BIOL Lecture 15 - The Cardiac Cycle
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
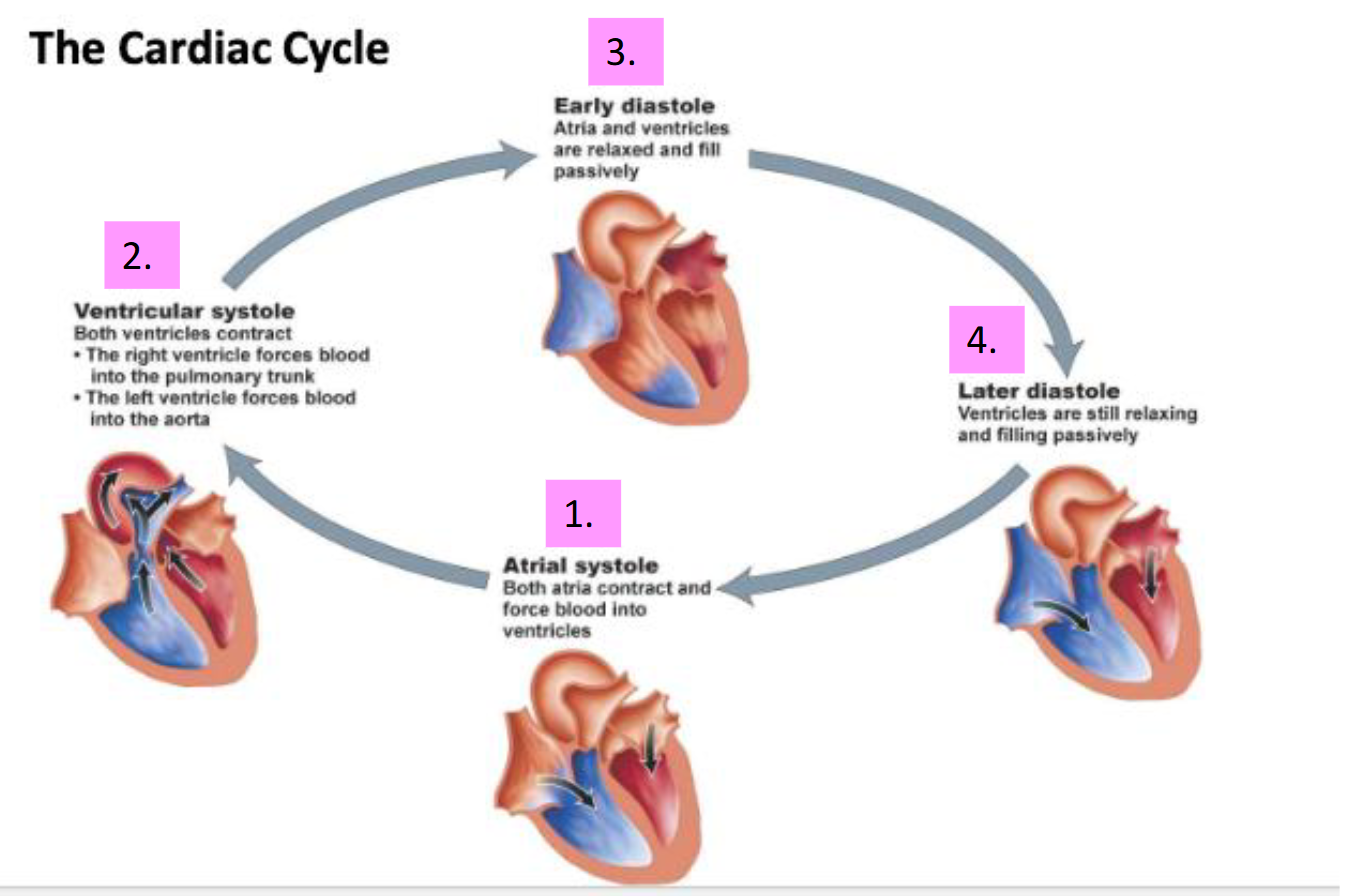
What are the main phases of the cardiac cycle?
Atrial systole (atria contract and push blood into ventricles), ventricular systole (ventricles contract and eject blood), early diastole (atria and ventricles relax and fill