Biomechanics Final SG - Butler
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
What is sports biomechanics? What does it focus on?
Sports Biomechanics
The application of mechanical principles to study human motion during sports
Focuses on:
decreasing injuries
Increasing performance
Biomechanics principles
What are the 5 biomechanics principles?
What is passive and active shock absorption? What if active absorption is decreased?
Biomechanics principles TMJDS
Transfer of energy
Movement strategy
Joint excursion
Dynamic stability
Shock absorption
Passive shock absorption (where we want to limit)
Bone, cartilage, meniscus, ligament
Active shock absorption (where we want to increase absorption)
Eccentric muscle contraction, dynamic stabilization
If decrease active absorption → increase passive compensation = increase risk of injury
Biomechanics principles - more on dynamic stability
How is it achieved? What is it?
Poor neuro muscular control of the LE will cause what three risks?
For risk 1, what is it? What motion at the ankle and the foot? Absorption of the GRF relying on _____ ______ rather than ______ ______.
For risk 2, what is it? Shock absorption of the GRF relying on _____ ______ rather than ______ ______. Increases loads for what joint? Failure to utilize? Due to the failure to hip hinge, this shows?
For risk 3, what is is? Poor control of what over what, causing increased loads on what joint?
Cutting tasks are reported as the cause of ____% of non-contact ACL tears in collegiate basketball & soccer players. What are the biomechanical risk factors for this this? (4)
Dynamic stability
Achieved through neuromuscular control of LE biomechanics. Athlete’s ability to stabilize the joints in all planes (sagittal / frontal / transverse)
Poor NMC of LE is a significant contributor to knee injury risk:
Risk 1 – Dynamic Knee Valgus
Frontal / transverse plane collapse of the LE
Ankle eversion
Foot pronation
Decrease absorption of GRF → relying on static stabilizers rather than dynamic
Risk 2 – Increased Knee Extension (stiff, decreased flexion)
Stiff, extended knee landing
Decrease shock absorption of GRF relying on static stabilizers rather than dynamic
Increased knee joint loads
Failure to utilize posterior chain
Fail to hip hinge in landing → decreased hip control → Increased hip IR / Add → Increase valgum
Risk 3 – Lateral Trunk Deviation (leaning over stance limb)
Asymmetric loading – too much load on one LE compared to the other
Poor control of the COM over BOS → increased knee joint loads
Cutting tasks are reported as the cause of 57% of non-contact ACL tears in collegiate basketball & soccer players
Biomechanical risk factors that have been identified
knee abduction / dynamic LE valgus
lateral trunk displacement over injured leg
decreased hip–knee flex angle
decreased PF angle
Biomechanics of Cutting / Change of Direction
Trunk
How should it move, and what would a negative finding look like and cause?
Pelvis
How should it move, and what would a negative finding look like and cause?
Facilitate force transfers in which direction?
Knee
How should it move, and what would a negative finding look like and cause?
Should be flexed about how many degrees? This is for _______ control.
Foot
How should it move, and what would a negative finding look like and cause?
Foot should land where relative to the body?
Trunk position
Should rotate & lean in the direction of cut
(-) ↑ lateral trunk flexion over the plant foot → knee joint loads
Pelvis
Should follow trunk and rotate in direction of cut
(-) Rotation toward plant foot = femur IR
Facilitates force transfer towards direction you want
Knee
Should remain in line with hip & ankle
(-) ↑ dynamic knee valgus angle → ↑ knee load
Should be flexed ~30° for eccentric control
(-) decreased Knee flex = increased GRF
Foot
Should land flat or toe-to-heel (to decrease brake force)
(-) Heel-first → ↑ horizontal braking forces → ↑ GRF
Should land close to the body
(-) Wide cut width → ↑ knee loading
Classifying Movement Pattern Dysfunction
Ligament dominance
What is it, what is its cause?
Quadriceps dominance
What is it, what is its cause?
Leg dominance or residual injury deficits
What is it, what is the cause?
Trunk dominance “core” dysfunction
What is it? What is the cause?
