Gen Med Exam 2 (Allie's Version)
1/158
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
159 Terms
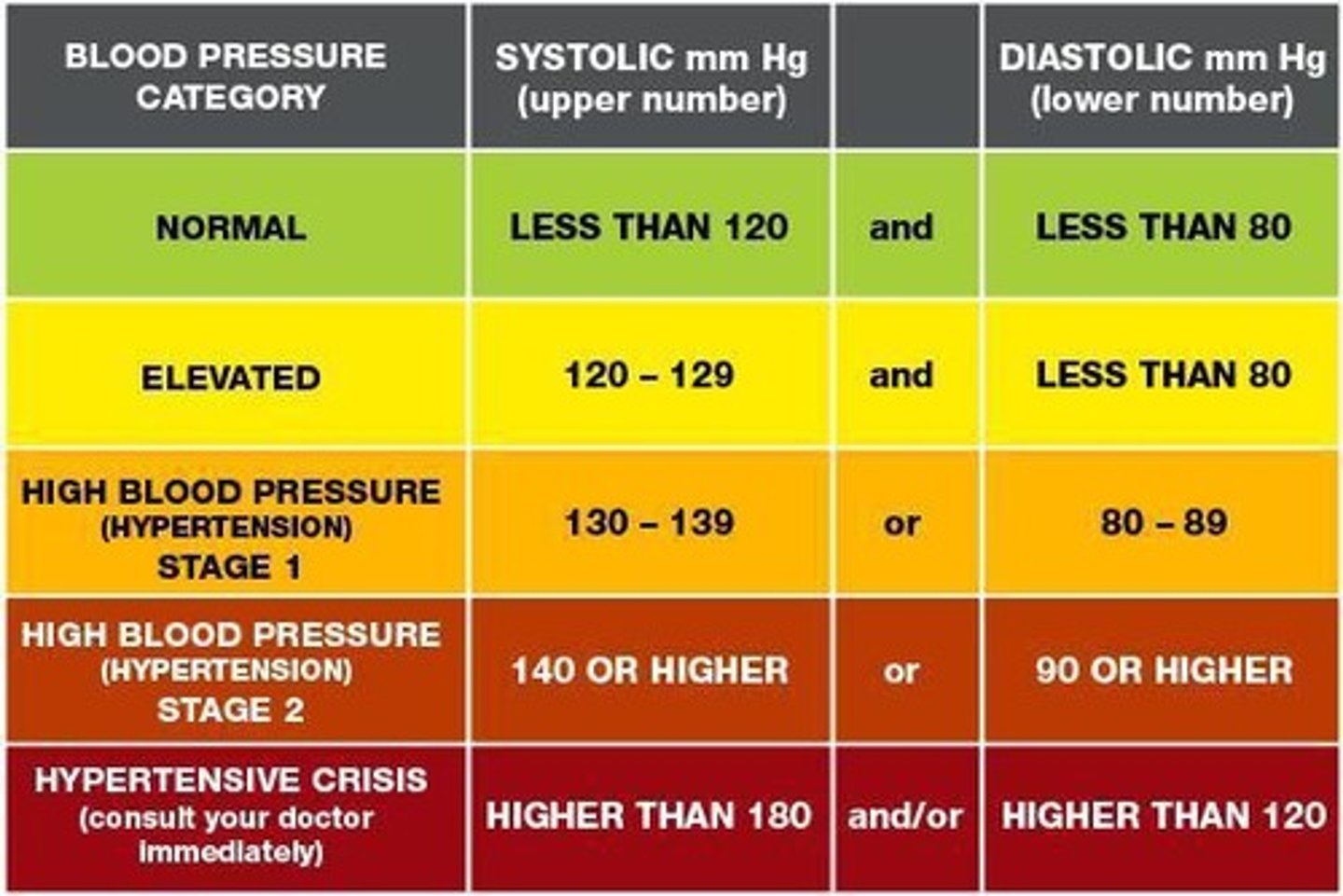
hypertension
persistent elevation of blood pressure
lower
BP tends to be ____ in children until about age 12 when it starts to be similar to adults
increases
prolonged HTN ____ the risk of CVD
- produces a pressure overload on the L ventricle, causing L ventricular hypertrophy
- diastolic dysfunction with impairment of LV relaxation develops early
prevention
____ of HTN
- everyone should know their BP
- frequent monitoring in those with risk factors
- physical activity
treatment; lifestyle
____ of HTN begins with ____ modification
- weight loss
- diet
- reduced Na intake
- PA
- smoking cessation
- alcohol cessation
- stress management
pharmacologic
____ management of HTN
- diuretics
- ACE inhibitors and ARBs
- vasodilators
- Ca2+ channel blockers
- beta blockers
- alpha adrenergic blockers
150; 300
exercise guidelines for HTN
- ACSM encourages ____ to _____ min/week of moderate to vigorous physical activity
- should be individualized to the person!!!
