MOD 1 - Esophagus
1/58
Earn XP
Description and Tags
Esophagus
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
where is the esophagus in relation to the trachea
posterior
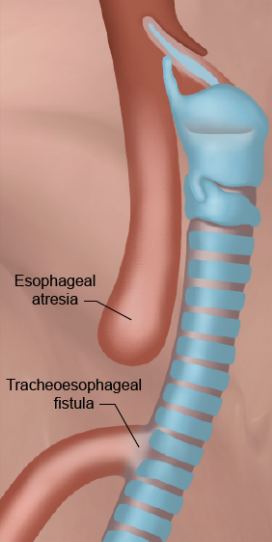
what is Esophageal Atresia with Tracheoesophageal Fistula?
a condition where the fetus’ wall between the trachea and esophagus is incorrectly developed leading to…
a) a blind pouch —> esophageal atresia
b) remain somewhat attached to the trachea forming a tracheoesophageal fistula (TEF).
what is the classification and etiology for Esophageal Atresia with Tracheoesophageal Fistula?
C: congenital
E: may be a link to gene malformations, usually a fistula is associated between the trachea and esophagus
what is the pathogenesis for Esophageal Atresia with Tracheoesophageal Fistula?
when the esophagus and trachea wall fail to form, the organs don’t separate, therefore a fistula occurs @T4 level
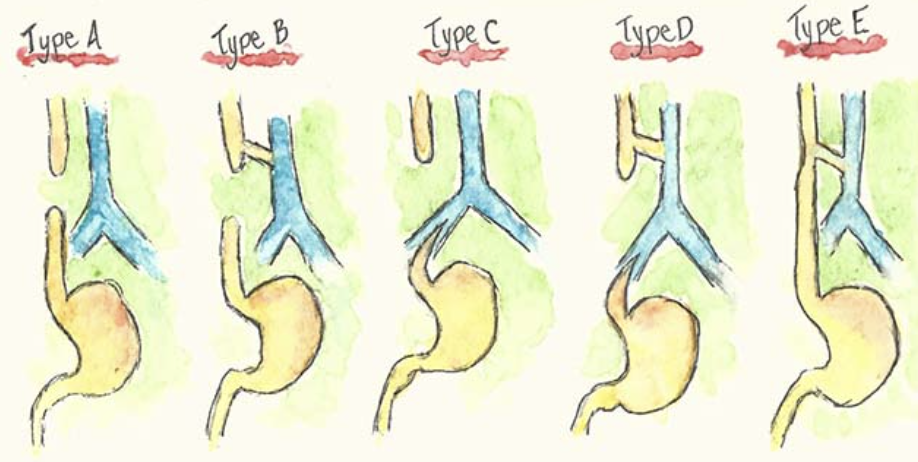
what are the five different types of atresia with and w/o TEF?
Type A: esophageal atresia only. no connection to stomach —> upper esophagus ends in a blind pouch and lower esophagus is sealed. (esophagus not connected).
Type B: upper esophagus connected to trachea, lower esophagus sealed. food and liquid will end up in the lungs
Type C: upper esophagus ends in a blind pouch, lower esophagus connected to trachea. air from trachea can go to stomach.
Type D: upper and lower esophagus connected to trachea. food and liquid will travel to lungs and bowel gas present.
Type E/H: esophagus complete but fistula is formed between esophagus and trachea so food and liquid could still enter into lungs and normal bowel gas patterns as food will enter stomach.
which types of atresia have bowel gas and which types do not have bowel gas?
No bowel gas: Type A, B
Bowel gas present: Type C, D, E/H
which type of atresia is the most common?
type C
what are the S&S of esophageal atresia w/ TEF?
cyanosis, choking, excessive salivation, dyspnea and gagging. Continual suction may be required to prevent aspiration pneumonia. There may be an inability to pass an NG tube into the stomach.
why is extra saliva a sign of esophageal atresia?
because saliva is usually swallowed and with no connection to the stomach, there is no way for the saliva to drain
what is the treatment for esophageal atresia w/ TEF?
aspiration is a major concern, surgical correction is needed. A thoracotomy is usually performed to attach the proximal to the distal esophagus.