Ligament Dominance
LE valgus at landing, Dynamic valgus
Foot placement not shoulder-width apart, Poor frontal plane knee control
Quadriceps Dominance
Excessive landing contact noise
Stabilizing the knee by primarily activating the quads, creates a stiff knee position
Leg Dominance or Residual Injury Deficits
Thighs are not equal side-by-side during flight. Asymmetrical loading
Foot placement is not parallel (front-to-back), Foot contact timing not equal
Trunk Dominance / Core Dysfunction
Thighs do not reach parallel (peak of jump)
Pause between jumps, Does not land in same footprint, Poor control of COM over BOS, ↓ proprioception

Clinical assessment tools
what is it? What tasks can be used? How to interpret scale? Stats?
Qualitative
Qualitative assessment of single leg loading
what is it? What tasks can be used? How to interpret scale? Stats?
Expanded cutting alignment scoring tool (ECAST)
what is it? What tasks can be used? How to interpret scale? Stats?
Movement screening for volleyball
what is it? What tasks can be used? How to interpret scale?
Quantitative
Knee ankle separation ratio (KASR)
what is it? What tasks can be used? How to interpret scale?
Acceptable valgus during a hop task
during IC? Max flexion?
-Qualitative-
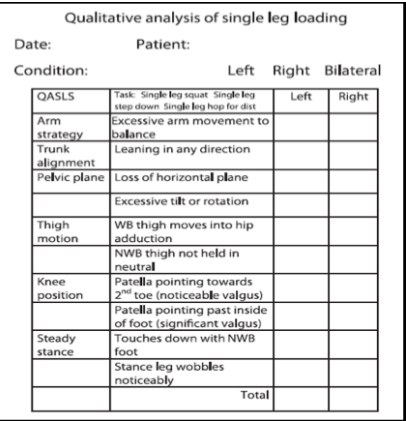
Assessment of Single-Leg Loading – QASLS
What is it?
A scoring of inappropriate movement strategies for single-leg tasks
What tasks can be used?
Applied to dynamic SL tasks (SL squat, etc.)
How to interpret score
Increase score = decreased quality of movement
0 = not present
1 = present
Cut off score >2 suggested
Stats
check intra- / inter-reliability
check validity compared to 3D motion capture
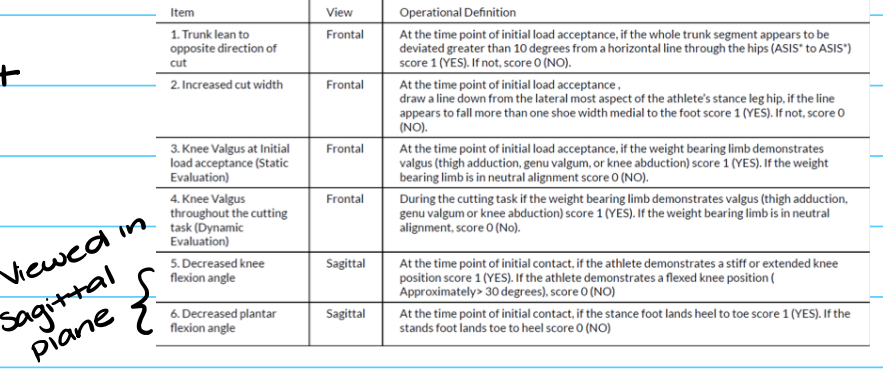
Expanded Cutting Alignment Scoring Tool – ECAST
What is it?
Qualitative analysis of trunk & LE alignment during a 45 degree cutting task (frontal plane)
What tasks can be used?
45 step cutting tasks
How to interpret score
increased score = increased risk
0 = not present ; 1 = present
Stats
check validity against 3D motion capture
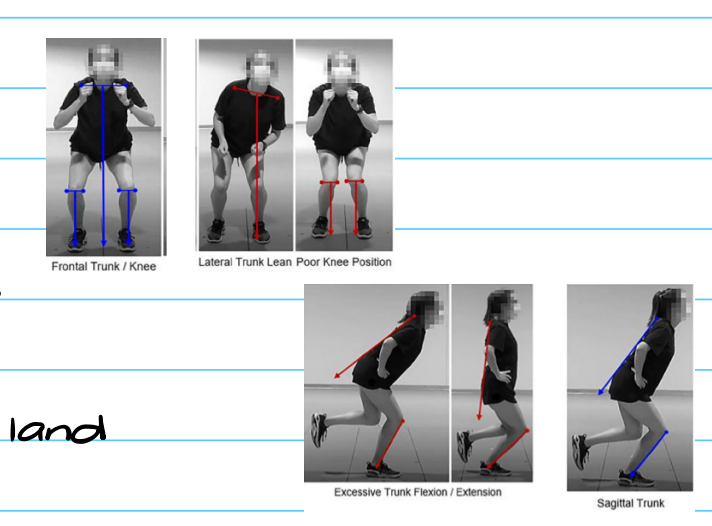
Movement Screening for Volleyball
What is it?
