N470: Cerebral perfusion (exam 2)
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
Elements of neuro assessment
- Level of consciousness
- Pupillary reaction
- Vital signs (MAP)
Examples of motor impairments (5)
- apraxia- cannot execute movement
- ataxia- poor coordination
-Dyskinesia- impaired voluntary movement
-Hemiplegia
-Nystagmus
Examples of sensory impairments (2)
-Anesthesia
-Paresthesia
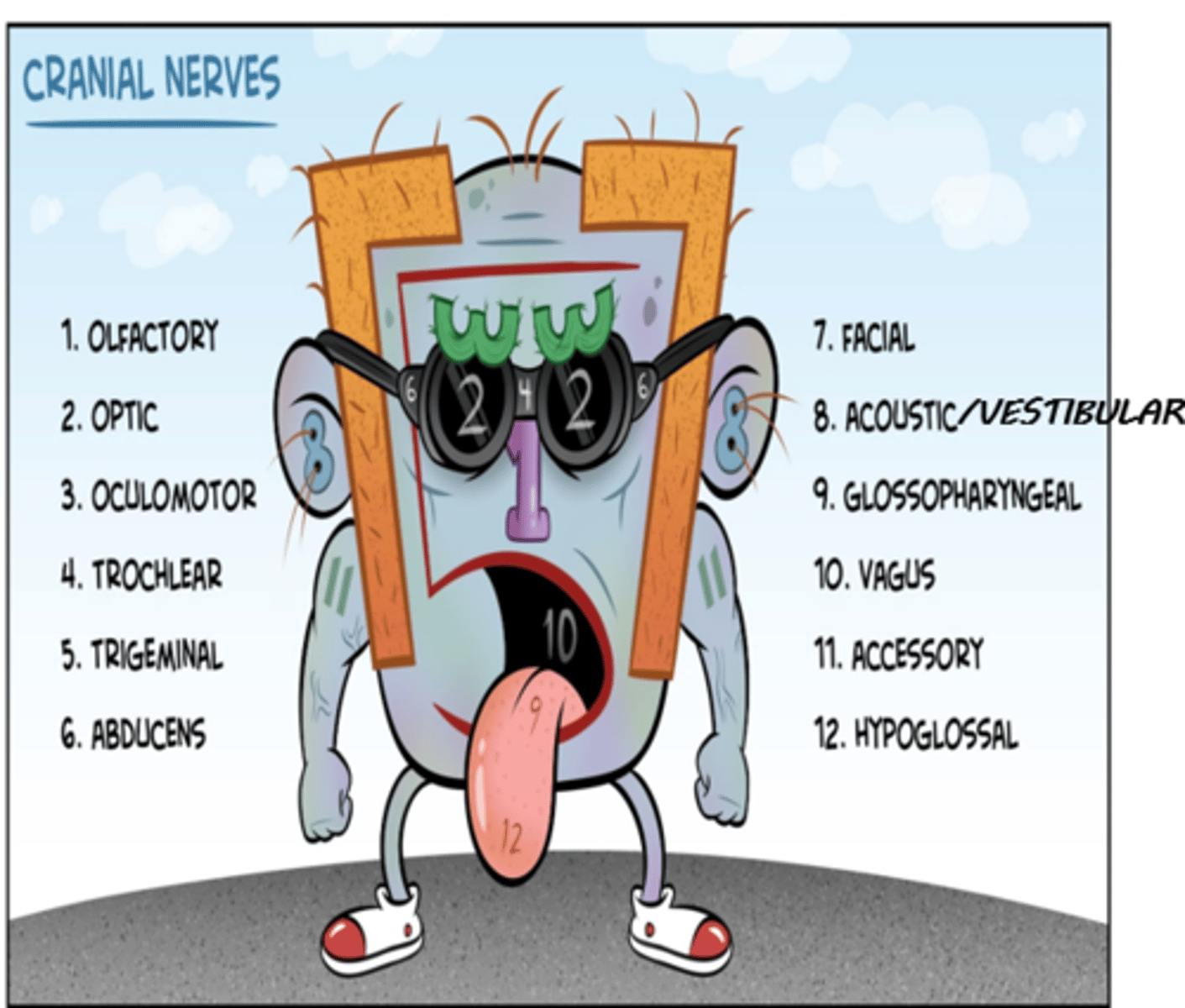
cranial nerves
I- olfactory (sensory)
II- optic (sensory)
III- oculomotor (motor)
IV- trochlear (motor)
V- trigeminal (both)
VI- abducens (motor)
VII- facial (both)
VIII- acoustic/vestibular (sensory)
IX- glossopharyngeal (both)
X- vagus (both)
XII- accessory (motor)
XII- hypoglossal (motor)
(Oh Oh Oh To Touch And Feel Very Good Velvet AH)
AND
(Some say marry money but my brother says big brains matter most)
Olfactory (I) function
sensory: smell
Optic (II) function
sensory: vision
oculomotor (III) function
motor: eye movement
trochlear (IV) function
motor: downward and outward eye movement
trigeminal (V) function
sensory: face, sinuses, teeth
motor: muscles of mastication
Abducent (VI) function
motor: outward eye movement (abducts eye)