passively), and late diastole (ventricles still relaxing and filling passively).
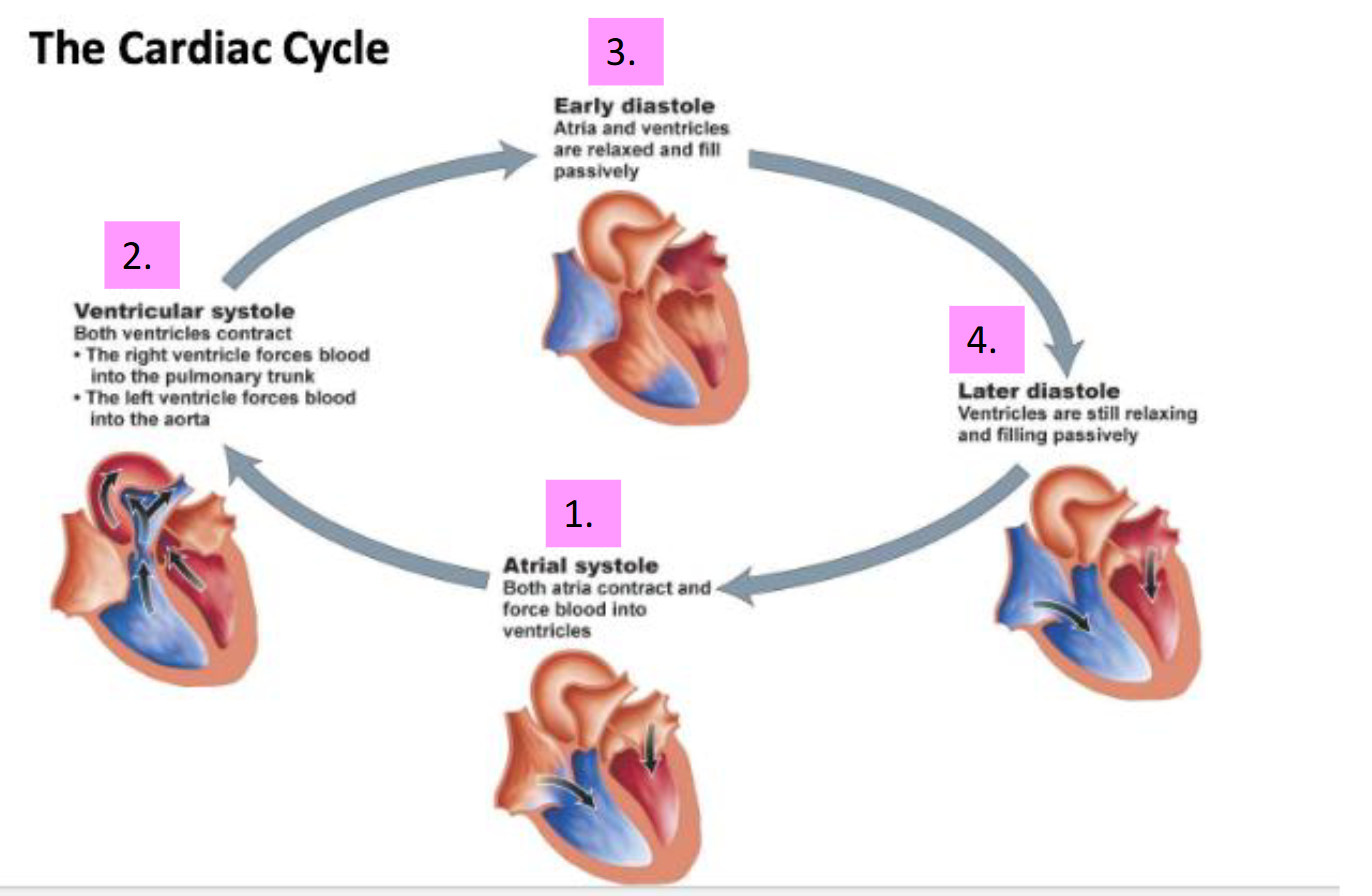
What occurs during atrial systole?
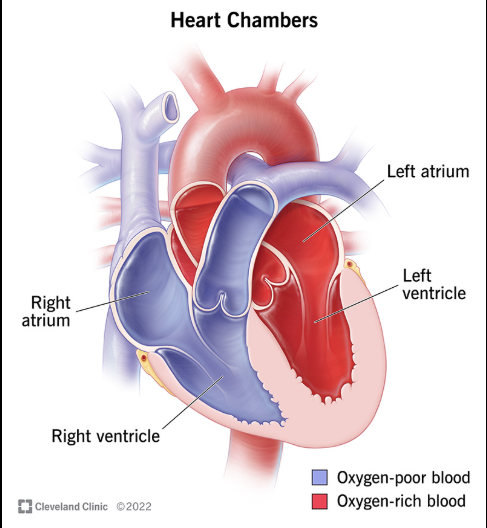
Both the atria are contracting and forcing blood to move into the ventricles
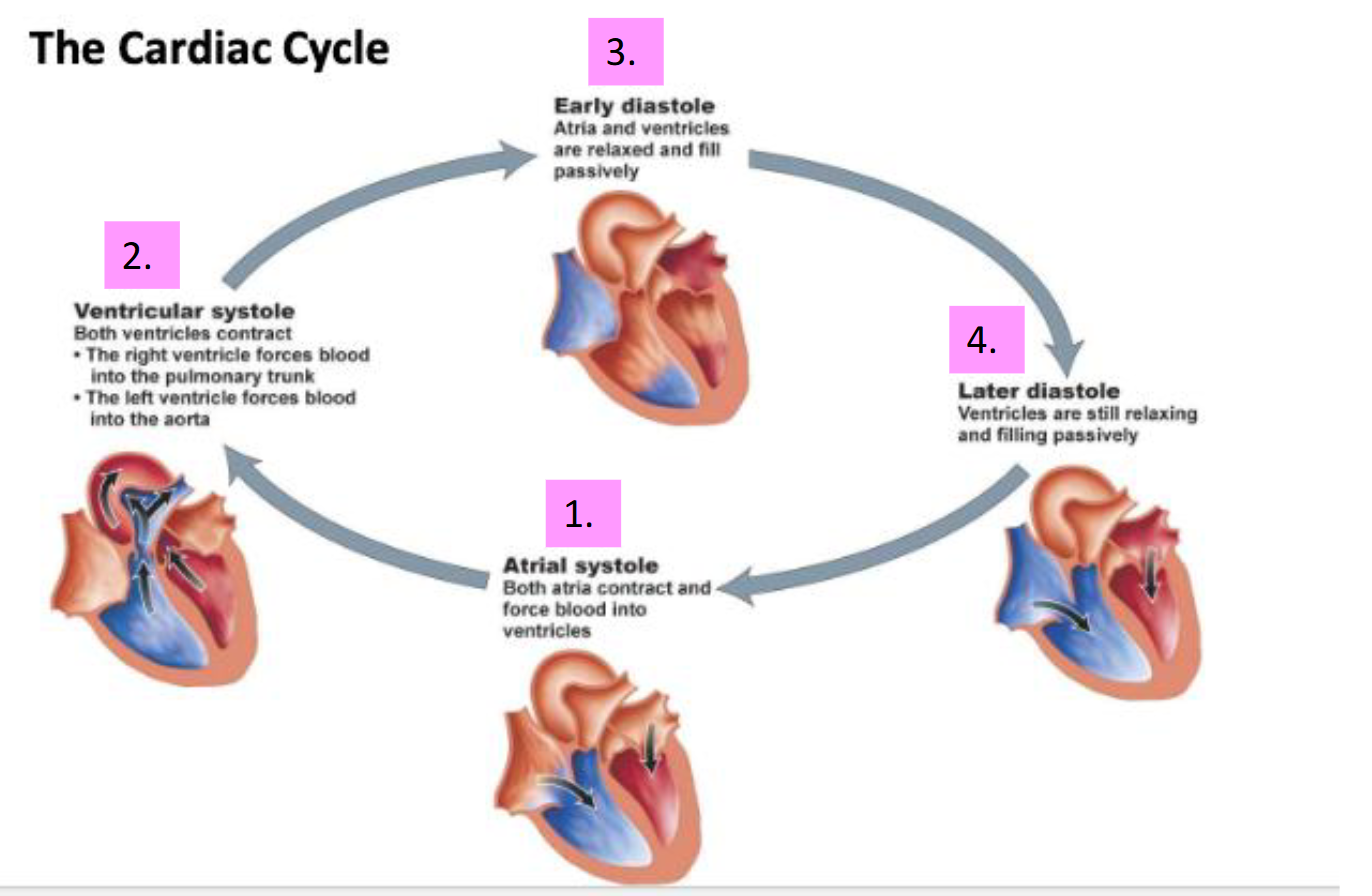
What occurs during ventricular systole?
