BIOL 4160, Module 7.b: Modification of Glomerular Ultrafiltrate (Boswell)
1/198
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
199 Terms
The initial ___ is modified as it flows through the tubular nephron forming the final urine
glomerular ultrafiltrate
The initial glomerular ultrafiltrate is modified as it flows through the ___ forming the final urine
tubular nephron
The initial glomerular ultrafiltrate is modified as it flows through the tubular nephron forming the ___
final urine
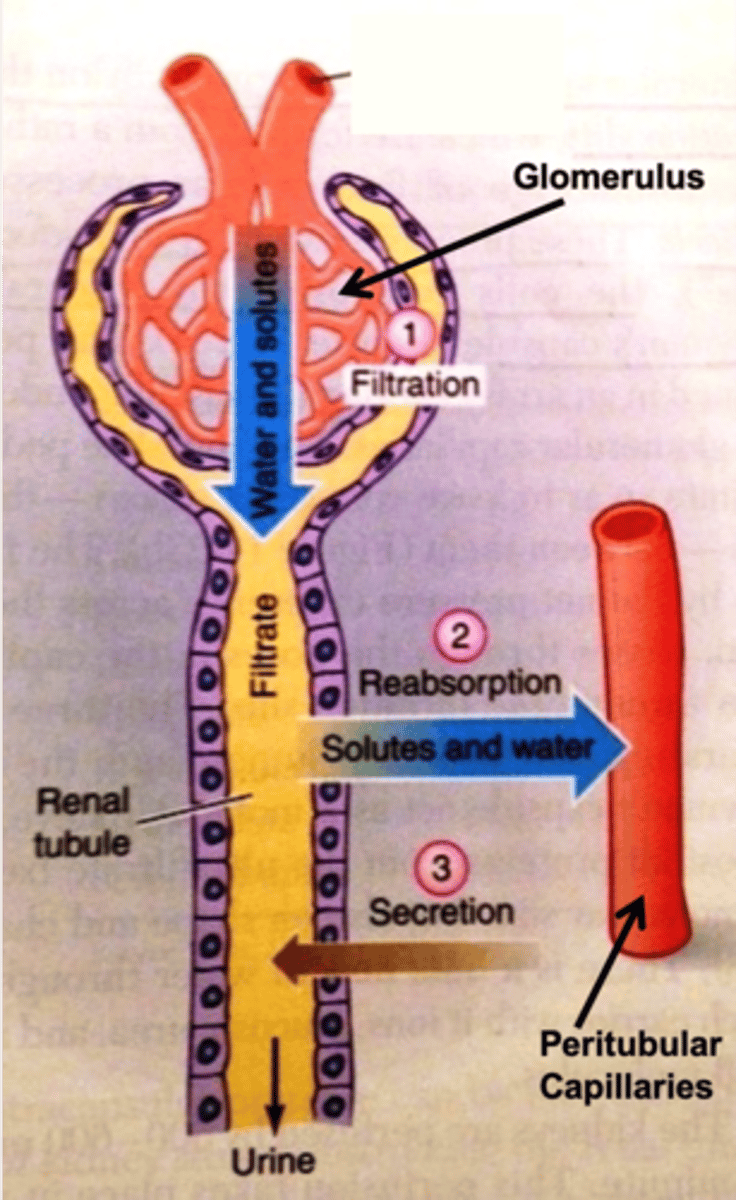
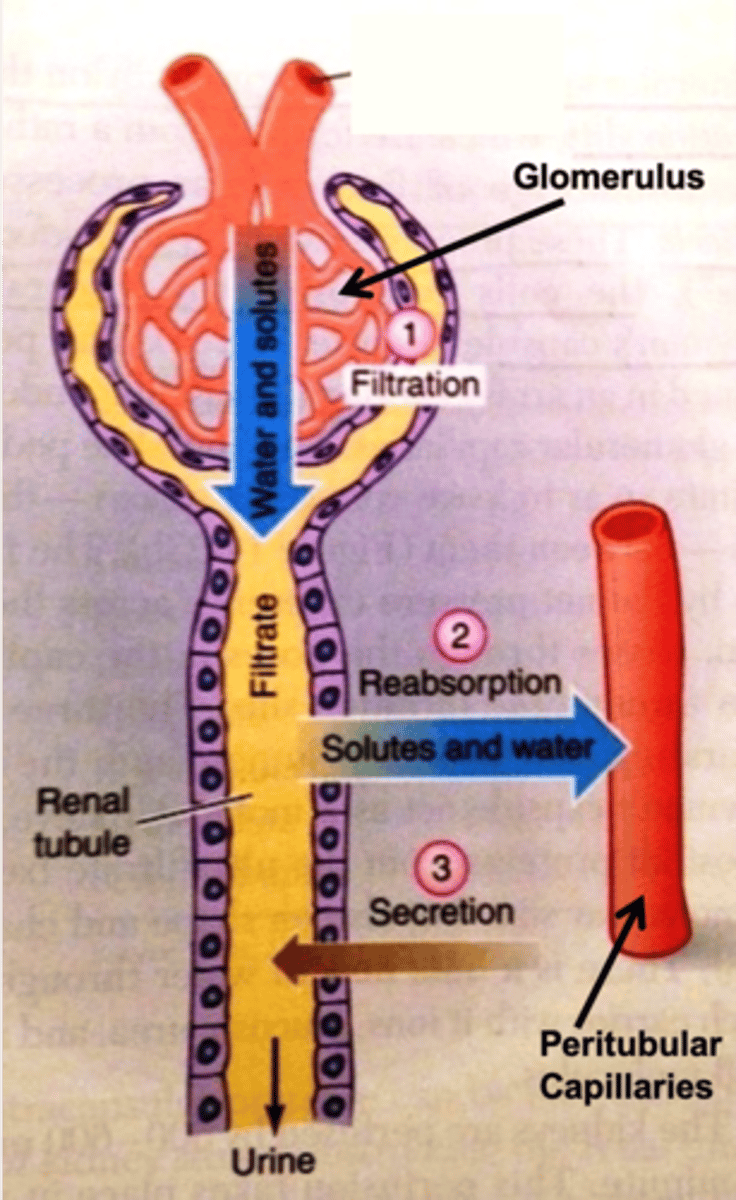
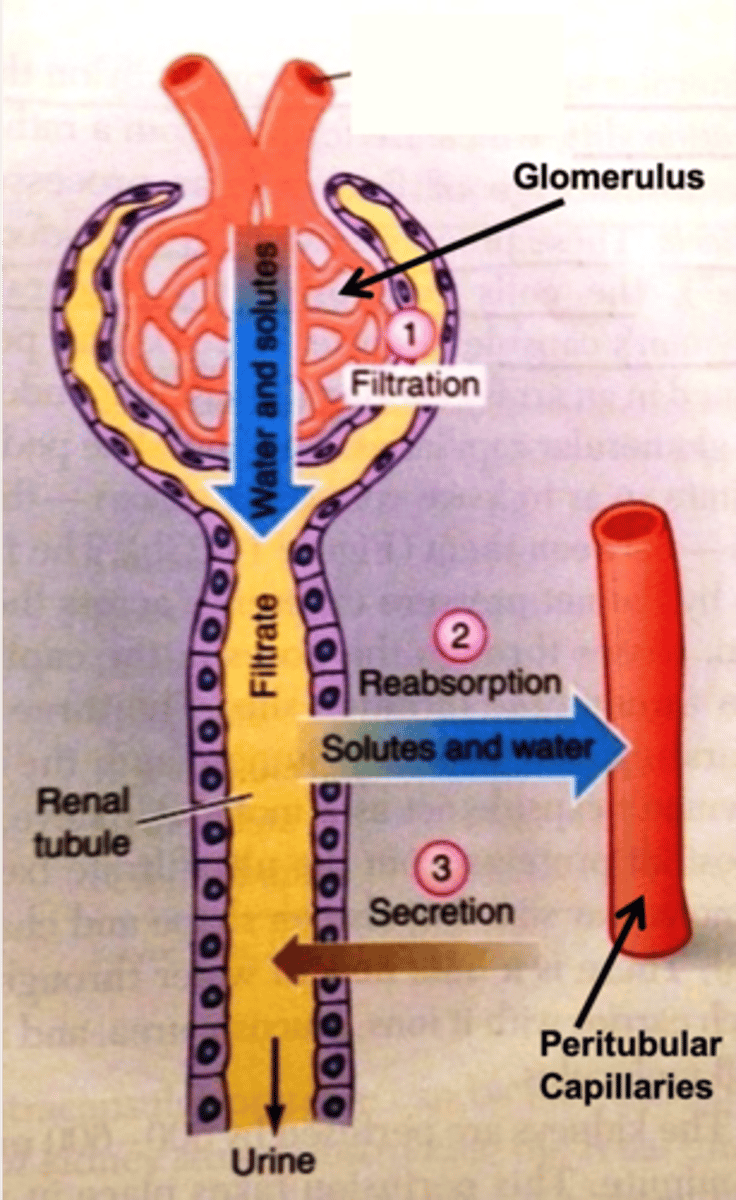
As the initial glomerular ultrafiltrate flows through the tubular nephron, which two major processes occur?
- Reabsorption of filtered materials from the tubular lumen into the kidney (interstitium/peritubular capillaries)
- Secretion of non-filtered materials from the peritubular capillaries into the tubular lumen
___ of filtered materials occurs from the tubular lumen into the kidney interstitium/peritubular capillaries
reabsorption
___ of nonfiltered materials occurs from the peritubular capillaries into the tubular lumen
secretion
In which "direction" does reabsorption take place in the tubular nephron?
from the tubular lumen into the kidney interstitium/peritubular capillaries
In which "direction" does secretion take place in the tubular nephron?
from the peritubular capillaries into the tubular lumen
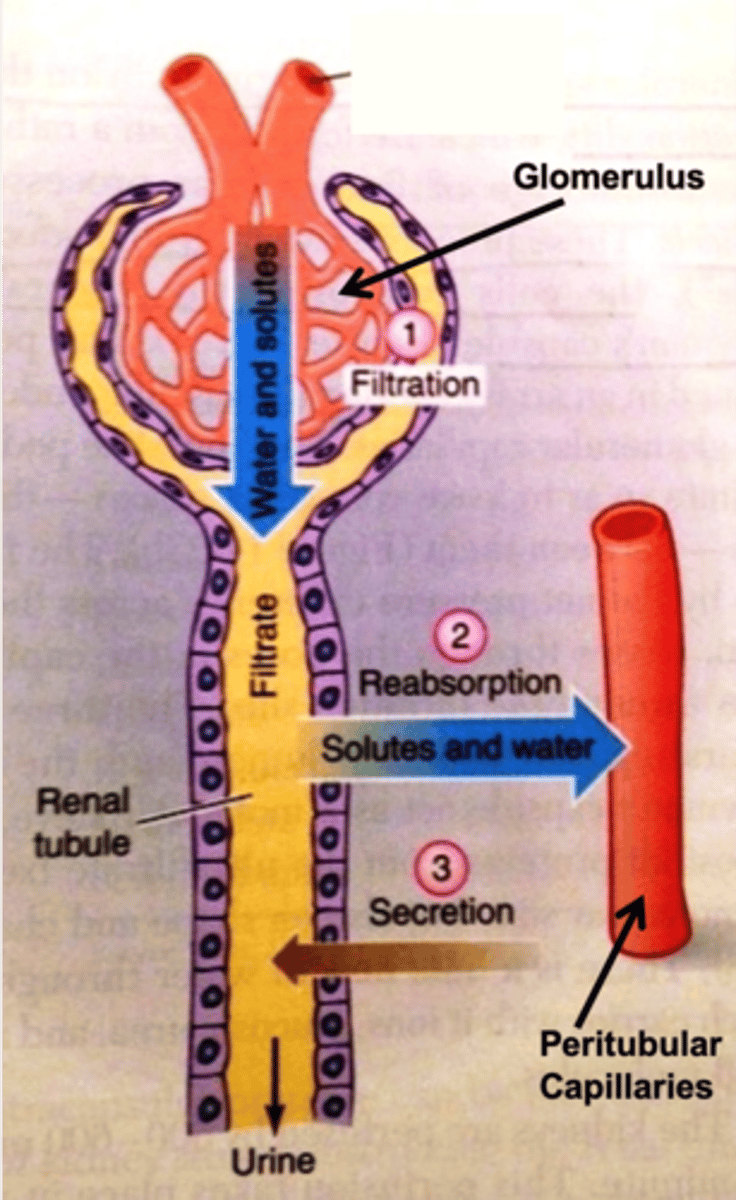
What are the four steps in the nephron in the process of forming the final urine?
1. filtration (glomerulus)
2. reabsorption (peritubular capillaries)
3. secretion (peritubular capillaries)
4. exretion
How does the concentration/components of the initial glomerular ultrafiltrate (filtration step) compare to that of the blood?
- same concentration (without plasma proteins)
In what vascular location does reabsorption occur in the nephron?
peritubular capillaries
Why does a lot of blood volume have to be reabsorbed?
a lot of blood volume was initially filtered out (need to take some back or you will have no blood volume by the end of the day)
How does secretion of non-filtered materials aid in the process of creating the final urine?
- Aids in the efficiency of ridding the body of excess or foreign material
- Taking components from the blood that were not filtered (selectively putting those materials in the ultrafiltrate)
portion of the nephron involved in 75% of all reabsorption
proximal tubule
portion of the nephron involved in countercurrent multiplication
loop of Henle
portion of the nephron that is involved in regulated reabsorption/secretion
late distal tubule/collecting duct
What is the "regional specialization" of the proximal tubule?
involved in 75% of all reabsorption
What is the "regional specialization" of the loop of Henle?
involved in countercurrent exchange
What is the "regional specialization of the late distal tubule/collecting duct?
regulated reabsorption/secretion
What is the order of the tubular components of the nephron?
