BC4 - glucose, electrolytes, minerals, urea, creatinine.
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
RECAP
Describe homeostasis of glucose
IN THE LIVER :
Alpha cells release GLUCAGON to increase glucose levels when low
Beta cells release INSULIN to decrease glucose when levels are high
What triggers :
glycogenolysis
gluconeogenesis
catecholamines, glucagon
cortisol, glucagon
both are inhibited by insulin
How can we sample the level of glucose in blood?
take a fasted sample
use serum or plasma, separate from cells within 1h.
Use Na fluoride tube → glucose stable for 3 days.
List some possible causes of hypogylcaemia
^ insulin
v gluconeogenesis / glycogenolysis
^ glucose utilisation
Iatrogenic
List some possible causes of hyperglycaemia
Physiological
postprandial, stress, dioestrus
Diabetes mellitus
endocrinopathies, insulin resistance
iatrogenic
What level of glucose in the urine counts as ‘glycosuria’ in the dog / cat?
10mmol/l dogs
13-16mmol/l cts
What is the most common cause of glycosuria in dogs vs cats
dogs - diabetes mellitus
cats - stress
Why do we test for ketoamines?
glucose levels fluctuate and are affected by stress - not super reliable
ketoamines are only elavated if constant hyperglycaemia
Name two ketoamines
fructosamine
glycated haemoglobin
Describe fructosamine
irreversible linking to plasma proteins (albumin) affected by albumin conc
reflects glucose conc over 2-3 weeks
hyper and hypo-thyroidism cause altered rate of protein turnover
Describe glycated haemoglobin
irreversible linking ot haemoglobin, affected by haemoglobin concentration
reflects blood glucose conc over 2-3 months
What can cause hyponatraemia through na+ containing fluid loss
Renal losses
hypoadrenocorticism
diuretics
Extrarenal losses
vomiting
diarrhoea
third space loss
skin loss
what can cause hyponatraemia through water retention?
odemas
CHF, hepatic cirrhosis, CKD
innapropriate ADH secretion
polydipsia
administration of na+ poor fluids
What are other causes of hyponatraemia
hyperglycaemia - increased plasam osmolarity
uroperitoneum
k+ depletion
Through what mechanism do hypotonic fluid losses cause hypernatraemia
renal losses
kidney disease
osmotic diretics
postobstructive diuresis
Extrarenal losses
diarrhoea / vomiting
thirds space loss
phosphate enema
Through what mechanism does pure water loss / inadequate intake cause hypernatraemia
water deprivation, hear stroke, fever, burns, diebetes insipidus, primary adisia.
What other causes for hypernatraemia are there?
salt poisioning, hypertonic saline, hyperaldoseronism, SAMPLE dehydration
Na+ and Cl- fluctuate together.
Corrected Cl- = normal Na+ / measured Na+ x Measured Cl-
What does it mean if the corrected Cl- is altered
the problem is with chlorine itself, not Na+
What can cause decreased altered chlorine?
lipaemia, vomiting, loop + thiazide diuretics, chronic respiritory acidosis, hyperadrenocorticism, glucocorticoids.
What can cause increased corrected chlorine levels?
KBr, spironolactone, fluid therapy, diarrhoea, chronic respiratory aklalosis, diabetes mellitus, hypoadrenocoricism, CKD, renal tubular acidosis.
How is potassium regulated
dietary intake
distrobution between ECF nad ICF
epinephrine, insulin, hyperkalaemia promote uptake into cells
renal excretion
excretion, reabsorbtion, secretion by principle cells (promoted by aldersteone)
What three things can cause hypokalaemia, expalin these.
decreased intake
prolonged anorexia, K+ poor fluids
shift from ECF to ICF
metabolic acidosis, insulin administration, IV glucose admin, catecholamines
renal losses
osmotic diuresis, renal tubular disease, CKD in cat, postobstructive diuresis.
ketonuria
GI losses
vomitig / diarrhoea
What three things can cause hyperkalaemia, expalin these.
shifting from ISF to ECF
metabolic inorganic acidosis
haemolysis
tissue necrosis
decreased renal excretion
renal disease
urinary tract obstruction
hypoadrenocorticsm
other
drugs, increased intake
What are the three major measures of Ca ++
free (ionised) - 50% biologically active
bound to anionic proteins - 45% bound to albumin
bound to non-protein anions - 5% citrates, phosphates, lactate
What Ca++ measuremnt is most informtive?
