Lecture 34: Visual Pathways
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
-ganglion cell axons exit retina via optic disk
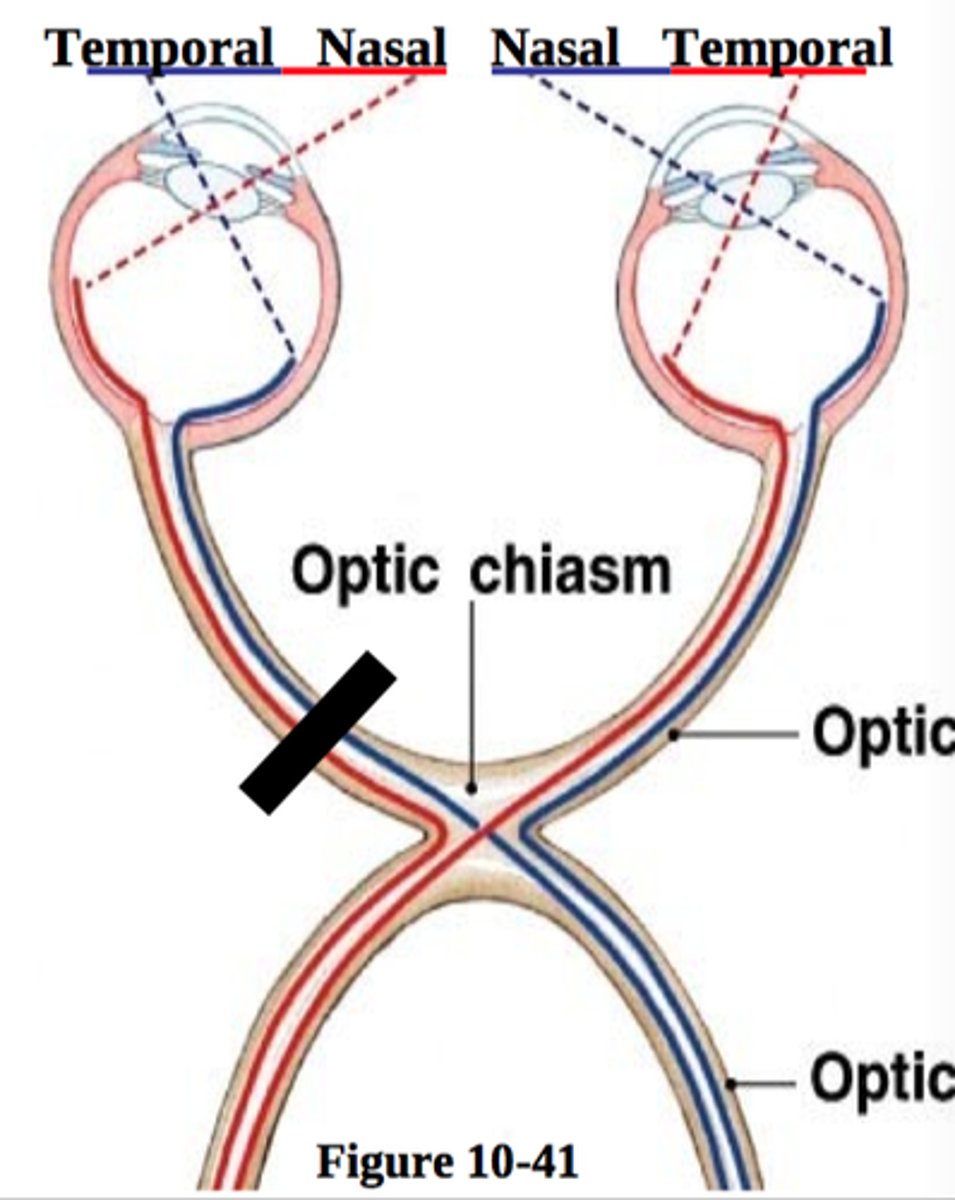
-axons bundle to form optic chiasm
-optic nerve travels posterior to optic chiasm
-bilateral ganglion axons form optic tract
-travels to many different nuclei
Describe the primary visual pathway:
Retinogeniculostriate Pathway
-primary visual pathway
-sends info from the retina to the LGN to the striate cortex
retino-hypothalamic pathway
-pathway that coordinate structures controlled by circadian rhythms
-sends info from the retina to the hypothalamus
Tectal system
