L2: Animal Models of Medial Temporal Lobe Amnesia
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
After discovery of memory deficits in HM, what did attention turn to
trying to identify the particular regions within the medial temporal lobe that were critical for memory function
What is needed to study the specific parts?
Animals models
with lesions of different brain regions
Why are animal models useful
Have similar neuroanatomy and neurophysiology to humans
Allows us to conduct experimental manipulations not possible on humans
Specific lesions
control over when lesions occur
control over the stimuli to be remembered and when they occur relative to lesions
we know what we presented them, so know what they should be able to remember
single-unit recordings
pharmacological manipulations
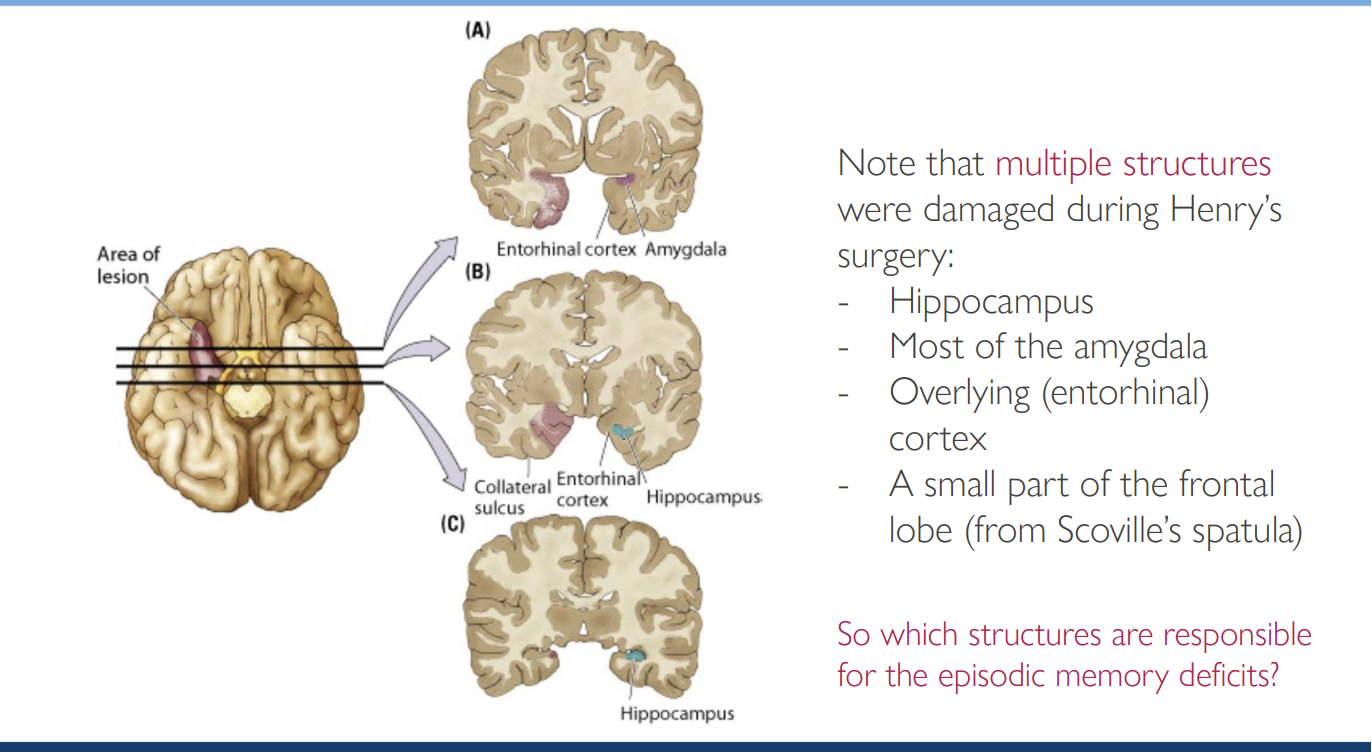
What deficits do we need to model to model patient HM
Imparied in declarative/explicit memory