Facial (VII) function
Sensory: taste
Motor: facial expression, salivation
vestibulocochlear (VIII) function
sensory: hearing and balance
Glossopharyngeal (IX) function
motor: pharyngeal muscle
sensory: posterior tongue, tonsils, pharynx
Vagus (X) function
motor: heart, lungs, bronchi, GI tract
sensory: heart, lungs, bronchi, trachea, larynx, pharynx, GI tract, external ear
Accessory (XI) function
Motor: neck and back muscles
Hypoglossal (XII) function
motor: tongue muscles
Which populations have the highest risk for TBI?
- 75+ yo
- males
PRIORITY neuro assessment pieces for TBI
1) Airway
2) breathing
3) circulation
Airway assessment for TBI (4)
- C-spine precautions
- Loose teeth, vomitus, bleeding obstruction
- edema, neck swelling
- LOC
Breathing assessment for TBI (5)
- Skin color
- Breathing spontaneously
- Respiratory rate/pulse oximetry/ ETCO2
- Chest rise/fall symmetric
- Breath sounds
Breathing assessment for TBI (4)
- Skin color/ temperature
- Pulse
- Blood pressure
- Obvious bleeding
What tool do we use to assess LOC?
Glasgow coma scale
Three categories assessed with GCS
- eye opening
- verbal response
- motor response
How is eye opening scored on GCS?