-pathway that coordinates head/eye movement towards the visual targets
-sends info from retina to the superior colliculus
pre-tectal system
-system that coordinates pupillary light reflex
-sends info from retina-->neurons in pretectum-->edinger westphal nucleus
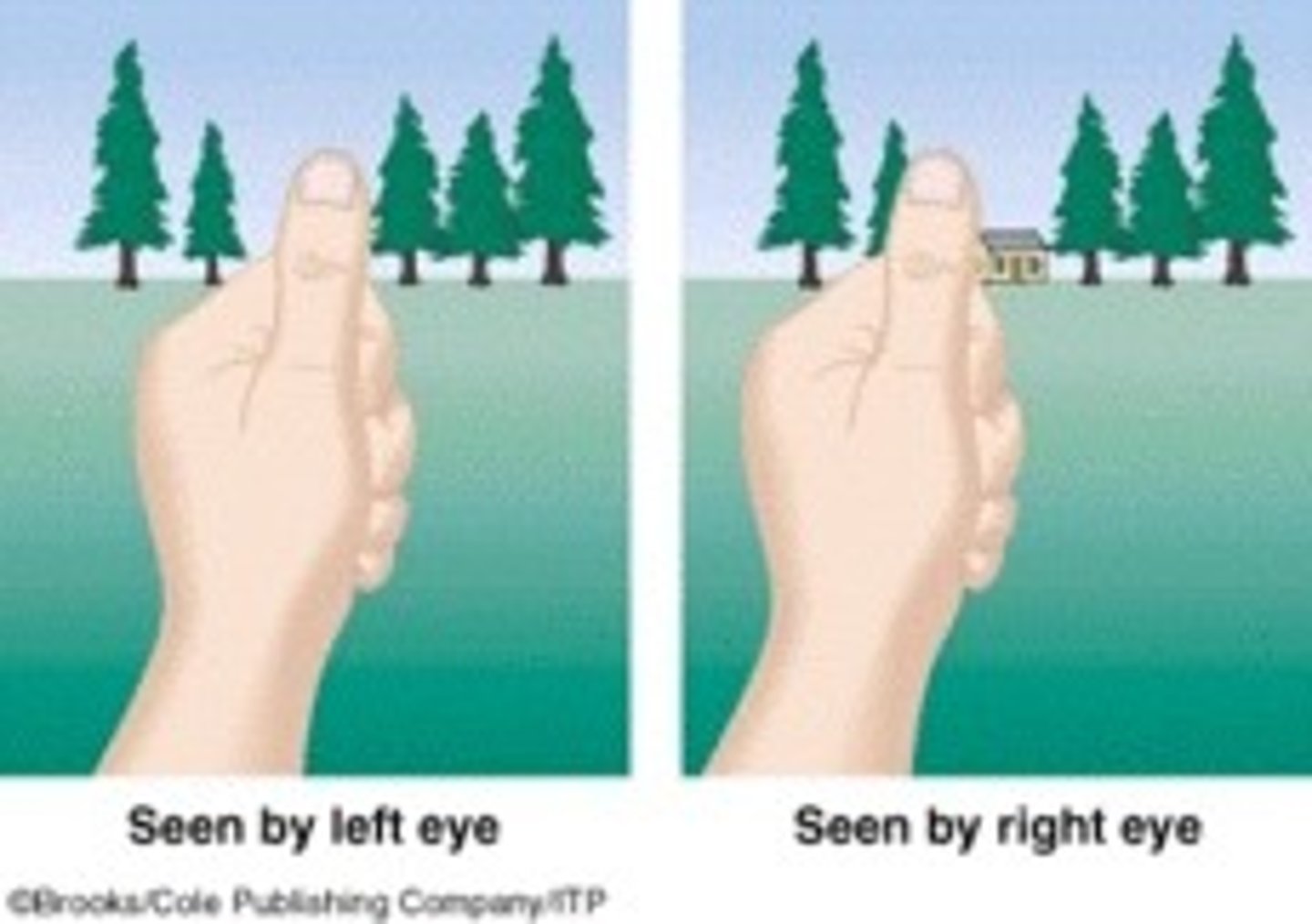
nasal visual field
for each eye individually, the part of the visual field on the same side of the eye as the nose
temporal visual field
Part of the visual field closest to the ears
retinotopic organization
-map established in LGN and maintained in projections to striate cortex
•Posterior - foveal/macular regions