Intact short-term memory
Normal intellectual function
Preserved capcity for some forms of learning (e.g procedural learning)
Where did initial animal model studies has lesions in
Hippocampus
How to measure memory if animals cannot talk? (and affects on Hippocampal lesions)
Association task
Delayed non-matching to sample task
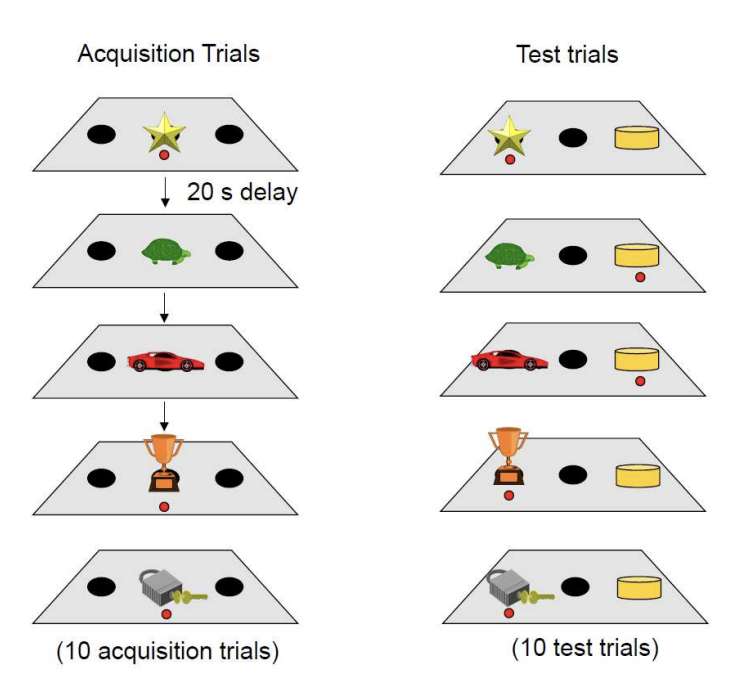
Association task procedure
Acquisition trial
present with object
some get a reward and some do not
acquire the memory of the objects that are associated with reward
Test trial
test with multiple objects
animals should pick the object that was preivously associated with the reward
Results of association trials in hippocmapal lesion models
association was unimpaired
basically like controls
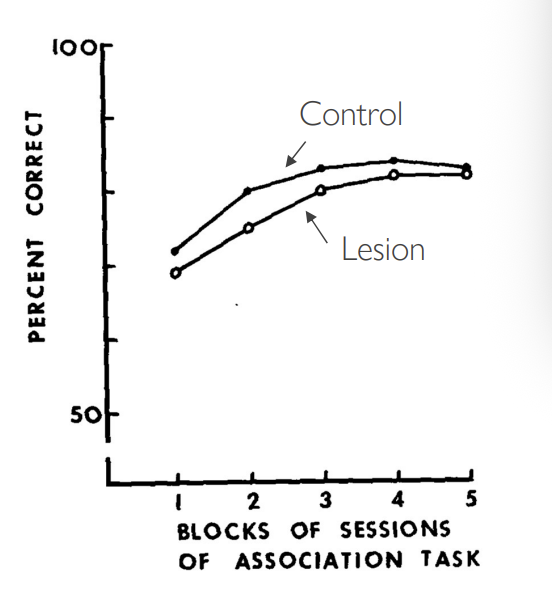
Why did hippocompal lesions leave performance on the association task unimpaired
Associative memory
memory of what went together with an item
