Neurological Disorders
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
Stroke
Cerebrovascular accident (CVA)
• A type of stroke
• The term was created to have a similar connotation to a heart attack
• Time is pertinent
• Must act quickly to preserve what we can, similar to a heart attack
• If cell death is severe enough → death
Result of impaired blood flow to the brain → brain cell death
Blood on neurons → neuron death
Death of brain cells caused by
• Lack of blood supply (ischemic)
• Bleeding in the brain (hemorrhagic)
Blood-brain barrier
Prevents blood from reaching neurons, which would result in brain tissue damage
Hemiparesis
Muscle weakness or paralysis on one side of the body
Face, upper/lower body, or combination
Aphasia
Difficulty communicating
○ Difficulty understanding
○ Or both
Brain requires 20% of CO
If this is altered → cell death occurs within 5 minutes
Autoregulation
The brain regulates blood flow via this process, allowing significant changes in blood pressure, as it can affect blood flow to the brain itself.
Factors impacting blood flow to brain
Cardiac output
Blood viscosity
Blood pressure
Collateral circulation
Done via Circle of Willis (a structure that sits at the base of the brain), which allows for blood to find a new path despite the slow narrowing of arteries.
Nonmodifiable risk factors
• Age
• Gender
• Ethnicity
• Family history
• Transient ischemic attack (TIA)
Modifiable risk factors
• Hypertension
• Heart disease
• Diabetes
• Smoking
• Obesity
• Sleep apnea
• Metabolic syndrome
• Sedentary lifestyle
• Drugs
• Alcohol
Age (stroke risk)
Risk of stroke doubles with each decade after age 55
Gender (stroke risk)
Women have a higher incidence of stroke and a higher death rate
Transient ischemic attack (stroke risk)
Lack of blood supply to an area of the brain, but not significant enough to cause an infarction
Many people who have a TIA will have a stroke within the same year
Hypertension (stroke risk)
Listed number one stroke risk and is often the target of stroke risk reduction due to how strongly it is connected to stroke (ischemic and hemorrhagic)
Heart disease (stroke risk)
Afib is associated with the development of blood clots due to blood pooling in the atria, which can lodge in the brain
CAD: if you have plaque in the heart, it is likely in the brain (it is not cardioselective)
Diabetes (stroke risk)
Damaging to the vascular system, which increases the risk of clots from platelets attempting to repair the damage.
Smoking (stroke risk)
Increases the risk of hemorrhagic stroke
The client must quit smoking
Can take up to 10 years to remove the risk of stroke due to smoking
Obesity (stroke risk)
Linked to other risk factors on the list: high blood pressure, hyperlipidemia, and diabetes
Sleep apnea (stroke risk)
Increases the risk of stroke and heart disease
During periods of apnea, which causes significant stress
Blood pressure goal for stroke risk reduction
Less than 120 systolic and less than 80 diastolic
TIA characteristics
• Transient episode of cerebrovascular insufficiency
• One-third of TIA patients will have a stroke within a year
• Lasts less than 20 minutes
• No radiographic evidence of ischemia
TIA symptoms
• Symptoms are similar to a stroke
• Neuro exam may be normal between attacks
TIA duration
Symptoms typically shorter than 20 min
If longer than 20 min → treat as a stroke
TIA education
Educate them on how to prevent having a future stroke and permanent disability
We don’t want them to think it was a false alarm or no need for concern
Strong chance they will have an actual stroke that same year
Changing risk factors will be so pertinent in preventing this
Modifying what we can
Ischemic stroke
• Approximately 87% of strokes are ischemic
• Can occur in large or small vessels
• Something is blocking blood flow to an area of the brain, a physical obstruction or blockage
Two kinds of ischemic stroke
Thrombotic
Embolic
Thrombotic stroke
Blockage forms in the vessel
More common of the two types
Damage to a blood vessel → vessel injury → formation of a clot
Atherosclerosis is accelerated by diabetes and hypertension (which is why they are both risk factors for thrombotic stroke)
Can present as a TIA for some patients due to reduced flow, but not a total occlusion. Brief symptoms from lack of oxygen, but flow is still present
If plaque ruptures → platelets rush to the area to correct damage → complete occlusion of the vessel → infarct in brain tissue → stroke
Embolic stroke
Blockage comes from somewhere else