Both the ventricles are contracting
Right ventricle forcing blood into the pulmonary trunk
Left ventricle forcing blood into the aorta
What occurs during early and later ventricular systole?
Early → Neither of the chambers are contracting
Atria and ventricles are relaxed and fill passively
Later → Still in a relaxed state
Ventricles are still relaxing and filling passively
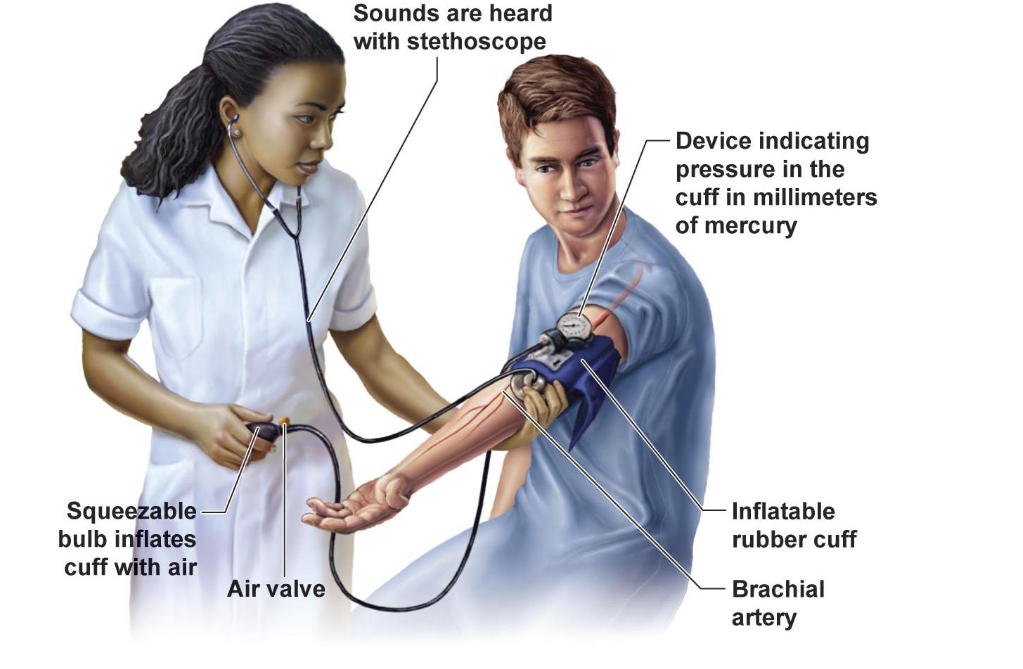
What is systole vs. diastole in blood pressure?
Systole is ventricular contraction and corresponds to the higher arterial pressure
Diastole is cardiac relaxation and corresponds to the lower arterial pressure (afterload is the diastolic pressure the heart works against to eject blood)
Normal blood pressure is 120/80
Top is systole number and bottom is diastole number
Diastolic arterial pressure is called the AFTERLOAD - the pressure against which the heart must work to eject blood during systole (systolic pressure)
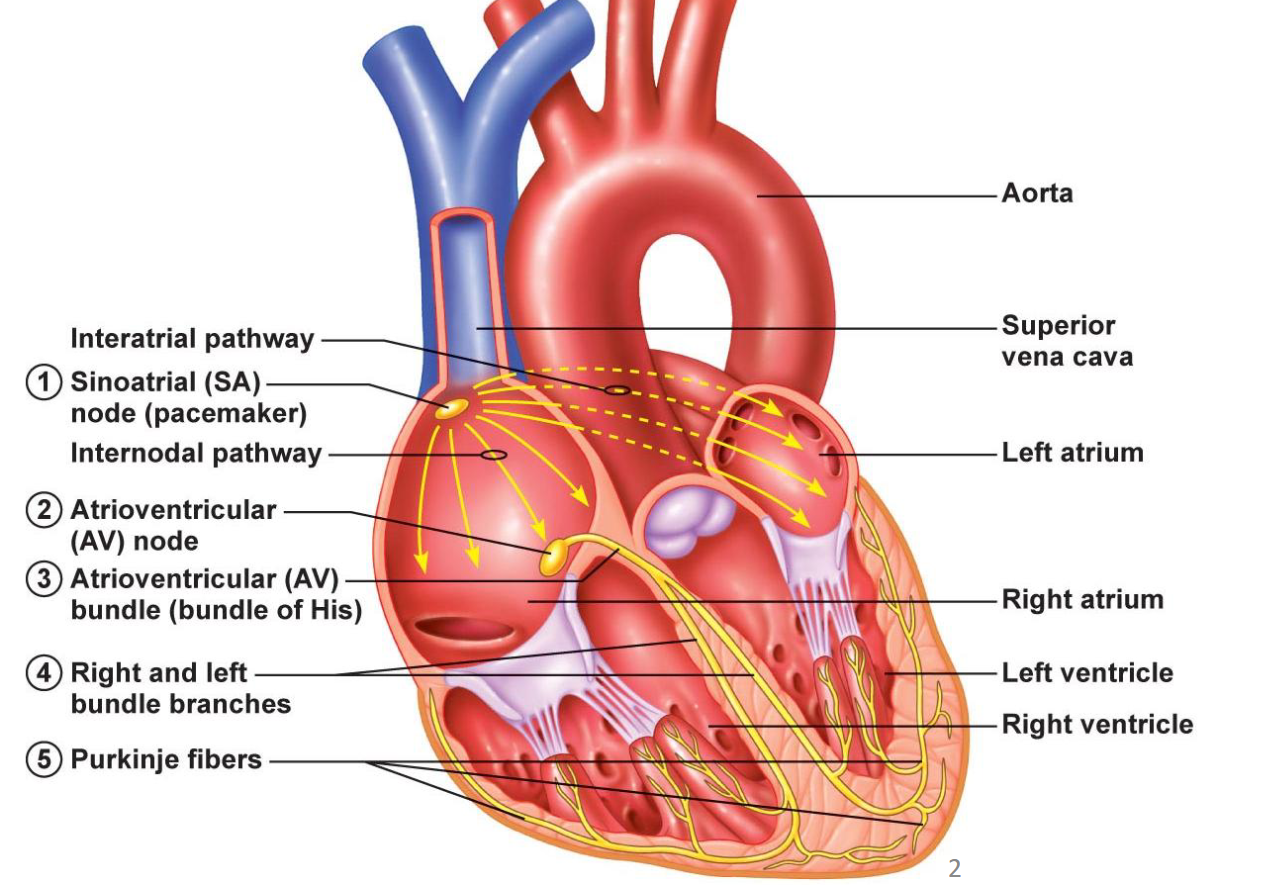
How do the SA nodes and the AV nodes help the heart beat?