exists to e.g associate a stimulus and reward
Assoiciative memory is more to do with the amygdala?
Hippocampus is needed for recognition memory instead?
Solution to these results
need to test instead for recognition memory:
Ability to judge familiarity of an item
exists to discriminate familiar vs novel items
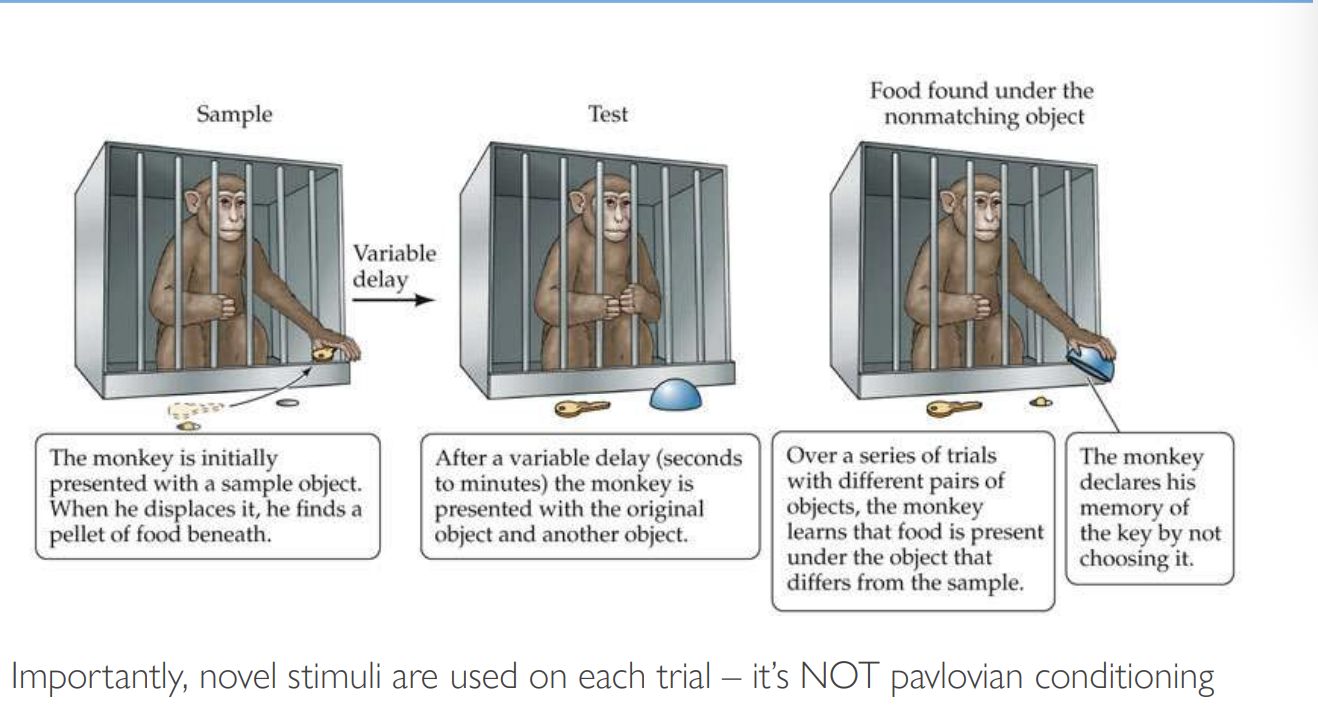
Delayed non-matching to sample test: testing recognition memory
Developed by Gaffan and Mishkin and Delacour
Sample
presented with sample object
gets reward hidden in the well if displaces the object
Test
Screen lowered between monkey and test tray
variable delay (minute or seconds)
presented with original object and another object
Food found under the non-matching object
learns that food is present under the object that differs from the sample
Therefore is recognising the known object and choosing a new one
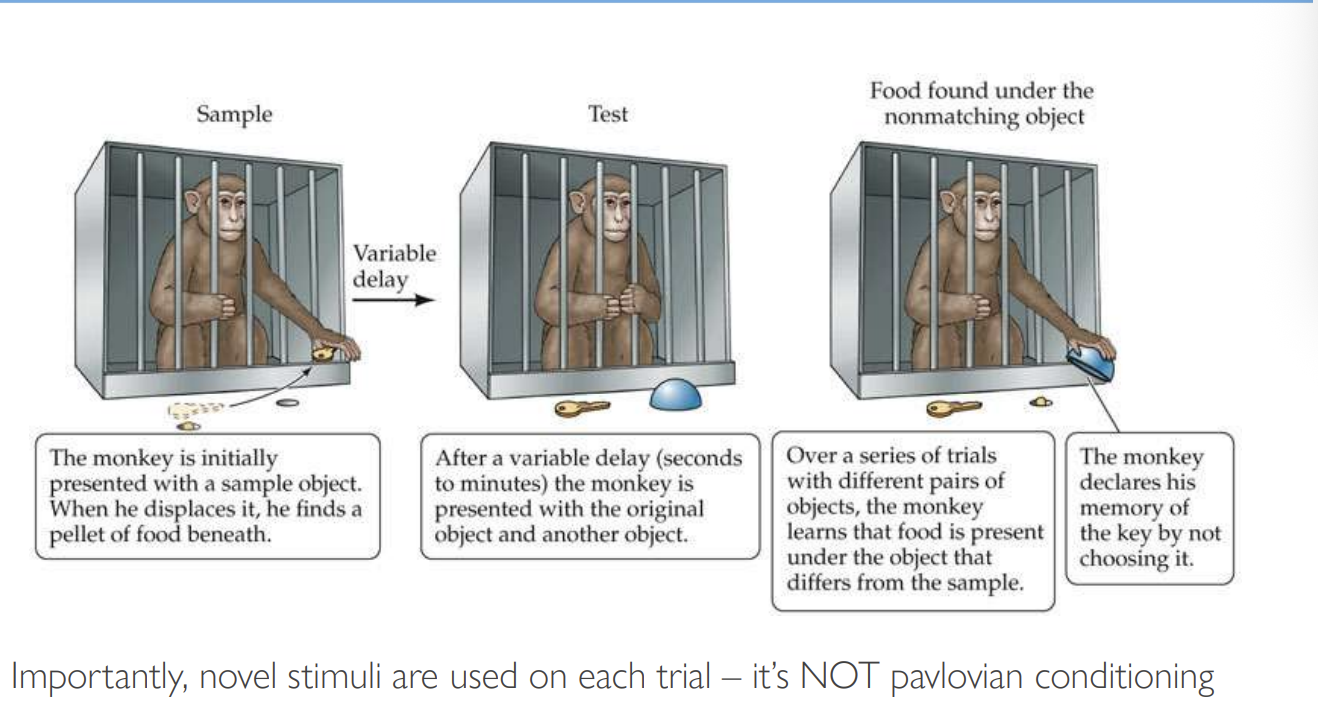
How is this test not pavlovian conditioning?