The second most common type of stroke
A clot or embolism breaks off from somewhere else in the body and lodges into brain
Travels from elsewhere
Commonly traveled from the heart
Afib patients carry a high risk of stroke, which is why they are placed on anticoagulants to mitigate that risk (Elliquis, warfarin
Artificial valves, endocarditis (damage to vessels)
Air and fat emboli can cause as well
Hemorrhagic stroke
Bleeding into the brain tissue
Blood in contact with neurons → extremely damaging to neurons
Ruptured vessel or aneurysm (weakening of vessel + outpouching of blood → risk for rupture)
Hypertension increases this risk
When blood comes in contact with brain tissue → neurons are destroyed
If the vessel ruptures → tissue distal to the vessel is not receiving any blood flow or oxygen → area of infarct
Two kinds of hemorrohagic stroke
Intracerebral
Subarachnoid
Intracerebral hemorrhage
Fairly deep in brain tissue
Common cause: ruptured vessel, specficically basal ganglia
Could be bleeding in just the brain itself or could be occurring in ventricles depending on what else is involved
Prognosis is very poor
More than half of patients die within 48 hours of injury (minutes to hours)
Usually associated with activity
Risk factors: hypertension (main), anticoagulants, brain tumors, trauma
Subarachnoid hemorrhage
Occurs between the arachnoid (sub=below arachnoid) and pia mater layers
Pia layer is very delicate and sits directly on brain
More superficial in comparison to intracerebral
The subarachnoid layer comprised of arteries and CSF
Cause is usually ruptured aneurysm
Common place for aneurysms to occur is bifurcations aka Circle of Willis (place for backup route)
Because it’s a circle with several roads, lots of bifurcations → more aneurysm risk
We see more aneurysms here
Silent killer → not any symptoms assosciated
Patients with this bleed will most likely die, with some instantly
Other types of hemorrhages
Not in textbook but still slightly relevant
Epidural and subdural hematoma
Epidural and subdural hematoma
Dural layer, more superficial
Subdural is typically a venous bleed → slower
Fall or motor vehicle accient
May not have initial symptoms
Older adult patients may have frequent falls and frequent subdural hematomas without even knowing due to natural atrophy of aging
Epidural are most often arteriole in natural
Due to an injury in the front of the back of the head (fall, motor vehicle accident, trauma)
More severe symptoms due to arteriole in nature, rapid bleed
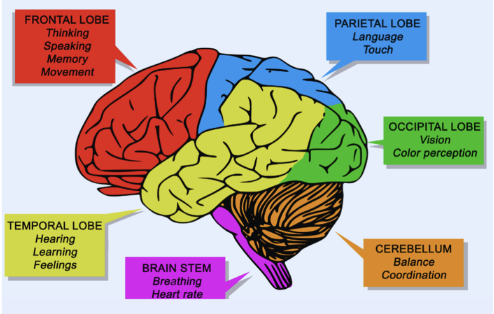
Stroke clinical manifestations
Depends on where in the brain the infarct occurs.
Not a notable difference in ischemic and hemorrhagic stroke
Symptoms will present contralateral to the side of the brain that is impacted
Right will affect left and vice versa
The lobe of the brain that is impacted will influence clinical manifestations
Strong chance that multiple lobes are impaired, depending on vessel location and what is fed or perfused by that vessel
Injury to the brainstem, the lowest part of the brain (breathing, vital signs), is not compatible with life and will typically result in brain death
Stroke & motor fxn impairment
Difficulty swallowing, decreased swallow reflex, hemiplegia
Stroke & communication impairment
Aphasia
Receptive aphasia: can’t understand or comprehend
Expressive aphasia: can’t produce words to speak language they’ve always known
Global aphasia: both receptive and expressive
Common in temporal lobe injuries → difficulty understanding
Common in parietal lobe injuries → difficulty speaking, MCA damage, posterior cerebral artery damage
“Trapped in your own brain.”
Stroke & changes in affect
Physical inability to manipulate facial expressions
Don’t process emotions the same
Feelings of hopelessness and depression due to the inability to perform ADLs
Not able to communicate
Impulsive and restless → frontal lobe damage (personality and behaviors)
Stroke education acronym
BE FAST
BE FAST → Balance
Sudden difficulty with balance
Walking, the gait looks strange
BE FAST → Eyes
Sudden vision problems in one or both eyes
BE FAST → Face
Facial droop/uneven smile
BE FAST → Arm
Arm weakness/numbness
Check for arm drift (motor)
Hold up both their arms parallel to the ground
Ideally tested with eyes closed
Progressive lowering of the arm if the eyes are closed
BE FAST → Speech
Slurred speech, difficulty speaking or understanding
Dysphasia, dysarthria (slurred), or aphasia
Tell the patient to say “You can’t teach an old dog new tricks.”