Nodes are small, specialized clusters of cells that help to generate and regulate electrical impulses → signals that make the heart contract and pump blood
SA nodes → Heart’s pacemaker, electrical impulses generated here
Av nodes → Help conduct those electrical impulses
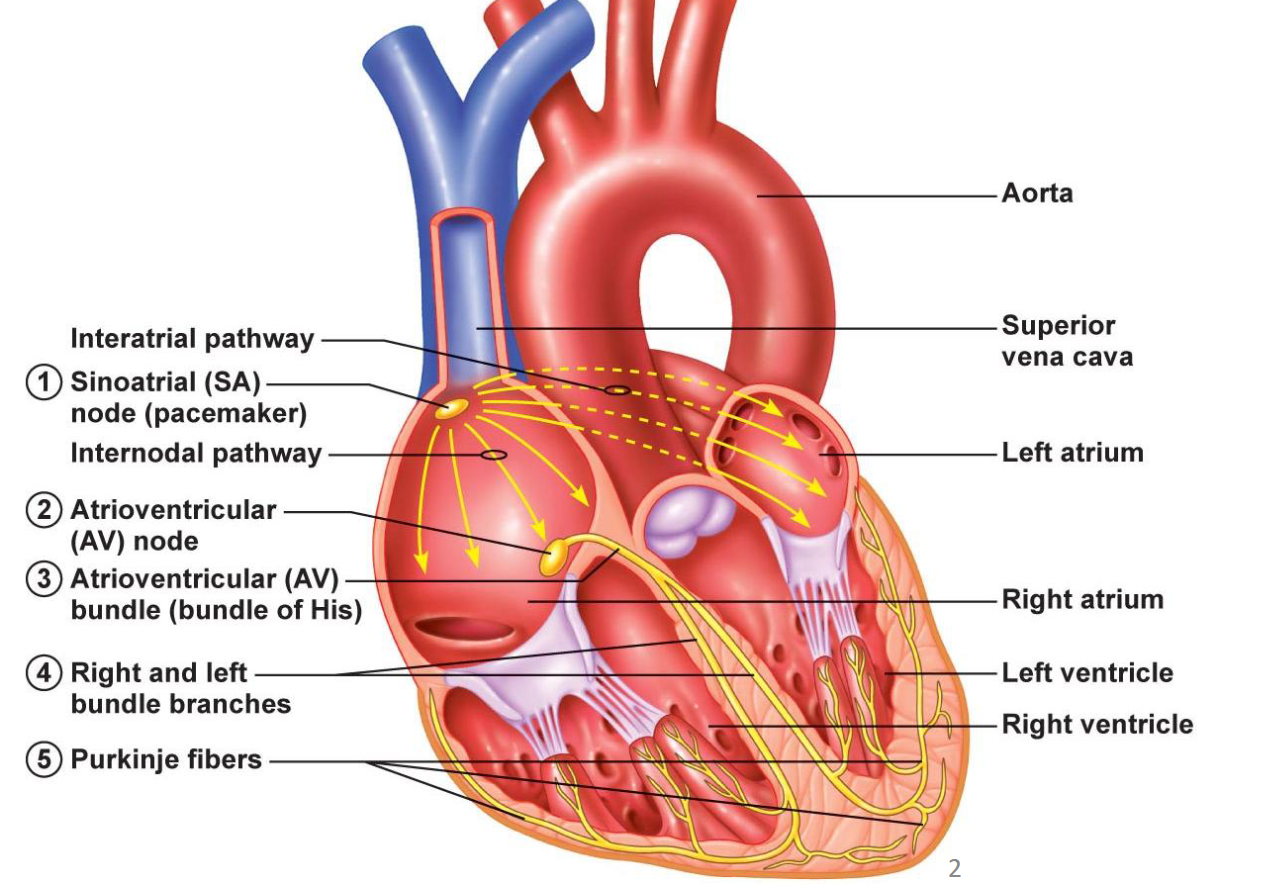
What structures conduct the electrical signal through the heart, in order?
SA node (pacemaker) → internodal and interatrial pathways → AV node → bundle of His → right and left bundle branches → Purkinje fibers → Down to both ventricles
Ensures both ventricles contract simultaneously and efficiently
What is the role of gap junctions in cardiac muscle?
Cardiac muscle consists of individual cardiomyocytes (cardiac muscle cells) connected by intercalated discs (GAP JUNCTIONS!) to work together as a single functional organ
Helps with ensuring that that signal is being propagated and moved forward to allow the heart to beat properly.
What are some examples of conduction problems in the heart?
Usually results in arrythmia (irregular heartbeat)
Abnormal SA node firing leading to a downstream effect (tachycardia [fast], bradycardia [slow])
Blockages e.g. at the AV node, vary in terms of degree of the blockage
Can slow down or prevent signal propagation from atria to ventricles
Ventricles can contract independently (bundle of His, 40 bpm)
Fibrillations are more serious, occurring when cells depolarize independently
Atrial fibrillation (also called A-fib) is a quivering or irregular heartbeat (arrhythmia)
Ventricular fibrillation, or V-fib, is considered the most serious cardiac rhythm disturbance!