RA of esophageal atresia w/ TEF
U/S and MRI can be used to detect this pathology in utero
water soluble contrast must be used for contrast studies
plain x-ray will show bowel gas or not
what is acquired tracheoesophageal fistula?
a TEF that occurs for causes other than congenital development abnormalities.
what is the classification and etiology of acquired TEF?
C: degenerative but also traumatic if an injury was the cause
E: result of malignancy in the mediastinum (majority of cases), trauma, infectious process
what is the pathogenesis of acquired TEF?
In terms of mediastinal malignancy, a tumor may grow large enough to encompass both the trachea and esophagus creating a tunnel between the two structures.
In terms of injury, if the injured area of the trachea or esophagus does not heal properly, it may ulcerate causing a fistula to develop between the two structures.
what are the S&S for acquired TEF?
Hemorrhaging of the fistula may occur causing blood in the sputum, aspiration pneumonia may occur as a result of food and liquid entering the lungs.

RA of acquired TEF
A plain CXR may show air within the mediastinum, if the TEF is a result of malignancy.
Fluoroscopy with water soluble contrast can be used to identify the actual fistula.
treatment of acquired TEF
surgical: treatment plans vary greatly depending on the ability to remove the mass. If so, repairs are done to the existing structures
non-surgical: a stent can be placed in the esophagus to maintain its patency and block off the fistula
what is Zenker’s Diverticulum?
A Zenker's Diverticulum is an outpouching on the posterior wall of the upper esophagus, specifically the hypopharynx, where the mucosa layer has herniated through the muscular layer
what is the classification and etiology for Zenker’s Diverticulum?
C: degenerative (usually occurs ages 40+), inflammatory if food gets lodged causing irritation
E: The mucosal layer of the esophagus herniates through the muscular layer at the bottom of the hypopharynx as a result of of the failure of the cricopharyngeal muscles to contract properly to aid in the swallowing of esophageal contents.
what is the pathogenesis for Zenker’s Diverticulum?
the cricopharyngeal muscles become weak which causes the area above these muscles (the pharyngoesophageal junction) to herniate posteriorly.
contents can get stuck and will not be able to pass through the esophagus
RA for Zenker’s Diverticulitis
barium swallow is the most common modality used
S&S of Zenker’s
urge to clear throat
risk of aspiration (aspiration pneumonia)
treatment for Zenker’s
no treatment unless they cause issues with swallowing
change diet to softer foods, eat slowly
excision of divericula
what is achlasia?
aka cardiospasm or megaesophagus, esophageal achalasia is a condition where the cardiac sphincter (lower end of the esophagus) fails to relax.
Classification and Etiology
C: degenerative neuromuscular
E: obstruction of the distal esophagus caused by degeneration of the nerves controlling the cardiac sphincter. This leads to incomplete relaxation of the cardiac sphincter resulting in incomplete clearing of esophageal contents into the stomach.
pathogenesis of achlasia
gradual degeneration to the nerves
reduced peristalsis in distal esophagus
distal esophagus dilates

RA of achlasia
xray shows widened mediastinum with an air fluid level
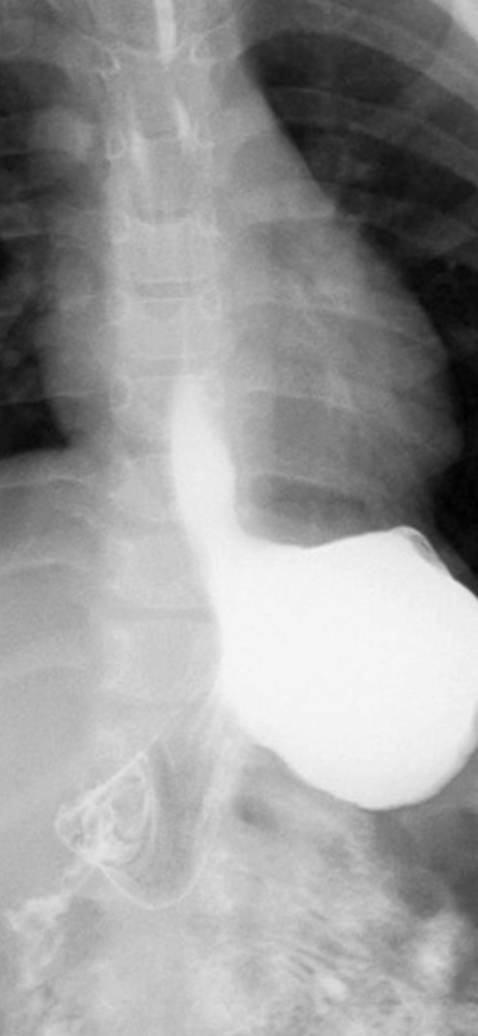
radiographic signs include bird’s beak, string sign or corkscrew esophagus
bird’s beak sign of achalsia
narrowing along the length of the cardiac sphincter

S&S
difficulty swallowing (dysphagia)
substernal pain
regurgitation
some weight loss due to insufficient nutrients
treatment for achlasia
lifestyle adjustments like eat slowly and not eating close to bedtime
meds to relax the cardiac sphincter prior to meals
botox can relax the muscles holding the sphincter shut — last six months and scars
balloon dilation to open narrowed area
myotomy — outer muscular layers of the sphincter are severed
what is GERD also known as
esophagitis
what is GERD
gastro-esophageal reflux disease is the opposite of Esophageal Achalasia b/c GERD is the relaxation of the cardiac sphincter which results in gastric contents to back up into the lower esophagus.
