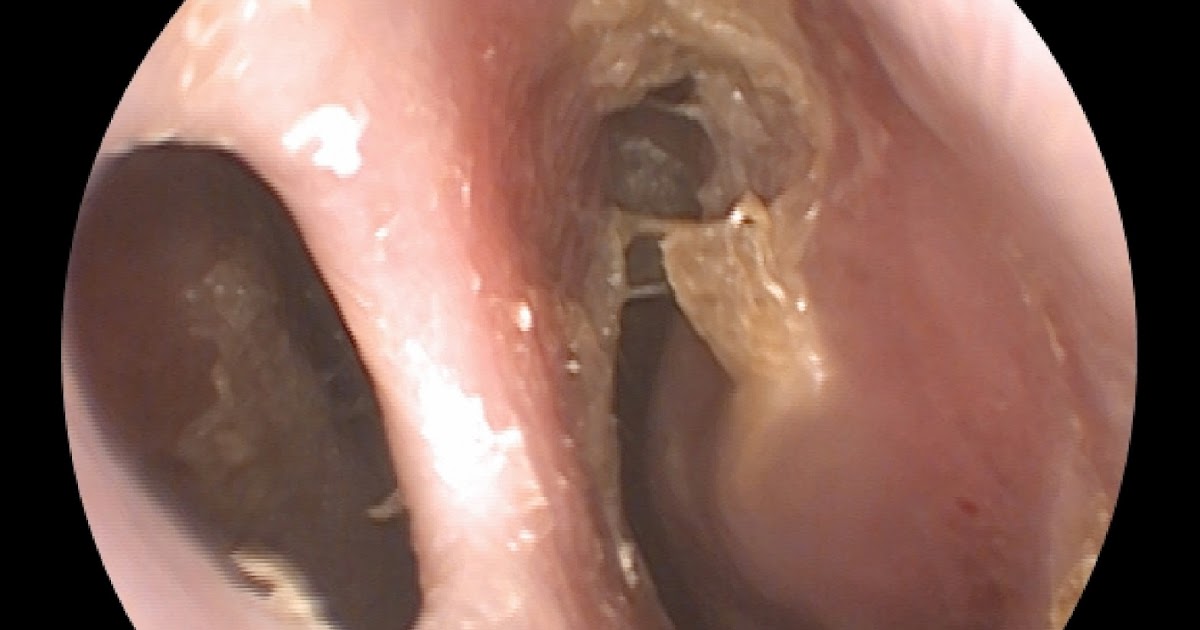
Chronic sinusitis etio/physio
Inflammation of the nasal cavity and paranasal sinuses for at least 12 consecutive weeks
etio = S. aureus is most common bacterial cause, Aspergillus is most common fungal cause, Mucormycosis is second most common fungal cause
RF = tobacco smokers
Chronic sinusitis presentation
Chronic obstruction, congestion (pain/pressure), mucopurulent nasal drainage, hyposmia, mucosa typically damaged, thickened and cilia spotty throughout sinus mucosa
Chronic sinusitis dx
CT
Biopsy or histology is diagnostic test of choice
Chronic sinusitis tx
Usually nasal issues -Allergies, polyps, turbinate disorders
Refer to ENT
Stop tobacco use
Abx if bacterial with ENT follow up
Amoxicillin, Augmentin, Doxycycline, Levo
Acute sinusitis etio/patho
Inflammation of the nasal cavity and paranasal sinuses, 1-4 weeks
Patho: same as in acute rhinosinusitis, usually URI precedes
Etio: mostly viral, very few actually bacterial
In order of frequency: Maxillary > ethmoid > frontal > sphenoid
Acute sinusitis presentation
in one or both nares, purulence, dental/facial pain, unilateral sinus tenderness, initial improvement but then worsening symptoms
10 days to 4 weeks of symptoms
Acute sinusitis dx
Acute sinusitis tx
Decongestants, antihistamines, analgesics, corticosteroid nasal spray
Abx if prolonged symptoms
antibiotics if bacterial cause, Amox, Augmentin, Doxy, Levofloxacin
Barosinusitis etio
Negative air pressure in one or more sinus cavities
Etio: acute forms with rapid change in ambient pressure (diving, URI, nasal blowing, high altitude), chronic forms with obstruction of usually maxillary sinus ostia
Barosinusitis presentation
Chronic sinus pain
Barosinusitis dx

Barosinusitis tx
Pain relief
Counsel: Avoid flying, diving, etc. during periods of
allergic/viral rhinitis or sinusitis
Benign tumor or masses in the nose
can be inverted papillomas = MC lateral nose wall/squamous papilloma
less common is hepangiomas = juvenile nasal angiofibroma
Malignant tumor or masses in the nose
rare = < 1%
malignancies in the nasal cavity typically present with nasal obstruction, congestion, proptosis, visual changes, diplopia, facial pain or numbness, and bleeding
late stages = cranial nerve palsies 2ndary to invasion of the skull base.
