PSYC 100 - Lec 8
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
What is conciousness
Everything we think about right now
Your awareness of your surroundings and yourself
Some believe it to be a stream of conciousness - a continuing flow of changing thoughts
Some scenarious where conciousness is not straightforward
Sleeping
Awake but having a seizure
Asleep but having vivid lucid dreams
What are the 3 levels of conciousness
When we are awale
usually what we think of when think of conciousness
we are awake and aware of whats going on around us
but our degree of our awareness varies a lot
When we are asleep
we are “unconcious” in a menaingful way but still very much alive and sensitive to external stimuli
When we do other things that influence our level of awareness
eg. taking drugs, hypnosis
What is an altered state of conciousness
A change in a persons ability to be fully aware of thier external surroundings and internal states
eg. being sleep, meditation, etc.
Levels of conciousness while we are awake
Concious awareness
Preconsciousness
Unconscious state (not the same as being unconscious in the way someone is when they’re passed out)
Conciousness while awake two components
States of conciousness - level of awareness for our external surroundings and internal states
differentiated by the amount and type of attention we’re able to pay to stimuli
Contents of conciousness - specific thoughts we are aware of about our interal states or external surroundings
Conciousness and attention
We must pay attention and be aware we are paying attention
But attention alone is not conciousness
Inattention blindness
If you aren’t paying attention to something visual, you are unable to report on the details of what the visual stimuli contain
Eg. the gorilla video
Main parts of the brain involved in concious awareness
Reticular formation
Thalamus
Hypothalamus
Cerebral cortex
How is the reticular formation involved in concious awareness
Role in being awake and, therefore, conciousness
Damage results in inability to stay awake; associated with comas
How is the thalamus and hypothalamus involved in concious awareness
An awake brain needs information processed
Signals from reticualr formation go to and through thalamus and hypothalamus
Damage or dysfunction in these pathwyas can result in things like narcolepsy or comas
How is the cerebral cortex involved in concious awareness
Important for the “awareness” aspect of conciousness
**relisten
Blindsight
It illustrates the separate roles of different parts of the brain in “sensing” stimuli and being “aware” of stimuli
Primary visual cortex is destroyed, leading to blindness
But individuals could still point to a spot of light and dodge obstacles
This suggests that parts of the brain are still registering external visual stimuli but the individual is not aware of it
Are babies concious
Your answer to this question depends a bit on how you define conciousness
If conciousness means bening humans, then yes
If conciousness means being awake, then yes
But when we get into metacognitive aspects of conciousness and self-awareness, we notice developmental changes
Development of conciousness
Babies obviously can’t describe their feelings of conciousness but we can tell that they pay atttention to things, hold concepts in mind, and engage in planned behaviours
We can also do tests of self-awareness to see at which point in development they become concious of themselves as distinct from other beings/things
eg. red dot test and them being able to recognize themselves in the mirror
When does concious awareness of self seem to develop? What about full conciousness?
Around 18 months
Around 22 months, as this age is associated with more advanced language use, the ability to reson inductively, and categorize concepts
What is concious awareness of self
Noticing that you are a unique being separate from others
Awake states other than conciousness
Sometimes it is understood in terms of hwo aware we are of things
Preconciousness and unconsciousness, they represent conceptually different levels of awareness
Preconciousness
Level of awareness in which information can become readily available to conciousness if necessary
Its not currently in our awareness but it is accessible
Automatic behaviours
A type of preconcious behaviour
Eg. do you remember every step each time you brushed your teeth last week? no you dont, as it is automatic
Unconcious state
state in which information is not easily accessible to concious awareness
Not the same as being “unconcious”
Analogous to info in long-term memory that we can’t retrieve
Things that guide our behaviour without ever having to rise to a level of conciousness
Implicit memory
knowledge that we have stored in emmory that we are not typically aware of or able to recall at will
the contents of our implicit memory allow is to perform a variety of tasks/skills without thinking deeply about all the individual parts of the task/skill
Evidence for unconcious “awareness”
Eg. riding a bike, “gut reaction” decisions in high-stakes scenarioous.
