Gender-Affirming Hormone Therapy; Obesity; Obstructive Sleep Apnea
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
What does gender identity refer to?
- A person's internal sense of gender
- Example: Man, woman, non-binary, agender, genderfluid
What does gender expression refer to?
- How a person presents themselves (e.g., clothing, hairstyle)
- Example: Masculine, feminine, androgynous
What does anatomical sex refer to?
Biological traits assigned at birth (e.g., chromosomes, hormones, reproductive anatomy)
What does sexual attraction refer to?
- Who a patient is drawn to
- Example: Heterosexual, homosexual, bisexual, asexual
How does gender-affirming behavior impact the physical and mental wellbeing of patients?
Respectful use of a patient’s preferred name and pronouns…
- Allows transgender and non-binary patients feel respected and affirmed
- Increases likelihood patients will seek care (not just gender-affirming care)
- Increases adherence to treatment plans for healthcare
- Increases open communication with healthcare provider team
Affirmative behavior is associated with improved mental health outcomes
What are non-pharmacologic therapy options for gender-affirming care?
Mental healthcare
- Psychological and behavioral support
Social transition
- Changing name/pronouns
- Dressing/grooming in a way that aligns with gender identity
- Voice training (for a more feminine or masculine vocal tone)
Harm reduction – intentional practices and policies designed to lessen negative social of physical consequences associated with human behavior
- Safer sex support (e.g., education, access to condoms)
- Syringe exchange services
- Substance use treatment (e.g., naloxone, fentanyl test strips)
- Shelter and other needs
Surgical options
- “Top” (chest) surgery
- “Bottom” (genital) surgery
According to WPATH Standards of Care, what criteria must be met to initiate hormone therapy?
- Persistent, well-documented gender dysphoria (≥ 6 months)
- Capacity to make a fully informed decision and to consent to treatment (and has consented to treatment)
- If significant medical or mental health concerns are present, they must be reasonably well controlled
- Patient must be informed of all effects and side effects of treatment (including those that are irreversible and those that affect fertility)
What pharmacologic agents are used in feminizing hormonal therapy?
- Estrogen (estradiol)
- Androgen blockers
- Progestins (not recommended)
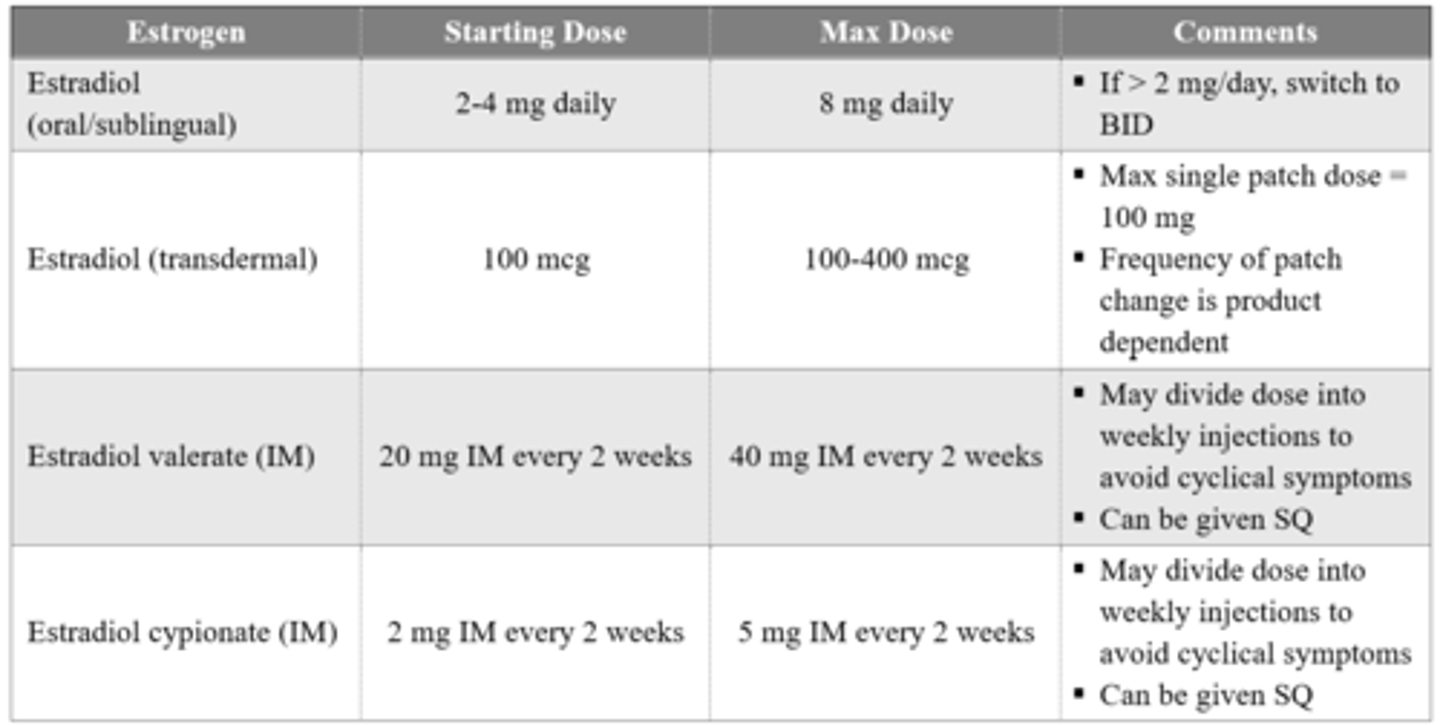
What estrogen products are used in feminizing hormonal therapy? Describe clinical pearls associated with its use.
Avoid ethinyl estradiol and conjugated estrogens
- Increased VTE risk
- Conjugated estrogens cannot be effectively monitored
Transdermal estrogen recommended for patients age > 45
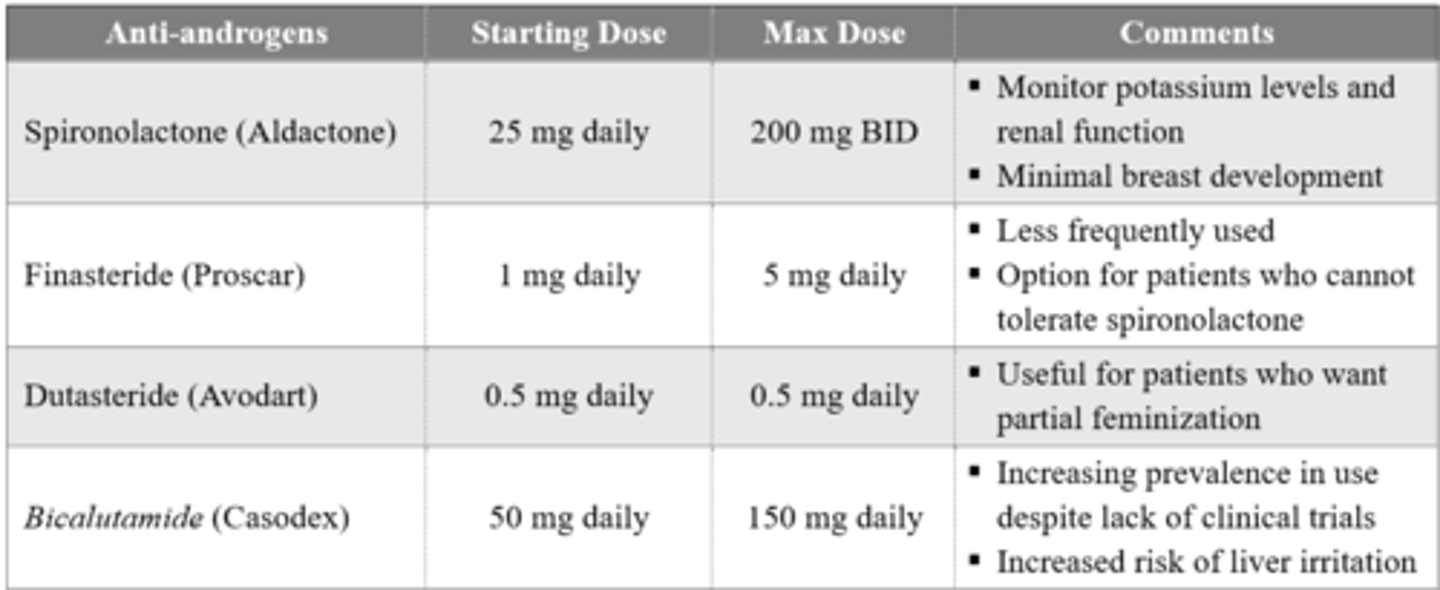
What androgen blockers are used in feminizing hormonal therapy?