free (ionised) Ca++
List some causes of hypocalcaemia
Iatrogenic - contaminaton, phosphate enema
Hypoalbumiaemia
Hypoparathyroidism
Inadequate mobilisation from bone
Inadequate digestion from GI
List some casues of hypercalcaemia
increased PTH or PTHrp
decreased urinary excretion
increased vitamin D
bone leions, haemoconcentraion
What are the three major measurements of Phosphorus (PO4)
free / ionised - 55%
nonprotein cations - 35%
catanionic proteins - 10%
How is phosphorus regulated?
renal clearance,
absorption in intestines
reabsorption from / depostion into bone
shifting between ECF → ICF
list some causes of hypophosphataemia
Increased urinary excretion eg diuresis, hyperparathyroidism
Shift from ECF to ISF eg hyperinsulinism, respiratory alkalosis
decreased intestinal absorbtion
defective mobilisation from bone eg eclampsia in dogs
list some causes of hyperphospahaemia
Decreased urinary exxcretion eg lowGFR, obstruction
Increaed intestinal absroption eg hypervitaminosis D
Shift from ICF to ECF eg tumour lysis syndrome
other - hypethyroidsm in cats, hyperadrenocorticism in dogs
What can cause an increase in creatinine?
decreased excretion (pre, post, renal)
high muscle mass, increased protein intake
What can cause a decrease in creatinine
reduced muscle mass
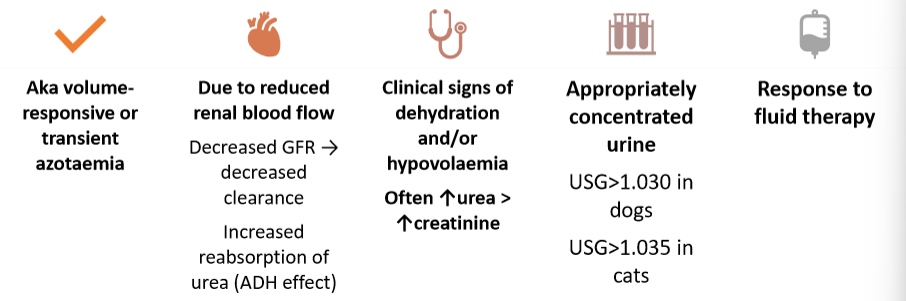
What are the signs of prerenal azotaemia
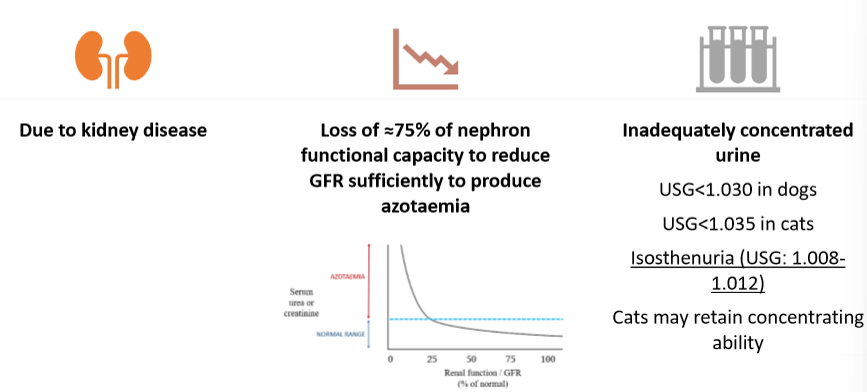
What are the signs of renal azotaemia
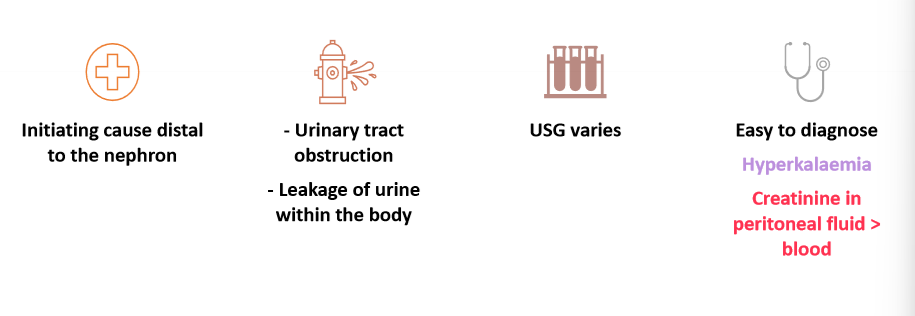
What are the signs of postrenal azotaeamia