- Bowman's capsule
- Proximal tubule
- Loop of Henle (Descending and Ascending)
- Distal Tubule
- Collecting duct
What is the regional specialization of each portion of the nephron attributed to?
attributed to specific permeability and transport characteristics of the local tubular epithelium (i.e., which plasma proteins are expressed)
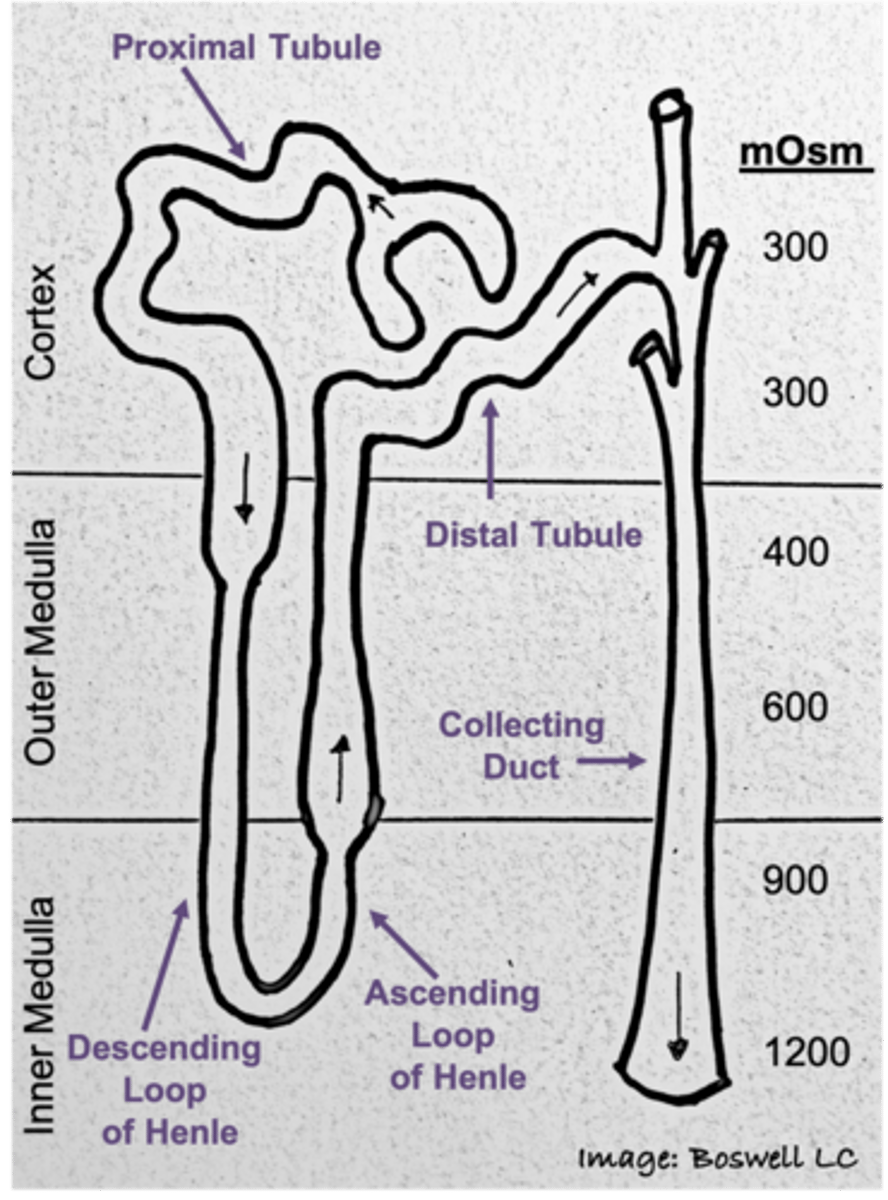
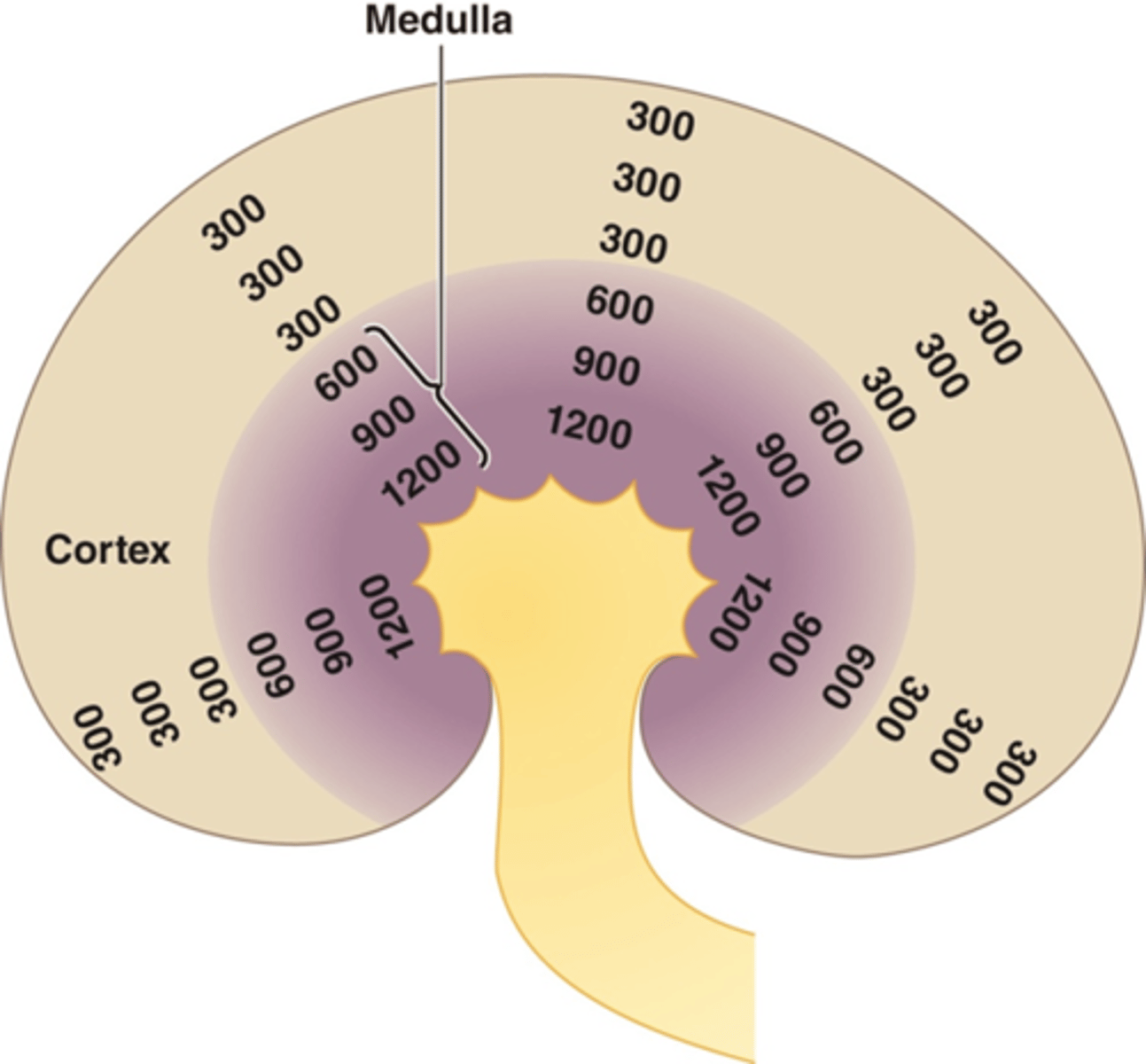
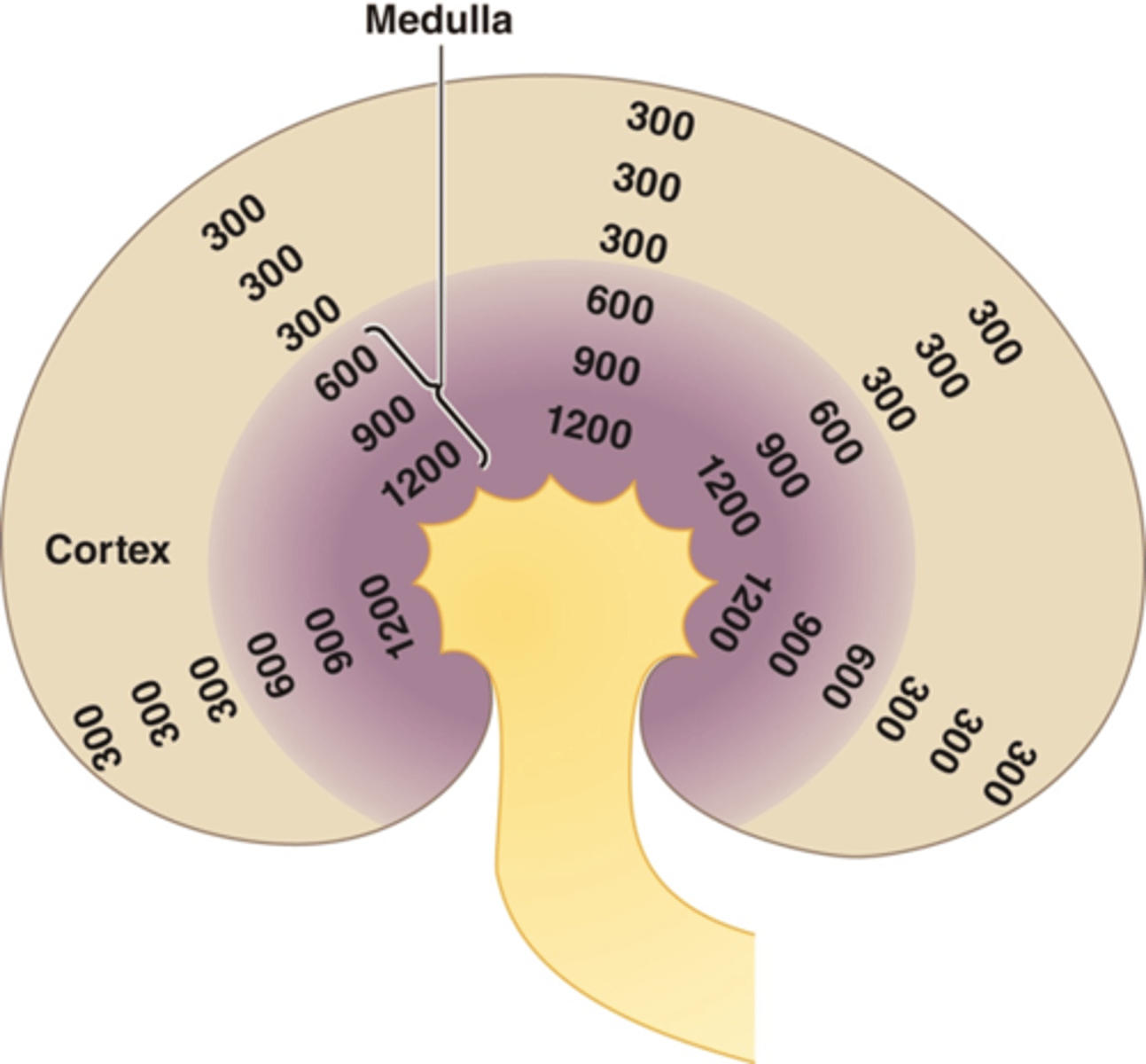
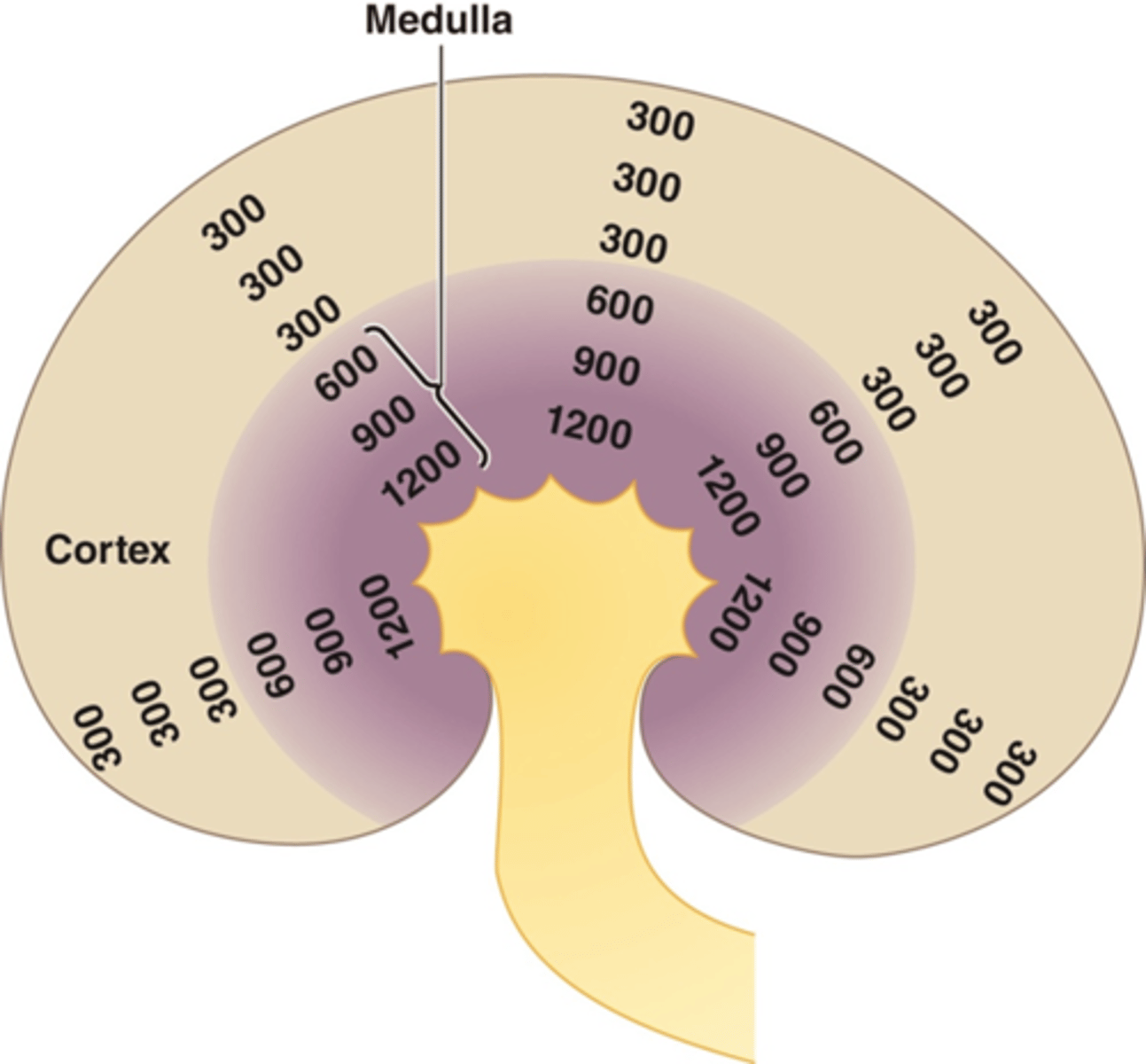
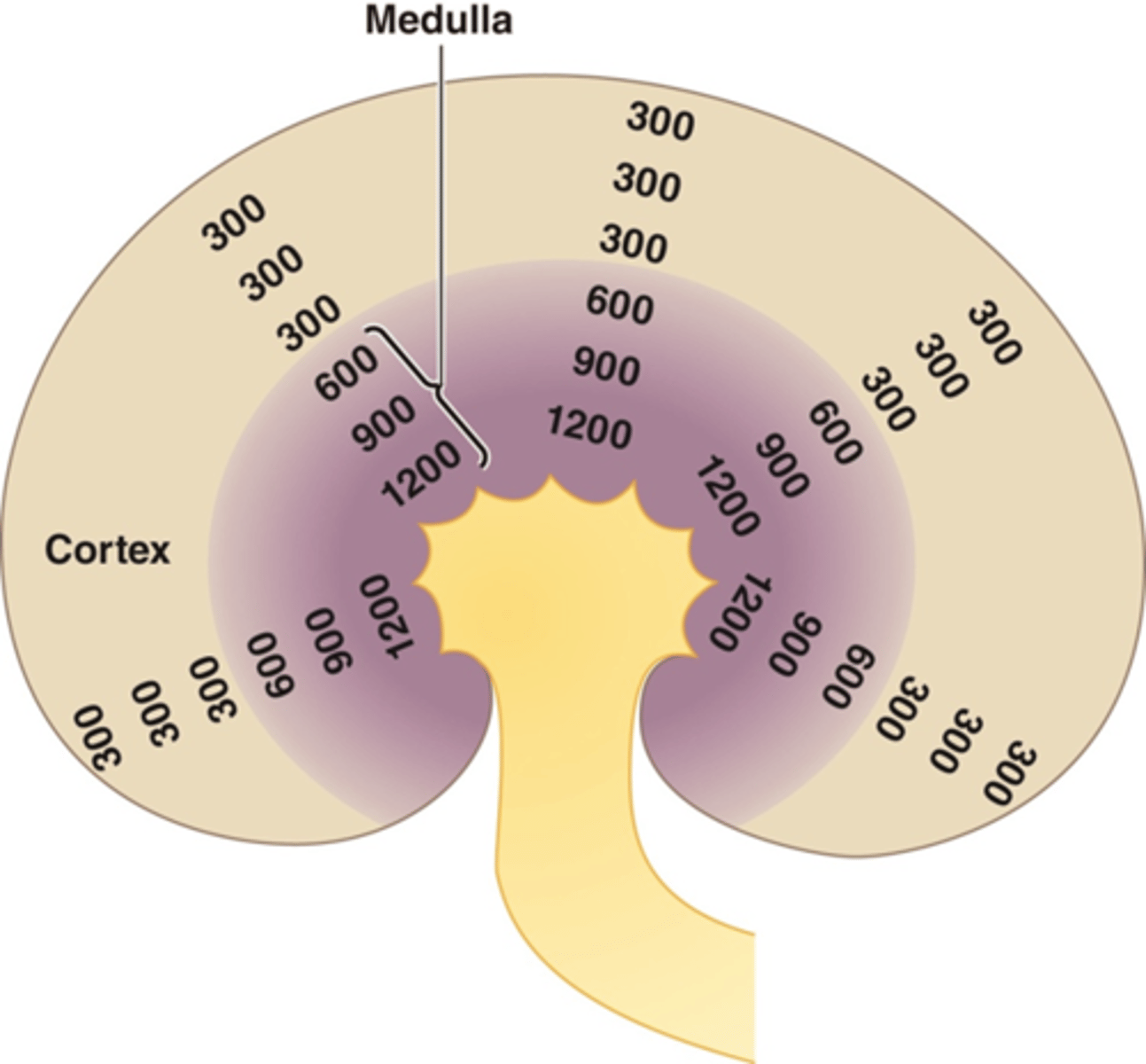
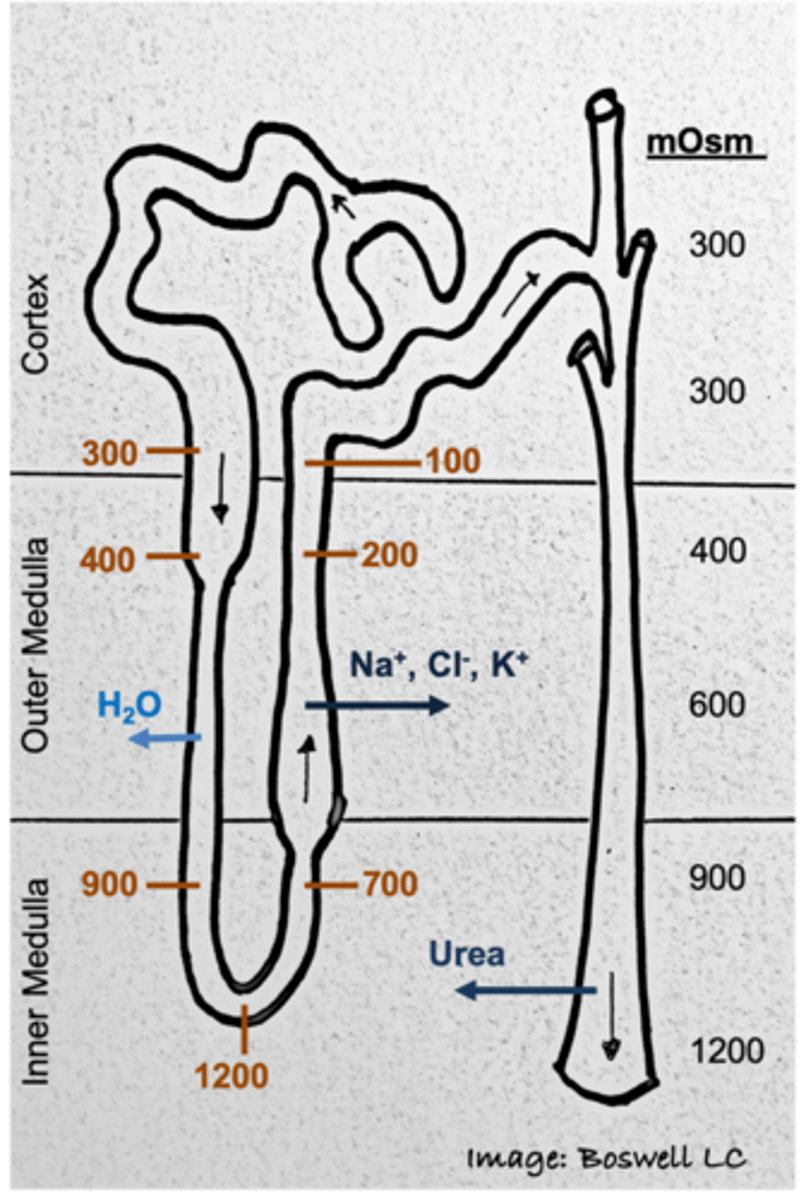
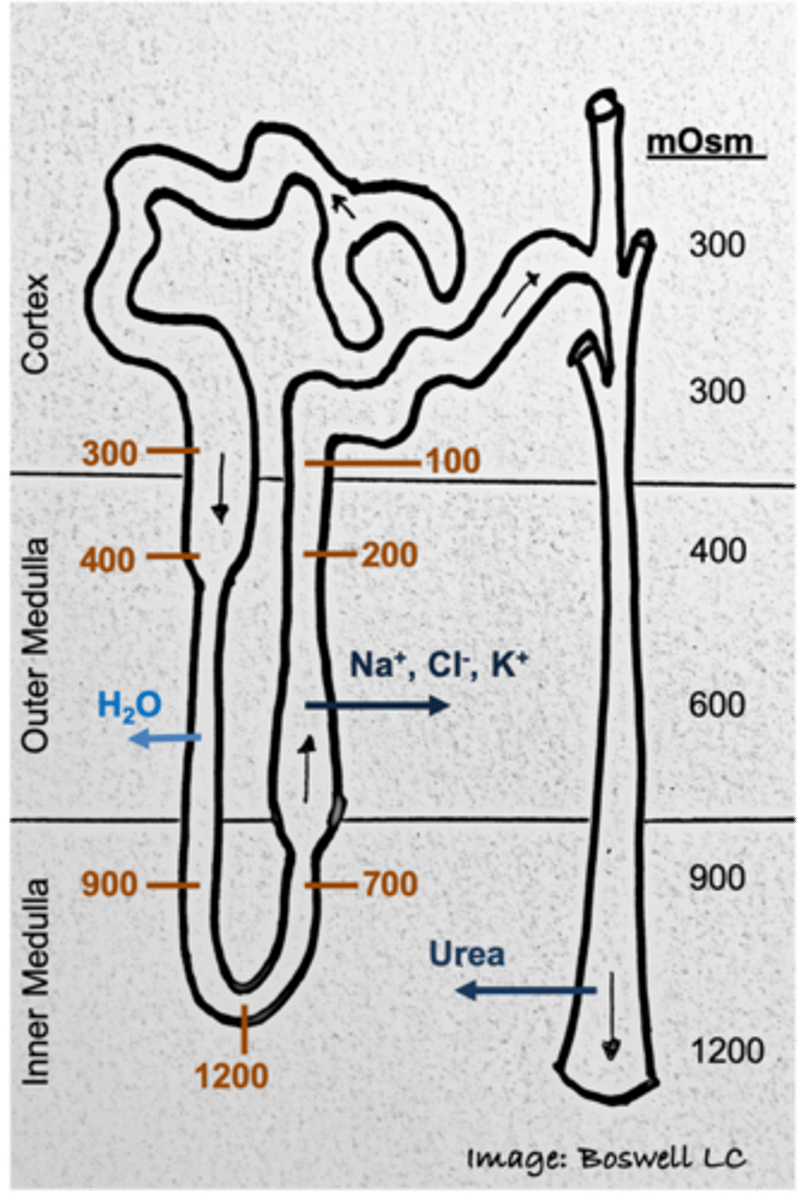
What kind of gradient exists within the tubular nephron?
osmotic gradient (300 mOsm to 1200 mOsm)
In the cortex of the kidney (outer portion) what is true of the osmolarity compared to plasma osmolarity?
osmolarity of interstitial fluid is equivalent to plasma (300 mOsm)
What happens to the osmolarity of the kidney as you go down into the medulla?
the interstitial fluid will get more concentrated