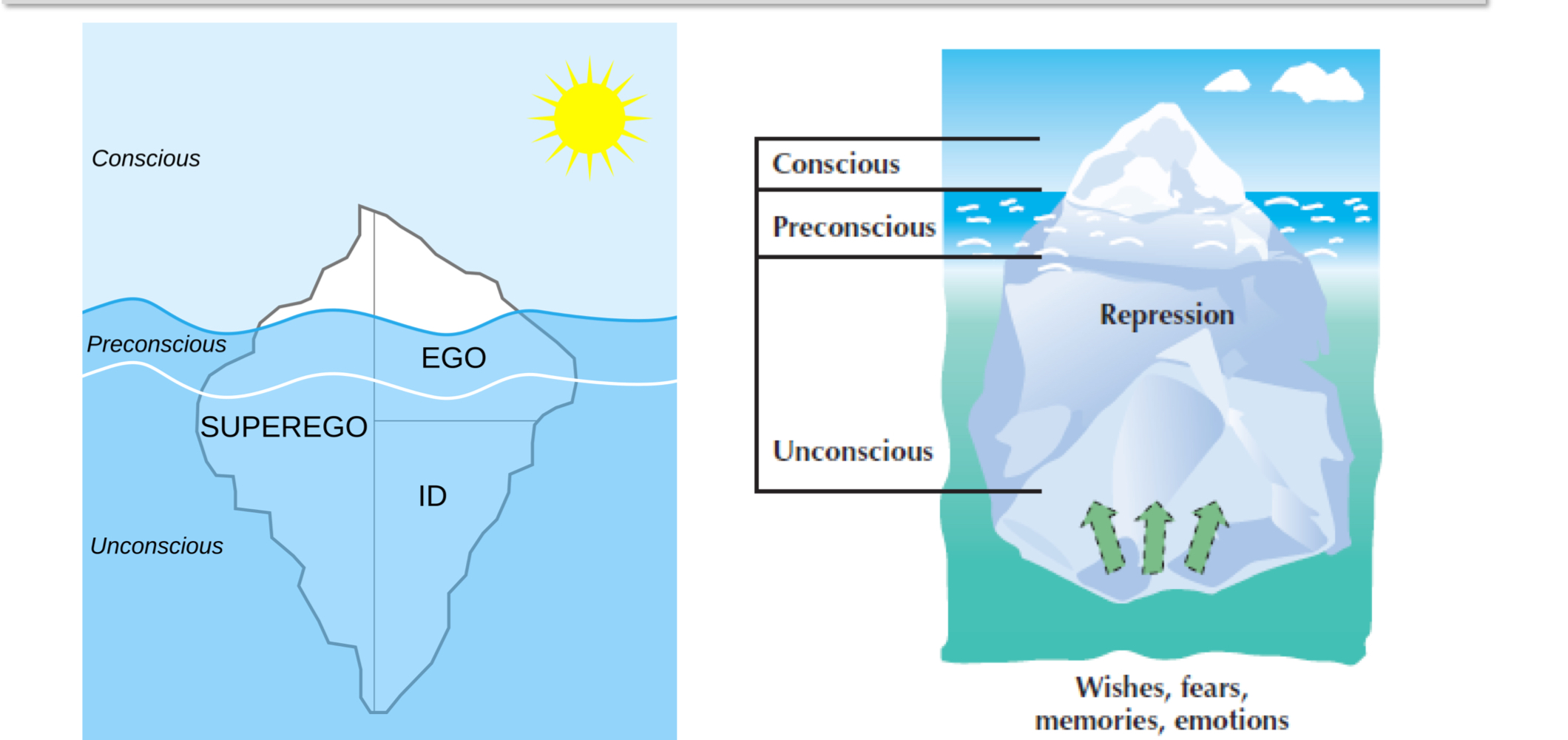
Freuds views of the unconcious
Freud is a major reason we started thinking about the “unconcious” in the first place
Freud imagine a very large role for the unconcious mind
Not only does the unconcious contain a lot of stuff but ti alos gouides our behaviour in a while bunch of ways according to freud
We sleep a lot
Approx. 25 years of sleep over the course of our lives
We can’t avoid it and experience serious negative effects if we try
Humans aren’t even the sleepiest animal
3 theories of sleep
Adaptive theory of sleep
Biological theories
Restoration theory
Adaptive theory of sleep
theory that organisms with bad night vision hide and sleep at night for the purpose of self-preservation, to keep away from predators
Doesn’t fully explain sleep patters in humans
Rooted in evolutionary theory
Biological theories
Sleep plays a role in growth and development
eg. babies sleep a lot of more than adults, something is happening in development
Restoration theory
Holds that sleep restores our brains and bodies; restores depleted resources, claens up “waste” that has accumulated throughout the day
Still does not explain why we sleep
Circadian rhythm
Patter of sleep-wake cycles that in human beings roughly corresponds to periods of daylight and night
We experience changes in alertness and body temperature in predictable ways during sleep/waking
Consistive repetitive pattern of sleep-and-wake
Sleep-wake rhthyms characteristics
Most people don’t have a strong prefrence of time of day for alertness
Although it’s likely that some of you consider yourselves “morning people
or “night owls”
Circadian rhythyms likely primarily determined by genetic factors
Environmental factors are also important
We can adjust our cycles by a few hours without a big consequence
What happens in the brain when we sleep
Sensory signals about daytime/nighttime tell parts of our brain to prep for sleep/waking
eg light of the sun dictates sleep/waking
shows how influential our vision is
Suprachiasmtic nucleus (SCN)
What is the suprachiasmatic nucleus
A small group of neurons in the hypothalamus responsible for coordinating the many rhythms of the body
Directss pineal gland to produce melatonin which triggers sleepiness
**shows how built in it is for our bodies to sleep
How is the circadian rhythm controlled
During the day, photoreceptors in the retina of the eye, send signals to the SCN about daylight, which helps regulate dopamine and melatonin production
This is why artificial lighting has an umpact on our sleep quality
In the total absence of natural light, our SCN may extend our bodys “day” and disrupt our circadian rhythm
We return to. aantural rhythm quickly upon being exposed to nautral light
How can we emasure sleep cycles
Use EEG to measure patterns of brain activity
Different patterns of brain waves denote different stages of sleep
We go through these stages in order and on repeatq
What are the different stages of sleep
Awake and alert
Awake and drowsy, relaxed waves
Stage 1
Stage 2
Stage 3, delta waves appear
Stage 4, mostly delta waves
REM, dreaming
Characteristics of sleep cycles
90 to 100 minutes per sleep cycle
One cycle consists of five stages
Over the altter part of the night, we spend most time in stages 1 and 2 and REM sleep
Pre-sleep period (hypnagogic state)
Alpha waves
Hypnagogic hallucinations
vivid sensory hallucinations
eg. exploding head syndrome
Myoclonic jerk
muscle spasm that accompanies hypnagogic hallucination of falling
Stage 1 of sleep
A few minutes
Bridge between wakefulness and sleep
Alpha waves change to slower theta waves
Stage 2 of sleep
15 to 20 minutes
More relaxed
Rhythmic breathing
sleep spindles (burst of rapid rbainw aves)
Stage 3 of sleep
Deep sleep
20-50% delta waves
Stage of 4 of sleep
Heart rate, bnlood pressure, breathing rates at lowest levels
Muscles relax
Sleepwalking more likely