a novel stimulus is used on each trial
After the DNMS rule has been mastered, recognition memory abilities typically are evaluated by what
Increasing the delay intervals interposed between the sample presentation and choice test
Increasing the number of items to be remembered

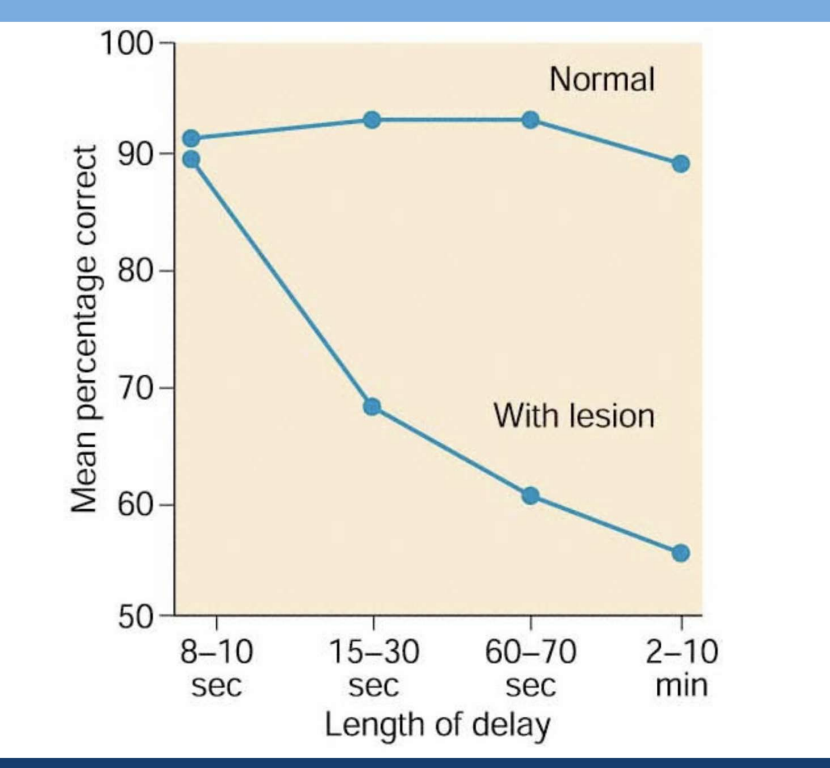
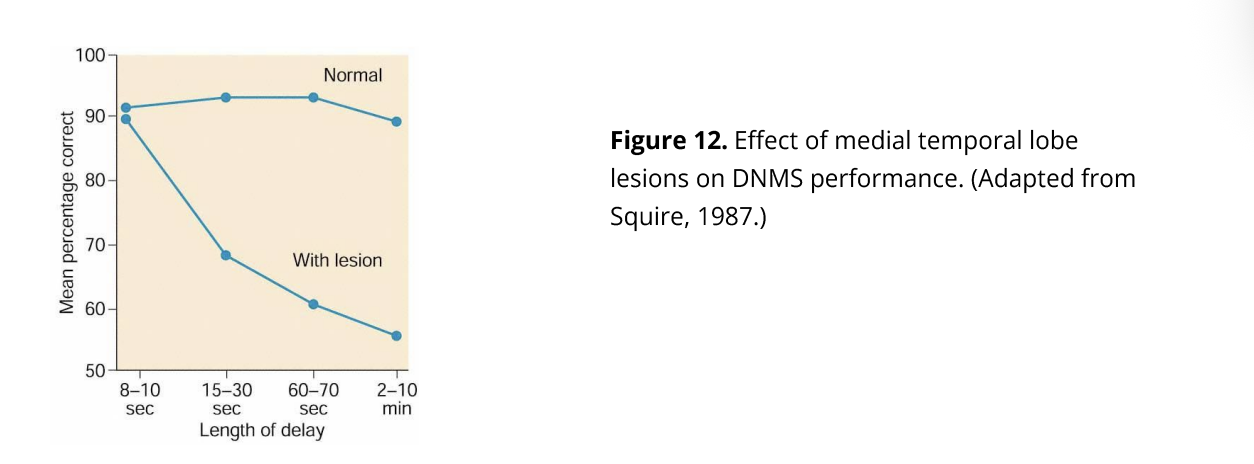
What were the results of the DNMS on general MTL lesions in monkeys? And how did this model HM?
Impaired performance of the DNMS
8-10 seconds→ no deficits
HM: similar to the short term memory of HM
Delay dependent effect→ more deficits
However, the next question to answer…
What specific structures in the MTL are supporting recognition memory?
