Lecture 32 - Drug Induced Skin Reactions
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
what are the 2 most common cutaneous drug reactions
Morbilliform/exanthematous eruption
Urticaria
what symptoms accompanied by a cuteneous drug reaction indicate a more severe reaction
Presence of a fever or other accompanying symptoms other than itch signals a more serious reaction (complex), which requires immediate referral
what are examples of simple reactions
Exanthematous eruptions, also known as morbilliform or maculopapular eruptions
what are qualities of simple reactions
Usually none, or limited, systemic symptoms (i.e. fever)
Benign and self limiting
Start as macules (pink/red in lightly pigmented skin; purple/brown/black in darkly pigmented skin), become confluent and later spread symmetrically, scaling and desquamation may follow
Itch may be present
what are qualities of complex reactions
Fever, arthralgia, shortness of breath, skin tenderness, mucous membrane involvement, angioedema or swelling of tongue, enlarged lymph nodes, end-organ injury
what kind of reactions are caused by type 1 IgE antibodies
urticaria, angioedema, anaphylaxis
what type of reactions are caused by type 2 cytotoxic drug-induced reactions
pemphigus and thrombocytopenia/purpura
what type of reactions are caused by type 3 immune complex reactions
vasculitis, serum sickness
what type of reactions are caused by type 4 delayed hypersensitivity reactions
exanthem, fixed and lichenoid drug
what type of reactions are caused by non-immune reactions
overdose, drug interactions
what type of reactions are idiosyndratic (don’t know cause)
DRESS (Drug-Related Eosinophilia with Systemic Symptoms), drug-induced lupus
what is the most common mechanism of drug reactions
type 4 delayed hypersensitivity
what are risk factors for drug induced skin reactions
women
elderly
immunosuppression (EBV, HIV)
number of drugs
genetic predisposition
prior history of drug reaction
primary drugs in hospitalized patients (penicillins, sulfonamides, NSAIDs)
what genetic factor is commonly associated with drug induced skin reactions
HLA-B variations
can you test your way out of a drug reaction
No genetic basis has been found for most adverse drug reactions, including penicillin-allergic reactions
what are considerations for skin-prick testing
Done 4-6 weeks post-reaction
Oral drugs can be crushed and dissolved for testing
Look for a hive response (IgE only)
Can get false positives and negatives
how can drug induced skin reactions be classified
according to timing into immediate reactions and delayed reaction
The most important information in determining if a rash/reaction is medication-related in its timing
what is considered an immediate reaction
< 1 hour from the last administered dose
e.g. urticaria, angioedema, anaphylaxis
what is considered a delayed reaction
> 1 hour and usually > 6 hours from last administered dose
occasionally weeks-months after the start of administration
e.g. morbilliform eruptions, fixed drug eruption, SJS, TEN, vasculitis
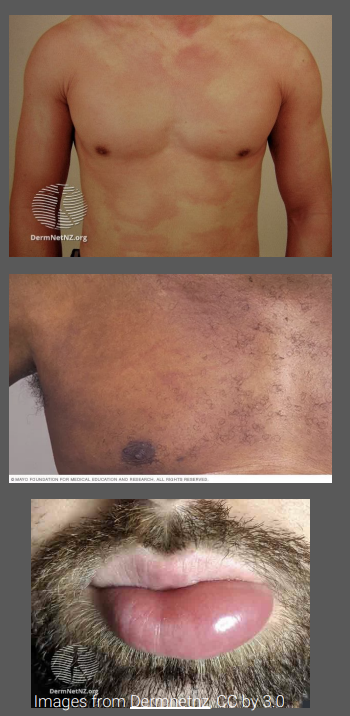
what is the clinical presentation of Exanthematous drug eruptions
Usually first appears on the trunk and then spreads to the limbs and neck
Distribution is bilateral and symmetrical maculopapular rash
Discrete lesions may merge together to form large patches or plaques
May be associated with a mild fever and itch. As it improves, the redness dies away and the surface skin peels off.