BE FAST → Time
Time is brain, time is tissue, the faster we address the infarct → better prognosis
Call 911
Call the emergency response team
Rapid response
Code white
Stroke diagnostics
Onset of symptoms
Blood sugar level
CT head/brain w/o contrast
MRI
CT angiogram (CTA)
CT perfusion (CTP)
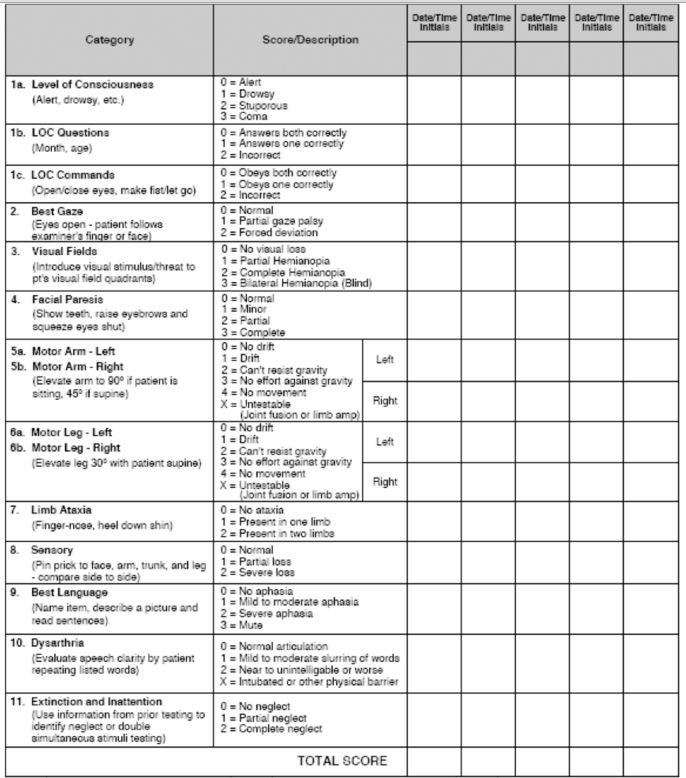
Stroke diagnostic → onset of symptoms
NIH stroke scale
Can impact treatment, especially if ischemic
More time in the hospital → clinicians have a better idea when symptoms began
Ischemic stroke can be treated if the onset is 4 ½ hours or less in the hospital
Pre-hospital will be 3 ½ hours or less
The timing has to do with the preservation of brain tissue over the associated risk of treatment (ex. bleeding)
The symptoms can quickly diagnose an ischemic stroke
Stroke diagnostic → blood sugar level
Low blood sugar can mimic a stroke!
Hypoglycemia stroke-like symptoms: weakness, confusion, speech changes
Doing a quick blood sugar check can prevent unnecessary stroke testing
Stroke diagnostic → CT head/brain w/o contrast
Standard
Can be done quickly without needing to know hx
Won’t be able to see an acute ischemic stroke, but will be able to see a brain bleed
Rules out hemorrhagic stroke or not, which determines treatment steps
Stroke diagnostic → MRI
Requires a screening form
Higher risk test
Contrast dye on the kidneys is contraindicated in low GFR or kidney impairment
If we don’t know this information, time is tissue → CT head is faster
Does give better visualization of vessels
MRI may be done for admitted patients with a known history
Stroke diagnostic → CT angiogram (CTA), CT perfusion (CTP)
Allows for looking at the impacted vessel, the size of the stroke, and where in the brain it is impacted to better tailor treatment
Stroke reoccurence
If a patient has had a stroke and has not modified any of the risk factors → still at risk for developing another stroke!!
Prevention of future strokes is pertinent
Reducing BP, associated cardiovascular risks, fat intake, and cessation of smoking (takes 10 years)
Stroke & nursing care/management
Medications
Antiplatelet
Anticoagulant
Antihypertensives
Rehabilitation care
Musculoskeletal function
Skin protective measures
Dysphagia precautions
Assistive feeding devices
Fall precautions
communication
Stroke & antiplatelets
Plavix (clopidogrel), Aspirin 81 mg
Prevents clots caused by platelets
Stroke & anticoagulants
Elliquis, Warfarin (Coumadin), Pradaxa
Important for patients for afib or artificial valves
Stroke & antihypertensives
Key!