Risk factor assessment for volleyball players
What tasks can be used?
SL squat
DL vertical jump
SL drop land
How to interpret score?
An observational screening to find common faults (trunk lean, dynamic valgus, etc.) in sagittal & frontal planes
-Quantitative-
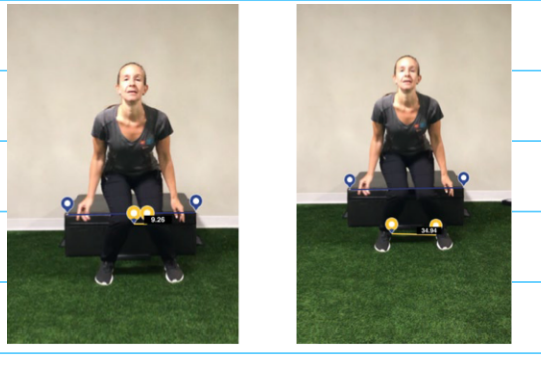
Knee ankle separation ratio (KASR)
What is it?
Measures distance between knees/ankles
What tasks can be used?
Drop vertical jump or hop tasks; any DL activity
How to interpret score
In drop vertical test:
1.0 = knee perfectly aligned with ankles; <1.0 Knee valgus; > 1.0 = Knee varus
<0.8 = ACL injury risk (excessive knee valgus). EX if KASR is 0.7 = BAD!
Acceptable valgus during a hop task
IC < 5 degrees ; Max flexion < 8 degrees.
UE sports biomechanics
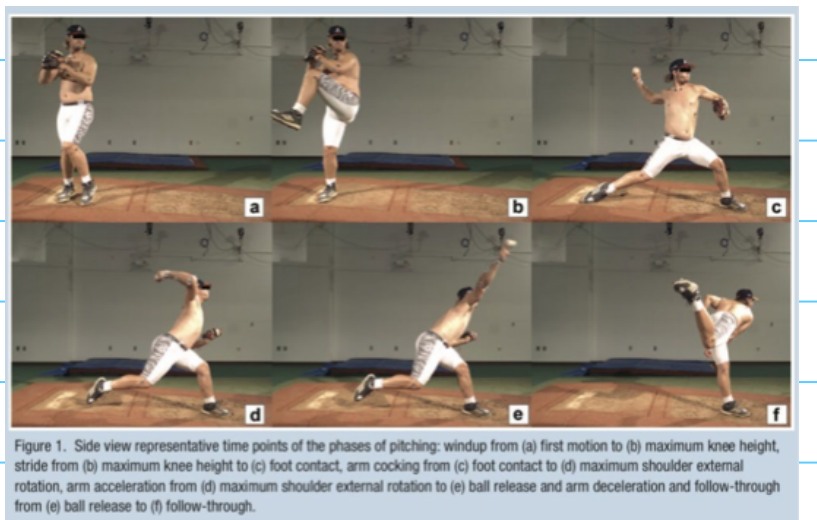
What are the pitching phases/biomechanics? (6)
Wind up
Stride
Arm cocking
Acceleration
Deceleration
Follow through
Pitching phases/biomechanics
Entire motion takes how long?
Angular velocities? (shoulder and elbow)
Ball release distraction forces are _____ times body weight
Increase ball velocity causes?
Use of entire kinetic chain is important to?