Compare the sympathetic and the parasympathetic nervous system
SNS → will carry signals that put your body's system on alert
PNS → carrying signals that relax those systems, so doing the opposite.
Concepts of balance and homeostasis, and having methods to turn signals up and turning those signals down as well.
How do sympathetic and parasympathetic systems affect heart function?
Sympathetic input (norepinephrine, epinephrine) increases heart rate and contraction strength respectfully
Parasympathetic input (acetylcholine) decreases heart rate
How much can heart rate and cardiac output increase with exercise?
Heart rate increases to nearly 200 bpm (Max heartrate is 220−age beats per minute)
Cardiac output can increase from ~5 L/min at rest up to 25 L/min (or ~40 L/min in elite athletes or 10 4L milk jugs)
HIT (High Intensity Training) can be used to increase fitness levels in a short duration of time

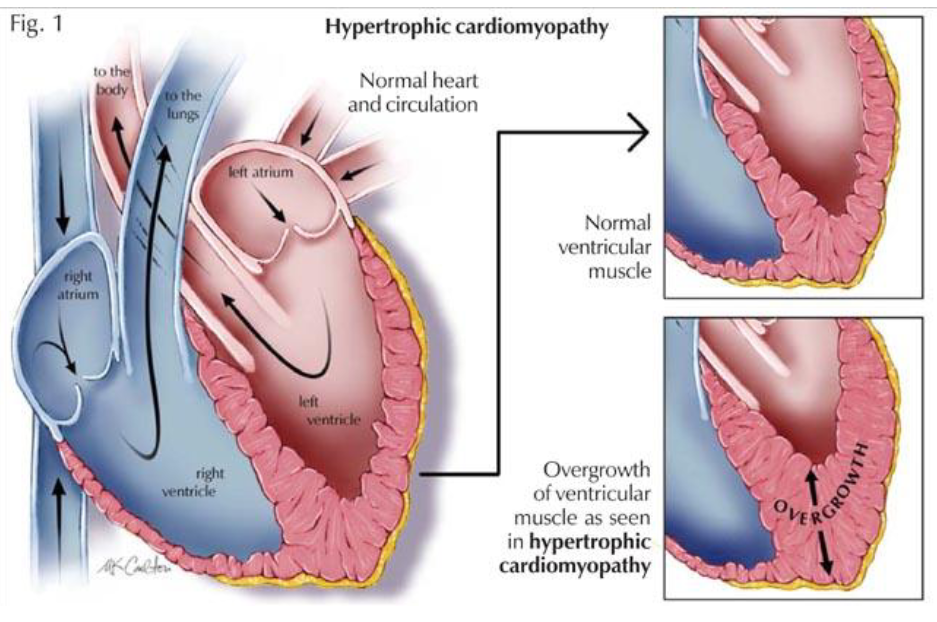
What is cardiac hypertrophy and when is it good vs. bad?
A sign of being “overworked”.
The heart muscle will respond and hypertrophy (increase in size) just like your skeletal muscle would respond to weight-lifting.
The Good (“Normal”): Athlete's heart – an appropriate adaptation! Occurs in both endurance athletes and weightlifters!
The Bad: Causes include high blood pressure and narrowing of
aortic valve ... the heart must work harder to overcome these adaptationsExample: In individuals who have obesity. Sometimes they will present with this cardiac hypertrophy, but in this case, it is considered a negative adaptation that can have poor consequences on their health
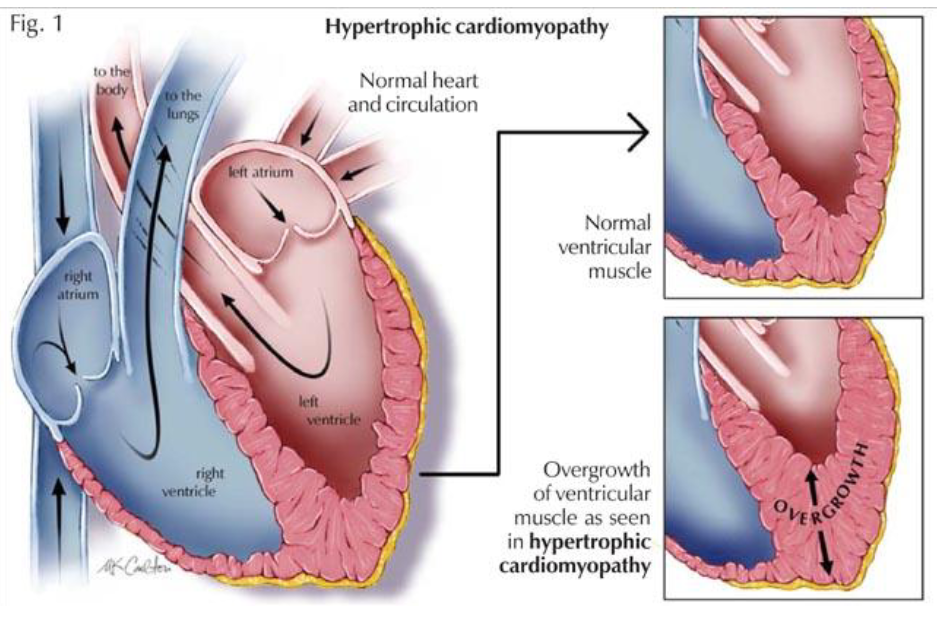
How do endurance athletes vs. weightlifters typically remodel their hearts?