Evidence regarding which androgen blocker to use is unclear
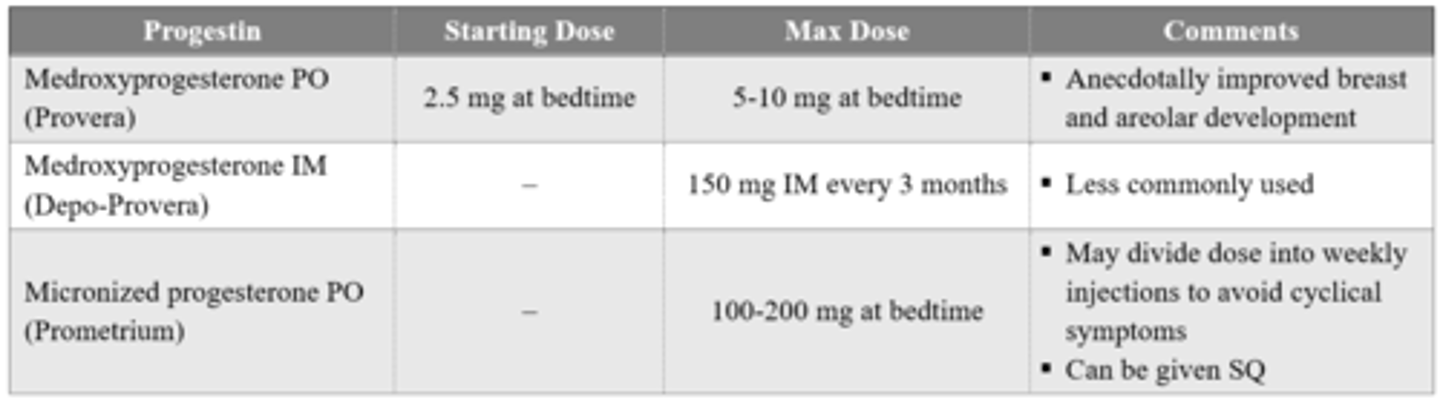
Are progestins recommended for use in feminizing hormonal therapy?
Not recommended by WPATH 2022 guidelines
- Benefits have not been clearly shown in clinical trials
- Risks include weight gain, depression, lipid changes, and rare meningiomas
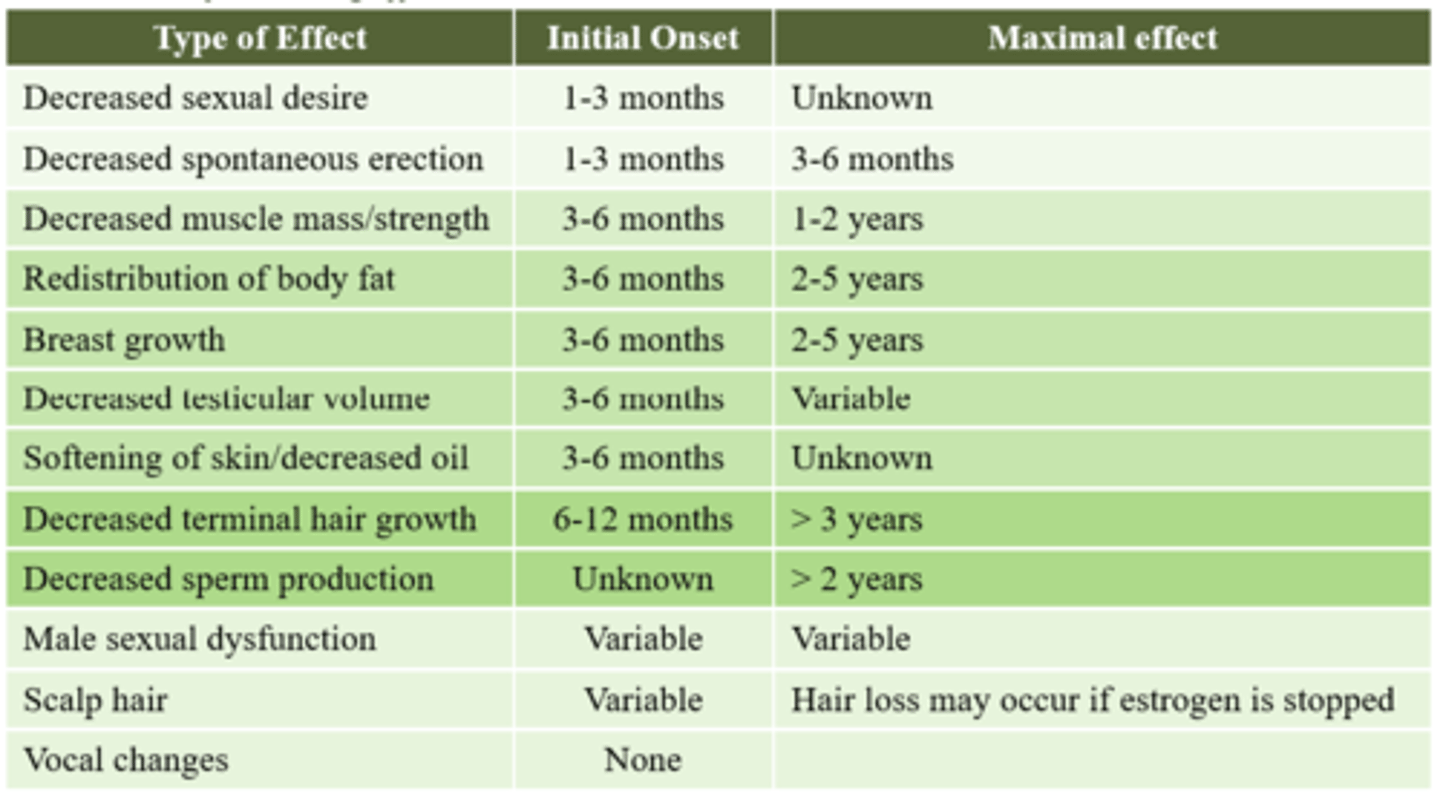
After initiating feminizing hormonal therapy, how long will it take for a patient to start experiencing different feminizing effects?