what is the mechanism of Exanthematous drug eruptions
Type 4 hypersensitivity reaction
what does “Morbilliform” mean
refers to rashes that resembles measles
Begins on trunk and upper extremities becomes confluent
Mucous membranes spared
what is the timeline for developing Exanthematous drug eruptions
Usually develops 7-14 days after starting a new medication
what are common causative agents of Exanthematous drug eruptions
Penicillins, sulfonamides, cephalosporins, anticonvulsants
how are Exanthematous drug eruptions treated
Stop the offending agent
Topical steroids for symptom relief and vasoconstriction
Resolves within 2 weeks without any complications or sequelae (residual symptoms)
what is the clinical presentation of Urticarial eruptions
Can affect any body site
Itchy and burning sensation (burning if deeper in skin)
Erythematous, edematous papules, and plaques, often surrounded by a vasoconstricted halo (wheals)
Angioedema – subcutaneous swelling of the skin or mucosa (eyelids, lips)
Lesions often last less than 24 hours and are characterized by spontaneous appearance and resolution
what is the mechanism of Urticarial eruptions
Type 1 hypersensitivity reaction mediated by IgE antibodies
what is the timeline of presentation of Urticarial eruptions
Appear within minutes to days of drug administration
Duration of individual lesions is less than 24 hrs
Urticarial vasculitis lesions last longer than 24 hrs
Acute urticaria <6 weeks
Chronic urticaria > 6 weeks
what are common causative agents of Urticarial eruptions
Antibiotics (penicillins, cephalosporins)
how are Urticarial eruptions treated
Stop the culprit drug
Consider oral antihistamines (usually at higher than standard dose for allergic rhinitis)
what is the clinical presentation of Fixed drug eruptions
Characterized by the formation of an erythematous or pigmented patch (round or oval shape)
Early lesions are sharply demarcated erythematous macules
Lesion may progress to become edematous, forming a plaque, which may evolve to become a bulla (blister) and then an erosion
Lesions are commonly solitary, however, there may be multiple lesions with random distribution
May become scaly and cause post-inflammatory hyperpigmentation
Patients do not generally report systemic symptoms (unless bullous form - rare)

what is the mechanism of fixed drug eruptions
likely a localized type IV hypersensitivity
how might the presentation of fixed drug eruptions vary
Classically a dusky, violaceous hue (non-pigmented fixed drug eruption exists)
Can be widespread (generalized fixed drug eruption)
what is a Generalised bullous fixed drug eruption
rare reaction
Numerous large blisters and erosions with normal skin between typically affecting <10% of the skin surface
Fever, malaise and arthralgia may be associated
what are common areas of involvement for fixed drug eruptions
Acral surfaces
Face/lips
Genitals
what is a potential consequence of fixed drug eruptions
post-inflammatory hypopigmentation after resolution
what are common causative agents for fixed drug eruptions
Tetracyclines
Sulfonamides
NSAIDs
Pseudoephedrine – associated with non-pigmented fixed drug eruption