classification of GERD
inflammatory
what is the etiology of GERD
Repeated reflux of gastric contents leads to weakening of the Cardiac Sphincter → this allows for even more gastric contents to enter the lower esophagus causing damage to the mucosal layer.
Ingestion of caustic chemicals and radiation damage due to radiation therapy
pathogenesis of GERD
reflux on a regular basis…
weakens the cardiac sphincter
lower esophagus becomes inflamed then scarred
prolonged contact with gastric secretions can lead to the formation of ulcers within the walls of the esophagus
what is Barrett’s Esophagus?
a result of prolonged contact with gastric secretions causing the destruction of the normal squamous layer of the esophagus, replacing it with epithelial tissue
this area of the esophagus tends to look like stomach tissue. Barrett's Esophagus is a precursor to adenocarcinoma of the esophagus.
S&S of GERD
heartburn,
dysphagia
substernal pain
Some patients with a sliding hiatal hernia also suffer from GERD.
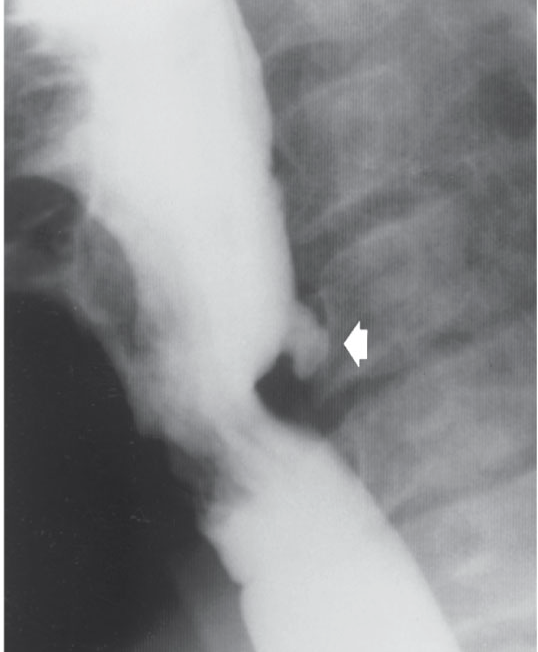
RA of GERD
Barium Swallow with UGI procedure is the standard for assessing GERD