What is the osmolarity of the most concentrated portion of the kidney? Where is this located?
1200 mOsm; within the inner medulla
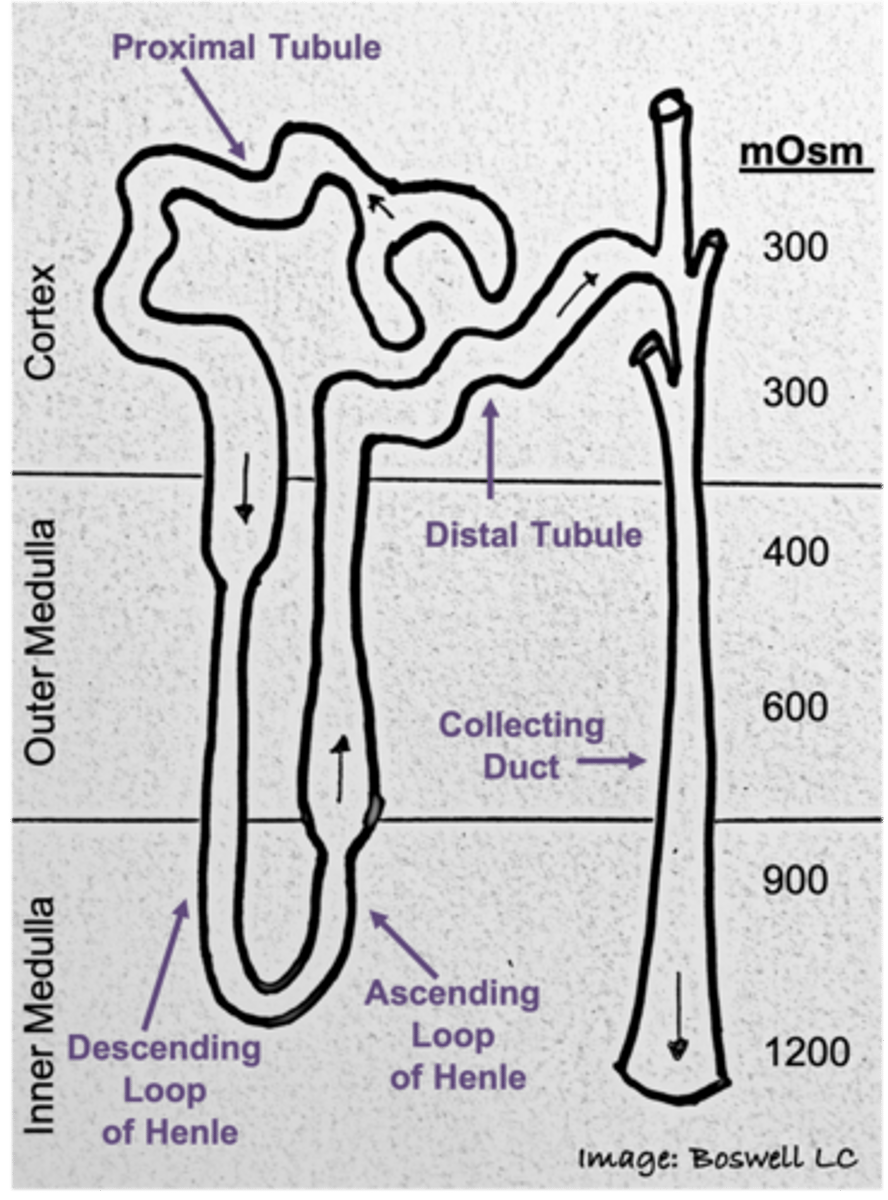
Gradient in the surrounding fluid of the kidneys as you go down into the medulla
Medullary osmotic gradient
In the ___ is where we see 75% of all reabsorption
proximal tubule
process by the loop of Henle that generates/maintains the medullary concentration gradient
countercurrent multiplication
Which region of the nephron is responsible for the concentration gradient seen in the interstitial fluid of the medulla of the kidneys?
loop of Henle
What does the late distal tubule/collecting duct base the regulated reabsorption/secretion of materials on?
the state of the body (ex: body status)
The Proximal tubule reabsorbs about ___% of filtered materials
75%
Which filtered materials are reabsorbed by the proximal tubules?
- Glucose and amino acids
- Electrolytes (ions: Cl-, Na+, K+)
- Water (iso-osmotic)
T/F: Reabsorption in the proximal tubule occurs due to the state of the body.