Entire motion is about 2 seconds
Angular velocities
>7000 / seconds @ shoulder
> 3000 / seconds @ elbow
Ball release distraction forces = 1.5 body weight
Increase ball velocity = increase forces at elbow and shoulder
Use of entire kinetic chain is important to transfer energy from lower body to upper body
Wind up
For forces and torque, are they high or low?
Starts?
Ends?
What supplies the forward momentum?
Low forces, Low torque
Starts: when pitcher begins to lift lead leg
Ends: when lead leg reaches max height
Push off force of trail leg supplies the forward momentum
Stride
Starts?
Ends?
Stride length? What if its too short or too open?
Knee flexion degrees needs to be? This it to?
Pelvis should?
Shoulders needs to? degrees for abd, horizontal abd, ER? What if horizontal abduction is excessive at foot contact?
Elbow flexion degrees?
Starts: End of wind up
Ends: @ foot contact with foot at closed angle (pointing to 3rd base)
pitcher pushes off the mound to move towards home plate
Stride length: distance from hind leg ankle to lead ankle divided by height . 85% of height is ideal.
Too short: not enough time to achieve optimal shoulder ER. Caused because of decreased SL balance, decreased hip strength.
Too open: Pelvis rotates too soon, leading to increased shoulder and elbow stress
Knee flexion about 45 degrees to absorb GRF
Pelvis should begin to rotate forward to name plate
Shoulders remain parallel to home plate
90 degrees abd, 20 degrees horizontal abd, 45 degrees ER
Excessive horizontal abduction at foot contact increases anterior forces at shoulder
Elbow flexion to 90 degrees.
Kinematic chain
Foot contact is important because it?
What is the KEY to maximizing the kinetic chain?
Requires what two things?
Foot contact is the source of energy that transmits up the body to maximize power output
Proper timing between rotation of the pelvis and upper trunk is key to maximizing the kinetic chain
Requires adequate spinal mobility and dissociation
Arm cocking
From what to what?
Trunk position? What should it not be and why? treatment?
Shoulder position max ER is? What if its too much and too little? Treatment?
Elbow position? What if its too little trunk angle and too little elbow flexion + early horizontal adduction?
Where is tensile strains observed along what locations? Highest at? Compressive forces observed along what location?
Scapular positioning: why is it important?
Upper trunk and pelvis reach max velocity when?
Dissociation of _____ and ______ control
From foot contact to max shoulder ER
Trunk position should have a slight forward lean at foot contact
Backward lean = increase shoulder and elbow joint loading because of decreased momentum arm. Treatment would be core strengthening and trunk proprioception training.
Shoulder positioning max ER is about 170 degrees
Too much ER: Increase internal impingement and elbow torque. Treatment would be shoulder proprioception training and strengthening
Too little ER: Usually due to decrease abduction. Treatment would be increasing ER ROM at 90 degrees abduction, and ensure adequate abduction ROM and strength.
Elbow position → should be at 90 degrees angle to trunk and flexed 90 degrees.
Lower angle to trunk post increases horizontal abduction at the shoulder which increases stress on anterior shoulder
Too little elbow flexion combined with early horizontal add with cause “leading with the elbow”
Tensile train observed along anterior shoulder and medial side of elbow is the highest at the late cocking phase. Compressive forces observed along posterior shoulder and lateral side of elbow.
Scapular positioning is important to maintain a stable base for humerus. Max ER → into max IR at > 7000 degrees / second.
Upper trunk and pelvis reach max velocities at late cocking
Dissociation of upper and lower trunk control.
Acceleration
Starts when?
Ends when?
IR velocity is? Shoulder IR with rapid _____ _____.
At ball release, the shoulder should maintain?
Trunk position should have? This maintains what? Trunk forward flexion is how much? What if its too little?
Lead knee should be what during this phase and Why? Decreased in this motion is due to?
Starts: Max ER
Ends: Ball release
IR velocity is > 7000 degrees / seconds (shoulder IR with rapid elbow extension)
At ball release, the shoulder should maintain 90 degrees abduction and elbow flexion at 25 degrees.
Trunk position → should have slight tilt toward glove hand (10 - 20 degrees) which maintains the shoulder abducted.
Too little trunk lateral flexion = side arm throwing mechanism compromised increasing medial elbow stress.
Lead knee should be extended during this phase to decelerate forward hip motion.