4: Spontaneous
3: To command
2: To pain
1: None
How is verbal response scored on GCS?
5: Oriented
4: Confused conversation
3: Inappropriate words
2: Incomprehensible
1: None
How is motor response scored on GCS?
6: Obeys command
5: Localizes pain
4: Withdraws from pain
3: Abnormal flexion to pain
2: Abnormal extension to pain
1: None
Mild head injury GCS score
GCS 13-15
Moderate head injury GCS score
GCS 9-12
-mortality 2.5%
Severe head injury GCS score
GCS 3-8
-GCS 5-8 - 12% mortality
-GCS 3-5 - 60% mortality
-GCS 3 - 80% mortality
If over 60 y.o. mortality 75% for any severe head injury
Causes of altered cerebral perfusion (10)
- trauma
- stroke
- tumors
- aneurysms
- seizures
- infections
- hypertension
- hypotension
- drugs
- cardiopulmonary bypass
two types of traumatic brain injury
blunt and penetrating
traumatic brain injury with no opening in the skin or communication with the environment; motor vehicle crash, assault, fall
blunt traumatic injury
traumatic brain injury in which a foreign object penetrates the body; gunshot, stabbing, impalement
penetrating traumatic injury

Examples of blunt traumatic injury
- Skull fracture
- Concussion
- Contusion
