Global Mental Health and Psychosocial Humanitarian Aid Final
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Refugees
Displaced people who have crossed borders
Asylum Seekers
People who desire to become refugees
Stateless People
Typically, people who have had their nationality taken away
Sources of Stress for Populations of Concern
war
displacement
lack of/issues related to identity
food insecurity
travel
economic issues
settling
Migration Process
Pre-migration → migration → post-migration
History of Refugees and Other Forced Migrants
1940s-1950s: reckoning with Holocaust
1951 UN Refugee Convention
1950s-1960s: small, mostly European refugee movements
1970s campaigns against torture
end of Vietnam War and instability brought new waves of refugees
1980: DSM-III introduces PTSD
Richard Mollica’s work on PTSD and depression in Cambodia
1980s-2000s: refugee research focuses on PTSD and depression
Epidemiology of PTSD and depression
research on asylum seekers in host countries pushed researchers to look at the effects of stressors in host countries
Application of stressors to larger refugee populations
Limitations of Literature
1) Emphasis on exposure to crisis events at expense of other conditions, contexts, and protective factors
2) Over-reliance on non-validated symptom checklists
3) Variety of distress across culture rarely validated
4) Little attention to anything other than PTSD and depression
Social and Community Psychology
not about psychopathology or stress and coping like clinical psychology
social interactions
community well-being
overlap with social work traditions
MHPSS
Mental Health and Psychosocial Support; psychosocial support is “any type of local or outside support that aims to protect or promote psychosocial well-being and/or treat mental disorder”
Multimodal Psychosocial Model
1) basic services and security (socio-ecological interventions)
2) community and family supports (socio-ecological interventions)
3) focused, non-specialized support (community-based trauma counseling)
4) specialized services (community-based trauma counseling)
Core Principles of MHPSS
promotions of human rights
equity in availability and accessibility
attention to avoiding unintended consequences
active participation of affected population
strengthening local resources and building on local capacities
Theories of Refugee Distress
Conservation of Resources (COR)
“Daily Stressors” Ecological Model
Adaption and Development After Persecution and Trauma (ADAPT)
COR
stress is caused by loss and/or the anticipation of loss
all humans have a basic set of needs, some variation related to cultural meaning of resources
loss often leads to loss spirals
intervention should focus on supporting environments
Daily Stressors Ecological Model
displacement is full of stressors that are not technically traumatic
impact of displacement and trauma on stress is mediated by ongoing stress
create supportive environments that reduce daily stressors, than can identify those with psychological disorders
*chart
ADAPT
conflict affects 5 core “psychological pillars” (safety, social bonds, justice, roles and identities, and existential meaning)
allows interventions to focus on pillars that are most disrupted by conflict
*chart
Trauma Focus
trauma is the problem, PTSD treatment is the solution
applying PTSD treatments in LMIC and refugee settings
2 characteristics of “best” models: assessment and RCTs
Treatment:
seems to reduce symptoms of people with common mental disorders and trauma in short-term across a number of contexts
can be “task-shifted”
demands resources and time that may not be sustainable
intervention is shown to work in readings and is necessary to look at practical aspects (environment) and have resource support (basic needs)
Clinical Assessment
usually structured or semi-structured clinical interview (PTSD and post-traumatic stress symptoms)