Stage 5 of sleep
Rapid eye movement (REM) sleep
Most associated w/ dreams
REM sleep
associated with rapid and jagged brain wave patterns, increased HR, rapid and irregular breathing, rapid eye movements, and dreaming
Can look at brain images to see brain activitiy while sleeping
What are dreams
Extra brain activitiy while asleep
Why do we have them and what do they represent though?
Informaiton processing theory of dreaming
Dreams involve processing info from the day (i.e encoding memory and problem solving ), could be related to restoration theory
Dreams could be a mental realm where we can solve problems and think creatively
Activation - synthesis model of dreaming
During sleep, that brain has a lot fo random activitiy via brainstem activitiy that activates the sensory systems of the cortex
Dreams could reflex the brains efforts to make sense out of or find meaning in the neural activitiy that takes palce during sleep
Freudian dream theory
Dreams represent the expression of unconcious wishes or desires
Not much evidence for this
4 notable types of dreams
Nightmares - dreams filled with intense anxiety
Nightmare or dream disorder anxiety - frequent or distressing nightmares, could warrant intervention
Lucid dreams - the sleeper fully recognizes that she is dreaming and occassionally actively guides the otucome fo the dream
Day dreams - fantasies that occur while one is awake and aware of external reality, but is not fully concious
Sleep and age
Babies spend more time in REM sleep
Seen as evidence that this is part of how young brains develop (important role of sleep)
Sleep requirements change as we age, as youo age things are not working in our body that can interfere w/ our sleep
Sleep deprivation
If we could sleep as long as we wanted most people would sleep 9-10 hours, but we do not always get this
Chronic sleep loss results in:
general depressed state
lower immune system
lower ability to concentrate
higher incidence of accidents
lower productivity and higher likelihood of making mistakes
Sleep hygiene
Practices and routnines to help sleep better:
Make your bedroom a place yoou associate most strongly with sleep
keep it dark, quiet, and cool
don’t have devices or screens in your room
uses process of classical conditioning, prepares the brain for sleep when in the room
Limit eating/drinking within 3 hours of bedtime
especially alcohol and caffeines, i.e giving your body/brain less to day
Limit naps and physical activitiy late in the day if you’re having trouble sleeping
Insomnia
Most common sleep disorder
Difficulty going to sleep or staying asleep
Caused by stress, therefore common treatment is CBT
More common in older people due to medical conditions, pain, medications, and depression
and anxiety
Sleep apnea
Second most common sleep disorder
Repeatedly stops breahting during the night leading to frequent awakenings, no recall of waking though
Possible to have hundreds of attacks per night
Can lead to cardiac arrest
People who snore are more prone
Airway blocked temporarily
Use CPAP machine
Excessive daytime sleepiness
Chronically tired, even if slept well
Narcolepsy
Uncontrollable urge to fall asleep
Suddently fall into REM sleep during the day
Can last up to 15 minutes
Genetic factors involved
No cure
Can lead to serious injury or death
Delayed sleep phase syndrome
Long delay in ability to fall asleep
Advanced sleep phase syndrome
Fall asleep between 6 ppm and 9 pm and wake ebtween 2 am and 5 am
Has to do with how body responds to wake signals
Restless leg syndrome
Strong urge to mvoe elgs before sleep, prevents sleep
Periodic limb movements of sleep
Strong urge to move legs during sleep, disrupt sleep
Sleepwalking
Mostly occurs during first 3 hours of sleep
Eventtually returns to bed
Inherited
Doesn’t ahppent aht frequently
Some people need to get help for it
Night terrors
Occurs ins tage 3 and 4 of sleep