How was this question addressed
Different surgical lesions on different parts of the MTS:
Bilateral aspiration of hippocampus
bilateral aspiration of amygdala
combined bilateral aspiration lesions of amygdala and hippocampus
Allowed postoperative recovery
Procedure of how these lesioned monkeys were tested
retained on DNMS at the 10 second delay (note: trained before surgery as a control)
memory challenged by increaing delay to 30,60 and 120 seconds
challenged further by increasing number of objects to be remembered
3,5,19
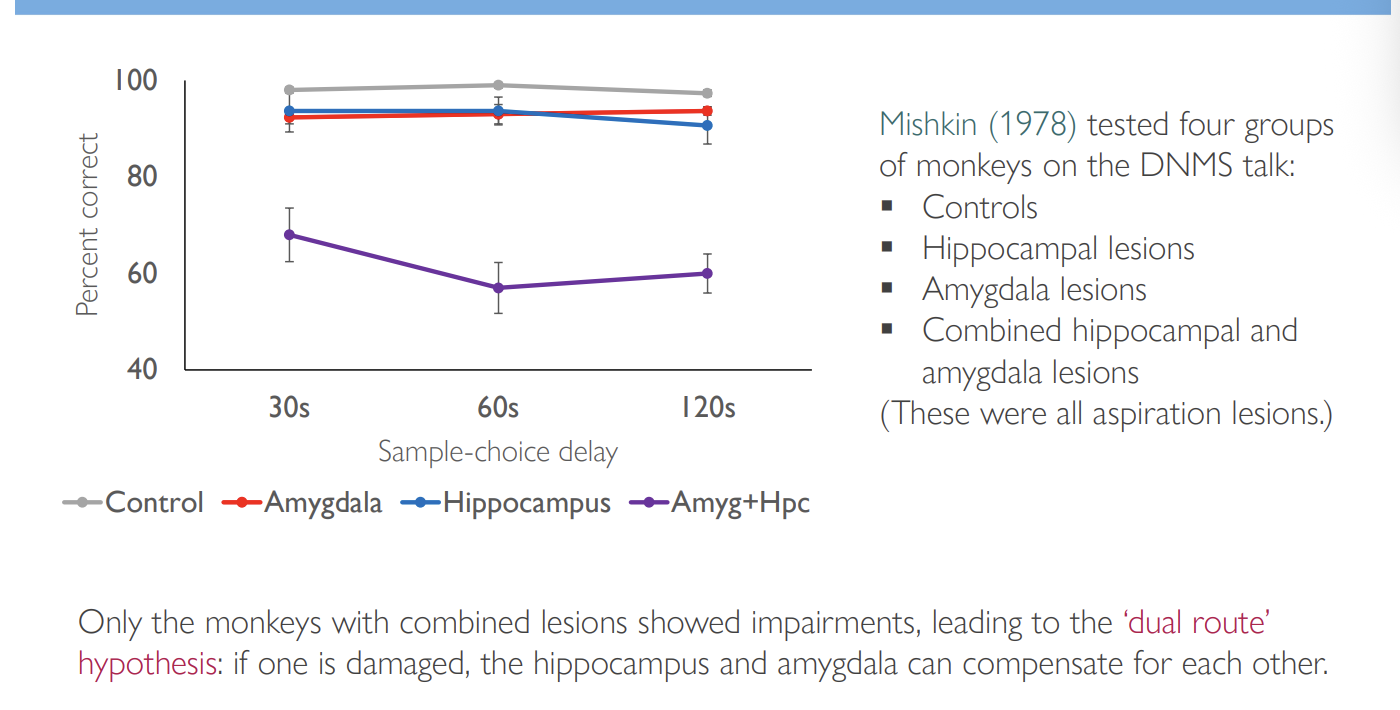
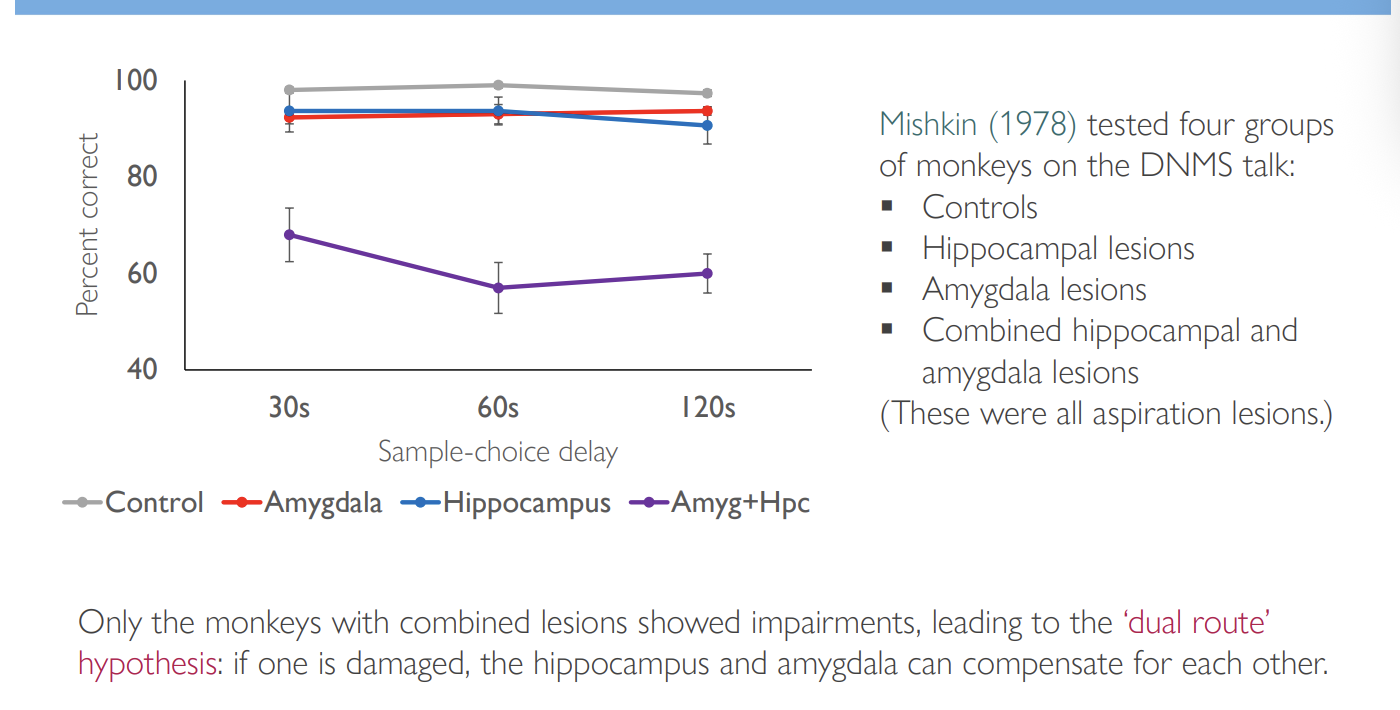
Results
Hippocampus alone→ negligible defects
Amygdala alone→ negligible defects
Combined→ severely impaired and severely deteriorated very rapidly across delays:
If retrained→ could do 10 second delay accurate
but 30 second delay→ 70% correct
and hardly any more for longer delays
Critique→ already down to 30 seconds in the normal results???