precautions; relative; breath
____ of exercise for pt. with HTN
- medical evaluation/clearance recommended with uncontrolled severe HTN (resting SBP > 180 OR DBP > 110)
- resting SBP > 200 or DBP > 110 is a ____ contradindication to exercise (especially vigorous)
- exercise should be stopped if SBP > 250 or DBP > 115
- avoid ____ hold and valsalva
hypotension
abnormally low blood pressure
orthostatic hypotension
abnormal drop in BP within 3 minutes of standing
- drop in systolic > 20 mmHg or diastolic > 10 mmHg
pooling; decrease; CV
hypotension is caused by ____ of blood in the LEs associated with:
- conditions that ____ vascular volume (dehydration, meds, hemorrhage, burns)
- impaired muscle pump function (bed rest, impaired mobility, SCI
- impaired ____ reflexes (meds, disorders affecting ANS, aging)
non
a fall in BP with an increase in HR indicates a _____ neurogenic cause
- HR is compensating, ANS is intact
neurogenic
a fall in BP with < 10 bpm change in HR indicates a _____ impairment
- baroreflex is not working (HR is not rising appropriately)
dizziness; syncope; blurred
s/s of orthostatic hypotension
- _____, lightheadedness, vertigo
- ____ and presyncope
- weakness, fatigue
- nausea
- ____ vision
- confusion
- falls
BP
diagnosing orthostatic hypotension
- ____ measurements in supine and standing
- tilt table test
cause; medications
treatment of orthostatic hypotension
- alleviate the ____
- conservative measures
- _____
education; slowly; ankle
conservative measures for orthostatic hypotension
- patient ____ : avoid situations that cause excessive vasodilation (alcohol, temp extremes), recommend activity modifications
- elevate HOB, have patient rise _____, wait for BP to stabilize with changes of position
- exercises: ____ pumps, UE/LE ROM, diaphragmatic breathing, crossing legs
- elastic stockings, abdominal binders
- physical fitness
lie; elevate
if there is an excessive drop in BP or the patient is symptomatic you should ____ the patient down, ___ their feet, document and notify the physician if symptoms do not improve
aneurysm
abnormal stretching or dilation of a vessel wall
- diameter 50% greater than normal
- results from vessel wall weakness
Atherosclerosis; marfan's; inflammatory
who is at an increased risk for aneurysms?