What baseline monitoring should be conducted prior to initiating feminizing hormonal therapy?
- Kidney function
- Bone mineral density
- Lipid profile
- Fasting glucose
- Liver irritation (AST/ALT)
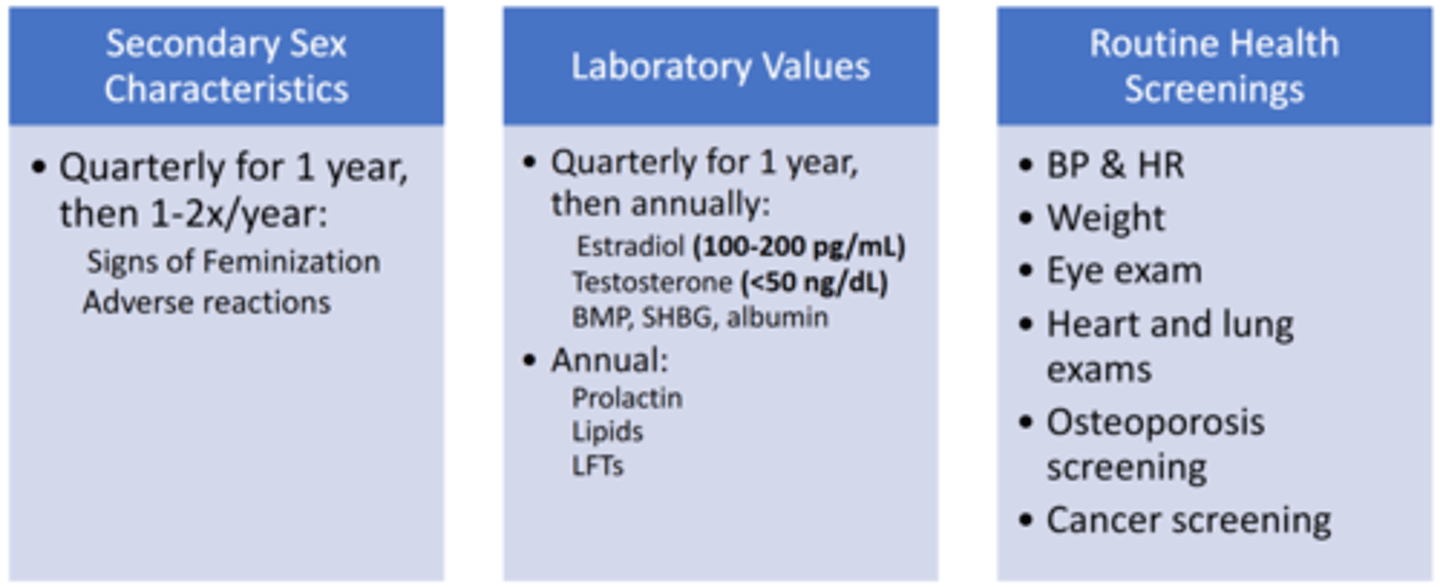
What ongoing monitoring parameters should be evaluated after initiating feminizing hormonal therapy?
What pharmacologic agents are used in masculinizing hormonal therapy?
Testosterone
Progesterone therapy can be used to suppress menses in addition to testosterone
- Can improve feelings of dysphoria
- Contraceptive of choose in this population
- Drug/dosing is indication-dependent
May also consider GnRH analogs (leuprolide) to suppress menses
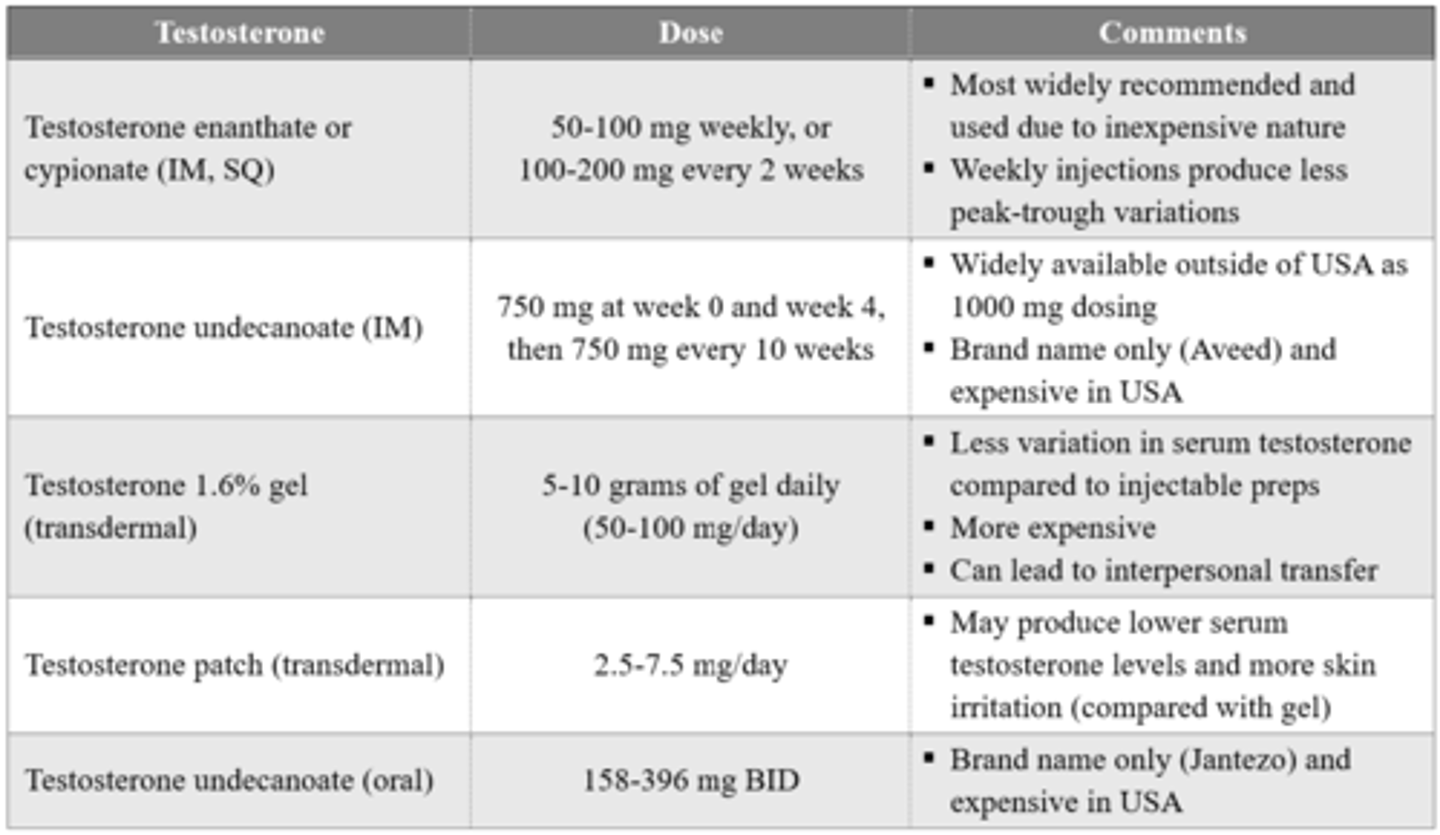
What testosterone products are used in masculinizing hormonal therapy?
