integ: abpsych (mood disorder)
1/132
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
133 Terms
Emotion
refers to a brief, intense, and specific psychological state triggered by a particular event or circumstance.
typically more focused and have a clear cause.
Mood
more prolonged and generalized emotional state that is not necessarily tied to a specific stimulus
more diffuse and can last for a more extended period
Mood Disorders
When mood episodes become intense and prolonged, cause distress and dysfunction
Major Depressive Episode
2
Lowest point of mood. Intense form of low affect.
most commonly diagnosed and most severe depression
extremely depressed mood state that last at least how many weeks
Major Depressive Episode
includes cognitive symptoms
includes disturbed physical functions
somatic or vegetative symptoms
distrubed physical functions in major depressive episode is also called?
disturbed physical functions and cognitive symptoms
most central indicators of a full major depressive episode
disturbed physical functions
altered sleeping patterns, significant changes in appetite and weight, or a notable loss of energy
cognitive symptoms in major depressive episode
feelings of worthlessness and indecisiveness is called?
anhedonia
episode is typically accompanied by a general loss of interest in things and a inability to experience any pleasure in life
more characteristic of severe episodes of depression than are reports of sadness and distress
4-9 months
duration of a major depressive episode, if untreated
5 or more
how many symptoms should be present in the 2-week period to be classified as major depressive episode?
major depressive episode
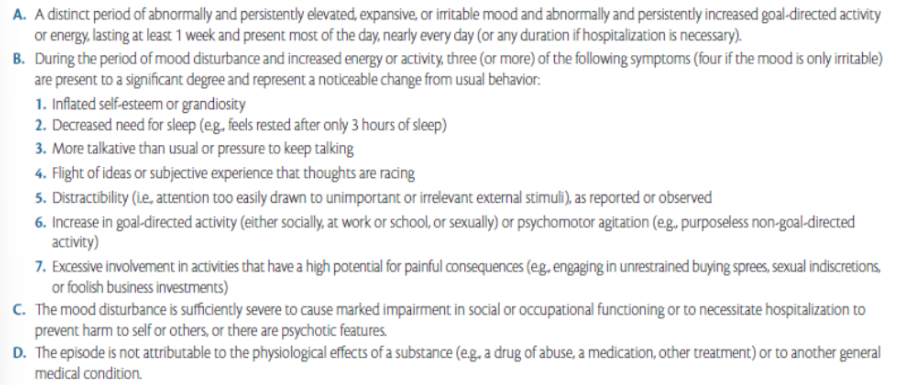
Mania
individuals find extreme pleasure in every activity
they become extraordinarily active (hyperactive), require little sleep, and may develop grandiose plans, believing they can accomplish anything they desire
“persistently increased goal-directed activity or energy”
flight of ideas
1 week and less
manic episode criteria require a duration of only how many if the episode is severe enough to require hospitalization
flight of ideas
speech is typically incoherent, because the individual is attempting to express so many exciting ideas at once
irritability
often part of a manic episode, usually near the end duration of a manic episode
3-4 months
if manic episode is untreated, it could persist until how many months
Hypomania
less severe version of a manic episode that does not cause marked impairment in social or occupational functioning
the episode is below the level of a manic episode
4 days
hypomania need to only last how many days to fit to the criteria
3
4
how many symptoms are needed for manic episide
how many are needed if the mood is only irritable
manic episode, therefore a bipolar i diagnosis
a full manic episode that emerges during antidepressant treatment (medication, electroconvulsive theraot) but persists at a fully syndromal level beyond the physiological effect of that treatment is sufficient evidence of a?
manic episode
Unipolar Depressive Disorders
disorders in which a person experiences only depressive episodes
individuals who experience either depression or mania
their mood remains at one “pole” of the usual depression—mania continuum
mania by itself (unipolar mania) probably does occur but seems to be rare, because most people with this disorder develop depression
Disruptive Mood Dysregulation Disorder
chronic, severe persistent (non-episodic) irritability through frequent verbal and/or behavioral temper outbursts in response to frustration and persistent irritable or angry mood between the outbursts
pervasive irritability, and intolerance of frustration
6 years
Disruptive Mood Dysregulation Disorder should not be applied to children with a developmental age of less than?