- HTN
- _____
- cigarette smoking (5x INCREASED RISK)
- family history
- male
- age
- congenital disorders of CT (_____ disease)
- _____ and infectious diseases
- trauma
location; appearance
aneurysms are named for their _____, size, and _____
asymptomatic
aneurysms are often _____
- people don't know they have one
thrombosis; rupture
aneurysms can lead to ____, dissection (tear), or ____
- MEDICAL EMERGENCY
conservative
a ____ approach is recommended for an aneurysm with physician follow up
- may require surgery, typically when > 5 cm
low; moderate; low; increased
Exercise considerations- ANEURYSM
- little research
- ___ to ____ intensity aerobic activities (may have high and low BP restrictions)
- ____ resistance if incorporating strengthening (not recommended with cerebral aneurysm)
- restrict exercise training with ____ size of aneurysm
PVD
includes disorders of arterial and venous blood vessels
PAD
arterial occlusive
inflammatory PVD
polyarteritis nodosa
ateritis
kawasaki disease
thromboangiitis
obliterans (buerger's disease)
wegener's granulomatosis
vasomotor PVD
raynaud's
venous PVD
varicose veins
chronic venous insufficiency
VTE
CVI (chronic venous insufficiency)
results from incompetent venous valves, inadequate muscle action, or venous obstruction
- damaged or incompetent valves allow venous blood to pool and flow backward, leading to increased volume and pressure in the vessel (venous HTN)
- veins become enlarged and weak
- Risk factors: age, genetics, obesity, prolonged standing, sedentary lifestyle, smoking, female hormones and pregnancy
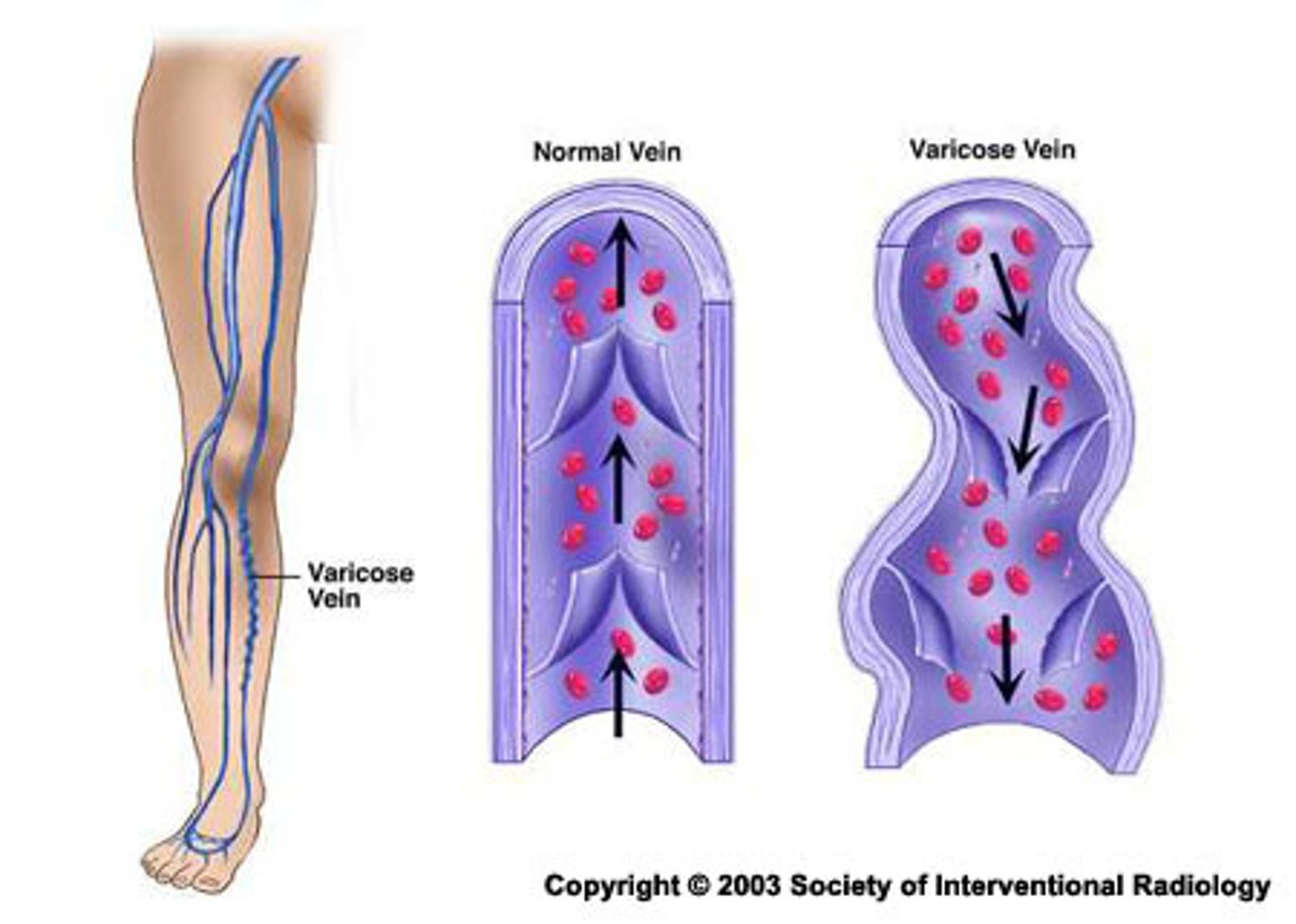
varicose; skin; ulcerations
CVI leads to:
- ____ veins
- spider veins
- swelling
- ___ changes (inflammation and fibrosclerotic remodeling)
- hemosiderin staining (rust looking skin)
- chronic leg _____ (80% of all ulcerations)
venous; surgical; prognosis
treatment of CVI
- promote ____ return
- rest and elevation throughout day
- avoid dependent positions
- raise foot of bed 6 in
- compression stockings, pumps
- ROM exercise, progressive ambulation
- wound care prn
- medical and ____ management
- poor ____ for resolution of CVI
true
T/F: you must take caution with compression dressings and elevation with CVI due to common comorbidities of arterial insufficiency, DM, and CHF
arterial
findings with _____ PVD
- aching/cramping that is predictable with activity and elevation
- edema may or may not be present
- reduced muscle mass
- elevation worsens symptoms, dependency improves symptoms
- aching begins at a specific time/distance when walking and goes away with rest, will return with exercise
venous
findings with _____ PVD
- aching, burning, cramping, fatigue while standing, heaviness, night cramping, swelling, throbbing
- edema is worse at the end of day, improves with elevation
- muscle mass is unaffected
- elevation lessens symptoms
- walking lessens symptoms
decreased; cyanotic; cool
more arterial PVD findings
- ____ or absent pulses, bruits may be present
- reduced hair, tight, shiny skin, thick/brittle nails
- ____ or pale skin color, dependent rubor
- ____ skin temp
- ulcers have a pale base, found at high pressure sites such as heel or tip of toes
difficult; hyperpigmented; warm; medial malleolus
more venous PVD findings
- pulses may be _____ to palpate due to edema
- skin: chronic cellulitis, dermatitis, ulceration