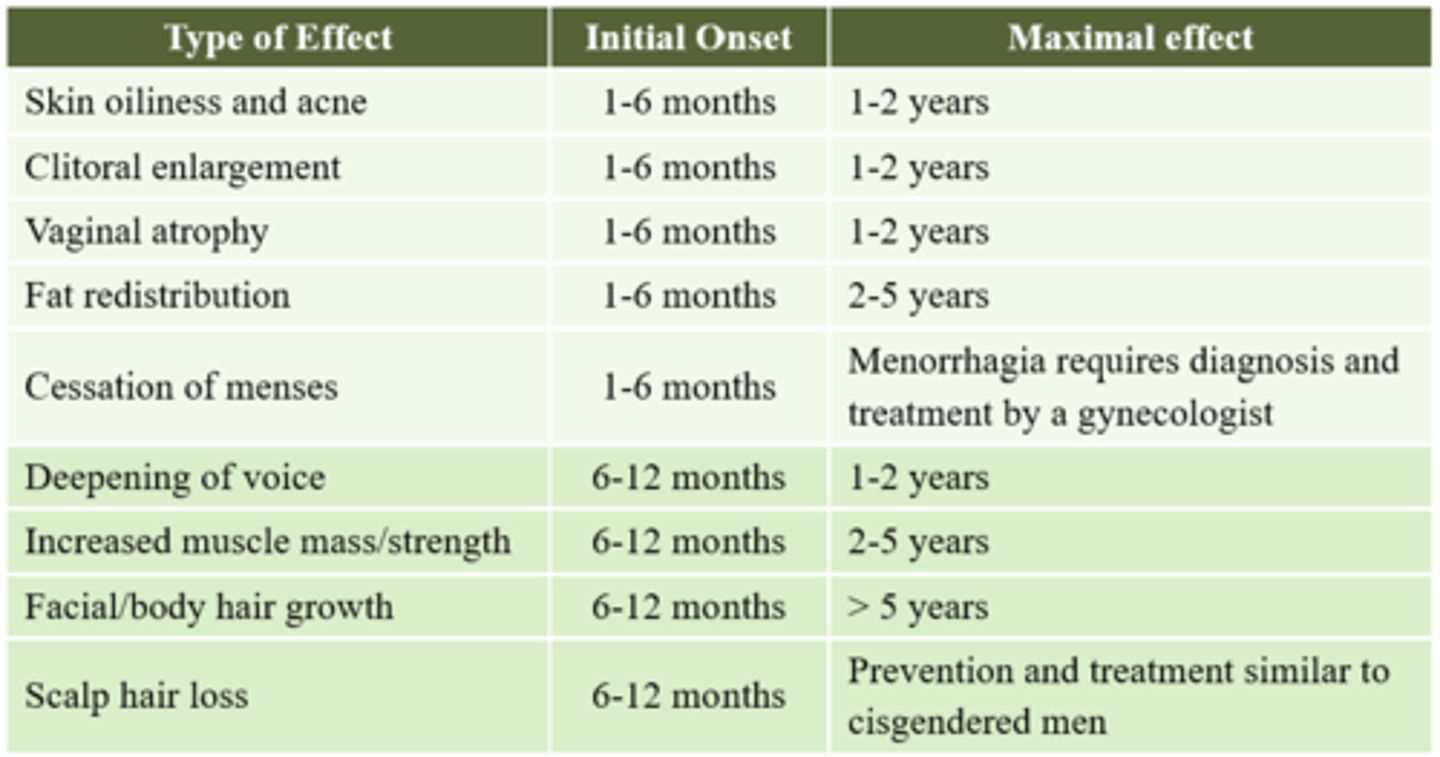
After initiating masculinizing hormonal therapy, how long will it take for a patient to start experiencing different masculinizing effects?
What baseline monitoring should be conducted prior to initiating masculinizing hormonal therapy?
- CBC, Hgb, Hct
- Lipid profile
- Fasting glucose
- Liver irritation (AST/ALT)
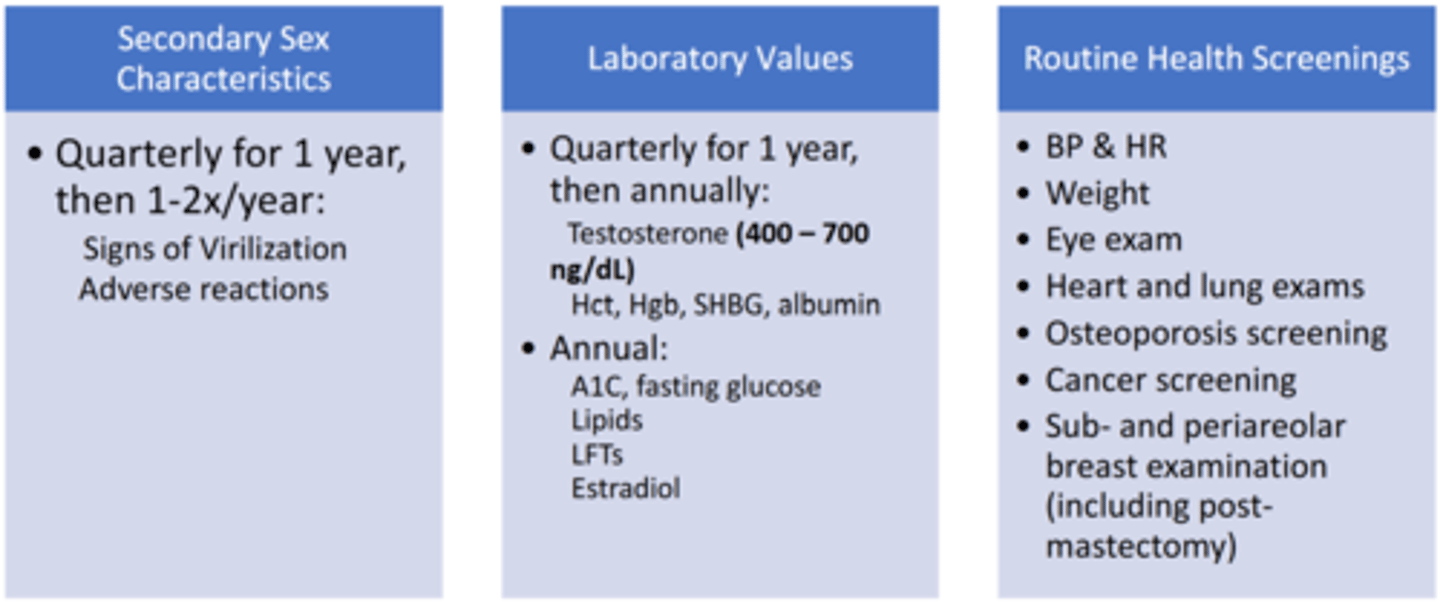
What ongoing monitoring parameters should be evaluated after initiating masculinizing hormonal therapy?
