Manual Testing in Hematology
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
Use of Peripheral Blood Smear
Used to analyze blood component microscopically - often created when an automated instrument flags an issue
How many identifiers should be on the PBS
At least 2 - name and accession number
When are albumin smears made for PBS
When there is increased number of smudge cells. Only a WBC diff is done on this smear.
How to prevent water artifact on a PBS with low hemoglobin
Let them dry longer
Characteristics of a good peripheral blood smear
Smooth even film with a feathered end
Minimum of 1 inch length
Blood should not carry off the edge or spill over the side
What causes a PBS to be too short
Blood spread too quickly, angle of spreading is >30 degrees
What causes a PBS to be too long
Spreading blood too slowly, angle of spreader <30 degrees
What causes a PBS to be too thin
Too little blood, low Hgb
What causes a PBS to be too thick
Drop of blood too large, patient abnormalities with viscous blood
Pre-test sample requirement for malaria testing
Travel history and indication
How many smears are required in the malaria protocol
8: 4 thin smears, 4 thick smears
What is the use of thick and thin smears for malaria
Thin smears: regular PBS to calculate parasitemia
2 are stained and examined in routine heme labs, 2 are forwarded to special hem for %parasitemia
Thick smears: used to examine for presence of malaria
All 4 are sent right to special heme
How to label malaria slides
Normal indicators, and include MAL or MALARIA or some indication that slides are for malarial examination
Purpose of creating buffy coat smears
Analyze and evaluate blood smears for Bacteria/parasites that may have been observed/questioned on the PBS. Diffs and RBC is not performed
If a PBS shows bacteria and the buffy coat shows extracellular bacteria, what does this indicate?
That there is bacterial contamination on the slides, the stainer, etc.
If a PBS shows bacteria and the buffy coat shows intracellular bacteria, what does this indicate?
Patient is septic
Winthrope tube method for buffy coat (steps)
1. Label 2 wintrobe tubes with patient name and accession number
2. Fill the wintrobe tube with EDTA whole blood and parafilm the top (approx. 0.8mm)
3. Insert wintrobe tube into test tube, secure with gauze
4. Centrifuge for 1500g for 10 minutes
5. Remove excess plasma (leave some above buffy coat, approx. 2mm)
6. Sift off the buffy coat and remaining plasma into separate tube (labelled microtube)
7. Repeat for 2nd tube, combine patient into one tube to increase sample yield
8. Prepare 2 smears and label according to protocol + label with buffy coat
9. Stain the slides with routine hematology staim
When is a cytospin differential indicated?
When the WBC count is above the reference range in order to aid in determining the increased WBC count in CSF or fluids
What is the use of a cytocentrifuge?
Concentrates fluids which normally have relatively low concentrations of cells
How does a cytoscentrifuge work
Slides are placed in centrifuge and the patient sample is added while soinning. Low speed of the centrifuge minimizes cell distortion and concentrates them into a button
How to look under a microscope for fluid analysis
Entire cell button scanned under 10X to search for large abnormal cells or tumor cells
50X or 100X used for cell differentiation
Any area of the cell button can be used for the differential
Use of bone marrow analysis
Determine overall cellularity and quantitate cells present in the bone marrow. Can also be stained differently to look for elements such as iron, reticulinm etc.
What is used instead of a BM aspirate if the bone marrow is hypocellular or there is increased fat/reticulin
Trephine or hole punch biopsy is used and processed by histo. These samples allow for evaluation of bone marrow
BM sample type for cell morph and diff
1mL aspirate in EDTA
Sample type of BM aspirate for immunophenotyping
1mL aspirate in bone marrow media at 4C
Sample type of trephine biopsy
2.0cm sample in a sterile collection container with gauze
What happens if there is no particles present in BM aspiration (no solid marrow tissue in the aspirate)
Another aspiration may need to be performed. Granules/Particles must be obtained for megakaryocyte analysis
BM Push smear
BM smear that can be used for differentials. One drop of aspirate on a glass slide pushed to make a ‘smear’. This is stained using routine hematology stains and special stains if requested. 8 push smears should be made.