Disruptive Mood Dysregulation Disorder
Must be before age 10 years and likely to change as children mature
disruptive mood dysregulation disorder
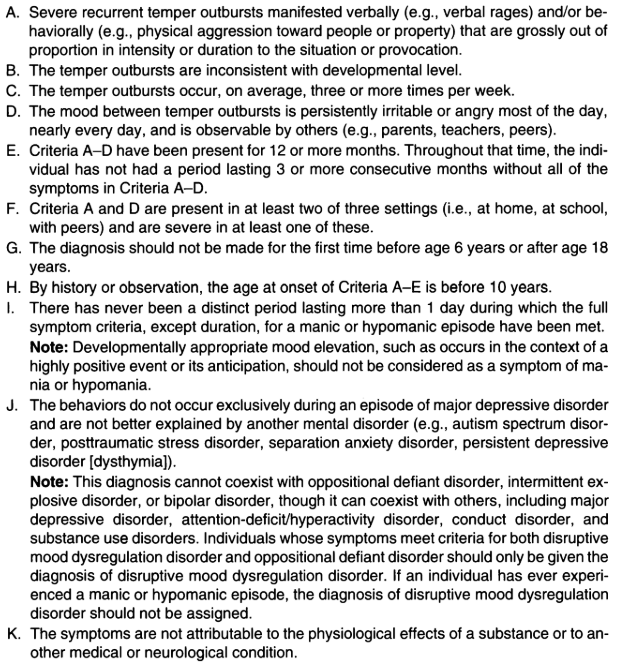
oppositional defiant disorder (ODD)
what disorder is the stronger overlap of disruptive mood dysregulation disorder
Integrated Grief
an acute form of grief in which the finality of death and its consequences are acknowledged and the individual adjusts to the loss
Often recurs at significant anniversaries
Considered as a natural way of confronting and handling loss
Occasional hallucinatory experiences of the deceased may occur
Complicated Grief
persistent intense symptoms of acute grief
Can develop without a preexisting depressed state
Presence of thoughts, feelings, or behaviors reflecting excessive or distracting concerns about the circumstances or consequences of the death
Psychodynamic theory of depression
Freud believed we unconsciously hold negative feelings toward those we love, in part because of their power over us
Depression is anger turned inward
Behavioral theory of depression
People become depressed when their responses no longer produce positive reinforcement or when their rate of negative experiences increase
beck’s cognitive theory theory of depression
Negative cognitions lead to dysfunctional beliefs
Ruminative Response Styles Theory
tend to dwell too much (ruminate) on how they feel and why they feel that way
Attributional Style
ways in which people explain the cause of events within their lives
Internal-External
Who or what is responsible for the event
Whether something unique about the person or something about the situation caused the event
Stable-Unstable
Perceived permanence of the cause
An event can be viewed as constant and likely to happen again (stable) or it only happens once (unstable)
Global-Specific
Universal throughout your like or specific to a part of your life
Cognitive Theory of Depression
persons susceptible to depression develop inaccurate/unhelpful core beliefs about themselves, others, and the world as a result of their learning histories
Depressed people constantly think in illogical ways and keep arriving at self-defeating conclusions
They tend to overgeneralize / draw broad negative conclusions on the basis of single insignificant event
Depressive Cognitive Triad
depressed people make cognitive errors in thinking negatively about themselves, immediate world, and their future
Negative Schema
a deep belief or mindset you develop about yourself, others, or the world—usually from past experiences—that makes you see things in a negative or distorted way.
a learned negative belief that affects how you think, feel, and behave.
ex: “The world is unsafe” (World schema)
Situation: You meet new people
Thought: “They might hurt or judge me”
👉 Leads to fear or avoidance
Self-Blame Schema
people feel personally responsible for every bad happenings
Negative Self-Evaluation Schema
“can never do anything correctly”
False Consensus Effect
Also called False Consensus Bias
People tend to overestimate the extent to which their opinions, beliefs, preferences, values, and habits are normal and typical of the others
believing your opinions, choices, or behaviors are more common than they really are
ex: You dislike a certain teacher
You think: “Almost everyone hates that teacher”
👉 But others might actually like them
Dichotomous Thinking
Also called absolutist / black and white thinking
Seeing only of the extremes of things, never the middle (e.g., good or bad, success or failure)
ex: Your friend forgets to reply
Thought: “They’re a bad friend”
👉 No consideration of other reasons
Overgeneralization
Making generalizations about a negative aspect
when you take one experience and make a broad conclusion as if it always happens.