- Hematoma (Epidural, Subdural, Intracerebral)
- Diffuse axonal injury (DAI)

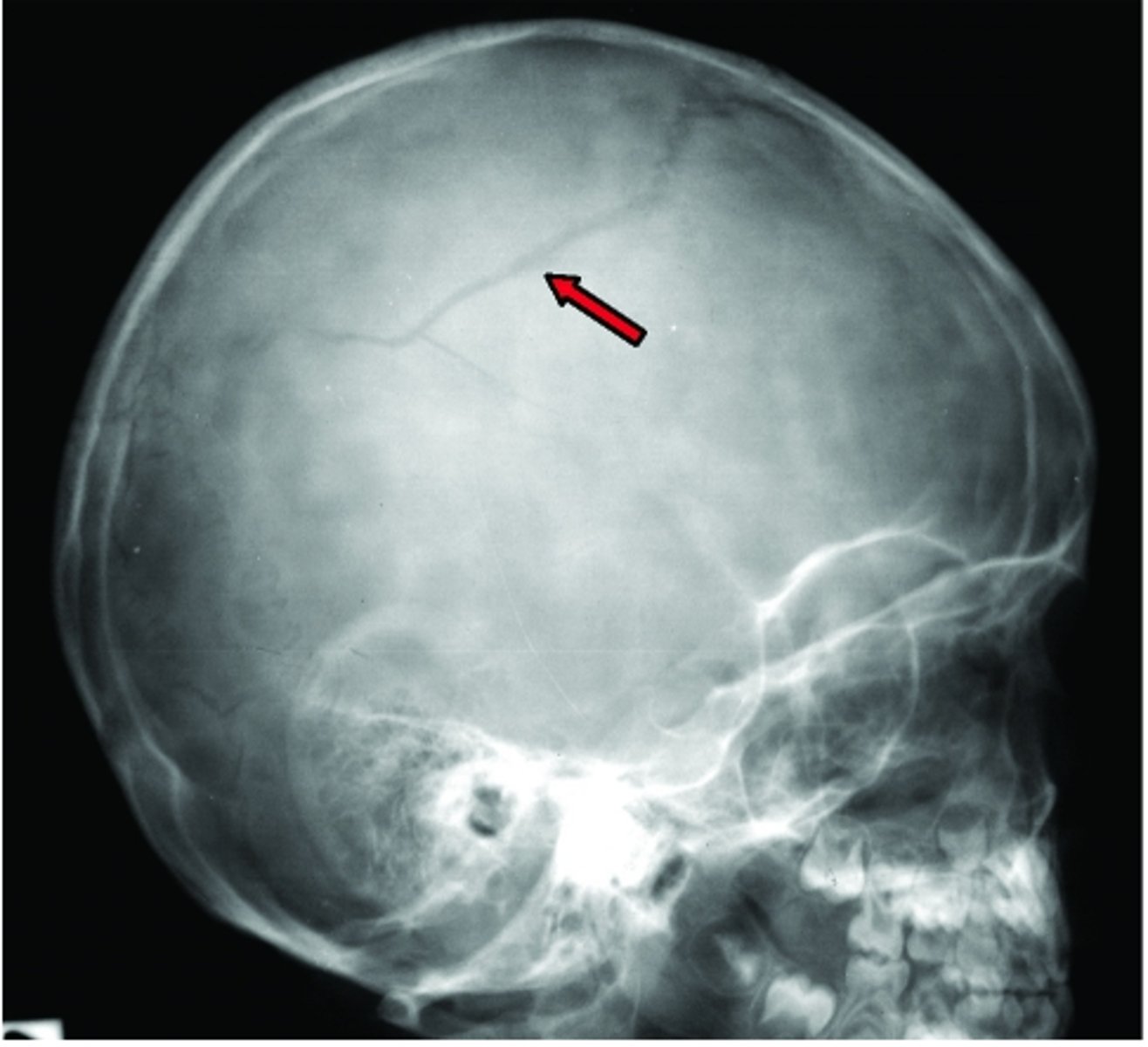
Skull fracture types (5)
linear, depressed, comminuted, simple, compound, basilar
skull fracture type- A break in the bone but no displacement; usually from low velocity injury
linear
skull fracture type- Inward indentation of the skull, requires a powerful impact
depressed

skull fracture type- Can be linear or depressed; no fragmentation or communicating lacerations; from low/moderate impact
simple
skull fracture type- Multiple linear fractures with fragmentation of bone into many pieces; from direct, high momentum impact
comminuted
skull fracture type- Depressed fracture and scalp laceration with communicating pathway into the intracranial cavity, severe injury
compound
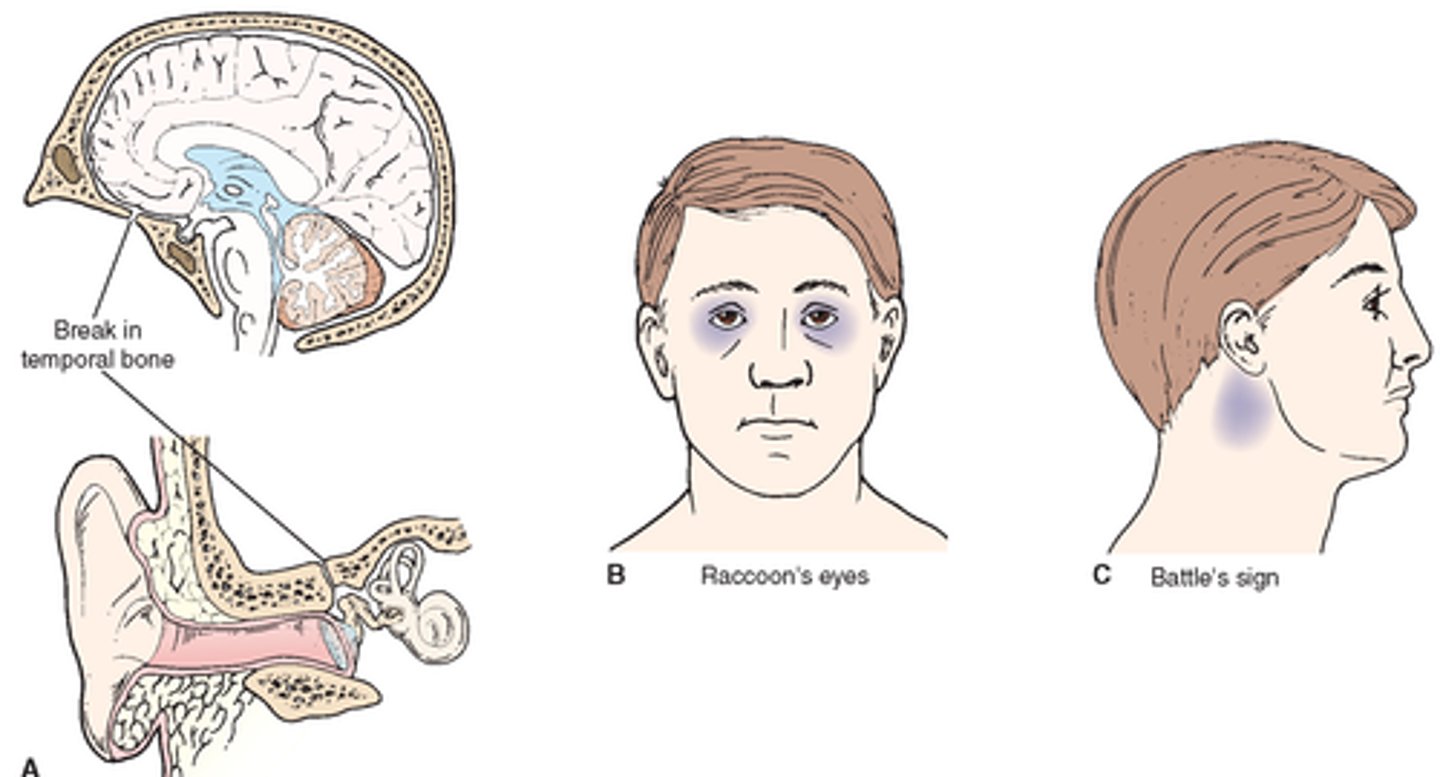
signs of a basilar skull fracture
1. Raccoon eyes
2. Battle sign- bruising behind ears
occurs after blow to the head hard enough to move the brain within the skull
concussion
occurs after a more severe injury when the brain rebounds against the skull from the force of a blow (a beating with a blunt instrument). Injury is directly beneath the site of impact.