False; this will occur no matter what; no matter the status of the body, we will reabsorb about 75% of all filtered materials by the time we get to proximal tubule
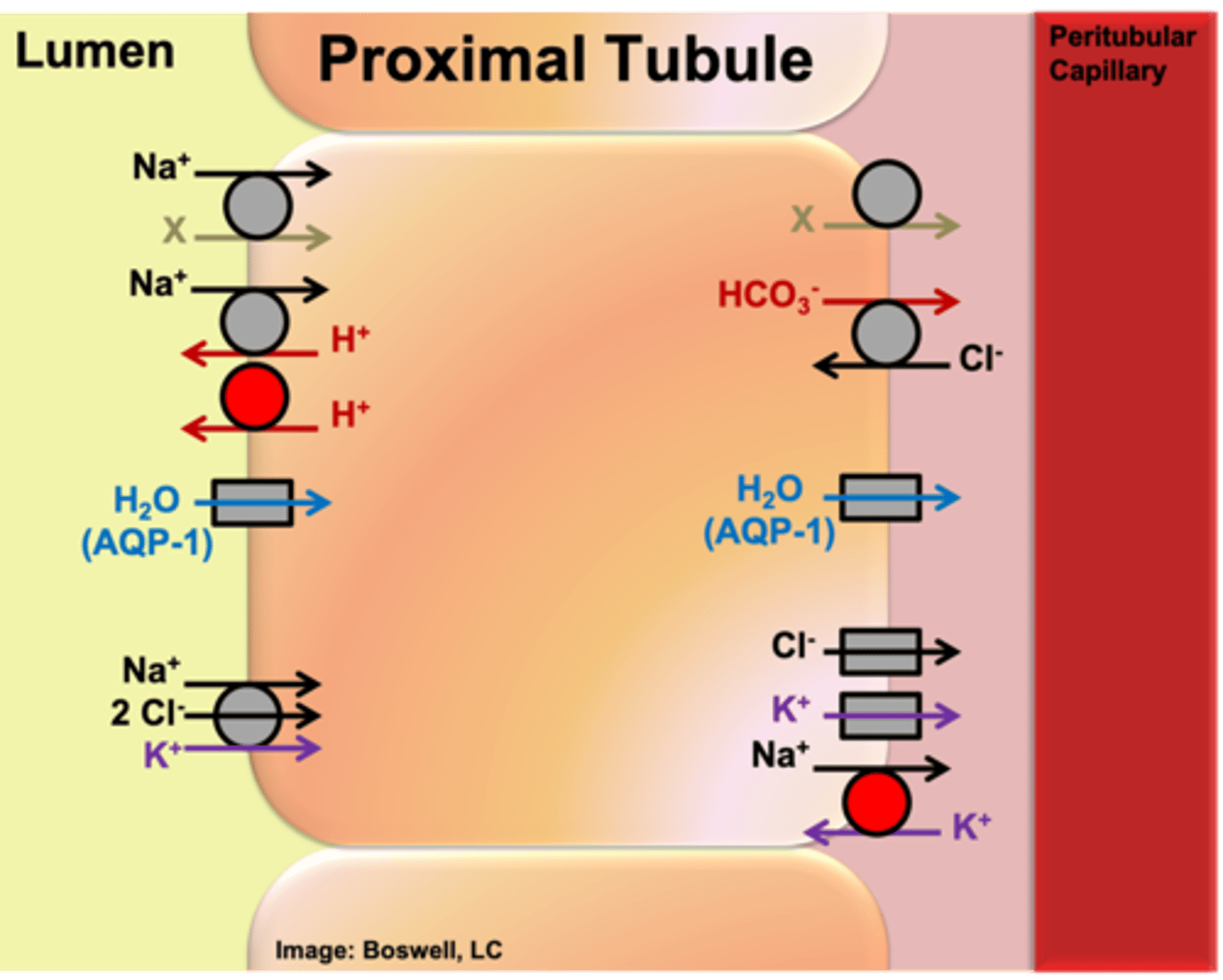
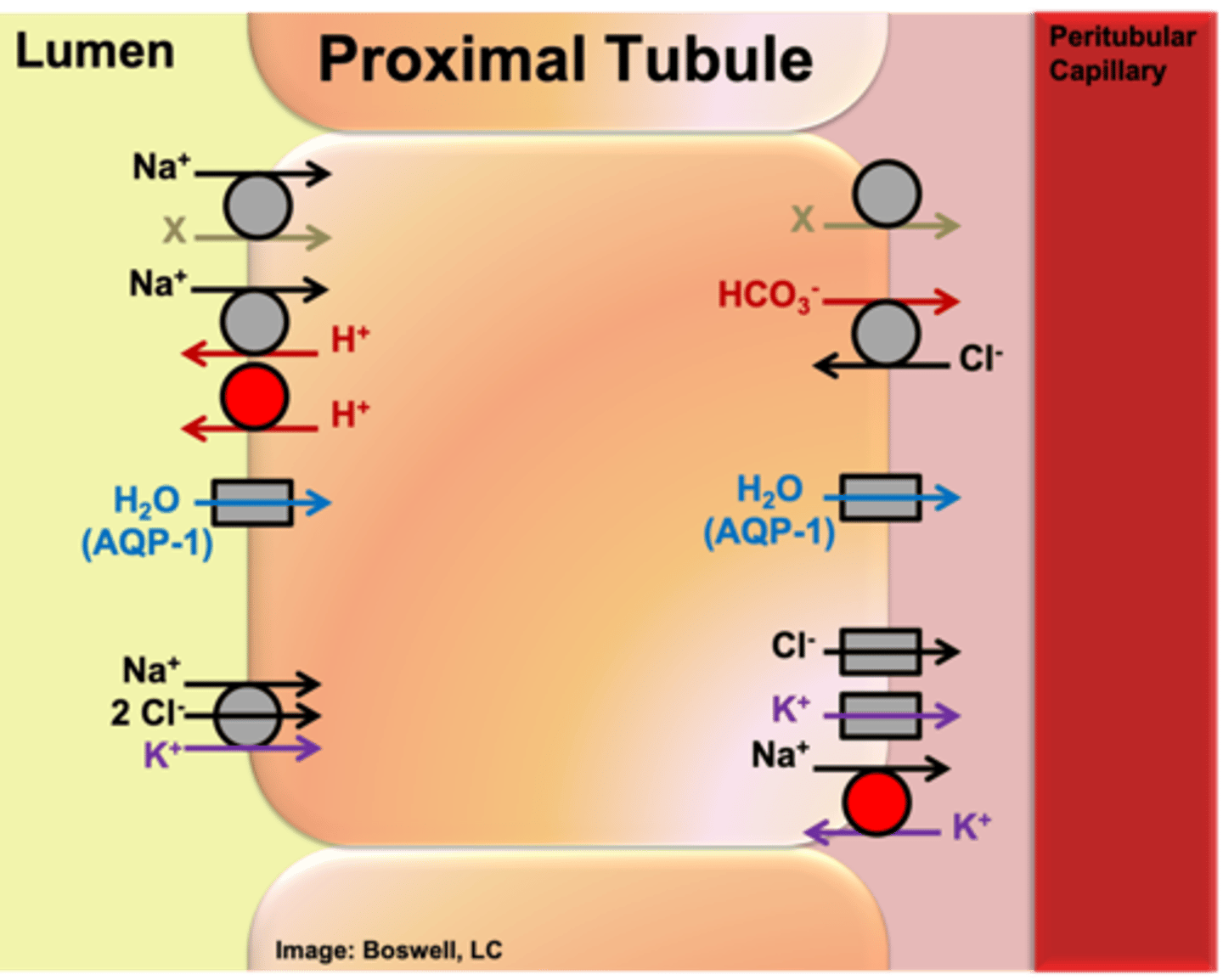
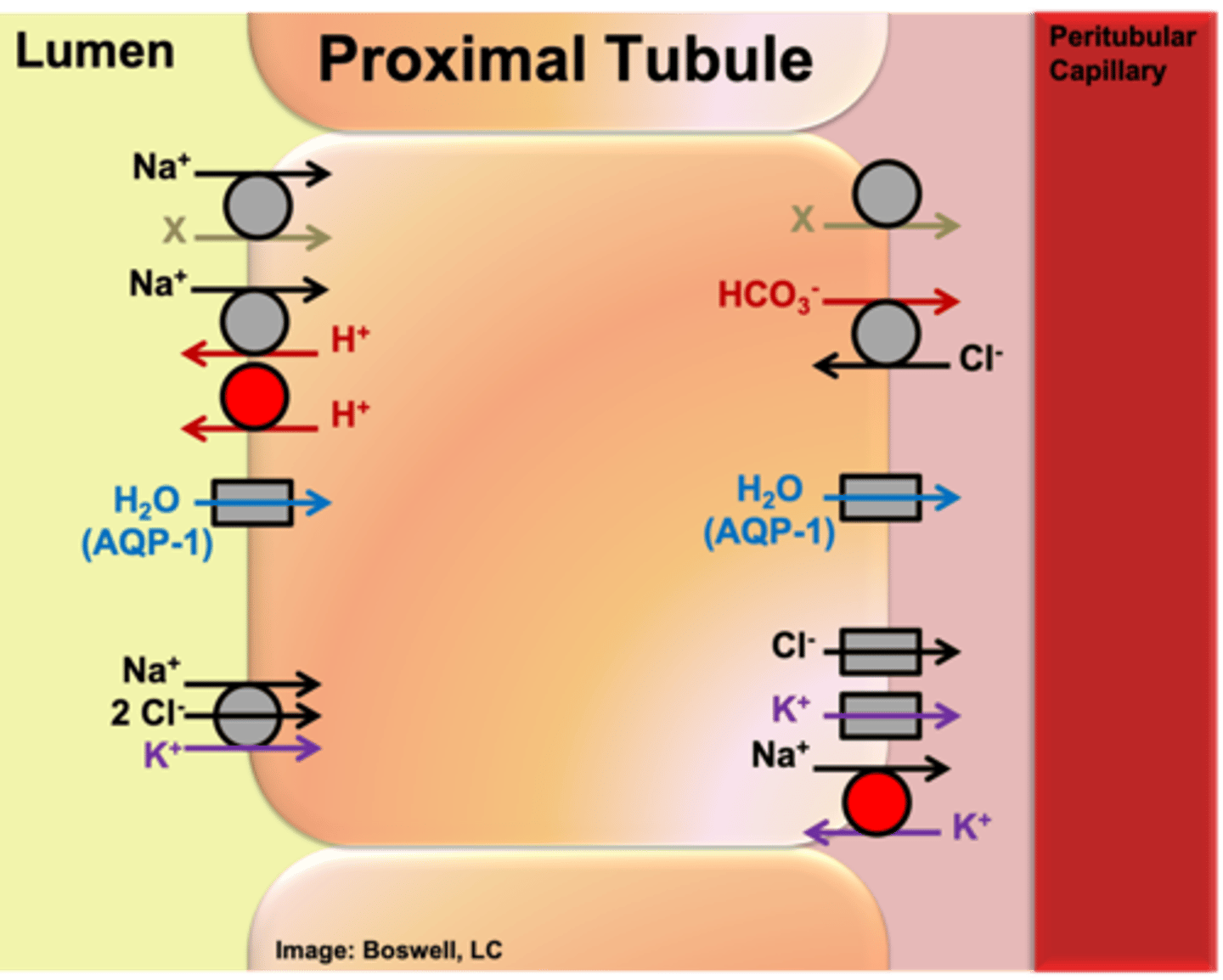
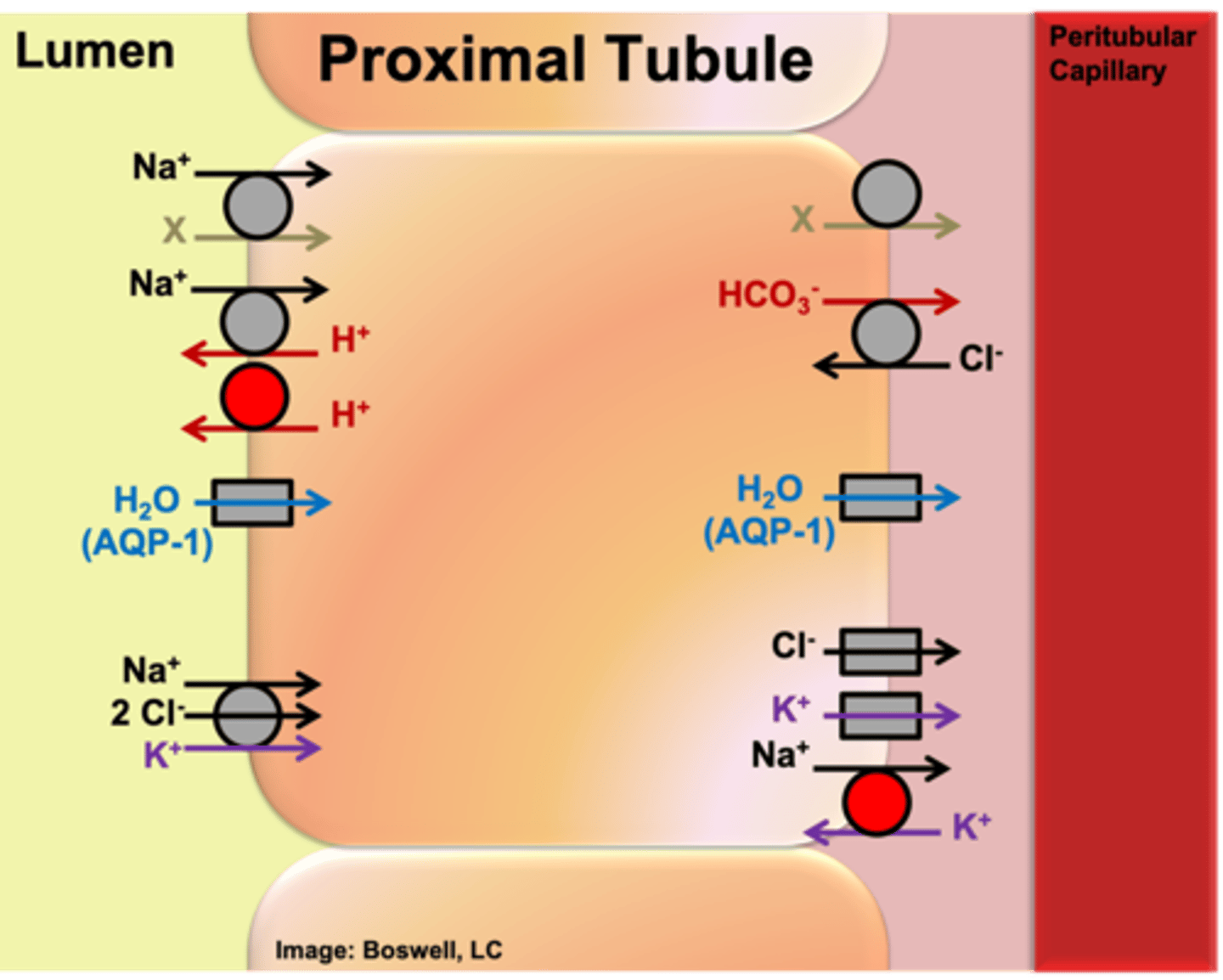
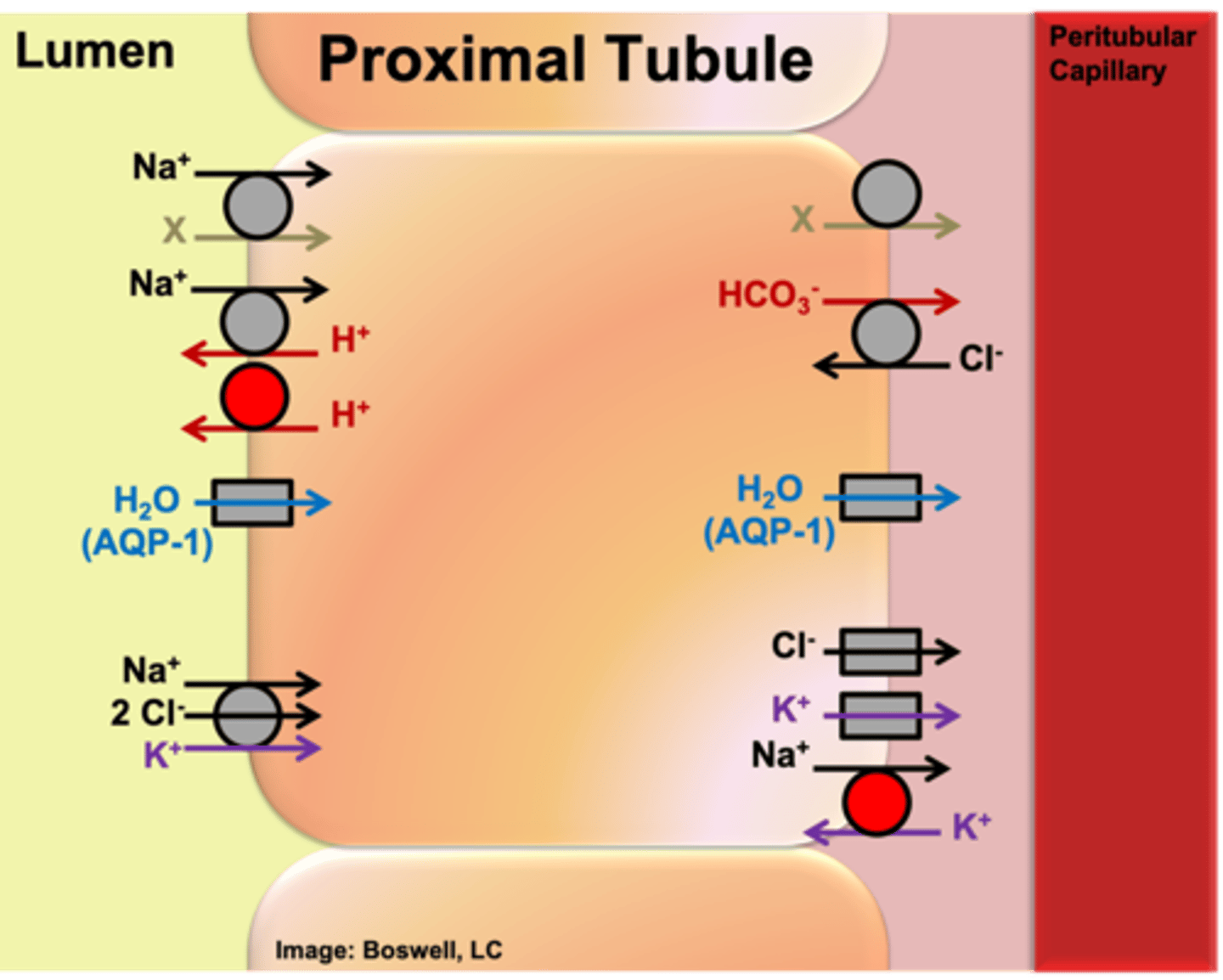
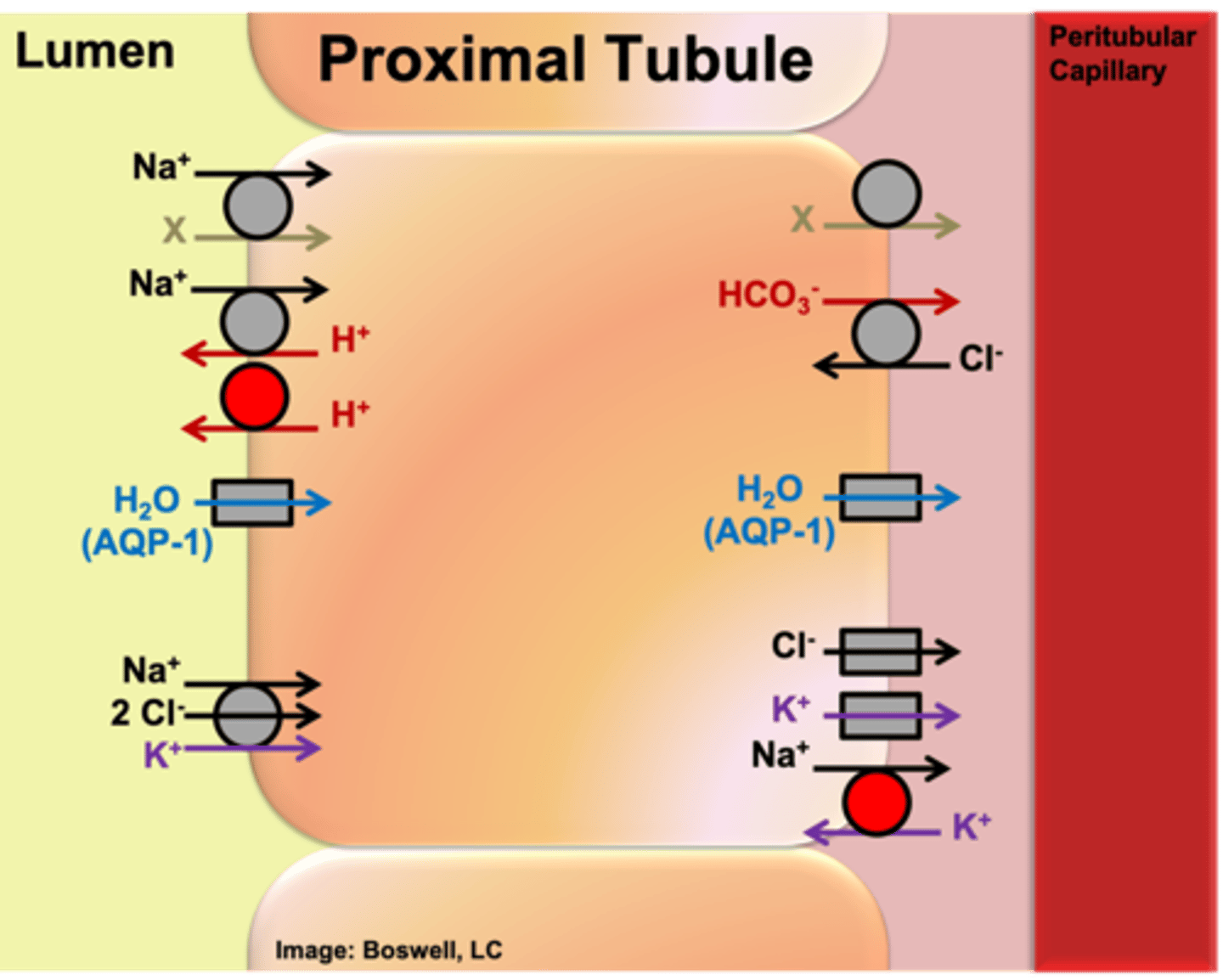
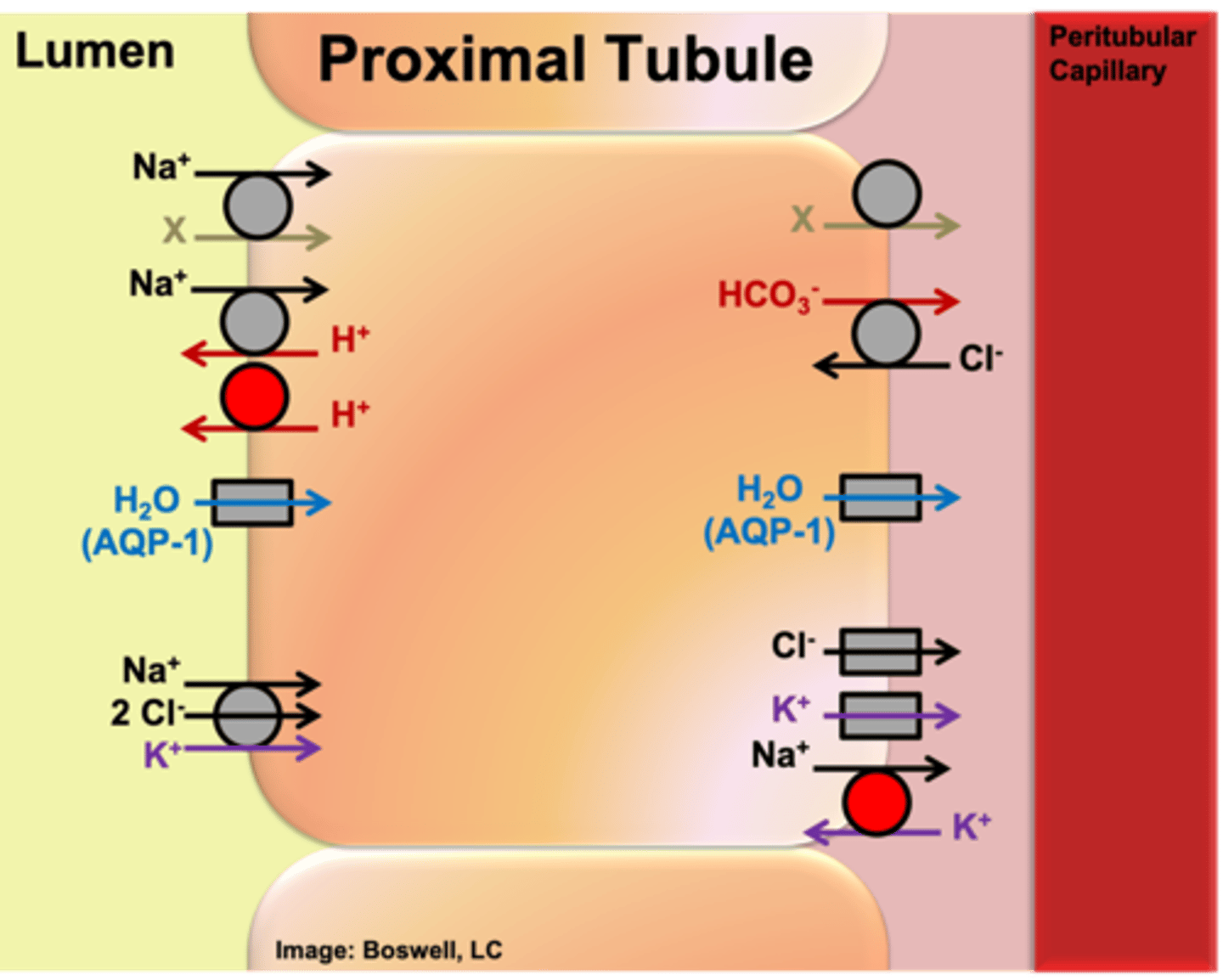