Describe the neurohormonal regulation of hunger/satiety.
Orexigenic (appetite-stimulating) pathways:
- Ghrelin: Appetite-stimulating hormone secreted by stomach
- Agouti-related peptide (AgRP) and neuropeptide Y (NPY): Inhibited by leptin
Anorexigenic (appetite-suppressing) pathways:
- Leptin: Satiety-promoting hormone produced by adipose tissue
- Pro-opiomelanocortin (POMC): Stimulated by leptin
Biogenic amines:
- Serotonin (5-HT): Key regulator of sleep cycle, mood, and satiety (activation of 5-HT receptors promotes satiety and decreases food consumption)
- Dopamine (DA): Central to motivation, reward, and reinforcement system
- Norepinephrine: Regulates sleep cycle, attention, and feeding behavior
What are risk factors for obesity?
Genetics
- Play a strong role in determining both obesity and distribution of body fat
Environmental/behavioral factors
- Dietary factors (e.g., availability/affordability/cost of healthy food, increased portion sizes)
- Reduced physical activity
- Sedentary behavior
- Socioeconomic status
- Religious and culture factors
Medications
Medical conditions
What are examples of medications that are obesogenic?
- Anticonvulsants (e.g., carbamazepine, gabapentin, pregabalin, valproic acid)
- Antidepressants (e.g., mirtazapine, TCAs)
- Atypical antipsychotics (e.g., olanzapine, quetiapine, risperidone)
- Conventional antipsychotics (e.g. haloperidol)
- Hormonal (e.g., corticosteroids, insulin, medroxyprogesterone)
- β-blockers
- Anti-diabetic agents (e.g., sulfonylureas, TZDs, insulin)
What medical conditions increase the risk of obesity?
Endocrine:
- Cushing’s syndrome
- Hypothyroidism
- Monogenic disorders (e.g., MC4R mutation, leptin or POMC deficiency)
Psychiatric:
- Depression
- Eating disorders
- Schizophrenia
Neurological:
- Prader-Willi syndrome – genetic disorder that causes an insatiable appetite and severe obesity
- Neurological injury (e.g., hypothalamic obesity)
What are benefits of weight loss in individuals with obesity?
Weight loss of 3-5% can result in clinically significant reductions in…
- Triglycerides
- Blood glucose, HbA1C
- Risk of developing diabetes
Further weight reduction will…
- Reduce blood pressure
- Improve LDL-C and HDL-C
- Reduce the need for medications
- Further reduce TGs and blood glucose
What are two diagnostic markers for obesity? Which is preferred?
Body mass index (BMI)
- Preferred marker for guiding therapy
- Increased BMI increases the risk of CVD, T2DM, and all-cause mortality
Waist circumference
- Central obesity predisposes individuals to developing CVD, T2DM, HTN, HLD, etc.
- Measure the most narrow circumference between the last rib and the top of the iliac crest
- Patients at high metabolic risk: >40 inches (men) and >35 inches (women)
What are non-pharmacologic therapy options for obesity management?
Reduced calorie intake: Implement evidence-based diets to create 500-750 kcal/day energy deficit
- Women: 1200-1500 kcal/day
- Men: 1500-1800 kcal/day
Increased physical activity
- All obese patients should receive a medical examination before beginning physical activity program
- Engage in moderate-intensity physical activity for 200-300 minutes/week
- When combined with reduced calorie intake and behavior modifications, increased physical activity can augment weight loss and improve comorbidities and cardiovascular risk factors
Behavioral modifications
- Help patients choose lifestyles that are conducive to safe and sustained weight loss
- Make realistic, patient-specific goals
- Avoid changing multiple behaviors at once
- Referral to support group or counseling service
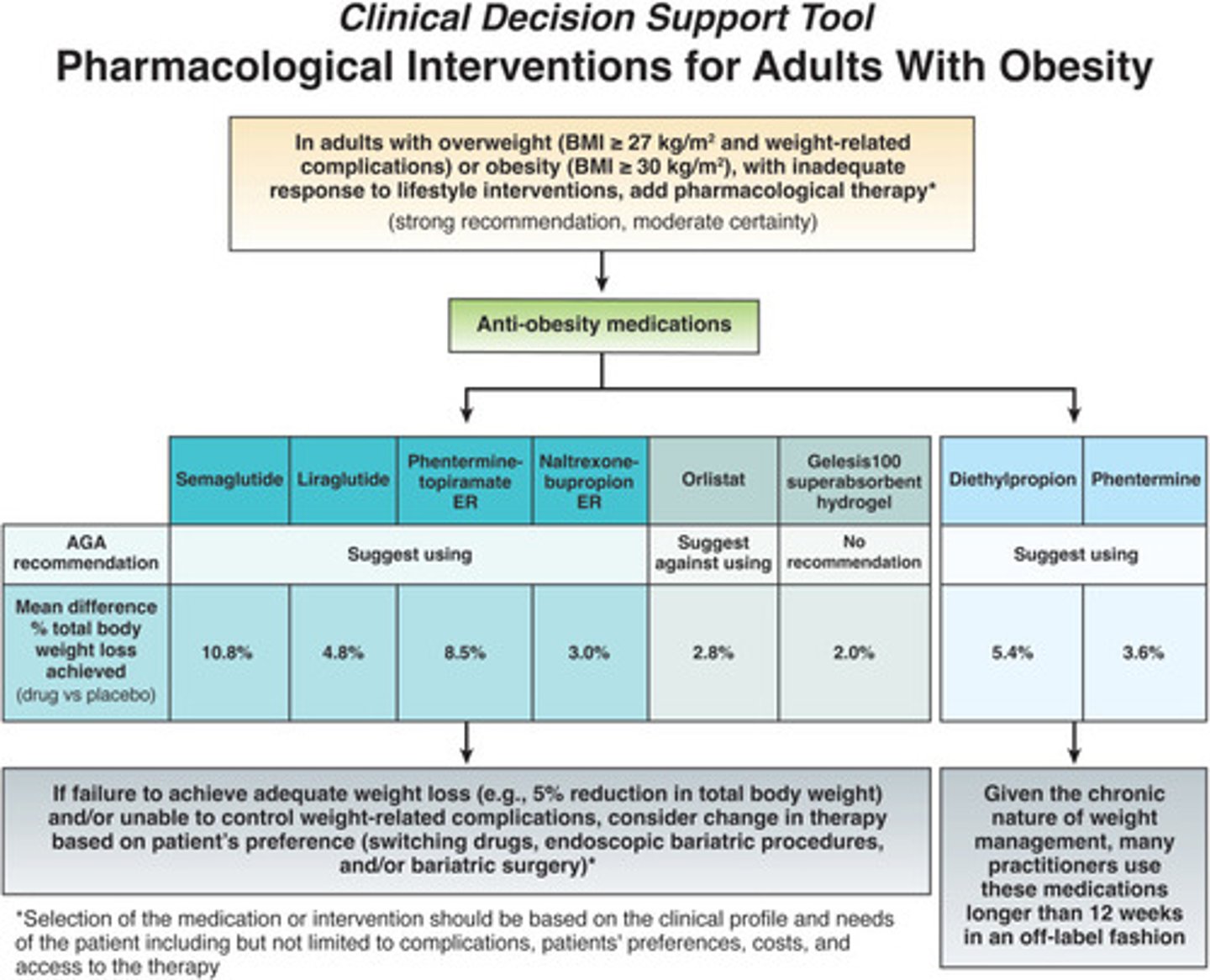
What are the BMI thresholds for initiating anti-obesity pharmacologic treatment?