*As GERD progresses, its appearance changes on imaging*
this image is early stage
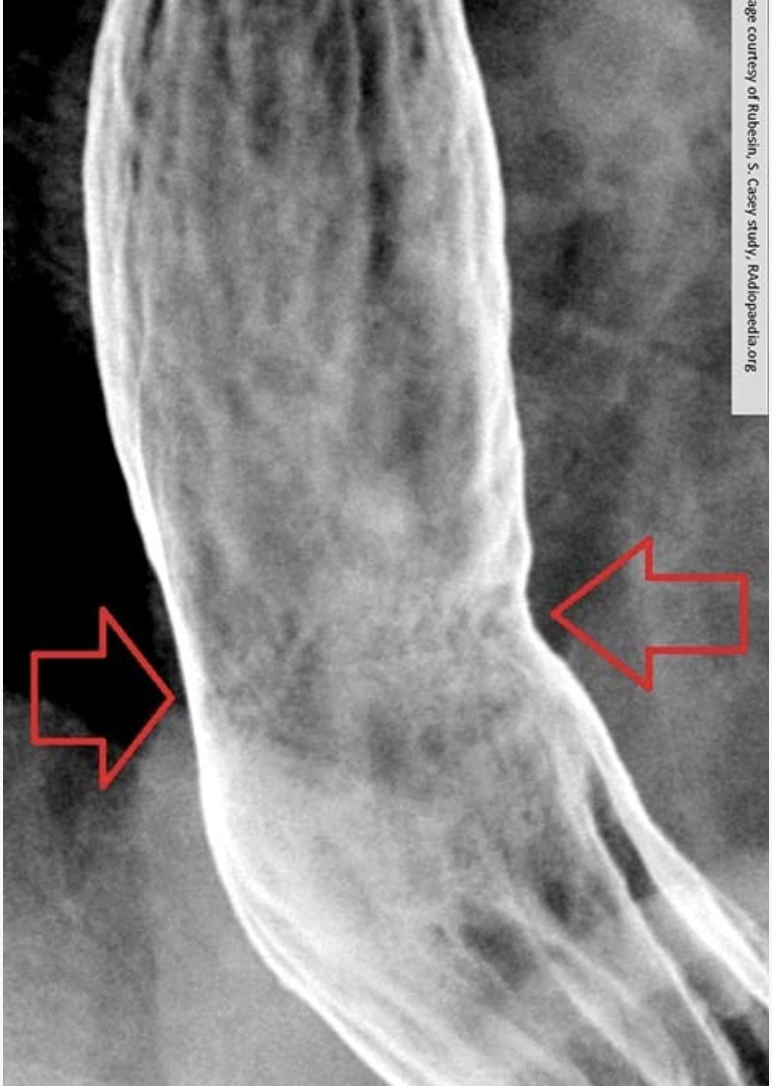
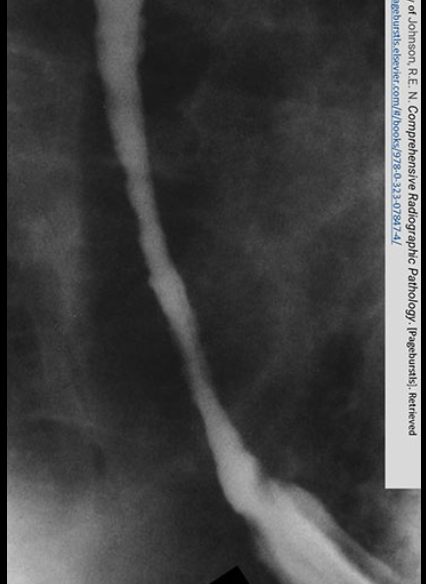
advanced stage of GERD
Obvious narrowing of the lower esophagus due to reflux. Notice the erosion.
what is the water siphonage test
for GERD
included in a UGI to assess reflux
pt drinks barium and is placed LPO and drinks water during fluoro
the rad looks at the cardiac sphincter to see if the barium refluxes while drinking water

treatment for GERD
alterations in diet and eating habits
antacids
surgery — Nissen fundoplication
what is esophageal varices?
the vascular dilation of collateral esophageal veins due to issues with the portal vein. (varices means swelling or enlargement of veins)
Classification and etiology of esophageal varices
C: inflammatory
E:
is a side effect of of liver pathologies (cirrhosis)
when the liver is not working properly, blood backs up into the portal vein → increase in BP (portal hypertension) —> stress on collateral veins —> enlargement
A non-liver related cause of portal hypertension is occlusion of the portal vein via thrombus.