What did Mishkin conclude from this
Dual route hypothesis:
if one is damaged, the hippocampus and amygadala can compensate for eachother
How did this explain the lack of deficits in early experiment that removed the hippocampus
suggests that the surgical approach spared the amygdala
so the amygdala could compensate for the lack of hippocampus?
So did Mishkin find a good model for HM? (How this model matched HM)
impaired on several different memory tasks but ability to acquire motor skills was intact
Evidence: Barrier motor skill taks, lifesaver motor-skill task
perform as control even after a month
Impairment in memory included modalities other than vision:
tactile recognition memory also impaired
Therefore: fitted HM’s global (polymodal) amnesia

Overall Mishkin’s model has all the hallmarks of a good animal model of amnesia
Short term memory intact
Long-term memory for new info disrupted
Skill learning was preserved
No obvious deficits in intellectual function
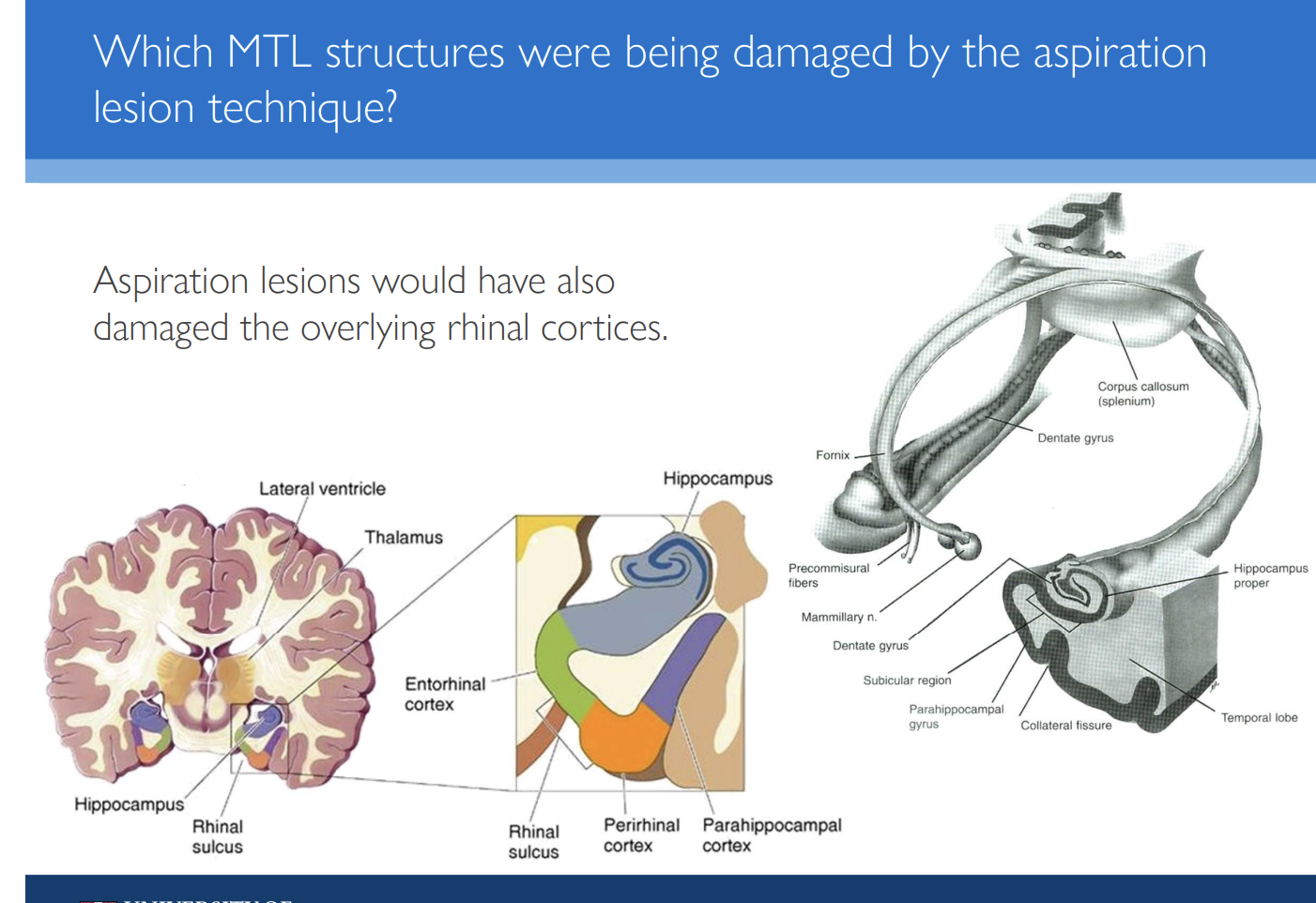
Problem with the model→ use of aspiration lesions
Removal via pumping sections out:
Causes some damage to brain strucutures outside the amygdala or hippocampus:
perihinal cortex
parahippocampal cortex
Entorhinal cortex
Why was this damaged deemed unimportant at first?