contusion
How does a CT scan look for a concussion vs a contusion
Concussion: cannot see
Contusion: may see diffuse bleeding
Shearing damage to the pathways (axons) that connect the different areas of the brain; this occurs when there is twisting and turning of the brain tissue at the time of injury; brain messages are slowed or lost, torn axons cannot be repaired
Diffuse axonal injury (DAI)
a victim of assault who has been hit in the head with a baseball bat would most likely suffer which type of injury?
a) penetrating injury
b) deceleration injury
c) acceleration injury
d) rotational injury
c) acceleration injury- caused by movement of the brain within the unrestrained head (whiplash injury)
Types of stroke (+ which is most common?)
ischemic (most common) and hemorrhagic
causes of hemorrhagic stroke
- Aneurysms
- Drugs
- Hypertension
causes of ischemic stroke
- drugs
- hypotension
Which populations have the highest risk/incidence for stroke?
- 65+ yo
- stroke belt- southeastern US
types of ischemic stroke
- thrombotic: begins with a clot
- embolic: clot on the move
types of hemorrhagic stroke
- subarachnoid hemorrhage- rupture of stressed vessel, aneurysm or vascular malformation
- intracerebral
Stroke assessment (7)
- decreased consciousness, changing personality
- drooping mouth & eyelid
- paralysis or weakness on one or both sides
- arm Drift, possible seizures
- pupillary changes & B/P HR RR
- nausea & Vomiting
- pain
Stroke assessment tools (2)
- BE FAST- balance, eyes, facial droop, arm drift, speech difficulty, time to call
- National institute of health stroke scale (NIHSS)- higher number = more severe stroke
How is a stroke diagnosed? (7)
- CT Scans
- MRI
- Lumbar Puncture
- Doppler Ultrasonography & Duplex Imaging- assessing for Carotid Artery Disease, DVT; SAH: transcranial doppler for vasospasm
- Echocardiogram - PFO or other abnormalities
- 24 hours of continuous cardiac monitoring - paroxysmal atrial fibrillation
- CT Angiography - Assessing for Vasospasm
Medical management for a stroke (6)*
1) Optimize cerebral oxygenation – “maintain a patent airway”- restore cerebral blood flow!
2) Manage BP and Temp
3) Minimize risk of stroke recurrence–anti-coagulant, anti-platelet meds
4) Prevent aspiration
5) PT/OT as soon as possible
6) Seizure precautions
medical management of ischemic stroke (4)
1) Infusion of (rtPA) tissue plasminogen activator within 3 hours of onset
2) Mechanical Thrombectomy (surgical coil retriever or aspiration device)
3) Anticoagulant Medications
4) Cerebral Edema - Mannitol
Medical management for hemorrhagic stroke
- prevent vasospasm
- prevent obstructive hydrocephalus
- surgery- craniotomy, craniectomy, aneurysm clipping/coiling
- burr holes
how to prevent vasospasm in hemorrhagic stroke patients?