- skin color: _____, brown discoloration, often superior to medial malleolus
- skin temp: may be ____ with infection, phlebitis
- ulcers often near _____ and gaiter area of LL, irregular border, often have pink/red base
VTE
Venous thromboembolism, includes DVT and PE.
DVT
typically occurs in LEs or pelvis
- small percentage occurs in UEs
- can progress to pulmonary emboli
pain; dilation
s/s of DVT
- ____ or tenderness in calf
- leg or calf swelling
- ____ of superficial veins
- warmth
- pitting edema
true
T/F: approximately 50% of DVTs are asymptomatic
80%
____ of symptomatic DVTs involve proximal DVT (iliac, femoral, or popliteal)
- usually more severe
- at time of diagnosis > 50% with a proximal DVT already have a PE
causes and risk factors of VTE
- previous venous thrombosis or embolism
- increasing age
- active cancer/cancer treatment
- severe infection
- estrogen containing oral contraceptives
- hormonal replacement therapy
- pregnancy or given birth < 6 weeks
- immobility (bed rest, flight travel, fractures)
- surgery/anesthesia/critical care admission
- central venous catheters
- inherited thrombophilia
- obesity
VTE prevention
education
hydration
activity
mechanical compression
medical management
- goal to decrease hypercoagulability of blood
- low molecular weight heparin
- warfarin
- greenfield filter (catches PE before entering heart)
Wells Clinical Prediction Rule for DVT
-active CA or w/in last 6 months
-paralysis, paresis or recent immobilization
-bedridden for 3+ days
-surgery requiring anesthesia in last 12 wks
-localized tenderness along deep vein
-entire leg swelling
-calf swelling at least 3 cm larger than asymptomatic leg (10 cm below tib tube)
-pitting edema in symptomatic leg
-superficial veins
-prev DVT
-high prob if 2 or more, unlikely if less than 2
prevent; vein; clot
VTE treatment goals
- _____ PE
- limit extension of thrombus
- limit damage to ____
- prevent another ____
s/s of PE
pleuritic chest pain, diffuse chest discomfort
tachypnea, tachycardia
hemoptysis
anxiety, restlessness, apprehension
dyspnea, persistent cough
sudden death
communicate; risk
mobilization with PE
- ____ with medical team before mobilizing
- need to determine ____ of mortality
- low risk vs high risk dependent on clinical parameters of PE severity, hemodynamic stability, signs of R ventricular dysfunction, and elevated troponins
CV; prevention
exercise safety and ____ prevalence
- increasing prevalence of CV risk factors and disease, particularly among minority groups and children
- shared risk factors exist between CV conditions and many MSK conditions
- APTA advocates for _____, wellness, fitness, health promotion, and management of disease and disability
true
T/F: individuals who do not smoke, maintain a BMI < 30, exercise 3.5 hours/week, and consume ample fruits, vegetables, and whole grains can reduce the risk of chronic illnesses (diabetes, heart attack, stroke, cancer) by an average of 80%
PAVS (Physical Activity Vital Sign)
a quick screening tool to assess PA levels
1. On average how many days per week do you engage in moderate to strenuous exercise? ____ days
2. On average, how many minutes do you engage in exercise at this level? ____ days
Total minutes per week = #1 x #2
Recommended 150 min/week of mod intensity or 75 min/week of vigorous intensity
CVD risk factors
Age, family history, smoking, sedentary, obesity, hypertension, dyslipidemia, prediabetes, stress, diet