Child screams in panic; goes back to sleep immediately and does not rememebr the event in the morning
Resolves by adolescnece
may be genetic
Very serious
REM sleep behaviour disorder
Acting out the dream while in bed and sleeping
Altered conciousness AKA
how we try to change what we’re aware of
Things we do delibertely
Hypnosis
Altered state of conciousness, with heightenied suggestibility, deep relaxation, and intense focus
Post hypnotic responses
Posthypnotic amnesia
Hypontic hallucinations
Decreased activitiy in aterior cingulate cortex when used to reduce pain
Two possible mechanisms for how hypnosis helps with pain relief
Divided conciousness theory: hypnosis splits awareness into two parts; one part responds to hypnotists suggestion, the other part continues to process pain information but at a less concious level
Social/cognitive process theory: the participant is hgihly motivated to believe in hypnosis, and, without awareness, works hard ot ignore the pain. less about hypnosis working, and more believing that it will work
What does neuroimaging techniques suggest for how hypnosis works
Suggests that the brains anterior cingulate cortex may be particularly involved when hypnosis is used to anaesthetize or reduce pain
Psychoactive drugs
Chemicals that affect awareness, beahviour, sensation, perception, or mood
Additction
Large concern
a psychological cimpulsion to take a drug, resulting from regular ingestion and leading to maladaptive patterns of behaviours and changes in physical response
Tolerance to drugs
mark of physical dependence on a drug, in which the person is required to take incrementally largfer doses of the drug to achieve the same effect
Withdrawal symptoms
Unpleasant and sometimes dangerous side effects of reducing intake of a drug after a person has become addicted
Negative reinforcement: taking the drug again to stop withdrawal
Depressants
Slow the activity of the central nervous system, reducing tension and inhibitions
Include alcohol and sedative-hypnotic drugs, and opiods
Can interfere with judgement, motor activtiy, and concentration
Sedative-hypnotics
Benzodiazepines
Produces relaxation and drowsiness; releives anciety
Eg. Xana, Ativan, Valium
Opiods
Derived frpm the sap of the opium poppy
Include opiod heroin, morphine, codeine, and OcyContin
Activate the opiod receptrors in the rbain, providing their analgesic effect and their related high
Reduce pain and emotional tension and produces pelasurable and calming feelings
Very affective
Some of the most addictive, through psoitive reinforcements (i.e producing pleasurable feelings)
Stimulants
Increases the activitiy of the central nervous system
Include, caffeine, nicotine, cocaine, amphetamines
Cocaine
Increases energy and alertness
Produces euphoric feelings of well-being (positive reinforcement)
Negatively imapcts memory, attention,a nd decision-making ability
Amphetamines
Small doses increase energy and alertness and reduce appetitie, very reinforcing
Large doses produces intozication and psychosis
Increases metahmphetamines (crystal emth) and MDMA (ecstacy), Adderal, etc.
Hallucinogens
Produce sneosry or perceptual distortions called hallucinations
LSD
Magic mushrooms
Mescaline (Buttons, mesc)
DMT
Ketamine
PCP
Cannabis
LSD
Dramatically strengthens visual perceptions (including illusions and hallucniations) along with profound psychological and physical changes
Depends on the dose
Some people have positive and some people have negative experiences
Cannabis
Marijauna, THC
Produes a mixture of hallucinogenic, depressant, and stimulant effects
Depends on formulation and dosage
Psychoactive drugs activate which pathway
The reward learning pathway or “pleasure pathway” in the brain
As brain is designed to respond to rewards => keep using the drugs
Reward-deficiency syndrome
People might abuse drugs because their reward centre is not readily activated by usual life events