Decrease knee extension = poor quad strength or unstable BOS.
Deceleration
When does this take place?
Tensile strain is noted where? This is to do what?
Compressive forces observed along what area?
Highest _____ control of ERs
Highest _____ tension
Immediately following ball release
Tensile strain noted on the posterior shoulder to decelerate the shoulder and control horizontal adduction
Compressive forces observed along the anterior aspect of the shoulder
Highest eccentric control of ERs
Highest posterior tension
Follow through
When does this happen?
Increased range of?
Requires what motion? What if this motion is too little?
Body moves in a forward direction until the arm stops moving
Increases range of closed kinetic chain hip IR
Requires increased hip IR ROM
Too little IR = CAM + Pincer impingement
Summary of injury risk for
Max ER (Late cocking)
Greatest force on _____ shoulder
Ball release (follow through)
Greatest force on _____ shoulder
Requires what two things to decelerate the body and arm?
Arm slot (the good 90 abduction)
Elbow is not maintained at ______ to trunk, causing?
Kinetic chain
Failure to utilize at all phases of the pitch increase the stress to what structures?
Requires good ________ of trunk and pelvis
Max ER (Late cocking)
Greatest force on anterior shoulder
Ball release (follow through)
Greatest force on posterior shoulder
Requires good balance and core strength to decelerate the body and arm?
Arm slot (the good 90 abduction)
Elbow is not maintained at 90 degrees to trunk, causing medial elbow stress
Kinetic chain
Failure to utilize at all phases of the pitch increase the stress to the shoulder and elbow
Requires good dissociation of trunk and pelvis
Abnormal gait: Neurological gaits
Parkinson gait
What is the posture like and how does that affect the COG?
People with this gait have a shuffling like motion, this means no what? (4)
rigidity or spasticity? Bradykinesia or akinesia?
People with this gat may demonstrate freezing, this means?
What is festination?
This gait it typically found in what conditions? (3)
Hemiplegic gait
What is it?
What two motions happen to the affected hip?
Ankle in _______ with weak ______ and ______.
Knee and hip move into what motion to compensate during floor clearance?
Typically found in what condition?
Ataxic gait
What is typically seen in this gait? (3)
What conditions is this typically found in?
scissoring gait
What happens to the BOS in this gait?
LE _______ due to _______ spasticity
Spastic dorsi or plantarflexion? This causes to the toes to?
Legs end up crossing what?
What condition is this typically found in?
Waddling gait
This gait occurs due to? This causes what to occur at the hip and what to occur at the trunk?
What condition is this typically found in?
Parkinson gait
Flexed posture of neck, trunk, hips and knees → moves COG anterior
Shuffling → NO heel strike, toe off, arm swing, or pelvic rotation.
Rigidity and bradykinesia
Freezing = difficulty initiating steps
Festination → urge to take short quick steps
Found with PD, Wilson disease and cerebral atherosclerosis
Hemiplegic gait
Unliteral weakness
IR and Add of affected hip
Ankle in drop foot with weak plantarflexion and inversion (equinovarus)
Knee and hip move into flexion to compensate during floor clearance
Found with strokes
Ataxic gait
Decreased coordination, staggering movement, widen BOS
found in cerebellar disease
scissoring gait
Narrow BOS
LE adduction due to Add spasticity
Spastic plantarflexion (equinovarus). Causes toes drag on the floor
Leg cross midline
Found with spastic CP
Waddling gait
Glute med weakness (bilaterally)
Pelvic drop on both sides (contralateral drop during stance) and trunk lean (ipsilateral in stance)
Found with muscular dystrophy
Abnormal gait: MSK gaits
Trendelenburg gait
What are the causes of this gait? (2 primary 1 compensatory)
This creates what at the pelvis and what at the trunk?
Lurching gait
What are the causes of this gait? (1 primary and 1 compensatory)
This causes what to occur? What does it mean if this occurs during stance VS during swing?
Circumduction gait
What are the causes of this gait? (3 compensatory)
What 4 things occur during this gait?
Steppage gait
What are the causes of this gait? (4 compensatory)
This causes what to occur during swing?