Hypertension is strongly linked to both ischemic and hemorrhagic stroke
Type depends on patient response
May require more than one
120/80 or less
Stroke & statins
Atorvastatin (Lipitor)
Lower cholesterol reduces the incidence of atherosclerosis buildup
Smooths out existing plaque formation to be less “sticky” to platelets
Less likely to form clots
Stroke & rehabilitation care
Musculoskeletal function
Skin protective measures
Dysphagia precautions
Assistive feeding devices
Fall precautions
communication
Stroke & musculoskeletal function rehab
ROM, passive, active
Focus on preserving function
Affected limb → elevate to reduce edema
Focus on reducing the injury of the affected limb; don’t pull on the arm because they can’t feel it
Prevent foot drop → encourage them to wear their own shoes
Hand cones to prevent contractions
Transfer to chair; slide board
Stroke & skin protective measures
Special mattresses, cushions for wheelchairs, keeping the skin clean, applying lotion to prevent skin dryness, and promoting ambulation/positioning
Stroke & dysphagia precautions
Sit them high while eating at 45-90 degrees
Thickened liquids
Speech therapy
Mouth care → stimulate awareness and create moisture
Stroke & assistive feeding devices
Promotes nutrition and ADLs
The more the patient can do for themselves, the better
Non-slip pads for dishes, rocker knife
Stroke & fall precautions
You know this.
Stroke & therapeutic communication
Allow the patient to feel like a person
Talk to them even if they can’t talk back
Assume they know what you are saying
Be patient and give them time
Communication boards
Spinal cord injury
Damage to the spinal cord
Most common causes of spinal cord injury
Falls
Motor vehicle accidents (most common)
Violence
Sports injuries (least common)
Types of spinal cord injruy
Primary injury
Secondary injury
Primary injury
Direct trauma to the spinal cord itself
Stabbed, violence, compressed
Secondary injury
Symptoms that following initial injury
Swelling → tissue death
When something swells, it pushes up against everything around it, and we don’t have a lot of extra space → surrounding damage
Classifications of spinal cord injury
Mechanism
Level
Degree
Mechanism of spinal cord injury
Look at the position the patient was in when the injury occurred
How was the spine manipulated?
Flexion? Hyperextension?
What were they doing?
In a car? On a horse?
Level of spinal cord injury
Where in the spine did the injury occur?
Higher injury → more severe deficits
Degree of spinal cord injury
Complete or incomplete
Complete → total loss of function below the level of injury, complete thickness
Partial → some portion of the spine is intact, some function below injury
Spinal cord injury clinical manifestations
Higher levels of injury, C3 or higher → inability to manage breathing or airway → requiring ventilators for life-sustaining treatment
Cervical injuries may prevent the patient from being able to clear secretions and protect the airway → oxygenation, or even ventilation
Injury T6 or higher → sympathetic nervous system dysfunction (which increases HR and BP) → these patients can’t do that now → bradycardia, hypotension
Dermatones
The body is innervated via dermatomes
Depending on where the injury occured → dermatones at and below the level of injury are anticipated to be affected
Spinal cord injury diagnostic
CT Scan
Assesses the degree and level of injury to anticipate effects on the patient, however…
Spinal and neuro injuries are a waiting game to see what is affected.
Spinal cord injury nursing management
Prevention – education
ABC’s
Spinal immobilizer
Bladder and bowel management
Inpatient rehabilitation
Spinal cord injury & prevention
Helmets, seatbelts
Spinal cord injury & ABCs
Med-surg care will typically be provided to patients with lower-level spinal cord injuries because their airway is still intact
Spinal cord injury & spinal mobilizer
Until we see healing
Before, during, after
Brace, wedges, collars
Spinal cord injury & bladder/bowel management
Bladder training: lost sensation of having a full bladder → have patient go to bathroom at set intervals
Try to avoid an indwelling Foley
Straight catheterizations rather than indwelling
Likely incontinent and requires perineal care
Spinal cord injury & inpatient rehab
Team approach: OT, PT, speech therapy, nurse, physicians
Some hospitals have on-site facilities, and patients will go to these facilities
Restoring function and independence.
Physical therapy is typically 2-4 hours in length, depending on what the patient can tolerate