sometimes will include cultural constructs of distress
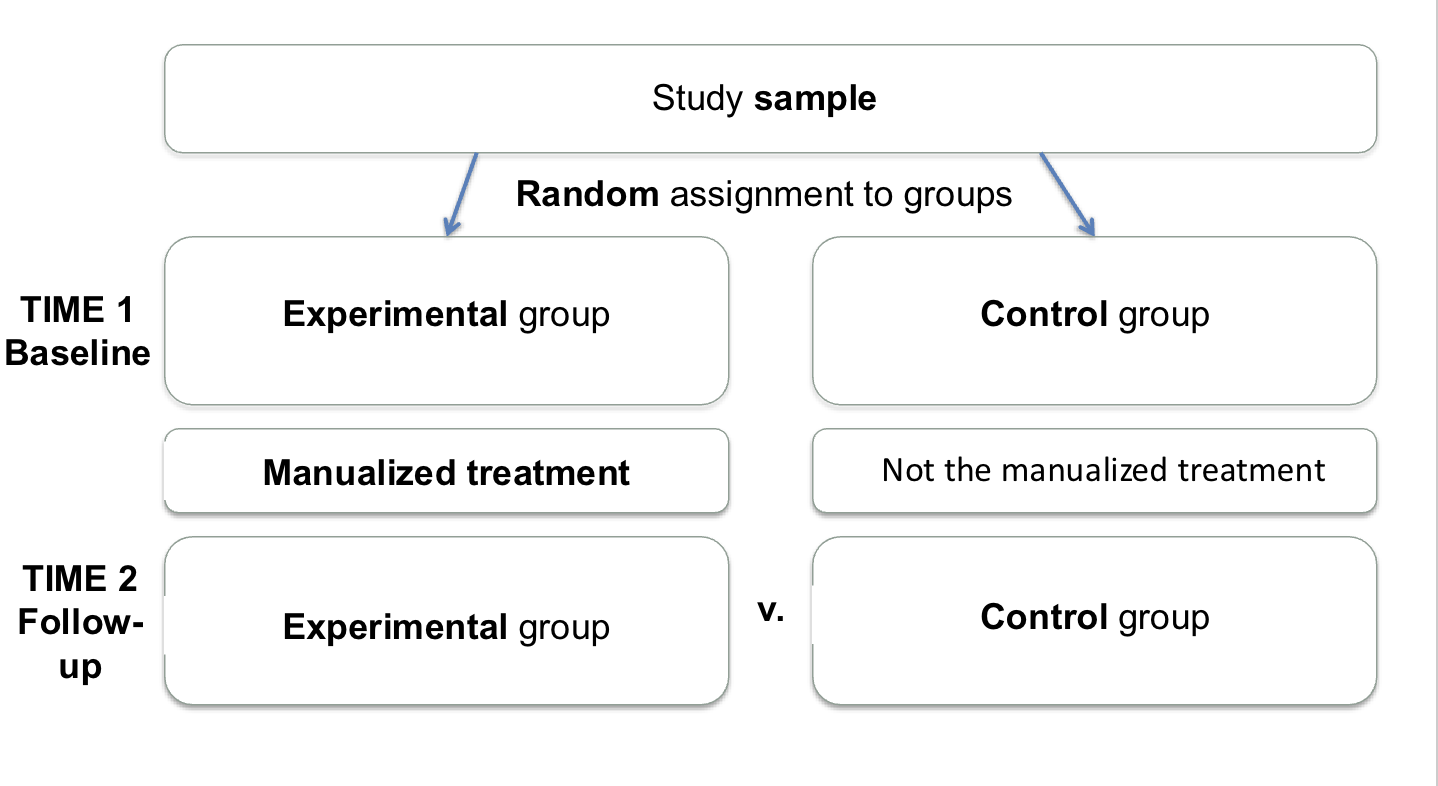
Randomized Control Trials
challenges include unstable conditions (lack of food lack of housing, natural distress, etc.), comorbidity, language barriers, and social isolation
experimental group: strict manualized treatment and treatment with guidelines
control group: counseling or treatment as usual and waitlist control
efficacious vs. effective (MHPSS cares about effectiveness)
Narrative Exposure Therapy
exposure therapy plus narrative therapy
first step is to build a timeline to identify “hot points”
acknowledging multi-trauma histories of many refugee stories
“hot points” are focus of exposure
exposure therapy is a conventional imaginal exposure brief therapy
reviewing worst “hot points” 3-6 times
monitoring arousal during the recounting
multiple RCTs in East African refugees
some European therapists
several task-shifted, locally trained practitioners
Frank Neuner
Rwandan and Somali refugees at Nakivale in Uganda
RCT with three “arms”
both treatment groups were supervisors to monitoring alone, and no different from each other
Cognitive Processing Therapy in DR Congo
trauma counseling for sexually assaulted women by IRC
“probable depression, anxiety, and PTSD” based on screener
emic inquiry and adaption of therapy
CPT is an empirically-supported PTSD treatment in U.S. and Europe
local MHPSS staff, lots of remote supervision
1 individual session and 11 group sessions
randomization of 16 villages (excluding one) into two arms
CPT vs. individual support and monitoring
both groups got better
CPT group got better more than individual group
maintained at 6 months
RCT After Conflict in Colombia
“Unified Protocol” targets neuroticism and emotional deregulation
Colombia IDP
PTSD 5.1x that of non-IDPs
adapted for IDPs
adaption
added an initial session for rapport and trust
text replaced with graphic material
involving patients’ own experiences as examples
delivered by clinical psych grad students
RCT study design
fair number lost to follow up
still large effect size differences
Testimony Therapy Buddhist Healing
traditional context
Khmer Rogue trials
therapy designed for witnesses
roots in 1970’s Argentina and Chile
“testimony” both a psychological and legal act serving justice as well as well-being
IASC
Inter-Agency Standing Committee
try to integrate idea that there should be trauma focused interventions and community focused interventions
people at UN who deal with refugees noticed discrepancy between people-focused on trauma treatment and others focused on broader approach (came up with agreements and guidelines to generate different activities to deal with stressors; also gave some new guidelines)
Critiques of Trauma Intervention
Psychological aspects: ongoing trauma; intervention as agitating clients
Practical Aspects: social support in isolating environments; resources
Critique of Psychosocial Programs
if trauma is conceptualized as the main problem, PTSD treatment is the solution
but multiple other psychosocial problems may exist as well
Sri Lanka’s NGO Tsunami
one village of 50 served by 27 NGOs
waste of resources into one village rather than others
practical issue
also problem of ignorance
Kate Chaos
uses play therapy to help children
lacks psychological approach
practical issue
not culturally informed
short-termed counseling programs
represents well-meaning attitudes of psychologists from high-income countries who have poor planning
problem of “savior attitude”
Seven Assumptions Behind Psychological Trauma Programs in War-affected Areas
1) Traumatization as a pseudo-condition
2) PTSD is the universal response to trauma
3) Large numbers need professional help
4) Best treatment is “emotional ventilation” and “working through” trauma