ex: One person rejects you
Thought: “No one will ever like me”
👉 You generalize to everyone
Personalization
Tendency for individuals to relate external events to themselves, even when there is no basis for making this connection
Egocentric thinking
Selective Abstraction
when you focus only on one negative detail and ignore all the positive or important parts of a situation
ex: People applaud, but one person looks bored
Thought: “My presentation was terrible”
👉 Focusing only on one reaction
Arbitrary Inference
You make a conclusion without enough evidence (or even with evidence against it)
ex: Your teacher looks serious
→ “She’s mad at me” (no proof)
Labeling and Mislabeling
Portraying one’s identity on the basis of imperfections and mistakes made in the past and allowing them to define one’s true identity
Minimization
Downplaying the significance of an event or emotion
Common strategy in dealing with feelings of guilt
Magnification
Effect of one’s behaviors are magnified
Stress-Appraisal/Cognitive Appraisal Theory
stress is a two-way process, it involves a production of stressors and the response of an individual subjected to these stressors
Primary Appraisal
understanding the stressor
Secondary Appraisal
involves those feelings related to dealing with the stressor or the stress it produces
Monoamine Theory of Depression
depression as a result of a deficiency in serotonin, norepinephrine, and dopamine
Suicide
process of killing oneself
Suicide Ideation
thinking seriously of suicide
Suicidal Plans
formulation of a specific method for killing oneself
Suicidal Attempts
person survives
Egoistic
Stemming from absence of social integration
Committed by social outcasts
Suicide is a solution to free themselves from loneliness
Altruistic
when a person takes their own life because they believe it will help others or benefit a group.
ex: A person in a very strict community feels they must die to bring honor to their family
Anomic
when a person feels lost, confused, or without direction because of sudden changes in their life or society.
ex: Someone loses their job and feels their life has no purpose
Fatalistic
Occurs when individuals are kept under tight regulation
When extreme rules or high expectations set on them
Interpersonal Psychological Theory of Suicidal Behavior
Proposed that an individual will not die by suicide unless they have both the desire to die by suicide and the ability to do so
Attempts to explain why individuals engage in suicidal behavior and to identify individuals who are at risk
Developed by Thomas Joiner
Fluoxetine (Prozac) – best known
SSRIs treatemtn for depression
Venlafaxine (Effexor) – best known
Mixed Reuptake Inhibitors TREATMENT FOR DEPRESSION
Tricyclic Antidepressants
Most widely used treatment before SSRI
Imipramine (Tofranil) and amitriptyline (Elavil) – best known
Tricyclic Antidepressants
Monoamine Oxidase (MOA) Inhibitors
Block the enzyme MAO that breaks down such neurotransmitters as norepinephrine and serotonin
Used far less often because of two potentially serious consequences: hypertensive episodes or death, when eating and drinking foods and beverages containing tyramine
Lithium Carbonate (Lithium)
Found in drinking water
Side effects: toxicity (poisoning), lowered thyroid functioning, substantial weight gain
Major advantage: effective in preventing and treating manic episodes
Most often referred to as a ‘mood-stabilizing drug’
Cognitive-Behavioral Therapy (CBT)
Learn to replace negative depressive thoughts and attributions with more positive ones
Develop more effective coping behaviors and skills
Interpersonal Psychotherapy (IPT)
Focus on the social and interpersonal triggers for their depression (such as the loss of a loved one)
Develop skills to resolve interpersonal conflicts and build new relationships
Electroconvulsive Therapy (ECT)
Most controversial treatment for psychological disorders after psychosurgery
Electric shock is administered directly through the brain for less than 1 second, producing a seizure and a series of brief convulsions that usually lasts for several minutes
Major Depressive Disorder
persistent depressed mood and/or loss of interest or pleasure nearly most of the day every day for at least two weeks
require that a person must be in a major depressive episode and never have had a manic, hypomanic, or mixed episode
Recurrent Episode
preceded by one or more previous episodes
Single Episode
first depressive episode
2 months
While most depressive episodes remit (at least how many months), depressive episodes often return at some point
Relapse
return of symptoms within a fairly short period of time
Recurrence
onset of a new episode of depression
puberty
Likelihood of onset increases markedly with
major depressive disorder
Considered as the most common mood disorder and second most prevalent type of disorder following anxiety disorders
2:1 ratio
major depressive disorder is higher for women than for men at a how many ratio
major depressive disorder
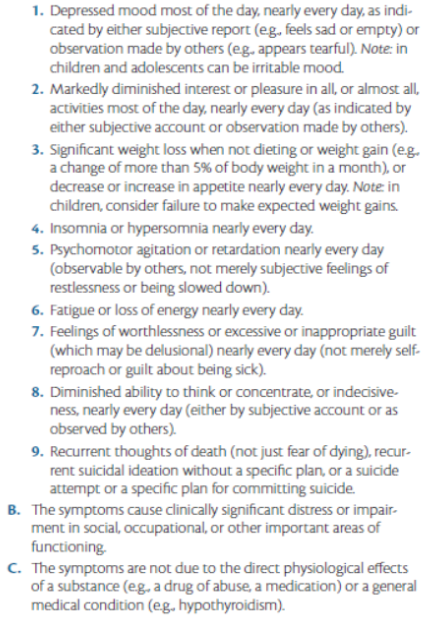
Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning: at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
Note: Do not include symptoms that are clearly attributable to another medical condition.
1. Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g., feels sad, empty, hopeless) or observation made by others (e.g., appears tearful). (Note: In children and adolescents, can be irritable mood.)
2. Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation).
3. Significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day.
(Note: In children, consider failure to make expected weight gain.)
4. Insomnia or hypersomnia nearly every day.
5. Psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down).
6. Fatigue or loss of energy nearly every day.
7. Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self-reproach or guilt about being sick).
8. Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others).
9. Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
C. The episode is not attributable to the physiological effects of a substance or to another medical condition.
Note: Responses to a significant loss (e.g., bereavement, financial ruin, losses from a natural disaster, a serious medical illness or disability) may include the feelings of intense sadness, rumination about the loss, insomnia, poor appetite, and weight loss noted in Criterion A,which may resemble a depressive episode. Although such symptoms may be understandable or considered appropriate to the loss, the presence of a major depressive episode in addition to the normal response to a significant loss should also be carefully considered. This decision inevitably requires the exercise of clinical judgment based on the individual’s history and the cultural norms for the expression of distress in the context of loss.
Chronic
Used when a person meets the criteria for a Major Depressive Episode continuously for the past two years
Anxious Distress
Used when a person also exhibits abnormal movements, immobility, abnormal behaviors, and withdrawal
Melancholic Features
3 of the following:
Early morning awakening
Depression worse in the morning
Marked psychomotor agitation/retardation
Loss of appetite/weight
Excessive guilt
Quantitatively different depressed mood
More heritable
Associated childhood trauma
Psychotic Features
Delusions or hallucinations (usually mood congruent)
Feelings of guilt and worthlessness are common
Poorer long-term prognosis
Atypical Features
Mood reactivity: brightens to positive events
2 of the 4 following symptoms:
Weight gain/increase in appetite
Hypersomnia
Leaden paralysis
Acutely sensitive to interpersonal rejection
More common in females
Responds to different class of antidepressant (MAOI)
Mood-Congruent Psychotic Features
Material of the hallucinations is related to being depressed
Ex. seeing demons or dark characters
Mood-Incongruent Psychotic Features
When material of hallucinations has nothing to do with being depressed
Ex. delusions of grandeur
Associated with poorer prognosis
Catatonic Features
Range of psychomotor symptoms from motoric immobility to extensive psychomotor activity, as well as mutism and rigidity
Peripartum Onset
Used if the onset of MDD occurs in close proximity (within 4 weeks) to childbirth
mood fluctuations and excessive preoccupation with the infant's well-being
Seasonal Pattern (recurrent episode only)
At least 2 or more episode in the past 2 years that have occurred at the same time (usually fall or winter)
Full remission at the same time (usually spring)
No other nonseasonal episodes in the same 2-year period
Also called seasonal affective disorder
Mixed Features
Experiences of manic symptoms but feel somewhat depressed or anxious at the same time
Neuroticism
a well-established risk factor for the onset of major depressive disorder
High levels appear to render individuals more likely to develop depressive episodes in response to stressful life events
Females
have higher risk in suicide attempts
Suicide Risk
have higher risk in suicide completion due to violent forms
Persistent Depressive Disorder
depressed mood most of the day, for more days than not, for at least 2 years