1) calcium channel blockers: Nimodipine, Verapamil injection
2) triple H therapy: Hypertension, hypervolemia, hemodilution
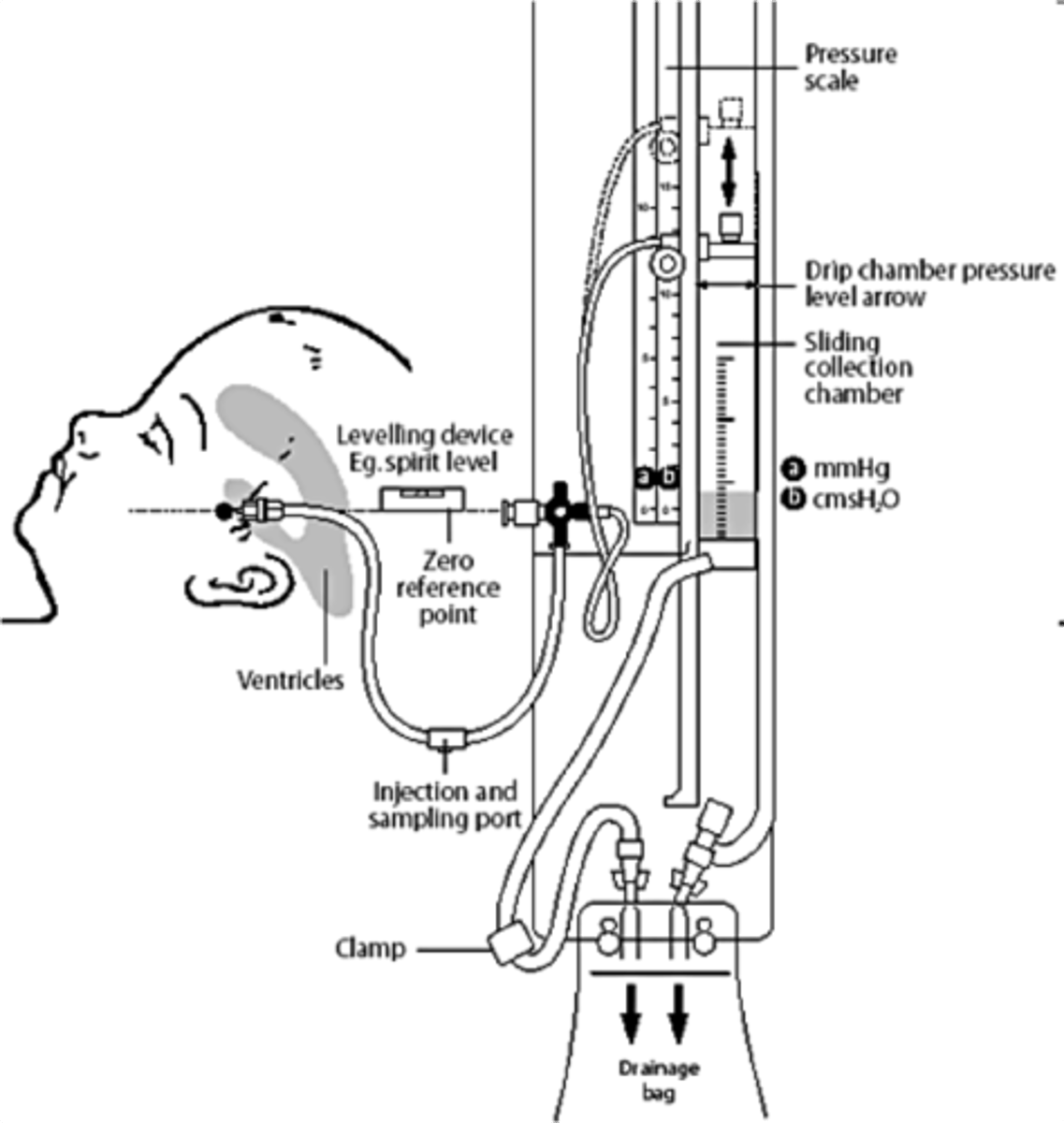
Medical management of Obstructive Hydrocephalus from hemorrhagic stroke
External Ventricular Drain (EVD) AKA "Ventriculostomy"
craniotomy vs craniectomy
Craniotomy-Bone flap returned
Craniectomy-Bone flap NOT returned
aneurysm clipping vs coiling
clipping- more durable
coiling- minimally invasive, shorter recovery time
Is the epidural hematoma a venous or arterial bleed?
arterial
what is the most common source of an epidural bleed?
middle meningeal artery?
Why does the epidural hematoma form the shape of a lens (convex) on CT/MRI?