BM Squash smear
used for megakaryocyte analysis. A BM particle is placed on a glass slide, and a second slide is used to squish the particle between the glass slides
BM touch prep biopsy smear
Trephine biopsy is lightly rolled and touched between two slides. Prepared in heme before fixation/processing for histo
Contnets of the Wright GIemsa Stain
Methylene blue, purified azure B, eosin.
Also requires ethanol and aged DH2O
pH 6.8
Use of each component of the Wright Giemsa Stain
Methanol - fixes cells and enhances dye uptake
Methylene blue and azure B (basic dyes) - stain acidic components: RNA/DNA, nucleic acids
Eosin - acidic dye stains basic components of cells; hemoglobin, eosinophil granules
Neutral pH of dye allows for staining of neutrophil granules
DH2O acts as buffer to improve contrast of cellular materials
Contents of the May-Grunwald-Giemsa Stain
May Grunwold contains eosin and methylene blue
Giemsa contains: eosin, purified azure B, methylene blue
Requires phosphate buffer and water at pH 6.8
Use of each stain component in May Grunwald Giemsa
MG - primarily cytoplasmic (does not demonstrate nuclear detail, PTLs, or malaria inclusions)
Giemsa - nuclear stain demonstration inclusions such as malaria, but does not stain RBC or neutrophil granules well
Common supravital stains and their uses
New methylene blue (retics, Heinz bodies)
Brilliant Cresyl Blue (retics, Heinz bodies)
Methyl violet, Crystal violet, Brilliant green = Heinz bodies
Contents of Perl’s priussian blue stain
0.2N HCl, Potassium Ferrocyanide. Also requires methanol and 0.2% aqueous safranin
Perl’s prussian blue staining principle
Slides are fixed in methanol
● Slides are incubated in the HCL and potassium ferrocyanide mixture.
● The HCL splits the ferric iron from hemosiderin
● Ferric ions combine with potassium ferricyanide to form a blue complex
● Only ferric irons are demonstrated – ferritin cannot be demonstrated as it is too small to
be seen with light microscopy)
● Slides are counterstained with aqueous safranin to increase contrast
Use of Perl’s Prussian Blue Stain in Heme
Demonstrates iron stores in BM Particle smears. Results are reported as decreased, normal, or increased.
What conditions cause increased iron stores in BM
Megaloblastic anemia
Hemolytic anemia
Sideroblastic anemia
Anemia of Chronic Disease
Lead Poisoning
Hemosiderosis
What conditions cause decreased iron stores in BM
IDA
Polycythemia vera
Use of MPO Stain
Stains primary granules in monocytes and myeloid lineage
Use of SBB stain
Stains primary and secondary myeloid granule lipids, weakly stains granules in monocytes
Use of PAS stain in Heme
Stains glycogen compounds found in lymphoid lineage
Use of NSE stain
Stains non-specific esterase compounds found in monocytes
Use of Leukocyte Alkaline Phosphatase staining
Can differentiate leukemoid reactions from CML, as leukemoid reaction shows increased staining
Contents and requrements of LAP stain
Contains: naphthol phosphate, Fast red violet salt, fast blue salt
Requires: Acetone, hematoxylin solution for counterstain
What conditions cause increased LAP staining
LAP can be increased in:
Leukemoid reaction
Multiple myeloma
Hodgkin’s disease
Myeloproliferative disorders such as Polycythemia vera (except CML)
Aplastic anemia
What conditions can cause decreased/minimal LAP staining
Chronic myelogenous leukemia (CML)
Paroxysmal nocturnal hemoglobinuria
Sickle cell anemia
Myelodysplastic syndromes
Effect of high pH on Hemeatology staining
increased dissociation of methylene blue = stain is too blue
RBC stain green/blue
Neutrophils appear toxic
Effect of too low pH on Hematology staining
Increased dissociation of eosin causing the stain to be very pink
RBC stain red-orange
WBC nuclei will be pale
Eosin granules are increasingly bright orange
What casues stain precipitate
Inadequate washing, stain drying on slide precipitated stain powder in solution requiring filtration
Effect of water artifact on hematology staining
Causes halos on RBCs (cells appear hypochromic and refractile)
When is a WBC correction performed
When >/= 2 nRBCs are present per 100 WBC in the blood smear
Corrected WBC formula
Automated WBC count / (100+nRBCs) x 100
Use of Miller Ocular Lens in Hemetology
Used for retic counts and malarial parasitemia levels.