how is a fixed drug eruption treated
Discontinuation of suspected medication
Avoiding implicated medication indefinitely
Topical steroids/systemic corticosteroids
Generalized blisters require intensive care or burn wound care
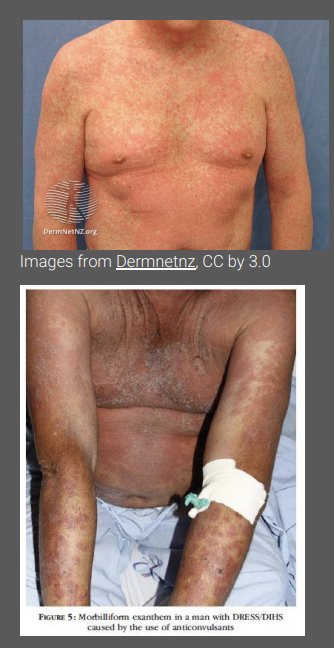
what is the clinical presentation of Drug reaction with eosinophilia and systemic symptoms (DRESS)
Systemic symptoms (high fever) present followed by the development of a rash
Morbilliform presentation but targetoid lesions, blisters and pustules may be present
Erythroderma or exfoliative dermatitis may follow in some patients
Facial swelling or mucosal involvement (lips, mouth, throat, genitalia) in some
Multiple organ involvement (e.g.lymph nodes, blood, liver, lung, GI, kidneys, neurological system, heart)
what are common causative agents for DRESS
Anticonvulsants (phenytoin, carbamazepine, phenobarbital)
Antibiotics (dapsone, sulfonamides, minocycline)
Antiretrovirals
Allopurinol
NSAIDs
what is the timeline for developing DRESS
Develops 2 to 6 weeks after the drug was started
how is DRESS treated
Stop the culprit drug
Most cases require prolonged treatment with systemic corticosteroids
Slow taper over several weeks or even months
what needs to be monitored long term in DRESS patients
Thyroiditis
Hepatitis is responsible for most deaths from DRESS (10% mortality)
Monitor TSH and T4 at 3mos, 1 yr, and 2 yrs post reaction
Pancreatitis
Development of Type I diabetes mellitus possibly
Chronic exfoliative dermatitis
what is the clinical presentation of Stevens-Johnson syndrome (SJS) OR Toxic epidermal necrolysis (TEN)
Prodromal illness (resembling an upper respiratory tract infection) for several days before rash
An abrupt onset of a tender/painful red skin rash starting on the trunk and extending rapidly over hours to days onto the face and limbs
The lesions may be flat, red, diffuse (macule)
Diffuse erythema
Blister development
Blisters then merge to form sheets of skin detachment, exposing red, oozing dermis
Painful (mucous membranes hurt)
what is SJS or TEN characterized by
Mucocutaneous tenderness
Positive Nikolsky sign
Skin fragility and erosion/necrosis
Skin lesions typically arise first on palms and soles
Involvement of oral, genital, ocular mucosa, esophageal, respiratory tract
how is SJS or TEN classified
SJS <10% body surface area (BSA) epidermal detachment
SJS-TEN overlap : 10-30% BSA involvement
TEN >30% BSA epidermal detachment
what is the timeline for SJS/TEN presentation
usually occur 7-21 days after initiation of the responsible drug
how is SJS/TEN treated
Discontinue the offending medication
Reduces risk of death by 30% per day
Systemic corticosteroids (Solu Medrol or dexamethasone)
Involve other care units: ophtho, urology, wound care, ICU, burn unit, plastics surgery
The following agents are debated for their role in management:
Cyclosporine (~7 days)
Etanercept 50mc SC x 1 dose
IVIg
how can Photosensitivity & Phototoxic Reactions vary
idiopathic
secondary to endogenous substances (porphyrins as in porphyrias)
secondary to exogenous substances (medications)
what are the 2 major types of photosensitivity reactions
phototoxic reactions (most common)