pathogenesis of esophageal varices
when the portal vein blood flow is impeded, it will go around the blockage by using collateral veins
the collateral veins are not designed for high pressure so they enlarge
swelling causes impressions
pts usually present with co conditions like GERD
RA of esophageal varices
barium swallow will show the impact
endoscopic U/S can diagnose
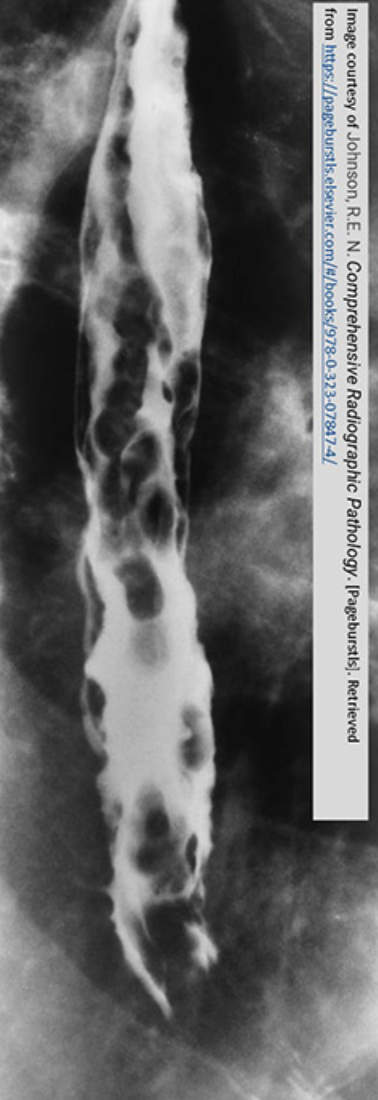
radiographic signs XR
rosary beads (oval filling defects)
worm tracings (long wavy impressions)
S&S of Esophageal varices
asymptomatic until veins rupture or bleed
similar to GERD symptoms
treatment of esophageal varices
vasoconstrictors
sclerotherapy
balloon tamponade for active bleeding of the esophagus
a shunt (TIPS) to open up portal vein
what is a hiatus hernia
when the diaphragm bulges through the diaphragm and into the chest cavity
classification of HH
degenerative as it typically occurs ages 50+ and is due to muscle weakening
etiology of HH
weakened phreno-esophageal ligament allows for a portion of the stomach to slip through the esophageal hiatus of the diaphragm and into the thoracic cavity.
difference between HH and diaphragmatic hernia
HH = only a portion of the stomach passes esophageal hiatus
Diaphragmatic hernia = entire stomach
pathogenesis of HH
phreno-esophageal ligament weakens, may dilate, allows for the stomach to slip through the esophageal hiatus
what are the two types of HH?
sliding HH = slides freely thru esophageal hiatus (certain actions or movements like coughing can help show the pathology)
paraesophageal HH = a portion of the stomach remains above the diaphragm at all times (no sliding)
what is the real danger of HH?
if the stomach twists while in the thoracic cavity — called a gastric volvulus
all other complications are due to reflux
S&S of HH
often asymptomatic
symptoms that are experienced are due to the relfux
treatment of HH
modifying eating habits and lifestyle, antacids, quitting smoking and drinking and sleeping in a position where the head is elevated above the stomach.
surgery for more severe cases
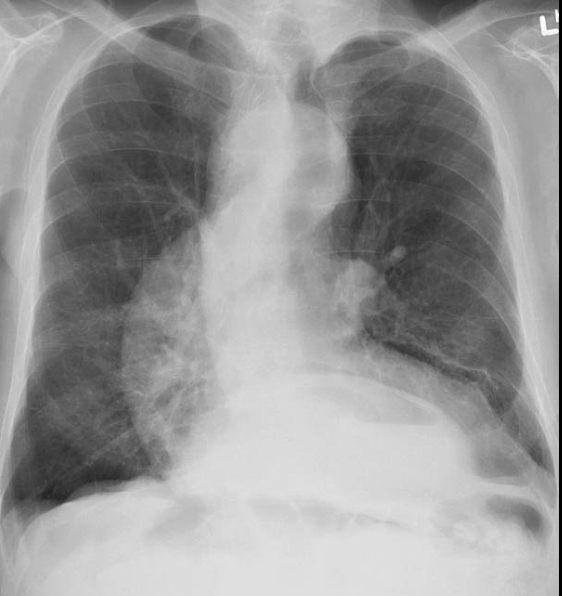
RA of HH CXR
large HH can show on CXR as a mass behind the mediastinum
RA of HH on BS or UGI
barium swallow and UGI will show smooth esophagus and stomach with rugae patterns (roughened structure above diaphragm)