The expansion stops at skull's sutures, where the dura mater is tightly attached to the skull.
bleeding Between the skull and the outer endosteal layer of the dura mater
epidural hematoma
sources of epidural hematomas (4)
-Temperoparietal locus (most likely) - Middle meningeal artery
- Frontal locus - anterior ethmoidal artery
- Occipital locus - transverse or sigmoid sinuses
- Vertex locus - superior sagittal sinus
Symptoms of an epidural hematoma
finish
Is the subdural hematoma a venous or arterial bleed?
venous
Is the subdural hematoma acute, subacute or chronic?
finish
Are acute hematomas a surgical emergency?
finish
Bleeding between the dura and the arachnoid layers
Subdural Hematoma
Source of Bleed in a Subdural Hematoma
bridging veins
How does a Subdural Hematoma appear on a CT?
Crescent-shaped
symptoms of a Subdural Hematoma?
Gradually increasing headache and confusion
bleeding into the subarachnoid space.
Subarachnoid Hemorrhage
causes/ risk factors for a SAH?
-Smoking, heavy drinking, illicit drugs
-Genetics
-People between 30 and 40 years of age
-More common in women than men - unknown etiology
tests for SAH diagnosis
CT, CTA
Lumbar Puncture
MRI (later)
Treatment for a SAH
finish
Nursing care for SAH
finish
Other than trauma what causes an intracerebral bleed?
abnormalities of blood vessels like aneurysm or angioma
What is a brain shear?
finish
Internal bleeding can occur in any part of the brain
intracerebral hemorrhage
Shear forces from brain movement commonly cause vessel laceration and hemorrhage into the ______________.
parenchyma
A subarachnoid hemorrhage is the accumulation of blood between the:
a) dura and the arachnoid layers of the meninges
b) dura mater of the skull
c) parenchyma of the brain
d) meningeal arachnoid layer and the brain
d) meningeal arachnoid layer and the brain
diffused axonal injury occurs when the brain:
a) twists and turns during time of injury
b) shifts forward and back during injury
c) experiences coup-contrecoup injury