Antalgic gait
What is the cause of this gait? (4 primary)
This causes what to occur? Reasons? (4)
Leg length discrepancy gait
This gait occurs due to? This can be seen in what conditions?
Compensatory gait that occurs cause the pelvis to do what? Causes the hip and knee to do what?
Trendelenburg gait
Possible causes:
Primary: weak hip abductors on reference limb, adductor contracture on reference limb
Compensatory: Leg length discrepancy → short contralateral limb
Creates:
contralateral pelvic drop on swing limb during stance on reference limb
ipsilateral trunk lean on reference limb during stance
Lurching gait
Possible causes:
primary: stance (weak hip extension)
Compensatory: swing (weak hip flexion)
Creates: Backward lean of trunk
During stance: LOG moves posterior, decreased hip extension torque
During swing: compensation for inadequate hip flexion
Circumduction gait
Possible causes:
Compensatory: advance the limb and clear the foot when hip flexion, knee flexion, and dorsiflexion are inadequate.
Creates:
Hip hike, hip flexion, forward rotation of pelvis, abduction of hip → in stance phase
Steppage gait
Possible causes: Compensatory
Inadequate knee flexion in initial swing for toe clearance
Inadequate dorsiflexion in mid swing for toe clearance (Foot drop, L5 radiculopathy, peroneal palsy)
Excessive contralateral knee flexion (shorten stance limb)
Long swing limb
Creates:
Excessive hip flexion and knee flexion during swing
Antalgic gait
Possible causes:
Primary: pain in reference limb due to pain at the trunk, hip, knee, ankle
Creates:
Decreased stance time on reference limb, decrease step length on opposite limb
Reasons:
Knee pain → decrease weight bearing
Forefoot pain → avoided toe off
Heel pain → increase toe weight bearing instead
Hip pain → decrease weight bearing
Leg length discrepancy gait
Occurs due to asymmetrical length of pelvis, tibia, and femur. Conditions that cause this are scoliosis and contracture
Compensatory gait
Pelvis: Drop on short side in stance with increase plantarflexion
Hip and knee: Longer limb presenting with increased hip flexion and knee flexion to help decrease length
Trunk deviations
What is it? Causes? (2 primary, 1 secondary, 1 compensatory, 1 contracture)
Forward trunk lean in stance
Causes:
Primary: skeletal deformity, decrease hip extension strength (pelvis falls forward, trunk follows)
Secondary: excessive anterior pelvic tilt
Compensatory: quad weakness (provides passive knee extension force by placing COM anterior to knee)
Hip flexion contracture: without compensatory lordosis → trunk follows pelvis into flexion
Pelvis deviations
Posterior pelvic tilt (Causes at stance (1 primary 1 secondary) and at swing (1 secondary))
Anterior pelvic tilt (causes at stance (2 primary 1 secondary))
PPT
At stance: Primary HS tightness; secondary hip flexion weakness
At swing: Secondary hip flexion weakness
APT
At stance:
Primary hip flexion contracture and hip extension or abdominal weakness
Secondary due to forward trunk lean
Hip deviations
Hip hike: what is it and what are the causes (1 for initial swing 1 for mid swing)?
Thigh medial rotation: what is it and what are the causes (2 primary 1 compensatory)
Hip hike
Excessive elevation of pelvis in swing on reference limb
Possible causes:
Compensatory toe clearance when there is not enough knee flexion in initial swing or not enough hip flexion and dorsiflexion in mid swing.
Thigh medial rotation
Position of femur with femoral condyles facing medially
Possible causes
Primary: Skeletal deformity (femoral anteversion), decreased motor control
Compensatory: to increase knee stability due to weak quads in stance
Ankle/foot deviations
During stance phase
Early heel off
When does this happen
Possible causes (2 primary and 1 compensatory)
No heel off
When does this happen
Possible causes (2 primary 1 secondary)
Excessive pronation
What is it?
Possible causes (2 primary, 2 secondary, 1 compensatory)
Excessive inversion (pes cavus)
What is it?