emerging CVD risk factors
CRP
- low risk < 1.0 mg/dL
- ave risk 1.0-3.0 mg/dL
- high risk > 3.0 mg/dL
Homocysteine
Kidney disease
Environmental factors, infection, abnormal sleep, etc.
Gender, racial and ethnic disparities
risk assessment and pre-participation screening
can be gathered during subjective questioning or using simple assessment tools
- PAR-Q+ and ePARmedX
- Framingham Risk Score
- ACC/AHA Risk factor profile
- other online resources
screening focuses on: risk factors for disease, s/s of disease, presence of disease
light intensity
- able to talk and/or sing
- RPE <3 or <11 (depending on scale)
- <40% HRR or VO2R
- <64% of maxHR
- <3 METs
moderate intensity
- able to talk but not sing
- RPE 3-4 or 12-13 (depending on scale)
- 40-60% HRR or VO2R
- 64-76% maxHR
- 3-6 METs
vigorous intensity
- difficulty talking
- RPE >5 or >14 (depending on scale)
- > 60% HRR o VO2R
- >76% maxHR
- >6 METs
inpatient; outpatient; maintenance
Cardiac rehab
- phase 1 = ____
- phase 2 = ____
- phase 3 = _____
indications for cardiac rehab
-MI
-stable angina
-CABG
-PTCA or other transcatheter procedure
-stable heart failure, cardiomyopathy
-valve disease/surgery
-heart transplant
-PAD
-at risk for CAD (DM, dyslipidemia, HTN, and obesity)
Phase 1 cardiac rehab
inpatient
goals:
- offset effects of bed rest
- patient monitoring and assessment of hemodynamic responses to allow safe return to activity
- identify impairments that influence prognosis
- prepare patient and support system for home progression
- recommendations for continued cardiac rehab
could be 24 hr stay if PCI, but often < 5 days for uncomplicated MI, CABG
immediate post MI
ECG changes
12-48 hrs post MI
cardiac enzyme changes
3 days to weeks post MI
removal of damaged (necrotic) myofibrils
3 weeks to months post MI
collagen bundle replaces muscle tissue
scar formation
AACVPR
risk stratification that helps to determine prognosis, rate of activity progression, supervision, and monitoring required
CV test and measures
- inspection
- vitals and pulse ox
- circulation
- auscultation
- activity evaluation (aerobic capacity/endurance)
normal
____ CV activity assessment
- gradual increase in HR (10 bpm per MET)
- sinus tachycardia on ECG (no change in chronic arrhythmias
- Gradual increase in SBP (10 mmHg per MET)
- small decrease/no change in DBP
- SpO2 97-100%
- increase in ventilation/hyperpnea
abnormal
____ CV activity assessment
- chronotropic impairment (sinus bradycardia, disproportionate increase, decrease or failure to increase with increasing workload)
- increase in arrhythmia
- ventricular arrhythmias
- ST segment elevation/depression
- chest discomfort/pressure
- SBP > 250, drop > 10 from baseline, or failure to increase with increased workload
- rise or fall of DBP > 10-15 or >115
- desat below 90% with activity
- hyperventilation/dyspnea/wheezing
- angina, SOB, dyspnea, palpitations, dizziness, pallor, fatigue, confusion
RPP
myocardial oxygen consumption is estimated by:
____ = HR x SBP
- aka double product
frequency; intensity
phase 1 ____
2-4x/day, at least 1x/day
____
- RPE < or equal to 13 (fairly light-somewhat hard)
- use of HR not necessarily appropriate, especially if on B-blocker
- monitor hemodynamic and symptomatic responses, ECG findings
duration; type
phase 1 ____
- 10-15 min
- begin with short bouts (3-5 min), use frequent rests (goal 2:1 exercise/rest)