5) There are vulnerable groups that need targeting
6) Rapid intervention prevents mental health problems, even more war
7) Local worker are overwhelmed
Solutions:
don’t treat PTSD
look for/answer other problems
don’t do pyschotherapy
Caregiver Support Intervention
not explicitly trauma focused
more than parent education
used for Syrian refugees in Lebanon
RCT showed benefits even under extreme stressors
mindfulness exercises seem to be the most useful and sustainable (though not for some)
emotional regualtion intervention
*chart
Ethics
Set of guidelines that direct behavior of groups of people; ethics in aid are complicated given high income/low income differentials
4 Reccommendations to Do No Harm
1) critical reflection that involves local ethical perspectives
2) greater specificity for appropriate acts
3) better documentation of interventions that work
4) improved education for psychosocial workers
Individualist Orientation
informed consent
ethical issues
nonholistic support
Deficit Focus
Conceptualizing people’s problems as problems
deficit trap
victimhood and empowerment
Capacity Building and Sustainability
dependency
poor training
silo-ing with MHPSS
subtle effects of power
“crisis chasing” approach
Ethical Issues and MH Workers
risks and problems of humanitarian aid staff
90% of humanitarian aid delivered by local staff
burnout in local staff
impact on post-NGO societies
Psychosocial Occupational Hazards
repeated exposure to overwhelmed people
situations with few positive options
strained social support network
Three Psychological Conditions
1) Secondary Traumatic Stress (“contagious PTSD”)
2) Vicarious Traumatization (broader condition that includes other symptoms of anxiety and depression)
3) Burnout (emotional exhaustion, depersonalization, and lack of personal accomplishment)
Prevention of Workplace Stress
Recognition by NGOs and UNCHR of high-stress nature of work
mandatory leave policies
enforcing standards
preparation for stressful working conditions
Institutional changes
improving physical workplace environment
clear decision making processes
regular peer contact and support
Open Mole
cultural concept of distress in Liberia
vehicle of narrative of change from conflict to post-conflict mental health sector
Healthworkers International (pseudonym for MH group in Liberia) used cultural concepts of distress for various diagnoses (Open Mole/anxiety, Open Mole/depression, Open Mole/schizophrenia, etc.)
shifting and expanding meaning of Open Mole as linked to trauma because of HI’s practice
local “psych team” in an ambivalent condition (still believed in validity of Open Mole, more than a symbol of MH disorder)
paradox of cultural sensitivity and health system development
Implementation Science
The study of putting something into practice; examining programs’ outputs and outcomes
Kohrt et al.Study
How competent are non-specialists trained to integrate mental health services in primary care?
Findings: general improvement in knowledge, but less impressive in competence (role play)
Recommendations:
1) standardized measure of knowledge and attitudes (more research on stigma and attitudes in order to better select MH staff)
2) standardized measure of competency (standardized role play and observation measure of competency)
3) training and supervision should not rely on number of hours (rather, rely on attaining knowledge and competency)
High-income Individuals in Low-income Countries
often occurs in MH programs
differential access to resources
role of incentives
entry and exit
Summerfield
critical of how humanitarian aid was done
said that trauma treatment was not specific enough and too broadly applied (pseudo-condition)
need to find who is suffering worse and know related factors for effective treatment (trauma is an event, not a condition
Deficit Focus
Looks at what’s wrong