d) bleeds below the Dural layers of the brain
a) twists and turns during time of injury
A diffuse axonal injury may be difficult to visualize on a CT/MRI because:
a) the shearing is too small to notice
b) the injury does not disrupt the structure of neurons
c) it can occur without bleeding
d) this type of injury is not serious
c) it can occur without bleeding
The skull is a rigid compartment filled to capacity with essentially non-compressible contents; If volume rises in one compartment, there must be a decrease of volume in one of the remaining compartments for pressure to remain unchanged
Monroe-Kellie hypothesis
what are the components inside the cranium, and how much space do they take up? (Monroe-Kellie hypothesis)
Brain 80%
Blood 10%
CSF 10%
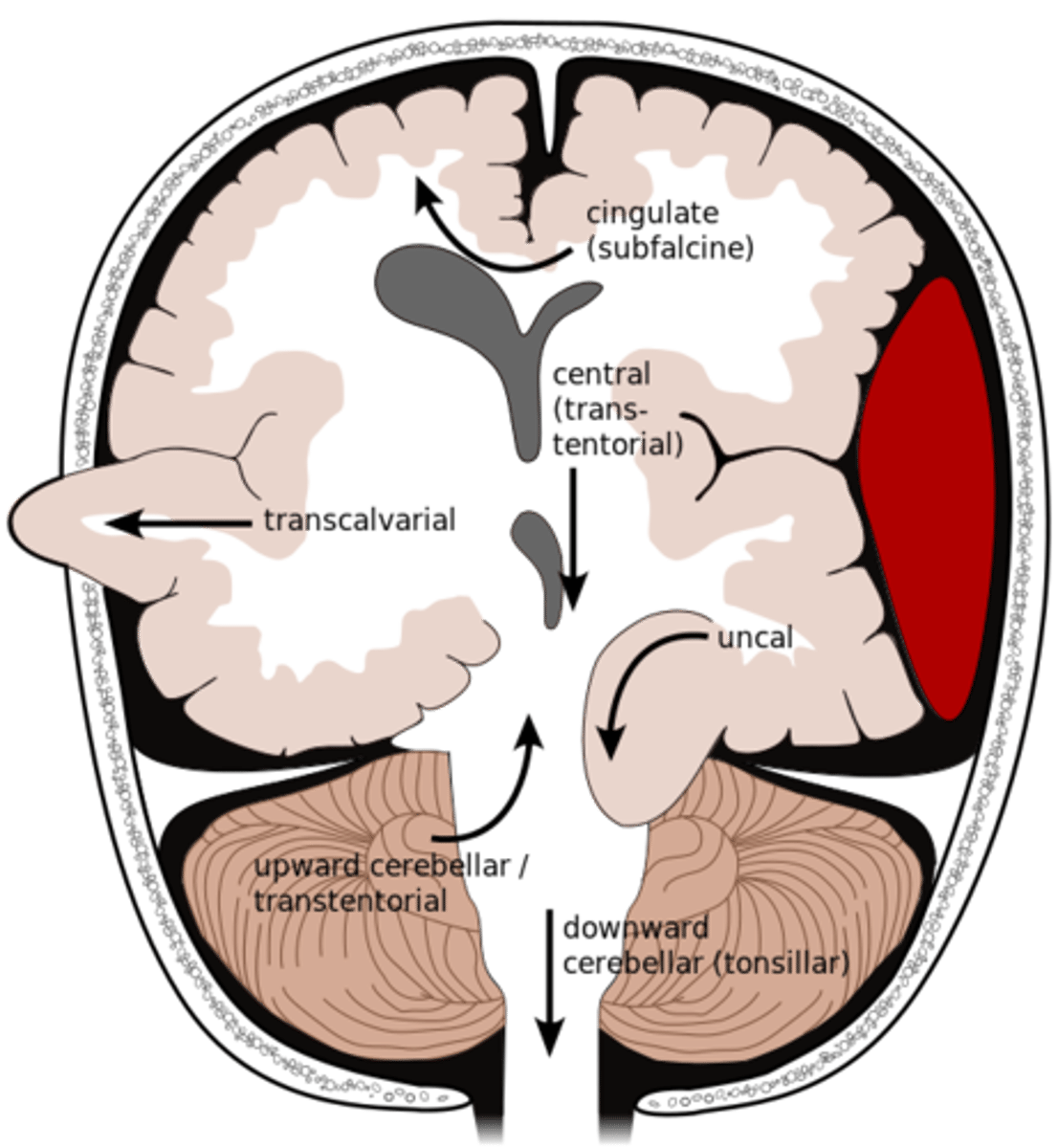
Types of brain herniation (6)
-Midline shift
-Uncal/Lateral (only time where pupillary changes are first sign)
-Transtentorial/Central
-Through Fracture
-Foramen Magnum (deadly)
-Space-occupying
normal ICP
0-15 mmHg
increased ICP
Persistent increase ≥20 mm Hg for >5 min
ICP must be maintained within normal limits to maintain adequate _____
CPP
a compensatory mechanism to keep cerebral blood flow constant; Cerebral blood vessels automatically constrict or dilate to maintain adequate cerebral perfusion pressure (CPP); MAP, CO2 & O2 levels drive this process
Auto-regulation
In auto-regulation, cerebral blood vessels constrict with ______ MAP, but dilate with _____ MAP; as CO2 rises and/or O2 falls, cerebral blood vessels _______ .... and vice versa
In auto-regulation, cerebral blood vessels constrict with high MAP, but dilate with low MAP; as CO2 rises and/or O2 falls, cerebral blood vessels dilate …. and vice versa
what is the zero point for the ICP transducer on the ventriculostomy?
lateral ventricles (tip of the ear)
CPP (cerebral perfusion pressure) formula*
CPP= MAP-ICP
MAP formula*
(SBP + 2DBP)/3
Normal CPP*
80-100 mmHg*
What does a CPP blow 70 lead to?*
ischemia and death*