What kind of cells make up the proximal tubule? Why is this significant?
The tube is just made of epithelial cells; reabsorption of materials will occur due to channels and carriers in the plasma membrane of the epithelial cells
The ___ membrane of the epithelial cells of the proximal tubule face the lumen.
Apical
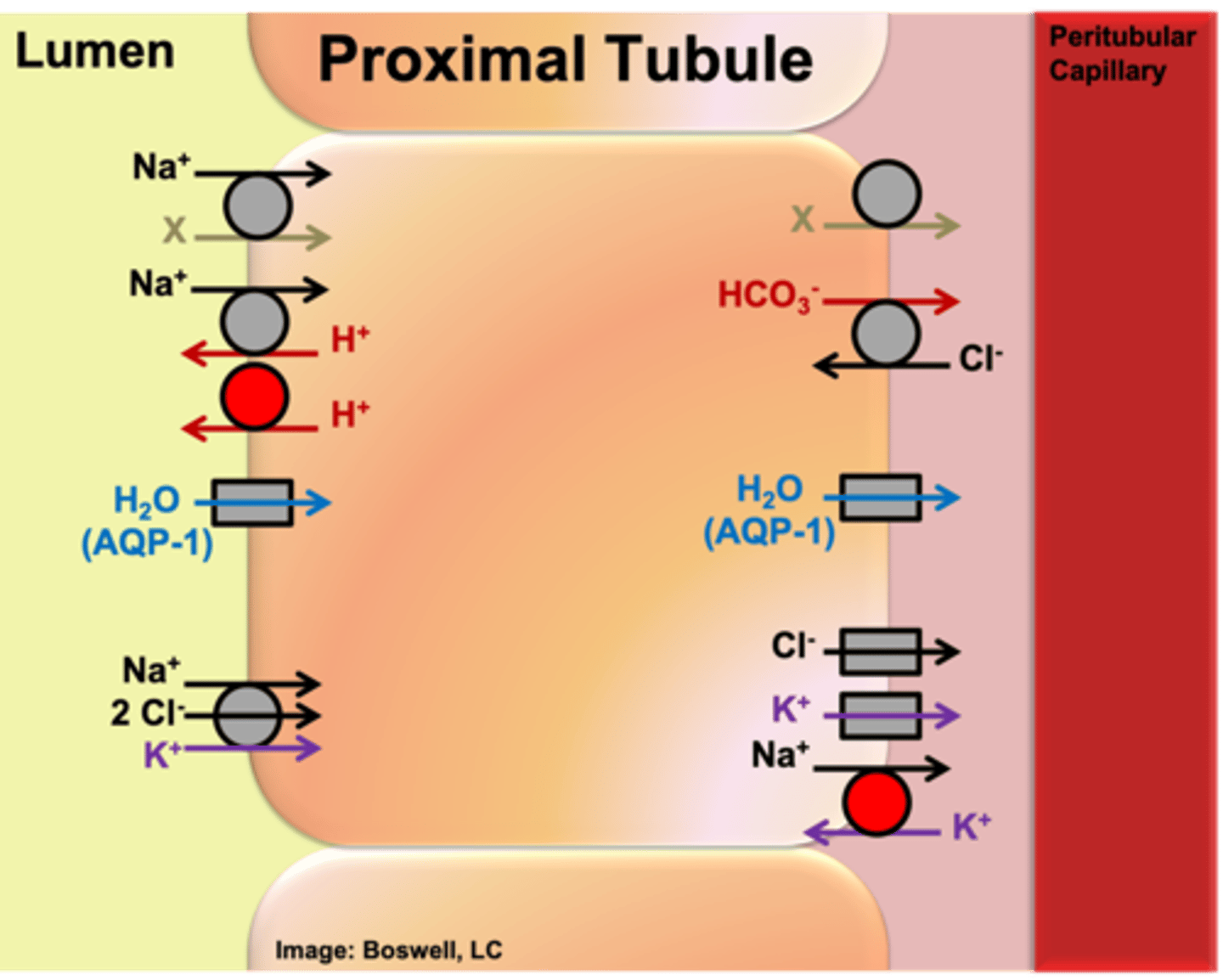
The ___ membrane of the epithelial cells of the proximal tubule face the peritubular capillary.