photoallergic reactions
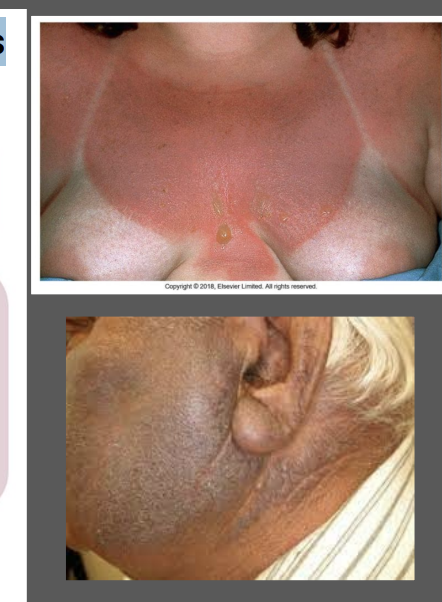
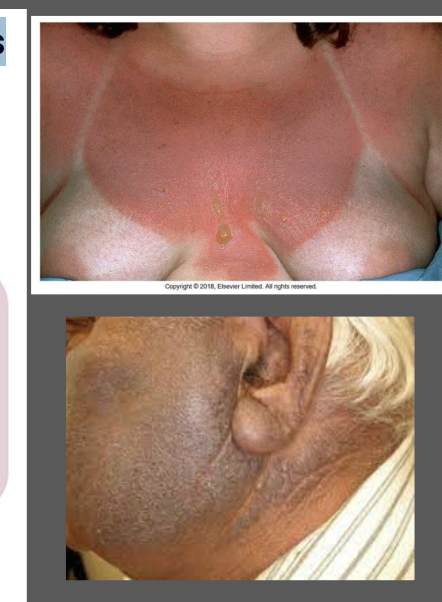
what is the clinical presentation of phototoxic reactions
appears identical to sunburn
involves sun-exposed sites only
secondary to tetracyclines, NSAIDs, thiazide diuretics
what is the clinical presentation of photoallergic reactions
secondary to a cell-mediated hypersensitivity to an allergen activated or produced by the effect of light on a drug
typically appears more eczematous
can be result of chronic dermatitis
involves both sun-exposed and non-sun exposed sites
secondary to quinolones, solfonamides, antimalarials, TCAs
how are Photosensitivity & Phototoxic Reactions treated
Discontinue offending agent
Topical corticosteroids
Use of broad spectrum sunscreen with an SPF of at least 30
what are non-pharm treatments for drug induced skin reactions
Care for the skin barrier, use unscented moisturizer or white petrolatum
Physical measure is helpful in cooling the skin by tepid showering
Tap water compresses can be used on blistering lesions
Oral lesions can be treated with warm water or saline rinses
how can arthralgia or pain be managed in drug induced skin reactions
Use acetaminophen or NSAID (as appropriate)
how can pruritus be managed in drug induced skin reactions
H1-antagonist antihistamines and nonsedating antihistamines
what is the appropriate dose of prednisone when using systemic treatment
1-2mg/kg/day
what are supportive measures for severe cutaneous reactions such as SJS/TEN
require intensive supportive care
Management of airway, monitor renal function, monitor fluid and electrolyte balance, more intensive pain control and infection prevention
what are monitoring and follow up parameters for drug induced skin reactions
After discontinuation of medication, most drug-induced cutaneous eruptions will resolve in 5–7 days
More severe drug reactions may take several months
Monitor for recurrence, development of malaise and fever = refer to physician
In DRESS, long term monitoring of organ functions may be required
what are red flags for drug induced skin reactions
Malaise or fever
Edema of the face, swelling of tongue
Lymph node involvement
Pustules and vesicle formation
Dusky or painful lesions
Skin fragility or tenderness
Mucous membrane involvement
Marked peripheral blood eosinophilia
Large body surface area involvement
Shortness of breath
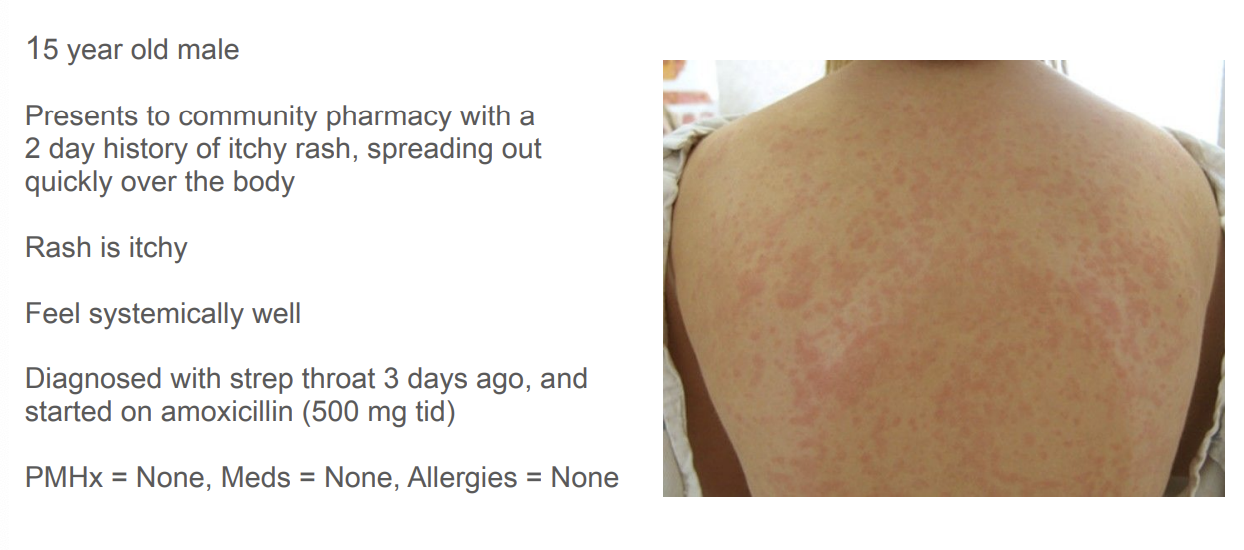
What additional information are you looking for to gain understanding of the presenting illness?
immunizations?
other medications?
previous medication reactions?
change in products used at home? (e.g. laundry detergent)
previous viral illness
recent travel

What is your assessment of the presenting medical issue? What evidence supports this assessment?
exanthematous eruptions - simple reaction

What is your management (treatment) plan?
topical hydrocortisone
antihistamines
potentially change the amoxicillin to something else

What steps will you take in regards to monitoring and follow-up?
if no major symptoms present, would be appropriate to re-challenge allergy in the future
monitor for red flags and worsening