Possible causes (2 primary, 1 secondary)
Foot slap
What is it and when does it occur
Possible causes (1 primary)
Flat foot contact
What is it and when does it occur
Possible causes (1 secondary and 1 compensatory)
Forefoot contact
What is it and when does it occur
Possible causes (1 primary and 2 secondary)
Abbreviation heel contact
What is it and when does it occur
Possible causes (2 primary, 1 secondary, 1 compensatory)
During swing phase
Contralateral vaulting
What is it and when does it occur
Possible causes (3 compensatory)
During stance phase
Early heel off
At midstance
Possible cause
Primary: PF contracture, overactive PF
Compensatory: to accommodate short reference limb
No heel off
At terminal stance
Possible causes
Primary: weak PF (surgical lengthening of Achilles tendon), Forefoot pain
Secondary: inadequate toe extension
Excessive pronation
More calcaneal/forefoot eversion
Possible causes
Primary: skeletal deformity (hindfoot valgus), weak posterior tibialis
Secondary: compensated forefoot varus, genu valgum
Compensatory: decrease ankle dorsiflexion
Excessive inversion (pes cavus)
More calcaneal/forefoot inversion)
Possible causes
Primary: skeletal deformity (hindfoot varus), equinovarus contracture
Secondary: due to genu varum
Foot slap
Rapid plantarflexion at heel strike
Possible causes
Primary: weak DF (common peroneal nerve palsy, L4 - L5 nerve injury)
Flat foot contact
IC made with both hindfoot and forefoot
Possible causes
Secondary: knee flexion contracture
Compensatory: weak quads
Forefoot contact
Initial ground contact made with forefoot
Possible causes
Primary: not enough DF or Knee extension
Compensatory: to accommodate shorter limb, heel pain
Abbreviation heel contact
Shortened interval of heel at initial contact
Possible cause
Primary: weak DF, PF contracture
Secondary: knee flexion contracture
Compensatory: weak quads
During swing phase
Contralateral vaulting
Excessive PF of opposite stance limb in swing on reference limb
Possible causes
Compensatory: to lengthen stance limb and achieve swing toe clearance because of → longer swing limb, not enough knee flexion in Initial swing, not enough DF in mid swing
Knee deviations
Rapid knee extension (extensor thrust)
When does this occur
Possible causes (2 primary 1 secondary)
Not enough knee flexion (stiff leg gait)
What is this and when does it occur
Possible causes (3 primary)
Rapid knee extension (extensor thrust)
After IC
Possible causes
Primary: weak quads, decreased motor control
Secondary: due to PF contracture
Not enough knee flexion (stiff leg gait)
Knee remains in extension during LR
Possible causes
Primary: Weak quads, decrease motor control, knee pain
Observational gait analysis
What is it?
Goal?
Qualitative assessment can occur through?
Camera placement?
Walking condition?
Footwear?
Clothing?
Reference limb?
Observation of a patients gait
Goal: Identify specific deviations from “normal” gait pattern
Qualitative assessment: through videos, apps, photos, real time assessment.
Camera placement: Level consistent, lateral anterior and posterior views
Walking condition: treadmill vs level ground, speed
Footwear: barefoot (unshod) and sneakers (shod)
Clothing: ensure visibility of all joints
Reference limb: limb of primary concern
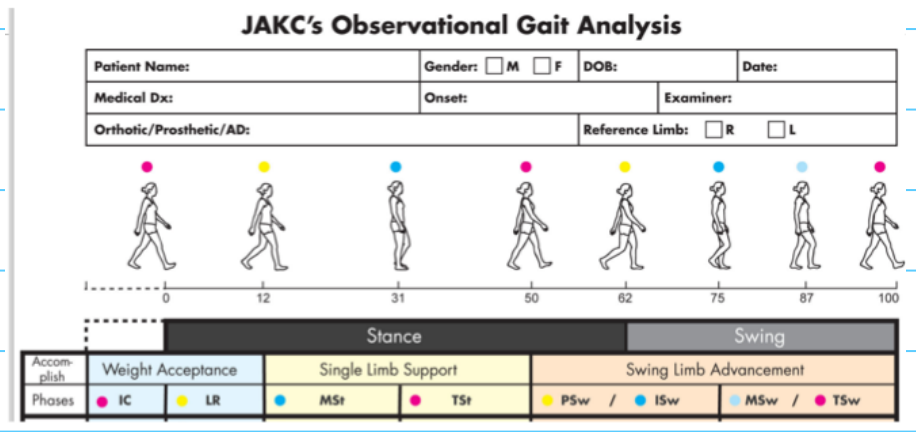
JAKC’s observational gait analysis
What is it? How does it categorize deviations?