Are gametocytes counted as infected RBCs for malaria
No. They are extracellular
How to calculate %parasitemia/%reticulocytes
%parisitemia = (Square B x 100) / Square A x 9)
What can be included in a laboratory evaluation of body fluids
Total volume, gross appearance, total cell count, differential cell count, crystal IDs, biochemical analysis, microbial examination, immunological studies, cytological examination
What evaluation of body fluids do hematology labs perform
Gross examination [appearance (color, clarity) - spun and unspun]
WBC count (TNC) - RBCs only reported if requested
Cytospin differential (if number of TNCs is >200)
What fluids are grouped together and known as serous flouids
CSF, Pleural, Peritoneal, Pericardial Fluids
What are serous fluids
Ultrafiltrates of plasma found in small amounts of the pleural, peritoneal, and pericardial cavities, where they serve as lubricant.
What is a transudate
An accumulation of body fluid caused by a non-inflammatory circulator disturbance. There will be an increase or deacrease in pressure that results in fluid formation
Examples of disorders that result in transudates
CHF (heart can’t pump properly = fluid backup and leakage)
Liver disease (decrease in albumin = decrease in oncotic pressure)
Renal disease (loss of albumin = decrease in oncotic pressure)
Obstructive tumors (poor lymph drainage)
What is an exudate
Excess amount of fluid caused by an inflammatory condition such as infection, malignancy, SLE or rheumatoid arthritis. There is an accumulation of fluid in association with vascular wall damage
What is CSF
An ultrafiltrate of plasma across the blood-brain barrier. Examining CSF is important in conditions such as meningitis, brain hemorrhage, or CNS involvement by leukemia)
What hematology testing is done on CSF
Gross examination of color/cllarity
Cell counts (TNC and RBC)
Cytospin differential (if number of WBC indicates)
What CSF tube is the hematology cell count performed on
The last one, as it has the least amount of cells present from the patient collection
When would a physiican order a CSF cell count on the first tube
When they want to rule our brain hemorrhage - must do cell counts on first and last tibe
Are CSFs older than 2 hours since recieved still worked up?
Yes, but a comment is made about the results.
What happens if there is any macroscopic abnormality in CSF (color or clarity)
A part of sample must be spun down for the spun appearance to determine if xanthochromia is present (orange/yellow color indicating bilirubin from cerebral hemorrhage)
What causes cloudy and colorless bodily fluids
High WBCs, microorganisms
Does the laboratory ever label incorrectly labeled fluid tubes?
No, but we allow the ordering ward to send a witness to label the samples before analysis occurs
Use of ordering crystal identification on synovial fluid
To ID joint fluid for uric acid
Clinical significance of increased reticulocytes in peripheral blood
Increase in RBC production or accelrated erythropoiesis. May be due to:
Hemorrhage
Hemolysis
Hypoxia
Hematinic injury
When must a manual reticulocyte count be done
If the automated reticulocyte count is:
Present with an interference flag
Relative result >30%
Absolute result >90 × 10^9
Use of ESR test (erythrocyte sedimentation rate)
Non-specifc test used as a marker for tissue damage or inflammation. Can be increased by infection, RA, TB, Cancer
Why does ESR increase in multiple myeloma?