- include warm up and cool down exercises
_____
- functional activities, large muscle group activities
documentation
phase 1 _____
- pt. position, level of assist and time
- type of sitting and/or standing exercises
- time period and distance ambulated, number of stairs
- number and duration of rests
- vital sign response to each activity
- education provided
CR phase 2
outpatient
- class I recommendation (leads to good outcomes)
- involves education, exercise, and behavior change
2
goals of phase ____ CR
- supervision and monitoring of the patient and assisting with implementation of a safe and effective physical activity program
- helping the patient return to vocational and recreational activities
- risk factor reduction
- improve pyschosocial well-being, which influences recovery from heart disease
frequency; intensity
CR phase 2 _____
- at least 3x/week, ideally 5-7x/week
____
- RPE 12-16
- may have exercise test 4-6 wks post hospital discharge
- 40-80% HRR or 75-80% HRmax if test available
- use HR at least 10 bpm below ischemic threshold is (+) exercise test
duration; type
CR phase 2 _____
- 20-60 min
- begin with multiple short intervals (<10 min), gradually increase (+1-2 min/day)
- include 5-10 min warm-up and cool-down (low intensity aerobic activities)
_____
- large-muscle group activities (walking, cycling, functional activity, FUN)
- supplement with increase in daily lifestyle activities (gardening, walk break at work, household work)
exercise testing
useful for diagnosis of CAD, evaluation of symptoms, determining prognosis and severity of disease, evaluation of functional capacity, activity prescription, evaluation of effectiveness of therapy, reassurance and motivation
- many pts. DO NOT have this
without
exercise intensity _____ an exercise test available
- activity should be gradually progressive in logical stepwise fashion of increasing energy costs (METs) with appropriate HR and BP monitoring (initial MET level based on estimate of baseline level of training, likely 2-4 METs)
- titrate based on RPE, s/s, physiologic response
- conservative prescription usually best initially
- FCE (6 min walk)
resistance
patient criteria for _____ training
- min of 5 wks after MI or cardiac surgery including 4 wks of consistent participation in a cardiac rehab program
- min of 3 wks following PTCA including 2 wks of consistent participation in a cardiac rehab program
- no evidence of: symptomatic heart failure, uncontrolled arrhthymias, unstable symptoms, uncontrolled HTN, severe valvular disease
resistance training
_____ _____ guidelines
- elastic bands, free weights, weight machines, body weight
- 2-3x/week, rest day between workouts
- 1 set of 8-10 reps for each major muscle group (30-40% 1-RM for UE, 50-60% 1-RM for LE, RPE 11-14)
- typically can progress 2-5 lbs for UE or 5-10 lbs for LE when 12-15 reps performed comfortably
- emphasize exercise safety
- stop exercises with any concerning s/s
work
assessing a pt's _____ environment
- primary movements (type of contractions) and muscle groups used
- MET demand
- environmental factors (temp stress)
- intermittent heavy work
exercise
____ prescription for return to work
- include both resistance and aerobic training
- include functional exercises (simulate work tasks and muscles used/movement patterns)
- expose them to similar environmental conditions if relevant to work setting