Endurance athletes – mostly an increase in LV chamber (need to increase cardiac output)
Weightlifters – mostly increased LV wall and septum thickness (need to overcome increased afterload – the amount of pressure needed to eject blood during ventricular contraction)
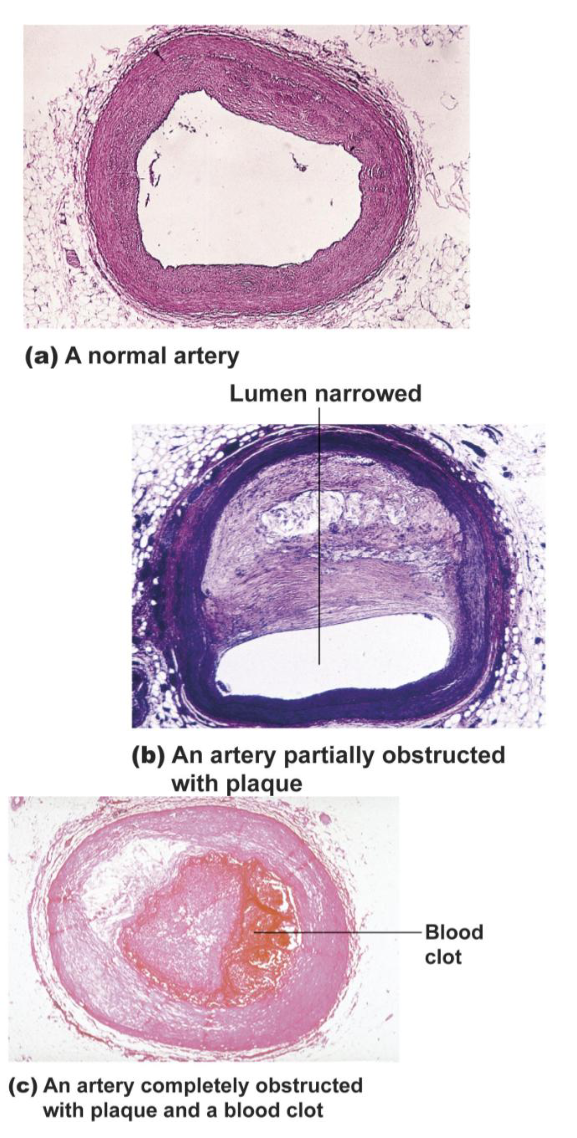
What is atherosclerosis?
Narrowing of arteries due to calcified fatty deposits (plaque) and thickening of the wall
Triggered by damage to arterial wall
(inflammation!)Can lead to heart attack or stroke
When this occurs in the arteries of heart muscle, it is called coronary artery disease
List key risk factors for atherosclerosis and how to prevent them
Factors that can put you at risk include elevated blood lipids (high LDL cholesterol), hypertension, inflammatory mediators (C-reactive protein)
Diet (lower sodium, higher potassium, lower saturated/trans fats, *cholesterol)
Instead of limiting dietary cholesterol, limit saturated/trans fats that can lead to high LDL levels
Genetics → Specific genetic variant makes it hard to reduce LDL cholesterol levels through lifestyle changes like diet. Individuals who don’t have this gene…easier to bring those LDL levels down
Smoking, physical inactivity, obesity/diabetes
Age and Others...
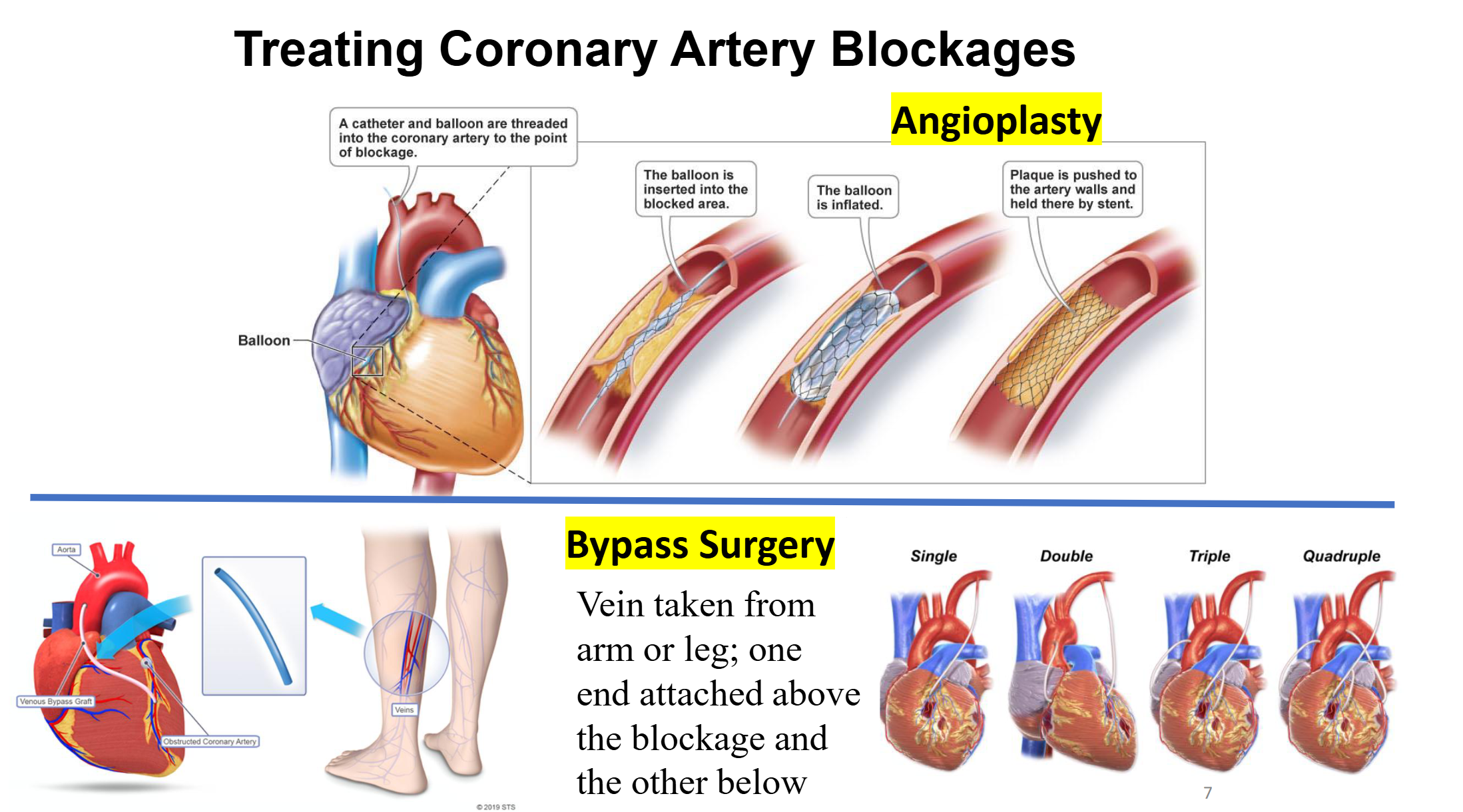
How can coronary artery blockages be treated mechanically?