damage not consistent from subject to subject → so would even out across data
removal of hippocampus and amygdala were required to produce memory impairment
any damage to anything else could be contributing to the memory impairment
Evidence that the extra damage is causing memory deficits: 1 Mishkin
Damage to Rhinal cortex (Rhinal sulcus)→ Entorhinal and perirhinal cortical areas:
Result:
Amygdala + rhinal cortex damage→ severe amnesia
Hippocampus + rhinal cortex damage→ much less severe impairment
Suggests: amnesia produced with damage to amygdala alone if rhinal was also damaged
Amygdala intact + damage to rhinal + hippocampus→ memory spared
Suggests: critical neural substances for memory in MTS are
amygdala and rhinal cortex
(not the amygdala and hippocampus)

Evidence that the extra damage is causing memory deficits: 2 (conflicting) Squire
damage amygdala + spared overlying cortex→ no memory deficits
Conclusion:
hippocampus + adjacent cortical areas→ ‘medial temporal lobe memory’ system is critical to memory
Evidence that the extra damage is causing memory deficits: 3
Two later studies:
Damage to perirhinal cortex alone (no amygalda or hippocampus damage)→ severe amnesia
Were is the rhinal cortex found?
In the ventral visual system

Next questions to answer
Is the rhinal cortex simply providing info to other MTL structures, or supporting memory in its own right?
Does the amygdala and hippocampus make unique contribution to memory?
maybe temporal cortical ablations impair memory because they are removing input to the amygdala and hippocampus??
With what help could this questions be answered
Development of surgical methods → Excitotoxic lesions
development of Magnetic resonance imaging (MRI)

Alvarez experiment with new technology (1)
lesions limited to hippocampus→ significant DNMS deficit
Crituque:
note: still quite small compaired to temporal cortical removal
only present at long delays between 10 to 40 mins
Image:
did not impair familiarity judgments?
In contrast: Murray and Mishkin (2)
Used MRI and neurotoxic lesions
Amygdala→ no effect on DNMS performance
Hippocampus→ not effect on DNMS performance

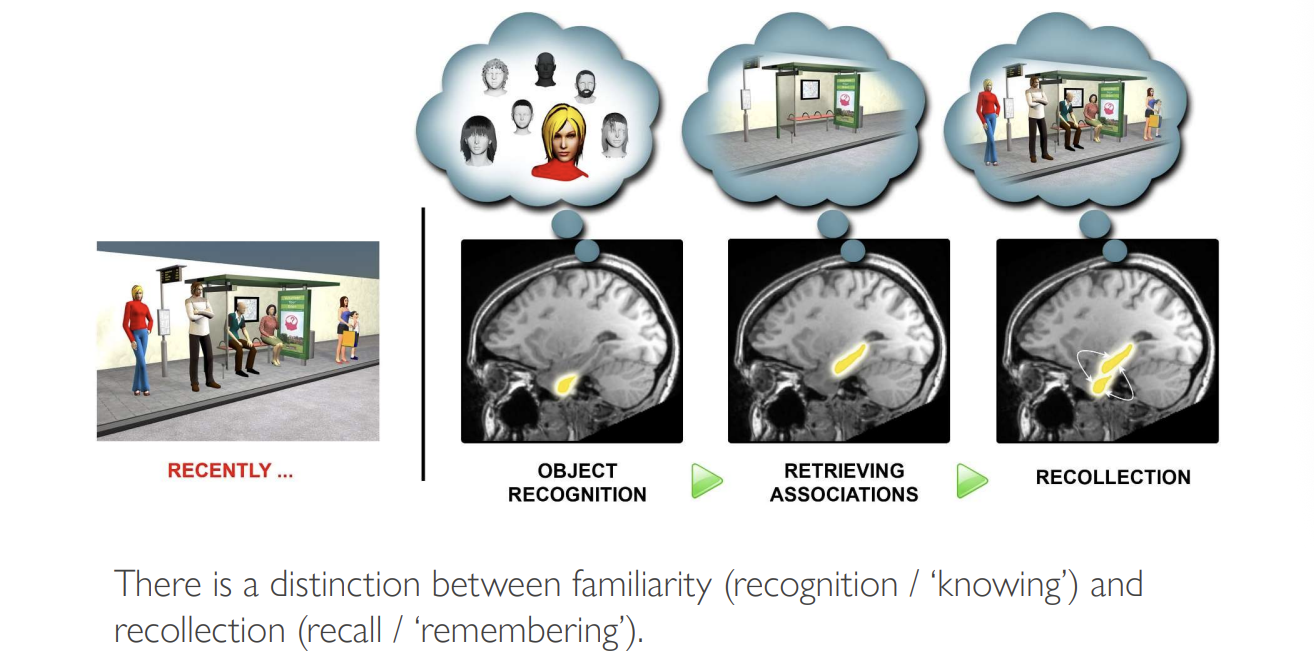
What are the perirhinal cortex and hippocamus contributing to DNMS performance: need to may a distinction between Familiarity and recollection
Familiarity:
recognition/ ‘knowing’
e.g you recognise a person but do not know where they are from
Recollection
recall/ ‘remembering’
e.g you recognise and recollect where they are from
Taking this into account: hippocampal damage results in
no impairment to familirarity judgments

Squire’s group found what
regardless of the lesion hippocampal damage always produced deficits on DNMS at delays of 10 mins or longer
Conclusion:
hippocampus might be needed for DNMS at longer delays?