Squamous cell M/C
Hormonal/environmental rhinitis etio
dusty workplace, (major problem when cannot change exposure or wear mask) toxic fumes at work, wood stove, irritants with hobbies, factories nearby etc.
Hormonal/environmental rhinitis tx
Saline NS, Corticosteroid NS, try to adjust environmental factors if able
Drug-induced rhinitis patho
Cocaine abuse, anticholinergic meds, overuse of oxymetazoline NS, Reserpine, beta blockers, Hydralazine, OCPs, ACE inhibitors, PDE-5 inhibitors (Viagra)
nonallergic & noninfectious
Drug-induced rhinitis tx
Noninfectious, change offending med
Atrophic rhinitis etio
anatomical deformity of nasal septum, turbinates exacerbated by conditions
Usually in elderly
OMC (ostiomeatal complex) is a
complex drainage system; flow vs obstruction
lack of flow = drainage can cause pain, pressure, then lead to infection
Atrophic rhinitis presentation
Dry nose, frequent anterior nosebleeds
Atrophic rhinitis dx
Atrophic rhinitis tx
Premarin cream- estrogen cream, corticosteroid nasal spray
Medicamentosa Rhinitis definition
non-allergic form of rhinitis that is caused by prolonged use of topical nasal decongestants
Aka rebound congestion
Medicamentosa Rhinitis tx
Change medication
Counseled to not exceed 3 days of nasal decongestant management
Vasomotor rhinitis etio/patho
nonallergic & noninfectious dilation of the blood vessels
Patho: Imbalance of ANS activity in elderly
Often confused with allergic rhinitis (AR), which is uncommon in elderly
Vasomotor rhinitis presentation
Chronic dry nasal mucosa, clear rhinorrhea
Vasomotor rhinitis dx
Vasomotor rhinitis tx
None very satisfactory
Saline nasal spray, corticosteroid NS, Azelastine NS, Ipratropium NS, Avoid contributing meds (caution anti-cholinergics)
Bacterial rhinitis (ABRS) etio/patho
Bacteria infects sinus cavity; much less common than viral
Patho: Impaired sinus drainage: MC d/t complication of viral infection.
Also mechanical obstruction of nose, dental infections, impaired mucociliary clearance, smoking
Etio: S. pneumoniae, H influenzae, M. catarrhalis
More apt to be ethmoid sinusitis causing a rhinosinusitis
In order of frequency: Maxillary > ethmoid > frontal > sphenoid
Bacterial rhinitis (ABRS) presentation (maxillary, ethmoid, frontal, sphenoid)
Erythema or edema over involved area, purulent drainage in nose or posterior pharynx.
Maxillary MC check pain or pressure that can radiate to upper incisors.
Ethmoid: Tenderness to high lateral wall of nose
Frontal: Pain around eyes and forehead
Sphenoid: Mid head tenderness
Acute rhinosinusitis: Facial pain or pressure worse/localized with bending down & leaning forward, purulent nasal discharge, nasal congestion or obstruction, HA, fever <4 weeks.
Bacterial rhinitis (ABRS) dx
Clinical criteria for bacterial cause: Persistent symptoms that last 10 or more days w/o improvement, a biphasic pattern where symptoms initially improve then worse |
Bacterial rhinitis (ABRS) tx
Amox, Augmentin, Doxycycline for 5-7 days
Viral rhinitis etio
Common cold, symptomatic inflammation of the nasal cavity and paranasal sinuses
Acute = <4 weeks
Primarily due to ARS
Etio: Rhinovirus, influenza, parainfluenza,
Viral rhinitis presentation
Erythematous, engorged nasal mucosa w/o intranasal purulence
Symptoms: Nasal congestion & obstruction, clear rhinorrhea, hyposmia. Associated cough, HA, malaise
Viral rhinitis dx

Viral rhinitis tx
Supportive management: symptoms are self-limited, roughly 7-10 days Decongestants to promote sinus drainage, analgesics, antihistamines, mucolytics, intranasal glucocorticoids, analgesics, and saline irrigation may also be used Manifestations: Eustachian tube dysfunction, acute rhinosinusitis |
Allergic rhinitis etio
Inflammation of nasal mucosa due to allergen
Pollen, mold, dust etc.
Etio: IgE mediated, mast cell histamine release due to allergens
MC Rhinitis
allergic rhinitis presentation
Edematous, pale or violaceous boggy turbinates with cobblestone mucosa
Allergic “salute”, allergic “shiners”
May have avascular polyps originating in ethmoid sinuses and extending into nasal airway
Symptoms: Nasal mucosal edema, congestion, rhinorrhea
allergic rhinitis dx
allergic rhinitis tx
Antihistamines, Decongestants, systemic/topical, nasal corticosteroid sprays
Referral for immunotherapy
-Intranasal corticosteroids- most effective pharmacologic therapy for allergic rhinitis and polyps