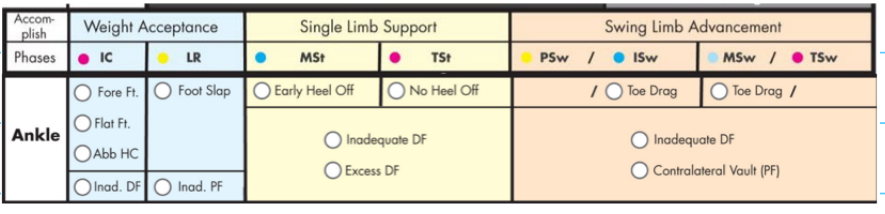
For each of the following joints how does the JAKC differ?
Ankle
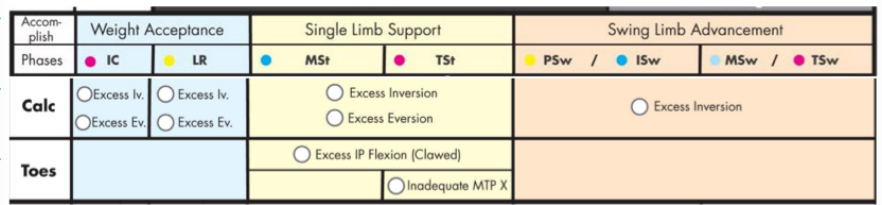
Calcaneus and toes
Knee and thigh
Pelvis
Trunk
(FOR THIS BUTLER SAID DONT STRESS ABOUT THE OBSERVATIONAL GAIT ANAYLSIS TOOL, JUST KNOW ITS USED TO ASSESS GAIT)
Jan Adams and Kay Cemy (JAKC)
Categorizes deviations into 3 gait tasks
Weight acceptance
Single limb support
Swing limb advancement
Ankle
Calcaneus and toes
Knee and thigh
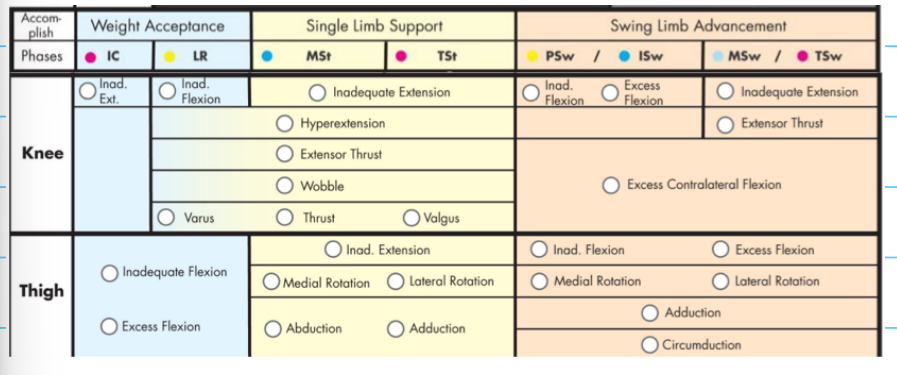
Pelvis
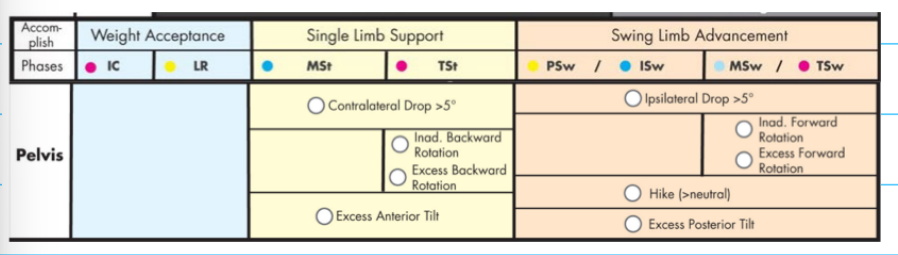
Trunk