Therefore what are the conclusions overall?
whether hippocampus contributes to recognition memory is still controversial
note: this is when modelling HM
But this does not match up with patient RB
Patient RB→ developed amnesia after ischamic accident
Selective damage to subregion of hippocampus→ CA1 subfield
no damage to rhinal cortex
Results: impaired DNMS
this has been modeled in monkeys and rats
What doesn’t match up to previous model:
how can lesions to one small region of hippocampus lead to deficits on DNMS
BUT
removing entire hippocampus→ no deficits
Investigating this: modelling RB and full hippocampal lesions in rats and performing DNMS
Learn DNMS
Ischemia induced
some have full hippocampal lesion some have just a region
Result:
Full→ DNMS intact
Region→ DNMS impaired
What did Baxter and Murray find in the relationship between hippocampal lesion size and DNMS impairment?
Hippocampal lesions:
Small hippocampal lesions→ more impaired on DNMS
compared to larger more complete hippocampal lesions→ less impairment on DNMS
negative correlation between hippocampal and DNMS
Rhinal cortex lesions:
Increased Rhinal cortex damage→ increased DNMS impairment
Positive correlation between rhinal and DNMS

Hypothesis of these results
Ischemia leads to ‘covert damage’:
neuropathy not due to loss of neurons→ so does not become apparent sing standard histological techniques
Other histopathological techniques reveal wide-ranging changes after ischaemia
What do wide-ranging changes were shown to have happened when looking at different histopathological techniques
Damage to Cingulate cortex
hyperexcitablility of surviving nuerons
loss of expression of certain proteins normally seen in certain populations of hippocampal cells
How does this ‘covert damage’→ confirmation in rats
Experiment and observation:
removal of hippocampus one hour after ischaemia prevents a deficit from occurring
Hypothesis of what is happening:
Ischemica→ cells in the hypothalamus die
abnormal firing or epileptiform activity
this alters the function of distant brain regions without causing cell loss:
e.g rewiring of the rhinal cortex
so does not look damaged but actually is
Overall explanation of the earlier studies being misleading in terms of contribution of the amygdala and hippocampus and the relative importance of the adjacent cortical areas (2)
Methods used to ablate amygdala and hippocampus damaged some perirhinal cortex during surgery
(More important) Amygdala and hippocampal lesions also damaged white matter tracts in the temporal lobe
this disconnets the temporal cortical areas from important afferent and effeerents and disabling their functions
(even though the cortex itself was still structurally intact)
Overall conclusion
DNMS have been used to model animal recognition (declarative) memory deficits observed in human amnesic patients
Early (aspiration) lesions
showed that recognition memory depends upon the MTL (possibly hippocampus and/or amygdala)
More specific lesioning techniques
showed rhinal cortex was important for recognition of memory
(not the hippocampus and/or amygdala)

So what does the hippocampus do?
see next lecture
Beyond the MTL memory system: damage outside of the temporal lobe can also produce what
Impairments in recognition memory
Why is this not surprising
given that patients with Korsakoff’s syndrome have memory impairments consequent to diencephalic damage
rather than medial temporal lobe damage
Studies in monkey have shed light on the neuroanatomical basis of amnesia in these cases:
Large midline thalamic lesions in monkeys lead to large deficits in DNMS
These lesions damage the anterior and dorso-medial nuclei of the thalamus
→ produces retrograde degeneration in the mammillary bdies
Bilateral lesions limited to either dorso medial nuclei or anterior nuclei produce
→Milder effects
Lesions to mammillary bodies alone
aslo produce mild deficits