Adults with BMI ≥ 30 kg/m2
Adults with BMI 27-30 kg/m2 with ≥1 comorbid risk factor
Exception: OTC orlistat (Alli) is indicated for adults with BMI ≥ 25 kg/m2
Per 2022 AGA guidelines, what pharmacologic agents are recommended in the treatment of obese/overweight adult with weight-related complications who have an inadequate response to lifestyle changes?
- GLP-1RAs (e.g., semaglutide, liraglutide)
- Phentermine-topiramate (Qsymia)
- Naltrexone-bupropion (Contrave)
- Phentermine (Adipex-P, Lomaira)
- Diethylpropion (Tenuate)
What are examples (brand and generic) of sympathomimetic amines that are used in obesity management?
Phentermine (Adipex-P, Lomaira): C-IV
Diethylpropion (Tenuate): C-IV
Benzphentamine (Regimex): C-III
Phendimetrazine (Bontril): C-III
What is the MOA for phentermine?
- Sympathomimetic amine
- Stimulates norepinephrine release
What adverse effects may occur with phentermine?
CV: HTN, tachycardia, palpitations
NS: Insomnia, headache, euphoria, tremor
Derm: Urticaria
GI: Constipation, diarrhea, xerostomia
GU: Impotence
What are contraindications for the use of phentermine?
- Hypersensitivity to phentermine
- History of cardiovascular disease
- Hyperthyroidism
- Glaucoma
- Use in agitated states
- History of drug abuse
- Pregnancy/lactation
- Concurrent MAOI use
What is the MOA for phentermine/topiramate (Qsymia)?
Sympathomimetic amine/anticonvulsant
- Phentermine: Stimulates norepinephrine release
- Topiramate: Suppresses appetite and enhances satiety
What adverse effects may occur with phentermine/topiramate (Qsymia)?
CV: Tachycardia
NS: Paresthesia, dizziness, insomnia, seizures (if stopped abruptly)
GI: Constipation, xerostomia
What are contraindications for the use of phentermine/topiramate (Qsymia)?
- Hyperthyroidism
- Glaucoma
- Pregnancy
- Concurrent MAOI use
What are some additional counseling points for phentermine/topiramate (Qsymia)?
Dose increases/decreases require titration
Qsymia is a REMS medication (due to teratogenic effects)
- Increased risk of congenital malformation
- Need to discontinue
What is the MOA for bupropion/naltrexone (Contrave)?
Not fully understood (plays a part in appetite regulation)
Bupropion:
- Weak inhibitor of dopamine and norepinephrine reuptake
- Increases satiety via POMC pathway
Naltrexone:
- Opioid antagonist
- Helps sustain weight-loss effects of bupropion
What adverse effects may occur with bupropion/naltrexone (Contrave)?
GI: N/V/D, constipation, xerostomia
NS: Headache, dizziness, insomnia
Boxed warning: Suicidal thoughts/behaviors, neuropsychiatric reactions
Unknown effects on cardiovascular morbidity and mortality
What are contraindications for the use of bupropion/naltrexone (Contrave)?
- Concurrent use of other bupropion-containing products
- Chronic opioid therapy
- Uncontrolled HTN
- Seizure disorder
- Bulimia/anorexia
- Concurrent MAOI use
- Pregnancy (Category X)
What are some additional counseling points for bupropion/naltrexone (Contrave)?
- Dose increases/decreases require titration
- Do not cut, chew, or crush
- May take with or without food, but avoid taking with high-fat meals
What are examples (brand and generic) of GLP-1 receptor agonists (GLP-1RAs) that are used in obesity management?
GLP-1RA:
- Semaglutide (Wegovy)
- Liraglutide (Saxenda)
Dual GIP/GLP-1RA:
- Tirzepatide (Zepbound)
What is the MOA for GLP-1RAs?
- Slow gastric emptying
- Increase satiety (i.e., reduces food intake)
What adverse effects may occur with GLP-1RAs?
GI: N/V/D, constipation
CV: Tachycardia, palpitations
Hypoglycemia
NS: Fatigue, dizziness, headache
Injection site reactions
What are contraindications for the use of GLP-1RAs?
- Serious hypersensitivity reaction (e.g., angioedema)
- PMH/FH of medullary thyroid carcinoma (black box warning)
- Thyroid cancer
- Multiple endocrine neoplasia syndrome type 2 (MEN 2)
- Pregnancy
What are some additional counseling points for GLP-1RAs used in obesity management?
- Dosing requires titration
- Inject SQ in upper arm, thigh, or abdomen (do not use IV or IM)
What is orlistat (Xenical, Alli) indicated for?
Xenical (Rx only): Adults and adolescent age > 12 years with...
- BMI ≥ 30 kg/m2
- BMI 27-30 kg/m2 with ≥ 1 risk factor
Alli (OTC): Adults with BMI ≥ 25 kg/m2 when used as an adjunct to reduced-calorie, low-fat diet
What is the MOA for orlistat (Xenical, Alli)?
Gastrointestinal lipase inhibitor
- Reversibly inhibits gastric and pancreatic lipases
- Inhibits absorption of dietary fats by 30%
What adverse effects may occur with orlistat (Xenical, Alli)?
- Abdominal pain
- Bowel urgency
- Oily rectal leakage
- Steatorrhea
- Nausea
What are some additional counseling points for orlistat (Xenical, Alli)?
- Rx only dosing is 2x the OTC dose
- Take within 1 hour of a fat-containing meal
- Omit dose if a meal is not eaten
- Separate multivitamins ≥ 2 hours before or after administration
- Side effects should decrease after a few months
What anti-obesity pharmacologic agents are indicated for children/adolescents?
When is bariatric surgery indicated?
Generally the last line treatment option for obesity
Recommended for patients with:
- BMI ≥ 40 kg/m2
- BMI ≥ 35 kg/m2 with obesity related comorbidities
What are the two main surgical mechanisms used in bariatric surgery?