Basolateral membrane
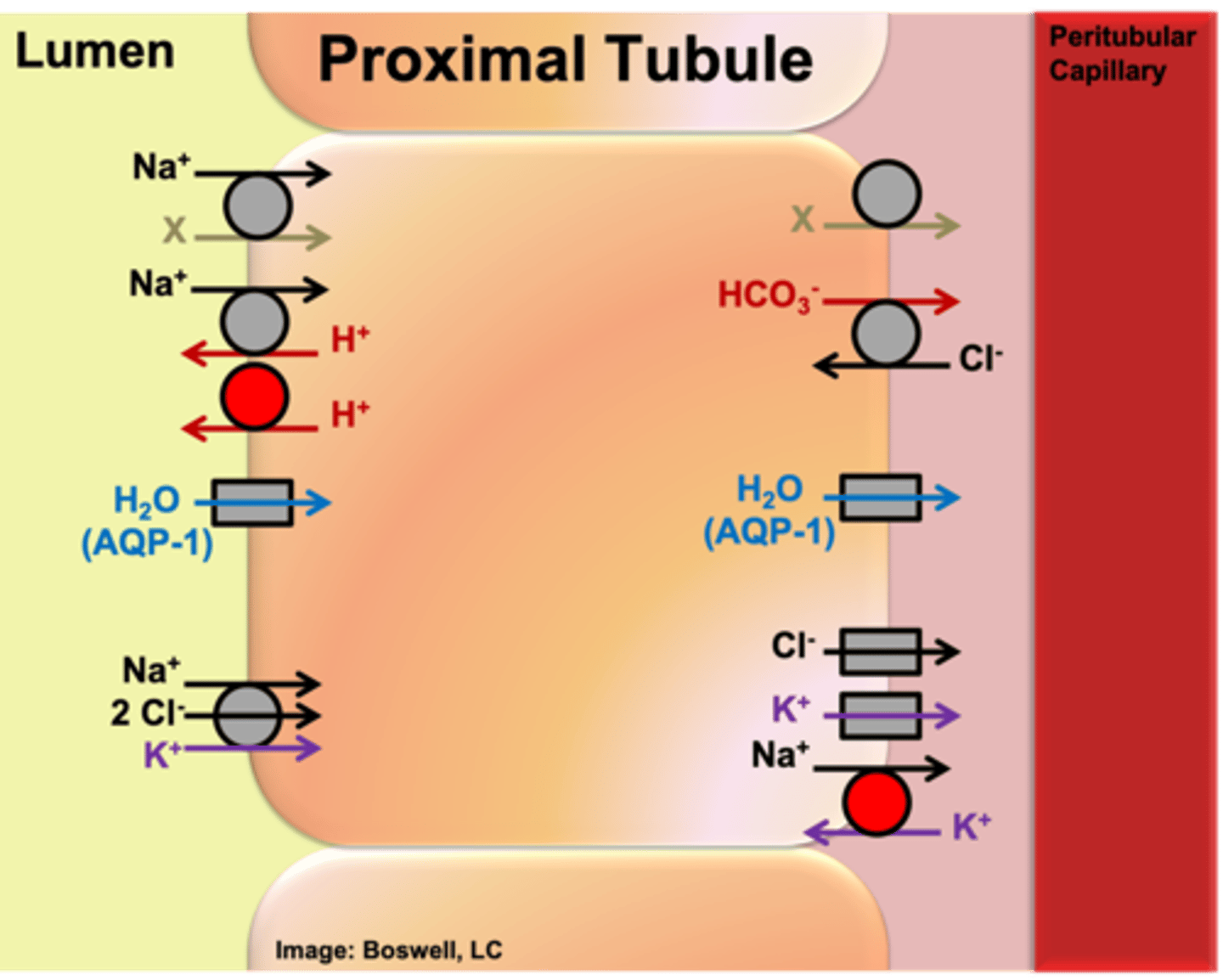
Which carrier (primary active) is ALWAYS present on every cell? On what face of the cell is it present on in epithelial membranes?
basolateral sodium potassium ATPase
When present on epithelial membrane, it will always be basolateral
From an evolutionary perspective, what is true of the value of glucose and amino acids in the ultrafiltrate?
Precious resources from an evolutionary perspective - not beneficial to rid the body of nutrients in the urine
By the time that the ultrafiltrate reaches the end of the proximal tubule, what is true of the reabsorption of glucose and amino acids?
take back all the glucose and amino acids
Which carrier(s) is involved in the transport of glucose across the epithelial cells of the proximal tubule in reabsorption?
- Across apical membrane: SGLT (secondary active transport; sodium moves down its concentration gradient and is used to power the movement of glucose from the filtrate into the epithelial cell)
- Across basolateral membrane: GLUT-2 (facilitated diffusion, which gets glucose back into the interstitial fluid of the plasma)
- Na+/K+ ATPase on basolateral side to establish concentration gradient
On which membrane is SGLT located in epithelial cells (of the proximal tubule specifically)?
apical membrane
On which membrane is GLUT-2 located in epithelial cells (of the proximal tubule specifically)?
basolateral membrane
How are amino acids reabsorbed back into the peritubular capillary in the proximal tubule (which TYPES of carriers are involved -- not specific names)? (Hint: Similar to glucose)
- secondary active transporter (like SGLT) on apical side
- facilitated diffuser (like GLUT-2) on basolateral side
- Na/K ATPase to establish concentration gradient
What are the most predominant ions (electrolytes) that are absorbed in the proximal tubule?
Na+ and Cl- (are the most predominant ions in the ECF)
What amount of sodium and potassium (electrolytes) is absorbed in the proximal tubule?
about 75%
Which carriers are involved in the reabsorption of electrolytes in the proximal tubule (and where are they located)?
- Apical membrane: NKCC (secondary active transporter powered by sodium moving down its concentration gradient; in order for conformational change to occur, Na+, 2Cl- and K+ have to all be bound)
- Basolateral membrane: Na+/K+ ATPase moves Na+ out of the cell (against gradient), K+ leak channel, and Cl- channel (Cl- follows sodium)
What percentage of the total volume of water is reabsorbed by the peritubular capillaries in the proximal tubule?
Reabsorb about 75% of total volume of ultrafiltrate by the time we reach end of proximal tubule
What is the "iso-osmotic" reabsorption of water in the proximal tubule? Explain.
- General fact: there is not net movement of water in an iso-osmotic environment (there must be an energy gradient)
- The osmolarity of the interstitial fluid and the ultrafiltrate are the SAME (appears to be iso-osmotic); water follows the reabsorption of Na+/Cl- (equal amounts are reabsorbed, no change to the osmolarity)
Which channel(s) are involved in the reabsorption of water in the proximal tubule (and where are they located)?
Apical and basolateral membrane: Type 1 Aquaporins
What is ALWAYS true for the permeability of the proximal tubule to water?
- Type 1 aquaporins
- Always expressed by cells that express them
- Located both apical and basolateral (different from other aquaporins)
- Proximal tubule is always fully permeable to water
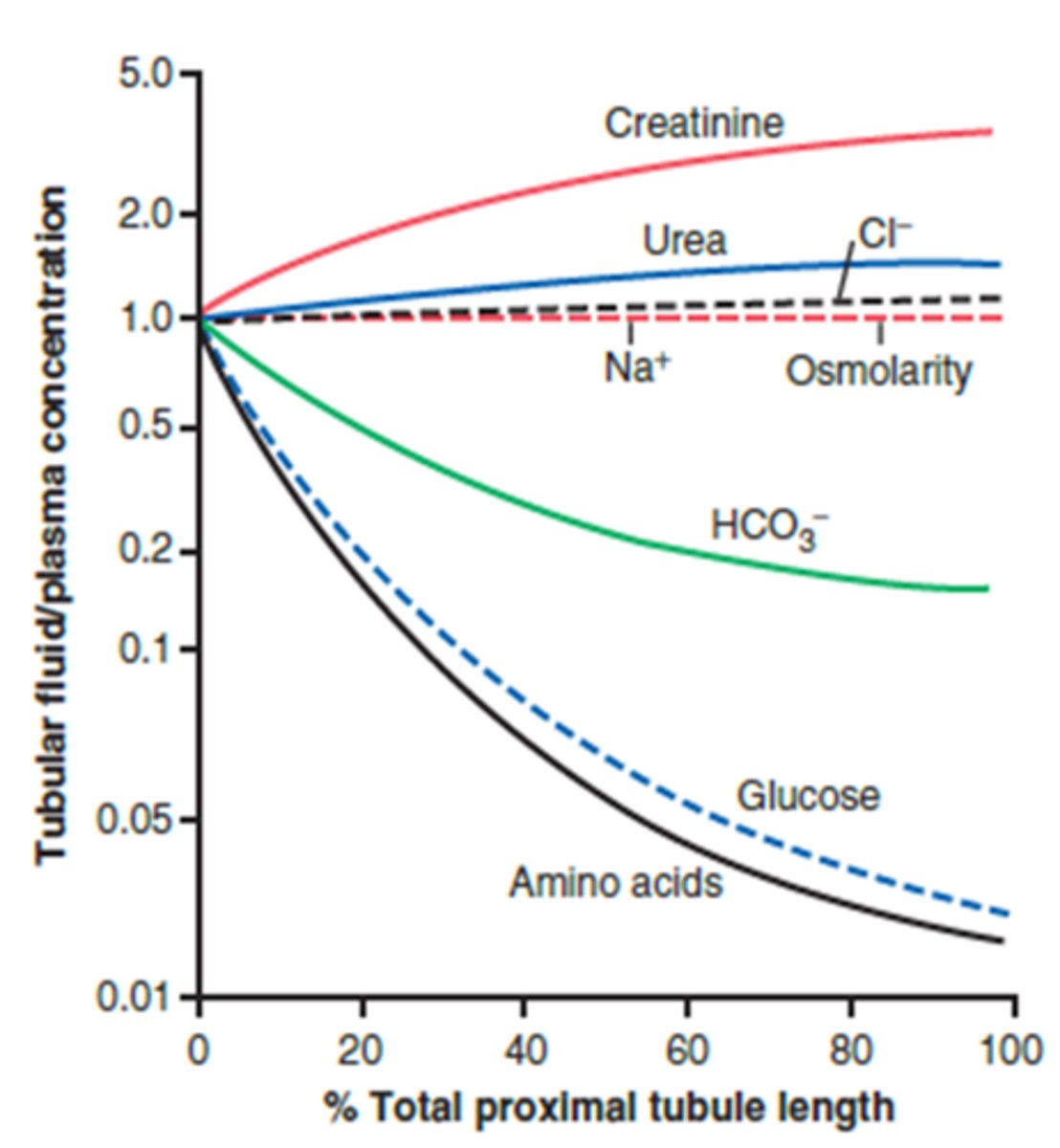
What is the composition of the ultrafiltrate a function of within the proximal tubule?
function of length along the proximal tubule
Upon reaching the distal end of the proximal tubule the ultrafiltrate:
How is it compared to the blood plasma?
iso-osmotic to blood plasma (300 mOsm)
Upon reaching the distal end of the proximal tubule the ultrafiltrate:
What has happened to the total amount of volume?
volume is reduced by about 75%
Upon reaching the distal end of the proximal tubule the ultrafiltrate:
What is true of the concentration of any solute not reabsorbed (ex: creatinine)?
Any solute not reabsorbed is 4X more concentrated
Upon reaching the distal end of the proximal tubule the ultrafiltrate is ___ to the blood plasma with an osmolarity of ___
iso-osmotic; 300 mOsm
Upon reaching the distal end of the proximal tubule the volume of the ultrafiltrate is reduced by about ___%
75%
Upon reaching the distal end of the proximal tubule the any solute not reabsorbed in the ultrafiltrate is ___ times more concentrated
4
The ___ is an avenue to rid the body of products in excess or that are foreign
final urine
In the proximal tubule what is true of the reabsorption of glucose and amino acids?
- Reabsorb all filtered glucose and amino acids (precious nutrients from an evolutionary standpoint - body systems are evolved to keep the precious nutrients)
- Freely filtered - but we reclaim a lot
Describe the "iso-osmotic" reabsorption of water in the proximal tubule.
- Net movement of water is not iso-osmotic (must be some sort of energy gradient to drive the net movement of water passively)
- Since the aquaporins are always present, water is following the active reabsorption of solute (sodium predominantly)
The reabsorption of which ion drives the reabsorption of all other materials in the proximal tubule, including water?
Sodium reabsorption really drives the reabsorption of everything else (water passively follows)
What happens to the osmolarity within the proximal tubule as it moves from 0% total length to 100% total length? What has drastically changed?