In the presence of excess proteins (like immunoglobulins), Zeta potential is decreased, allowing for RBCs to form rouleaux, stack, and fall quicker than normal
Tube requirement for ESR
EDTA
How is ESR testing performed
Blood is aspirated into a ESR westergren tibe and allowed to rest for one hour. Once the RBCs are settled, the distance from the botom of the plasma meniscus to the sedimented RBC is recorded in mm
Effect of abnormally shaped cells on ESR
Decreased (slower settling)
Effect of increased number of RBCs/WBCs on ESR (leukemias, PV)
Decreased (more crowding, thcieker blood)
Effect of anemia on ESR
Increased (less crowding, thinner blood)
Effect of microcytosis and macrocytosis on ESR
Microcytosis: Decreased (light and smaller cells fall slowly)
Macrocytosis: Increased (heavier cells fall quickly)
General effect of Plasma proteins on ESR
Plasma proteins counteract negative charge of RBCs (as they are positive) and increase possibility of Rouleaux formation. Therefore increased levels of fibrinogen, immunoglobulin, and albumin all decrease ESR
Mechanical factors that effect ESR testing
Tilted tube increases ESR (shorter distance to travel)
Cold temps decrease ESR (increased viscovity)
Warm temps increase ESR
Excess EDTA decreases ESR (EDTA causes RBCs to shrink)
Delay in setting up test decreases ESR (shape changes)
Vibration from centrifuge increases ESR
Use of Monospot testing
Red cell or latex agglutination tests that detect heterophile antibodies that the body produces in response to infectious mononucleosis
How does the BioSign Mono Immunoassay test work?
Bovine RBCs are used in a direct solid-phase immunoassay. If heterophile Abs are present in patient blood, they will bind and be captured by an antigen bad (made out of bovine RBCs).
After, a conjugated dye is mobilized to provide visual indication on the presence or absence of the antibodies and a QC line
What does the osmotic fragility test demonstrate
Increased RBC fragility in specimens in which RBCs have decreased SA to Vol ratios (seen in Hereditary Spherocytosis)
How does Osmotic fragility testing work
RBCs are subjected to increasingly hypotonic solutions, so water rushes into the RBCs to equilibrate. Cells with a smaller SA to Vol ratio will lyse more easily, and cells with a larger ratio (target cells) will take up more water without lysing.
How can confirmatory testing for G6PD deficiency be done?
A G6PD kinematic enzymatic assay
How does the G6PD kinematic enzyme assay work?
Patient RBCs are lysed, and the released G6PD will convert glucose-6-phosphate into 6-phosphogluconate, which reduces NADP to NADPH proportionally. The rate of production is measured as the absorbance at 340 nm by a spec

What is a quick screening test for G6PD?
Same kinematic enzymatic G6PD reaction, but the fluorescence of NADPH is measured

How can Pyruvate Kinase levels be tested for PK deficiency?
Quantitative Enzymatic Assay
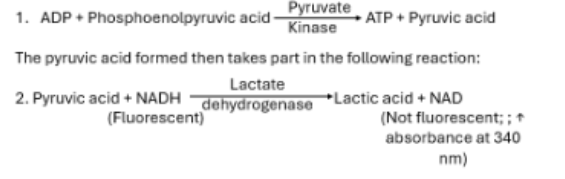
How does the PK Enzymatic assay work
Patient RBCs are lysed and WBCs removed (as WBC’s falsely increase results). Released PK converts phosphoenolpyruvate into pyruvic acid while converting ADP into ATP.
The pyruvic acid reacts with LDH to be converted into Lactic acid, while NAD is converted into NADH. The rate of converseion of NAD to NADH is measured at 340 nm with a spec
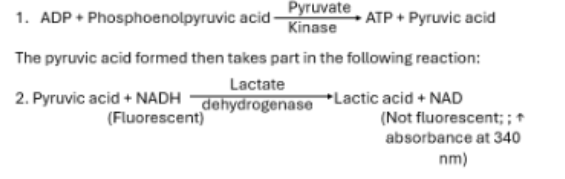
How can a screening test be done for PK deficiency
Same enzymatic test method as the quantitative test, but NADH fluorescence is used to screen
Effect of reticulocytes + transfusion on patient PK levels
Sources of interference when performing a PK assay. Must be noted before performing.