Angioplasty → Insertion of a balloon into a blocked area
Balloon is subsequently inflated, and the inflation of this balloon then pushes plaque to the artery walls.
A stent is placed in order to keep that plaque pushed up against those walls.
Bypass Surgery → Vein taken from arm or leg; one end attached above the blockage and the other below
Single, double, triple, or quadruple bypasses are possible
Define systolic and diastolic arterial blood pressure
BP varies with cardiac cycle
Systolic BP is the maximum arterial pressure during ventricular contraction
Diastolic BP is the minimum arterial pressure when the heart relaxes between beats, maintained (not zero) by elastic recoil of arterial walls
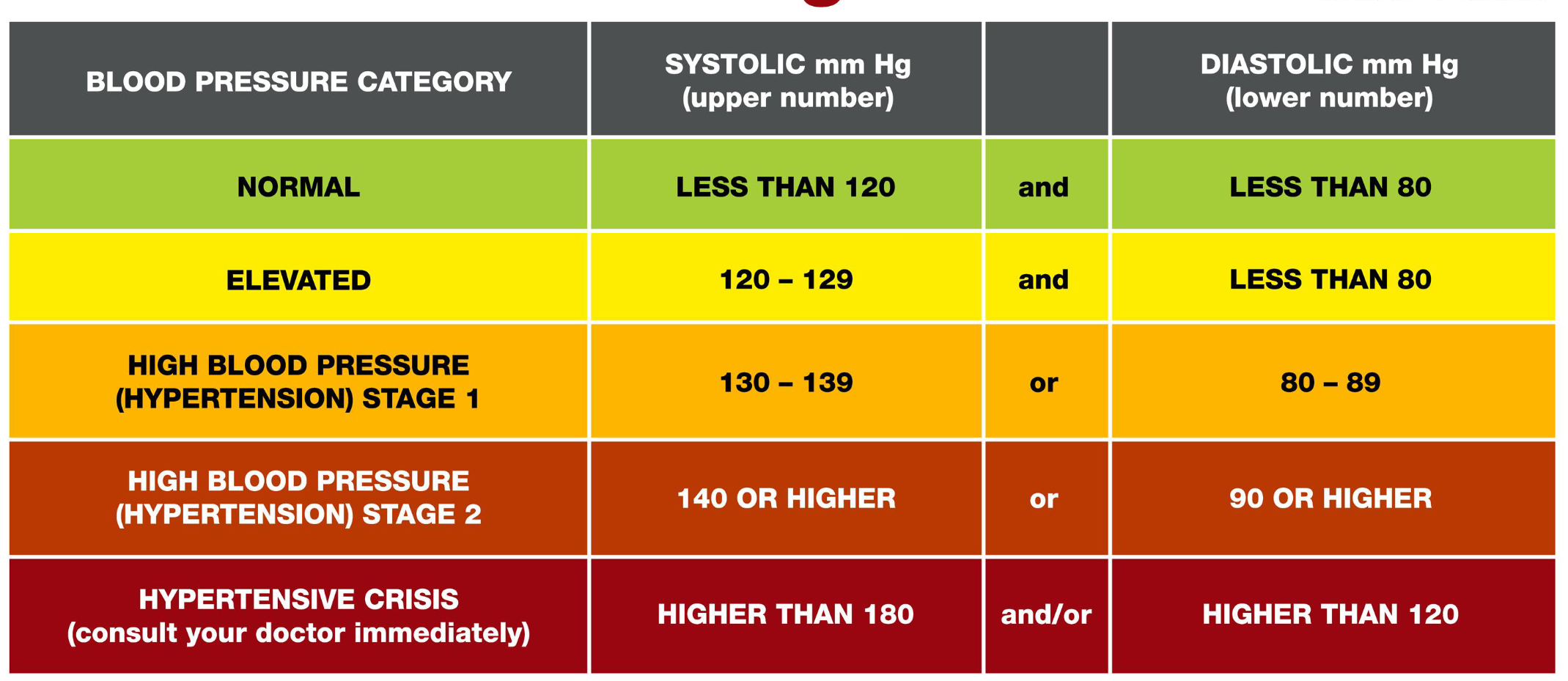
Normal Range → Systolic < 120 mmHg and diastolic < 80 mmHg
Blood Pressure Catergories
Hypotension is when blood pressure is too low!
Blood pressure should stay near the normal/healthy range
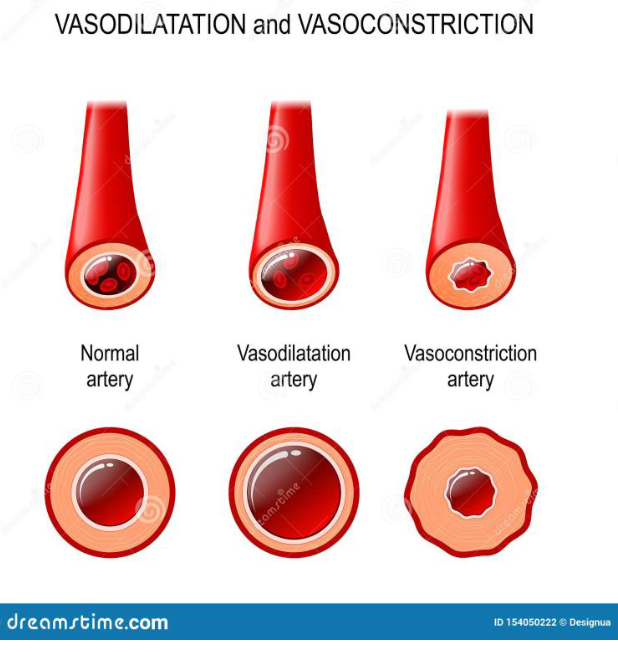
How does neural control cause vasoconstriction in arterioles?