- Iso-osmotic reabsorption of water - at the end of the proximal tubule we have the same osmolarity that we had at the beginning (equivalent to the surrounding fluid); still approximately 300 mOsm
- What has changed drastically is the composition of what solutes are making up the number of solute particles (Ex: Start with 100 mL of fluid and 100 mg of solute - if we reabsorb 75% of both, we will have 25 mL of fluid and 25mg of solute; still same osmolarity, just different molecules)
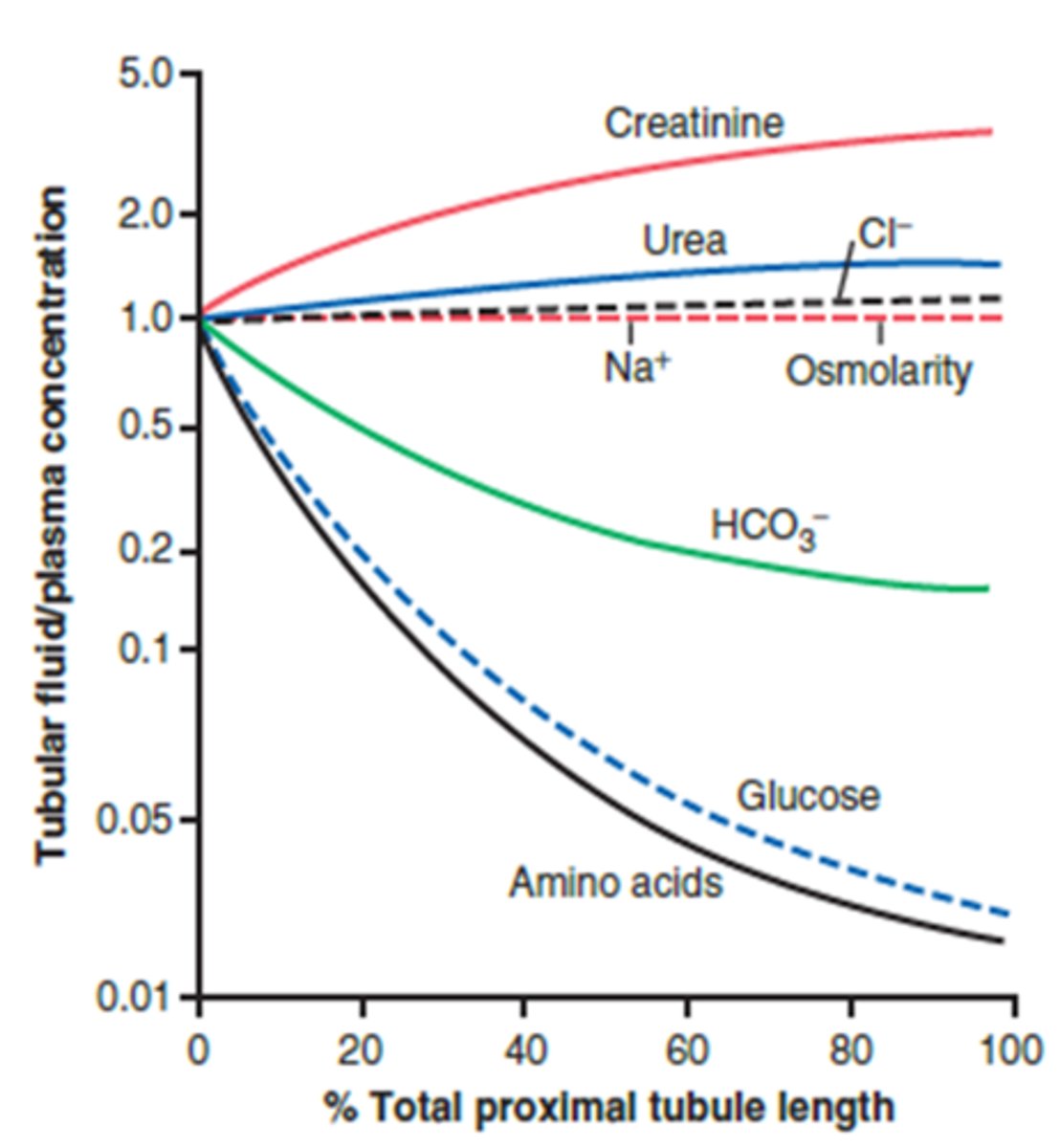
What happens to the total amount of glucose and amino acid within the proximal tubule as it moves from 0% total length to 100% total length?
Total amount present in ultrafiltrate will drop almost to zero from its original value
What happens to the concentration of glucose and amino acid within the proximal tubule as it moves from 0% total length to 100% total length?
- Concentration is much lower - reabsorbing precious nutrients at a higher rate than we are absorbing volume (reabsorbed in excess of water)
example of a dissolvable solute freely filtered that is not reabsorbed by the proximal tubule
creatinine
What happens to the total amount of creatinine within the proximal tubule as it moves from 0% total length to 100% total length? Concentration?
- Total amount stays the same (all of it is still in the ultrafiltrate)
- However, the same total amount is in a less volume of fluid- higher concentration
- Ex: 100 mg of creatinine in 100 mg of water at beginning vs. 100 mg of creatine in 25 mg of water (4x more concentrated)
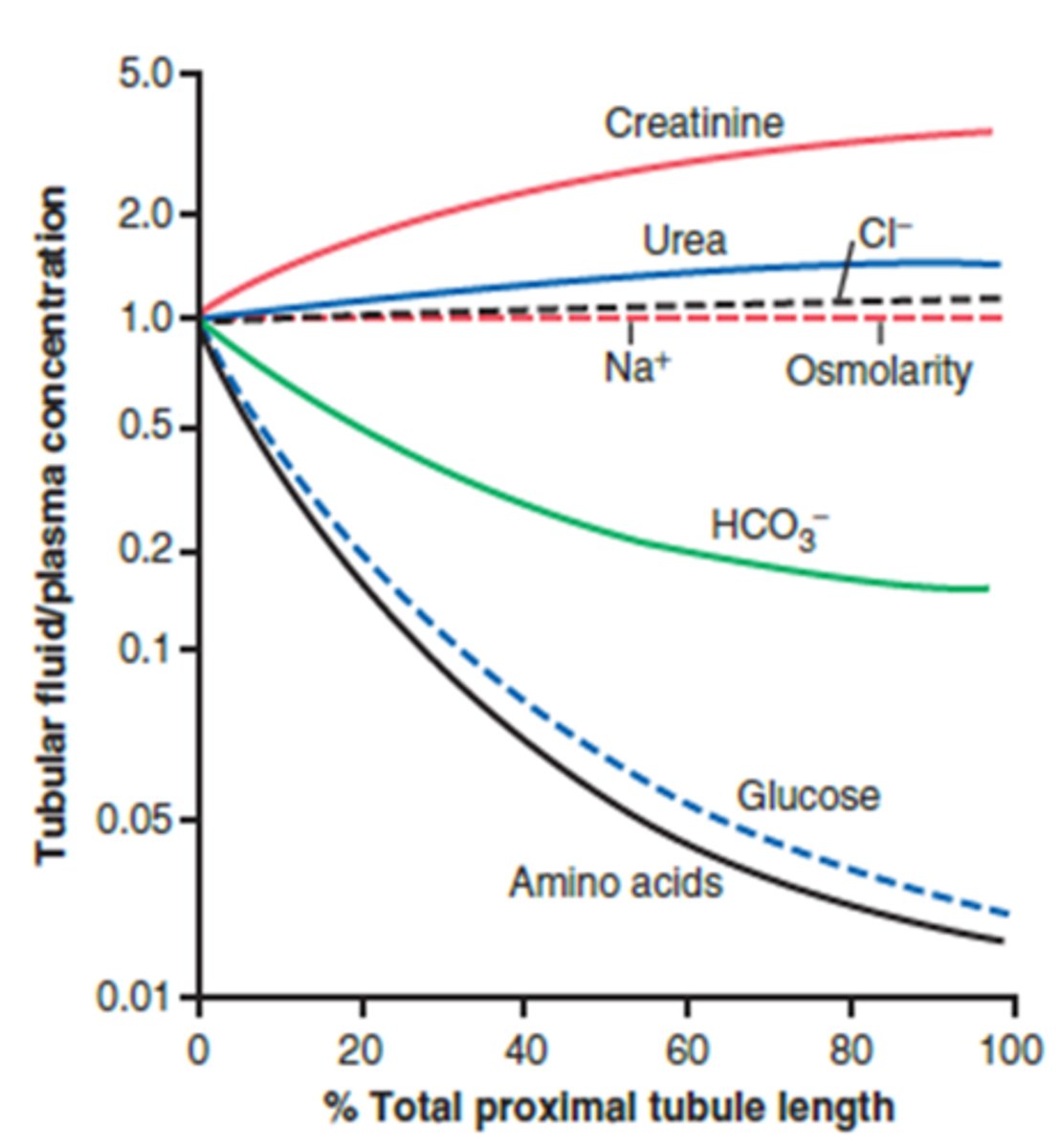
What happens to the total amount of Na+ and Cl- within the proximal tubule as it moves from 0% total length to 100% total length? Concentration?
- Both reabsorbed as the ultrafiltrate goes along the length of the proximal tubule
- Concentration does not change because they are reabsorbed at the same rate as water
- 100 mg NaCl in 100 mL of water; 25 mg NaCl in 25 ml of water
T/F: Bicarbonate is freely filtered during glomerular filtration.
True
What happens to the total amount of bicarbonate within the proximal tubule as it moves from 0% total length to 100% total length? Concentration?
- Reabsorbed as ultrafiltrate flows through (acid base balance)
- Smaller total amount than at start
- Concentration is decreasing - reabsorbed in excess of water volume (but not to the same extent as glucose and amino acids)
The ____ functions as a countercurrent multiplier that creates/maintains a vertical medullary concentration gradient
loop of Henle
The loop of Henle functions as a ___ that creates/maintains a vertical medullary concentration gradient
countercurrent multiplier
The loop of Henle functions as a countercurrent multiplier that creates/maintains a vertical medullary ___
concentration gradient
Which two things are required of a countercurrent multiplier (required in countercurrent multiplication)
Countercurrent multiplication requires energy and asymmetry
How does the length of a countercurrent multiplier relate to the concentration gradient?
The longer the multiplier, the greater the concentration difference from top to bottom
What is the role of the loop of Henle?
functions as a countercurrent multiplier that creates/maintains a vertical medullary concentration gradient
Where does the loop of Henle create a concentration gradient?
the local interstitial fluid of the kidneys
Countercurrent multiplication requires ___ and ___
energy (to make a thermodynamically non-favorable system); asymmetry
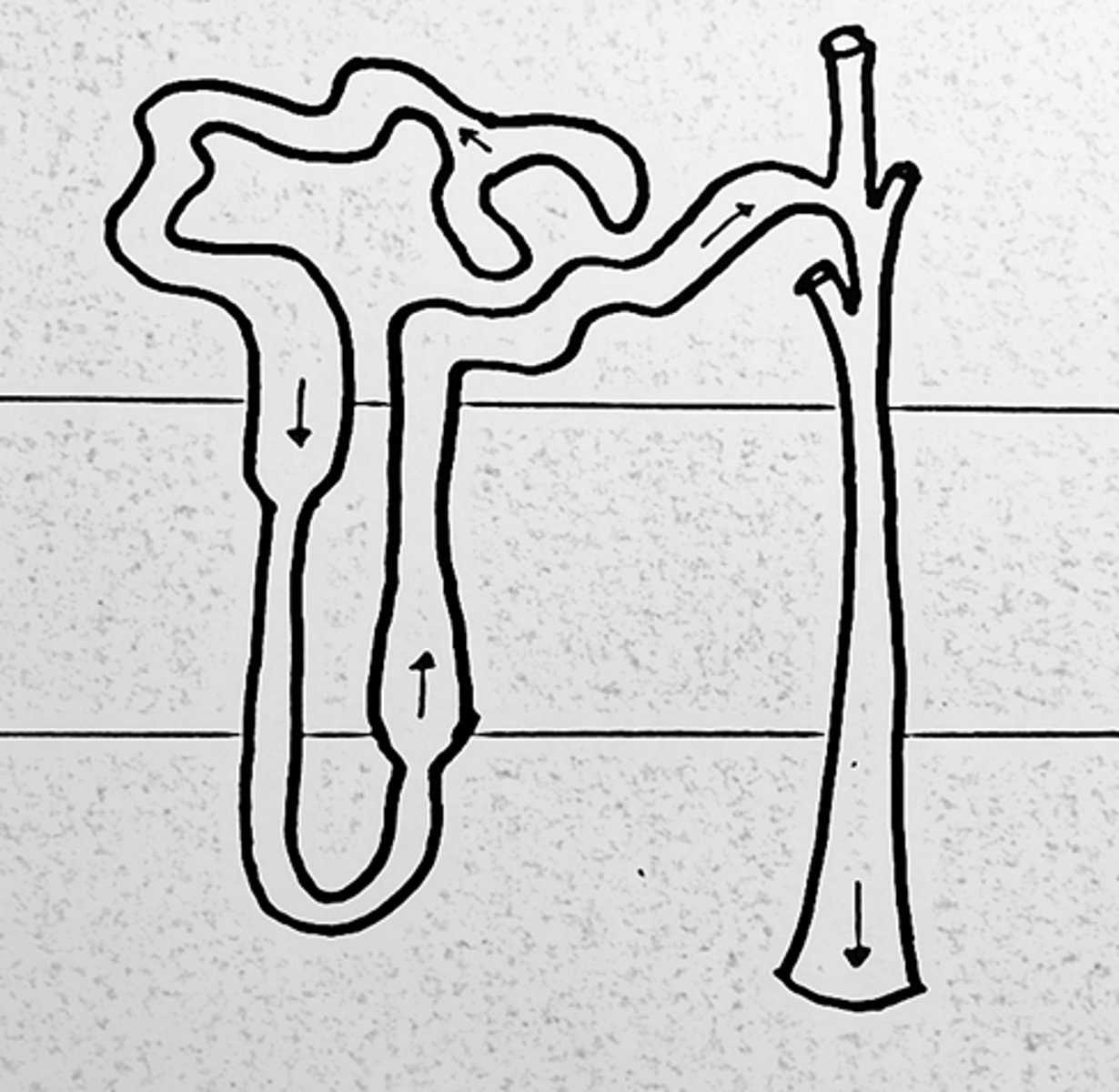
What two portions can the loop of Henle be divided into?
the descending and ascending limb
How does the ultrafiltrate travel through each portion of the loop of Henle?
Ultrafiltrate flows down the descending limb, hairpin turn and then back up ascending limb
The ___ the countercurrent multiplier, the greater the concentration difference from top to bottom
longer
When does the creation of the concentration gradient within the kidneys begin?
Once you are alive and kidneys are functioning, there is always a vertical concentration gradient (depths more concentrated than outer cortex)
What is the maximum concentration gradient of the depths of the Kidneys (inner medulla)?