2
phase ____ education
- risk factor reduction (secondary prevention)
- selecting appropriate exercise intensity
- patient self-monitoring during activity
- ability of a patient to recognize adverse symptoms
CR phase 3
maintenance is focus (self monitored home program)
- requires 30-60 min, 3-5x/week, continues indefinitely
- compliance is an issue (20-50% continue exercise after 1 year)
independent
considerations for ____ exercise
- cardiac symptoms are stable
- appropriate responses to exercise (HR, BP, ECG)
- demonstrated knowledge of proper exercise principles and awareness of abnormal s/s
- motivation to continue exercise w/o direct supervision (adherence)
benefits
____ of CR
- risk factor reduction
- improvement in exercise tolerance and symptoms (decreased myocardial O2 demand due to reductions in HR and/or BP at any given submaximal work rate
- increased VO2max and functional capacity
- improved psychosocial well-being and quality of life
- decreased mortality
false (should not start until compensated)
T/F: patients with decompensated (uncontrolled) CHF should begin aerobic exercise training, no matter if CHF is compensated
red
_____ light HF warning signs
- difficulty breathing even at rest
- unrelieved SOB
- wheezing, chest pain, or chest discomfort
- feeling faint
- confusion
- call physician immediately or immediate visit to the ED
yellow
____ light HF warning signs
- weight gain > 3 lbs in 1 day or 5 lbs in 1 week
- increased swelling
- increase cough
- increase in SOB w/ activity
- increase in number of pillows needed
- communicate with physician as the patient may need adjustment in meds
green
_____ light HF warning signs
- no SOB
- no weight gain
- no swelling
- no chest pain
- no decrease in ability to maintain activity level
- proceed with interventions/exercises/activity as planned
heart failure
what condition is the exercise prescription for?
F- 3-5 days/week
I- moderate to high
- 3/10 on dyspnea scale
- also use RPE, many patients on B-blockers
- 50-90% peak VO2 or peak work
- some pts. may benefit from HIIT training
T- progressively increase to 20-60 min/day
T- walking or cycling preferred
tolerate
A person with heart failure can begin resistance training once they can ____ aerobic training
- 3 nonconsecutive days/week
- begin at 40-50% of 1-RM, gradually progress to 60-80%
- 2-3 sets focusing on major muscle groups
- consider NMES
dyspnea
What is often the best monitor of intensity?
NYHA Class 1
Maximum 6.5 METs
- No limitation on PA
- Ordinary PA does not cause undue fatigue, palpitation, or dyspnea
NYHA class 2
maximum 4.5 METs
- slight limitation of PA
- comfortable at rest, but ordinary PA results in fatigue, palpitations, or dyspnea
NYHA class 3
maximum 3.0 METs
- marked limitation of PA
- comfortable at rest, but less than ordinary PA causes fatigue, palpitations, or dyspnea
NYHA class 4
maximum 1.5 METs
- unable to carry out PA without discomfort
- sx. of cardiac insufficiency at rest
- if any PA is undertaken, discomfort is increased
poor; inspiratory
Patients with CHF have ____ ventilatory muscle strength
- Improvements in ventilatory muscle strength and endurance, dyspnea, peak VO2, and 6MWD have been shown after a program involving _____ muscle training
diaphragmatic; decrease
____ breathing and inhibition of excessive accessory muscle use may _____ the work of breathing for a person with HF