Alpha-receptors are located on arteries.
Norepinephrine and epinephrine bind to (alpha-2) adrenergic receptors
This causes arteries to constrict (vasoconstriction)
This increases blood pressure! (Diameter/area where the blood can flow is lower → higher pressure state!)
E.g. during exercise
More so about redirecting the blood flow away from non-exercising tissues, for example, the digestive system, and then directing them more towards exercising muscles, which require more blood flow.
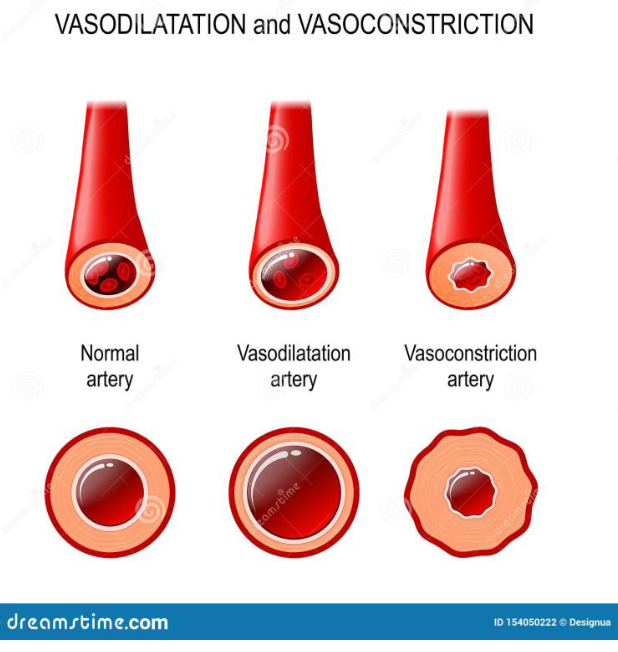
How does neural control cause vasodilation in skeletal muscle arterioles?
Blood vessels in skeletal muscles lack alpha-receptors
Norepinephrine and epinephrine bind to b2 adrenergic receptors found in arteries of skeletal muscle
This dilates vessels of the skeletal muscles (vasodilation) so they can receive increased blood flow (body will send more blood flow to the area that needs it most)
E.g. also during exercise!
What happens to blood pressure during Aerobic (Cardio) Exercise?
Blood pressure only increases minorly during exercise compared to cardiac output that has a dramatic increase (5x, up to 8x in athletes!)
Distribution of blood does not increase proportionally – blood flow is diverted to where it is needed during exercise! The working muscles!
Dilation of vessels to skeletal muscle and heart increases blood flow to muscles (β2 receptors and local metabolites)
Constriction of vessels to the gut and kidneys decreases blood flow to these organs (a2 receptors)
Dilating vessels in the muscle decreases resistance and we have a lot of muscle mass!
So, blood pressure does NOT increase dramatically during exercise!
How does resistance (weightlifting) exercise affect blood pressure differently from aerobic exercise?
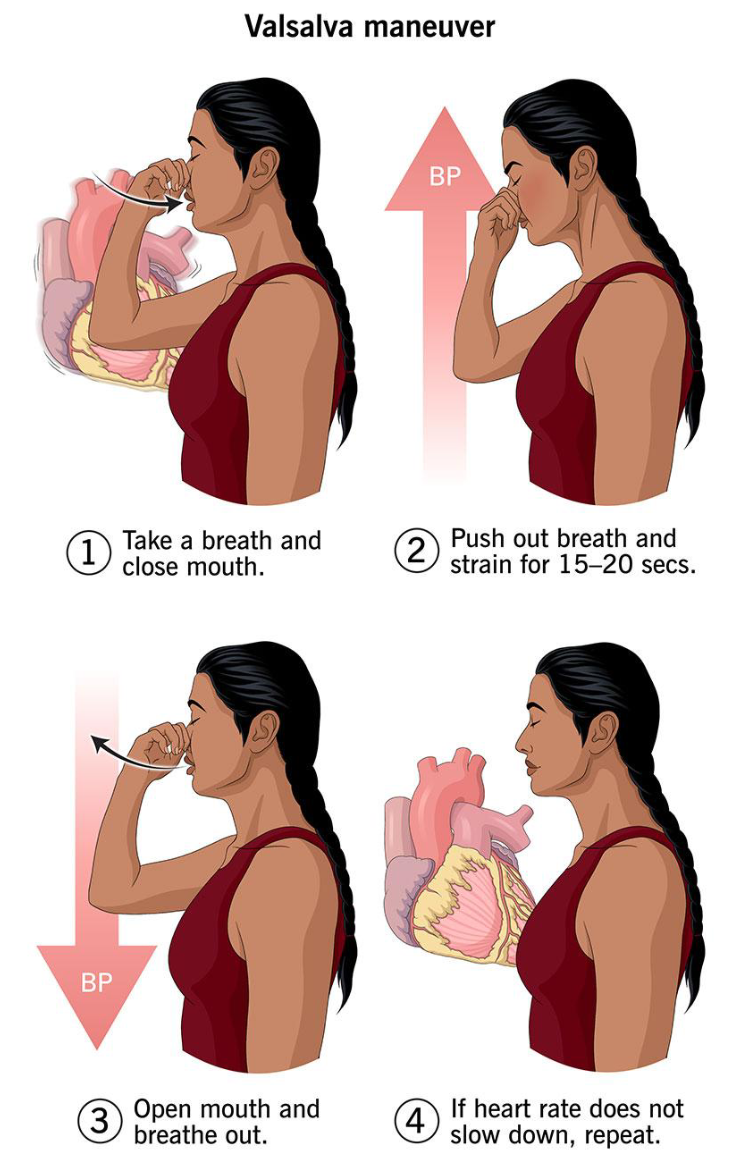
Resistance exercise (e.g. weightlifting) CAN cause dramatic increases in blood pressure - up to 345/245 mmHg! (not concerning since only happening for a short time)
Due to the Valsalva maneuver, which increases intrathoracic pressure, temporarily raising BP and reducing venous return
Holding the breath and straining during a lift, which increases intrathoracic pressure, transiently elevates blood pressure, and can slow heart rate