Restriction
- Limits caloric intaking by reducing stomach’s reservoir capacity
- Results in more gradual weight loss
- Absorptive function of small intestine remains intact
Malabsorption
- Decreases absorption of nutrients by rerouting the digestive track
- Shortens length of small intestine
- Significant metabolic complications are possible (e.g., protein calorie malnutrition, micronutrient deficiencies)
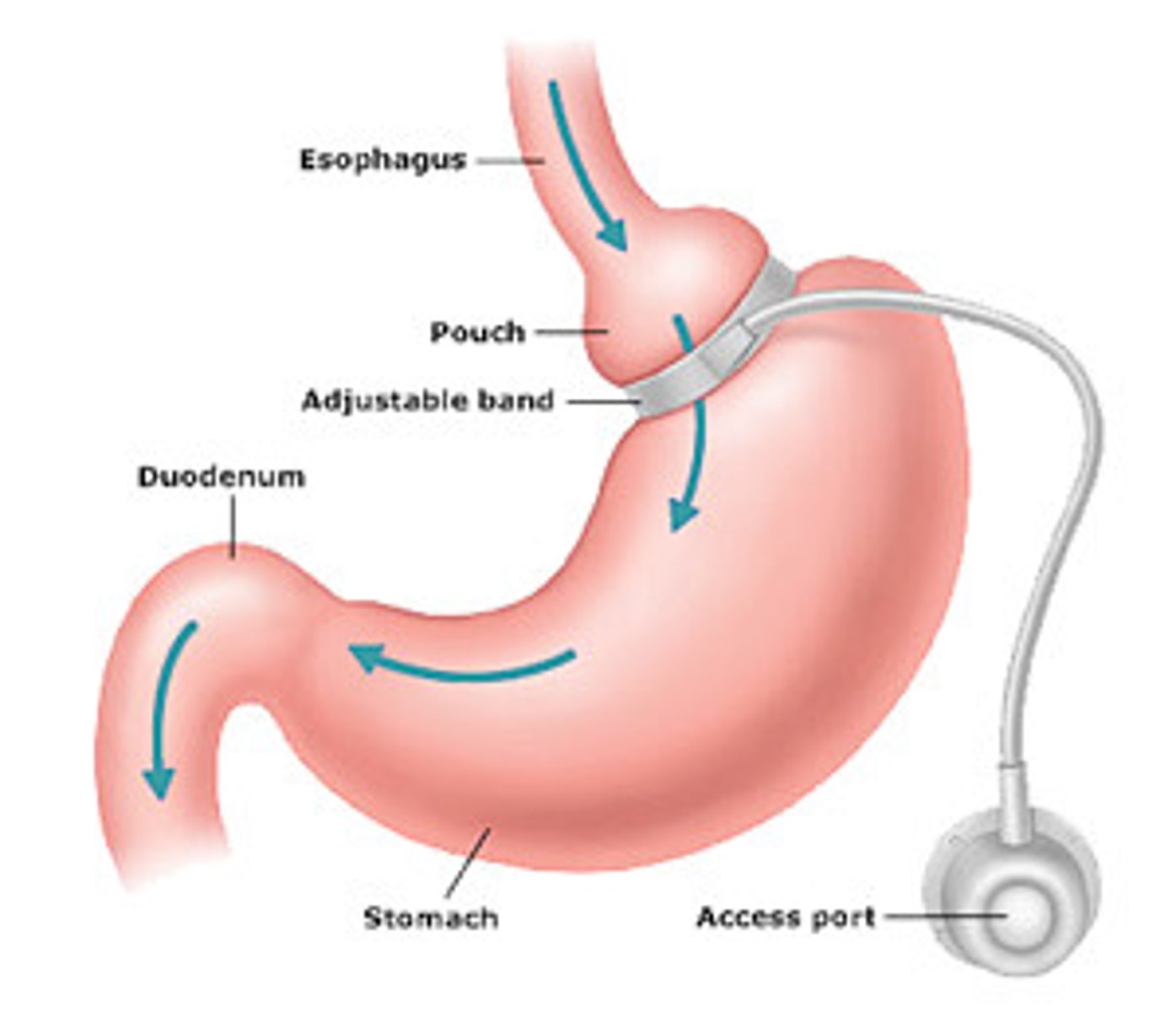
Describe adjustable gastric banding (GB). What surgical mechanism is used?
- Mechanism = restriction
- Reversible
- Least invasive, but also least effective
- Major complications less common
Describe sleeve gastrectomy (SG). What surgical mechanism is used?
- Mechanism = restriction and gastric hormonal changes (i.e., decreased ghrelin)
- Irreversible
- Minimally invasive
- More effective than GB method
- Limited malabsorption side effects

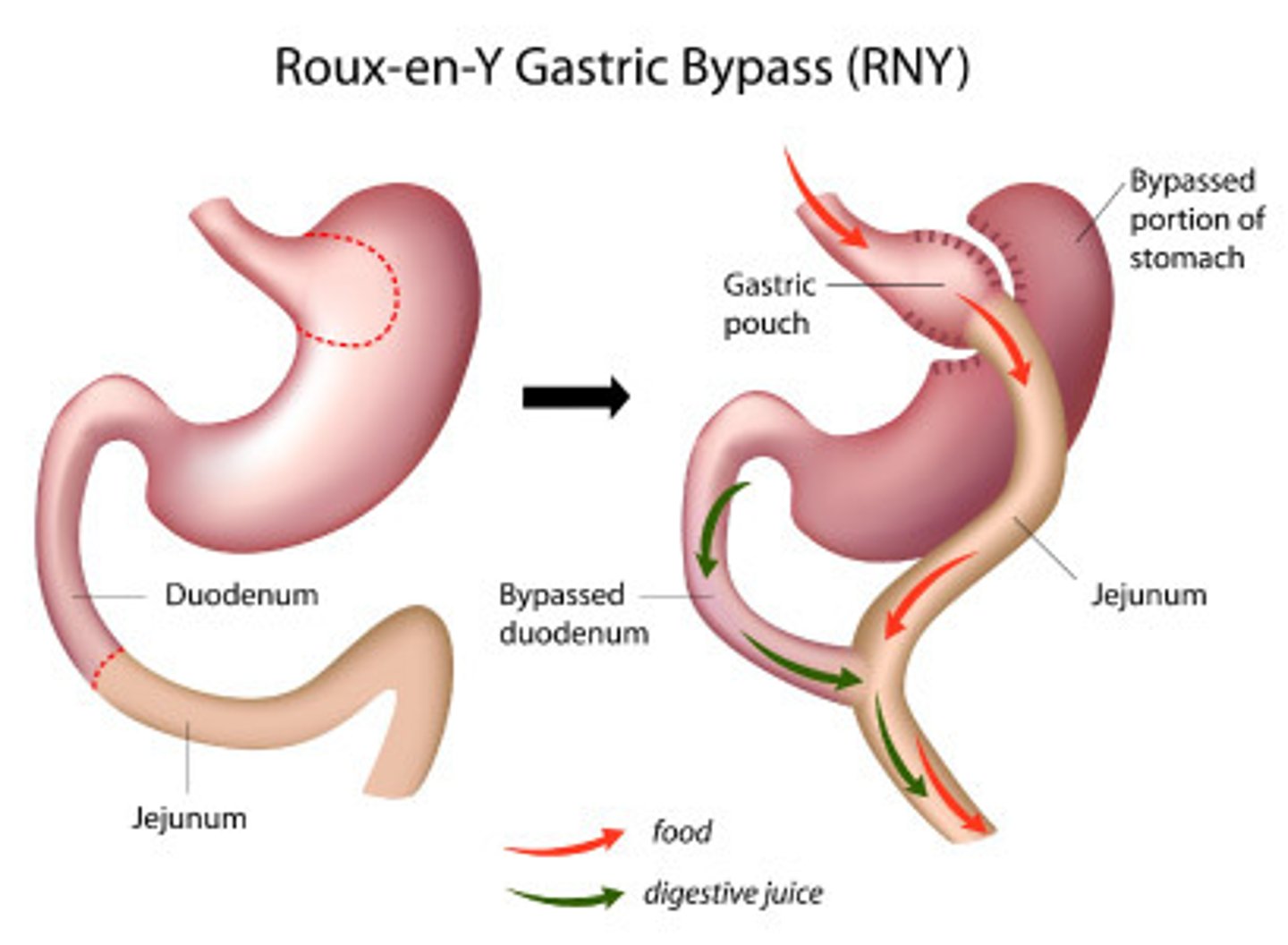
Describe Roux-en-Y bypass (RYBG). What surgical mechanism is used?