1200 mOsm
What function is the descending limb of the loop of Henle involved in?
osmotic reabsorption of water
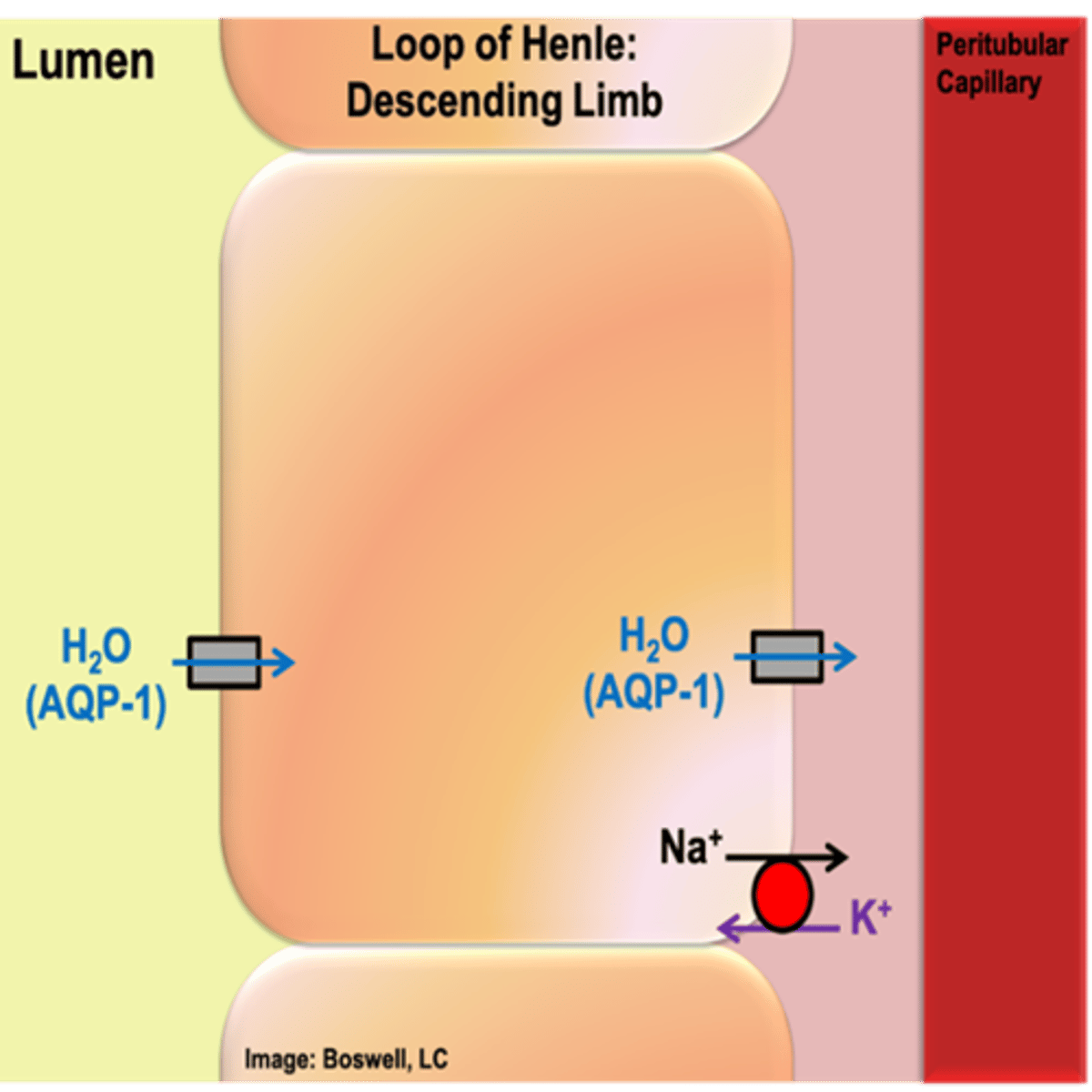
What function is the ascending limb of the loop of Henle involved in?
active reabsorption of sodium chloride
portion of the loop of Henle involved in the osmotic reabsorption of water
descending limb
portion of the loop of Henle involved in the active reabsorption of sodium chloride
ascending limb
At the end of the loop of Henle, the ultrafiltrate is ___-osmotic to the blood plasma and has an osmolarity of ___mOsm
hypo-osmotic (about 100 mOsm)
At the beginning of the descending loop of Henle, what is true of the osmolarity of the ultrafiltrate?
Ultrafiltrate is 300 mOsm just like the surroundings
Which proteins cause the descending loop of Henle to be freely permeable to water?
- Have AQP-1 (like the proximal tubule)
- Both sides (apical and basolateral) – freely permeable to water
(also have Na+/K+ ATPase)
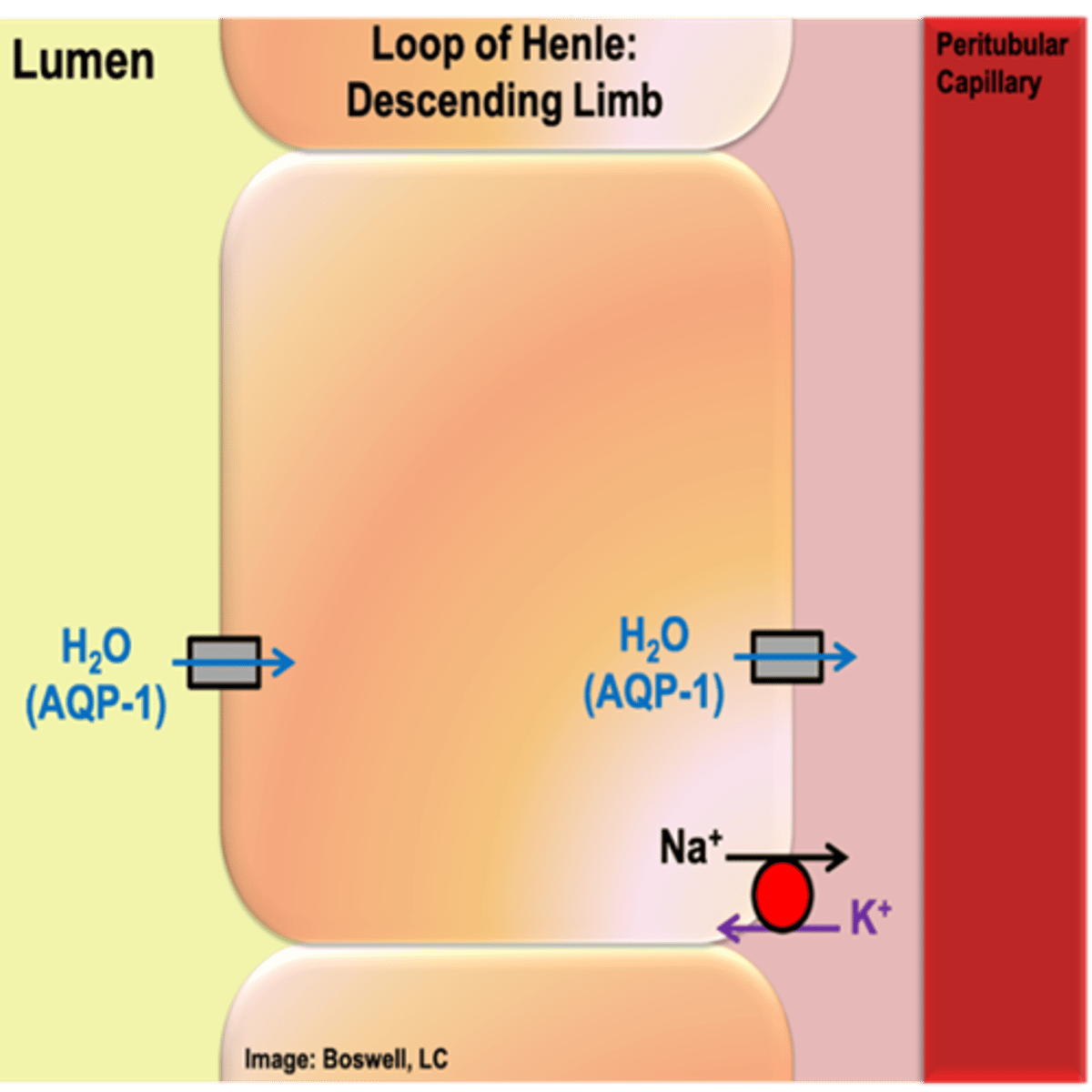
What type of reabsorption occurs in the descending loop of Henle? Explain how this process occurs.
- osmotic reabsorption of water (AQP-1 on apical and basolateral side)
- As ultrafiltrate flows down descending limb into innermedulla, equilibrates with its surroundings
- Water is continued to be reabsorbed until the equilibrium is reached
By the time the ultrafiltrate reaches the bottom of the loop of Henle, what is true of its concentration?
1200 mOsm (reabsorption of water --> same number of solutes, but smaller volume of water)
T/F: The ascending limb of the loop of Henle is permeable to water
False; NOT permeable to water (no AQP-1)
What type of reabsorption occurs in the ascending limb of the loop of Henle? How does this occur (what proteins are present to allow this)?
- The cells of the ascending limb do not have aquaporins (water does not diffuse in or out of these cells at a physiologically relevant rate)
- actively reabsorbs sodium and chloride (most abundant, bulk of the salt that is reabsorbed); some potassium is reabsorbed
- Similar carriers to proximal tubule: NKCC transporter – secondary active transporter utilizes Na+ (moving down its gradient from the lumen into the cell), Na+/K+ ATPase establishes low Na+ in cell on basolateral (and moves Na+ rest of way), channel for Cl- (follow Na+) and K+ leak channel on basolateral (move down concentration gradient)
- K+ leak channel on apical membrane (allow K+ to exit into lumen for NKCC transporter use)
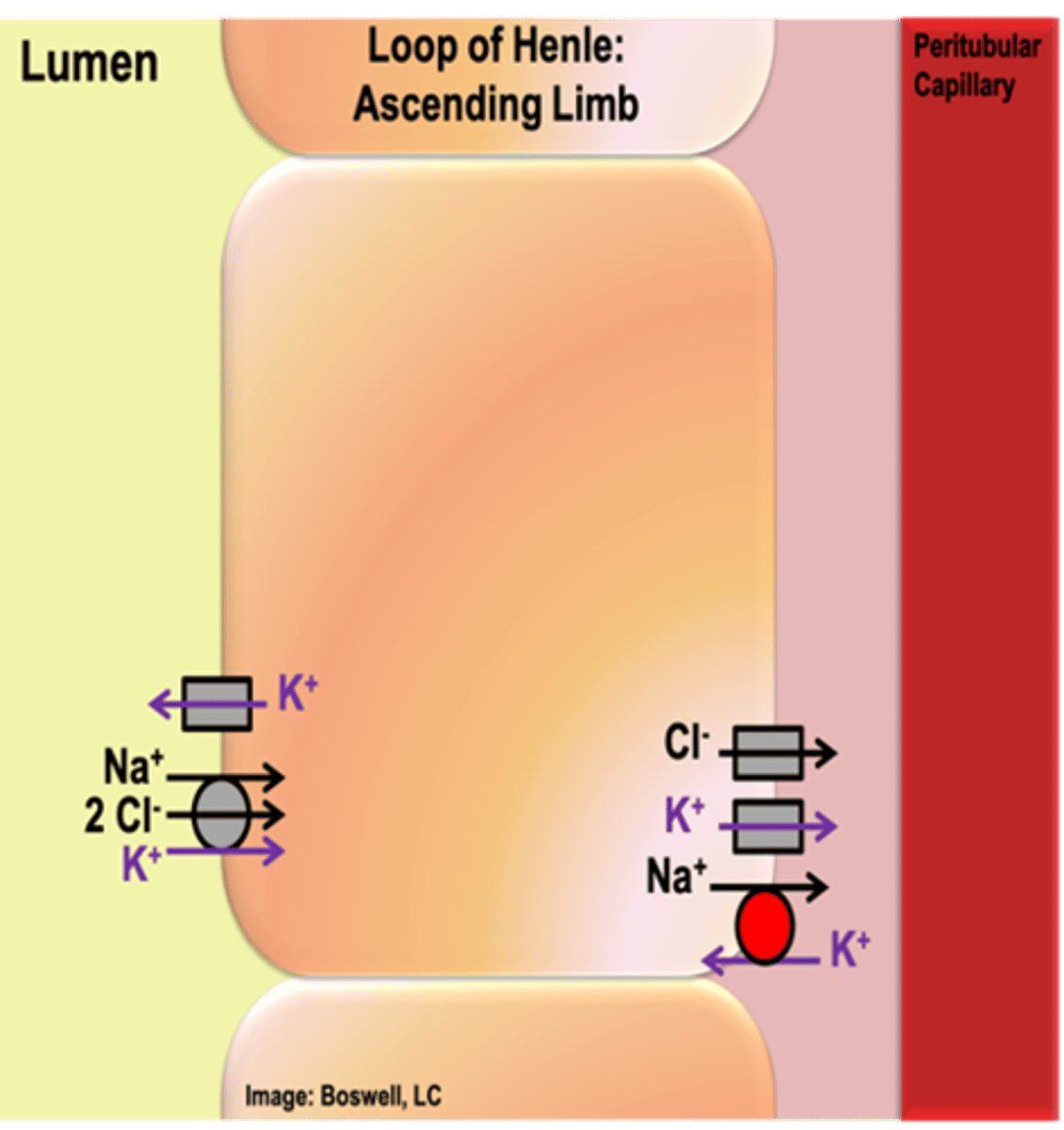
How does the location of K+ leak channels in the loop of Henle differ from the proximal tubules?
- There is also a potassium leak channel on the apical membrane
- if K+ is fully brought out of the lumen the NKCC will not work (conformational changes are contingent on the presence of all ions)
By the time the ultrafiltrate reaches the end of the loop of Henle, it will be ___ to normal body fluids
hypo-osmotic (100mOsm)
By the time the ultrafiltrate reaches the bottom of the loop of Henle (hairpin turn), it will be ___ to normal body fluids
hyperosmotic (1200 mOsm)
What structure is often called the "diluting portion" of the nephron? Why?
- loop of Henle
- At the end of the loop of Henle, if you did nothing else to the ultrafiltrate it would be hypo-osmotic to body fluids (can rid the body of excess water)
T/F: You can only produce urine that is hyperosmotic to plasma.
False; You are able to produce urine that is hypo-osmotic and/or hyperosmotic (as concentrated as 1200 mOsm); function of the late distal tubule/collecting duct
In the distal portion of the collecting duct, what solute/chemical is it permeable to? Why is this important?
- urea (waste from break down of amino acids)
- By the time we get to the final urine, urea is much more concentrated in the final urine than it is in the ECF body fluids; If you provided an avenue, it will go down its concentration gradient into its surroundings
___ are specialized capillaries that function as countercurrent exchangers
vasa recta