- Mechanism = restriction and malabsorption
- Irreversible
- More invasive
- Comparable efficacy to SG
- More major complications
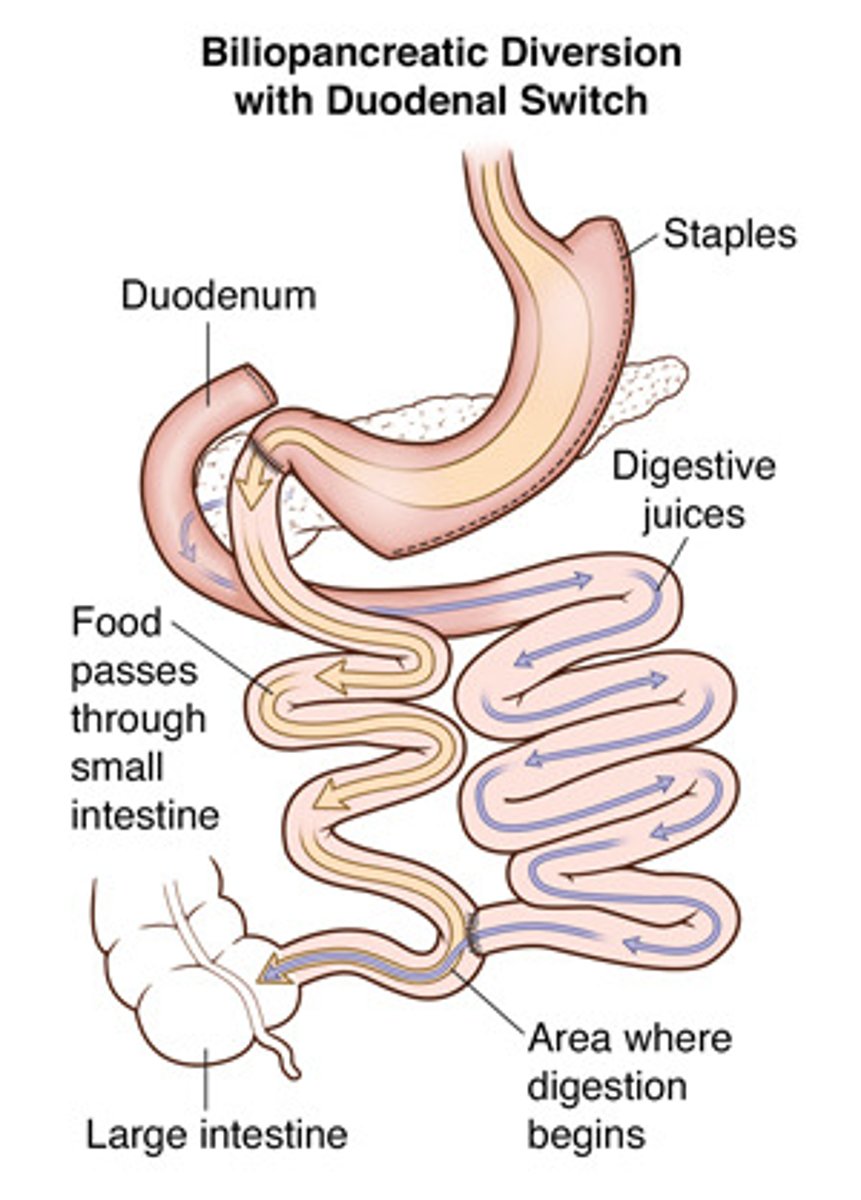
Describe biliopancreatic diversion with duodenal switch (BPD/DS). What surgical mechanism is used?
- Mechanism = restriction, malabsorption, and gastric hormonal changes
- Irreversible
- More invasive
- Slightly more effective than RYBG method, but more complications
What complications may occur as a result of bariatric surgery?
- Bleeding
- Nutritional deficiencies
- Post-operational dilation of bypassed stomach
- Peritonitis
- Dumping syndrome
What vitamin supplementation is required after bariatric surgery?
- Multivitamin with minerals
- Calcium citrate
- Vitamin D3
- Vitamin B12
- Vitamin A (BPD/DS only)
- Vitamin E (BPD/DS only)
- Vitamin K (BPD/DS only)
- Iron (as needed)
Describe the pathophysiology for obstructive sleep apnea (OSA).
Airway blockage occurs during sleep due to soft tissue inside the throat collapsing
- Apnea = repetitive episodes of cessation of breathing during sleep cycle
- Results in blood oxygen desaturation
- Lack of oxygen triggers brief arousal from sleep to breathe
What are risk factors associated with OSA?
- Obesity – #1 risk factor
- Craniofacial abnormalities (e.g., small jaw)
- Lifestyle (e.g., cigarette smoking, alcohol use)
- Menopause
- Age
- Family history
What is the preferred therapy for OSA management?
Non-pharmacologic therapy options
What are non-pharmacologic therapy options for OSA?
Lifestyle changes (e.g., weight loss, smoking cessation)
Positional therapy (e.g., side-sleeping
Breathing devices
- CPAP: Delivers continuous pressure, cheaper than BiPAP, needs little monitoring
- BiPAP: Delivers two pressures for inhalation and exhalation, more expensive, needs monitoring of delivered pressures
- AutoPAP: Adjusts air pressure automatically based on patient’s needs
Strength exercises
Surgery
What is the only pharmacologic agent indicated to treat OSA on its own? Describe any associated warnings.
Tirzepatide (Zepbound): Dual GIP/GLP-1 receptor agonist
Indication:
- Moderate to severe OSA in adults with obesity
- Other uses: Obesity (Zepbound), T2DM (Mounjaro)
Adverse effects/warnings:
- GI effects = common
- Black box warning: Risk of thyroid C-cell tumors
- AKI, acute gallbladder disease, pancreatitis, hypoglycemia
What wake promoting agents are indicated for OSA-related daytime sleepiness (after and with PAP therapy)? Describe their MOA and associated warnings.
Non-traditional CNS stimulants (C-IV):
- Modafinil (Provigil)
- Armodafinil (Nuvigil)
MOA:
- Increases dopamine levels by inhibiting reuptake (but not considered a dopamine agonist)
- Relatively unknown
Adverse effects/warnings:
- Dermatologic effects (e.g., rashes, SJS, DRESS, TENS)
- Caution in patients with CVD
- Potentially habit forming
Describe the MOA, indication, and warnings associated with solriamfetol.
MOA:
- Selective dopamine-norepinephrine reuptake inhibitor
- Relatively unknown
Indication:
- OSA-related excessive daytime sleepiness (after and with PAP therapy)
- Other uses: Narcolepsy
Adverse effects/warnings:
- Schedule C-IV controlled substance
- Psychiatric effects
- Caution in patients with CVD
- Potentially habit forming