•Anterior - peripheral regions
striate cortex organization:
below
upper visual field projects _____ the calcarine fissure of the occipital lobe
above
lower visual field projects ________ the calcarine fissure of occipital lobe
monocular blindness
Common causes include glaucoma, optic neuritis, elevated intracranial pressure
Binasal Hemianopia
-may be due to ICA aneurysms
-lesion at one side of the optic chiasm
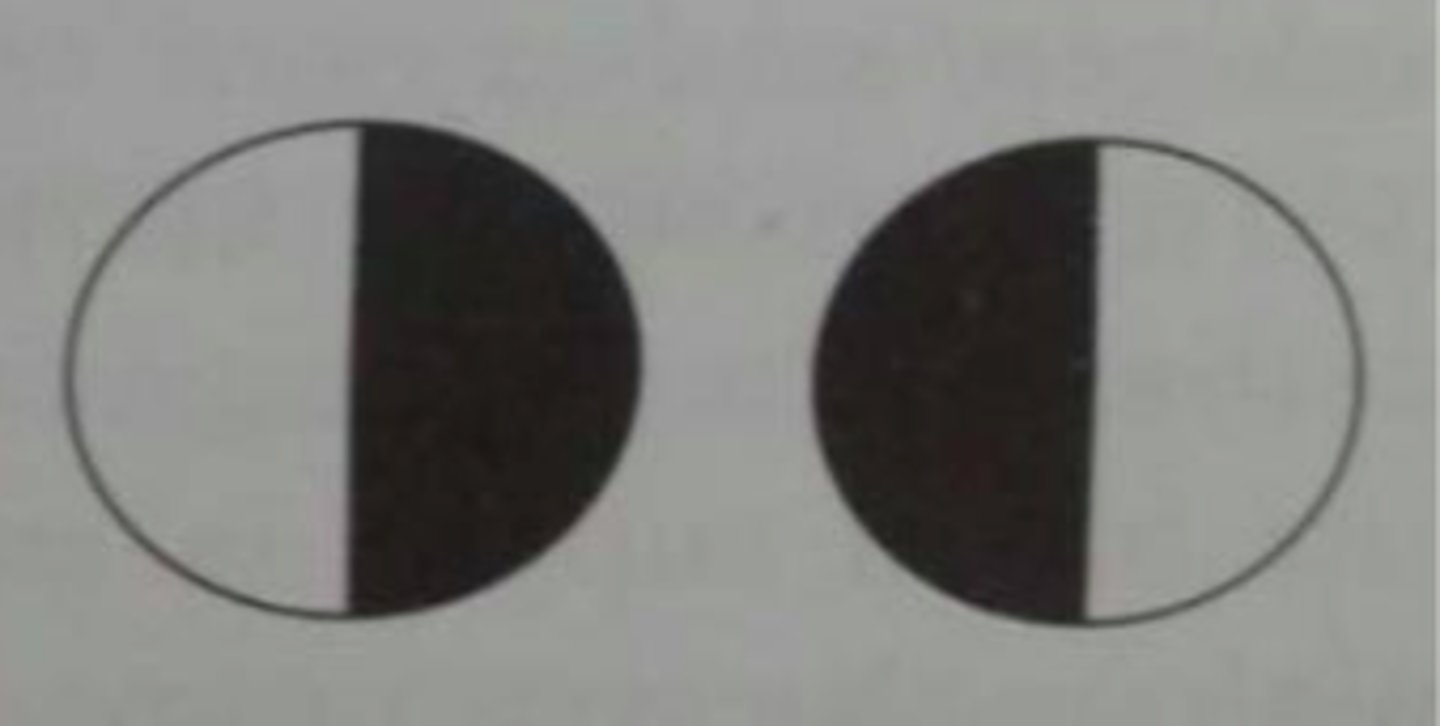
bitemporal hemianaopia
-damage to the optic chiasm, typically asymmetrical loss
-common lesions in this area include pituitary adenoma, meningioma, craniopharyngioma, and hypothalamic glioma
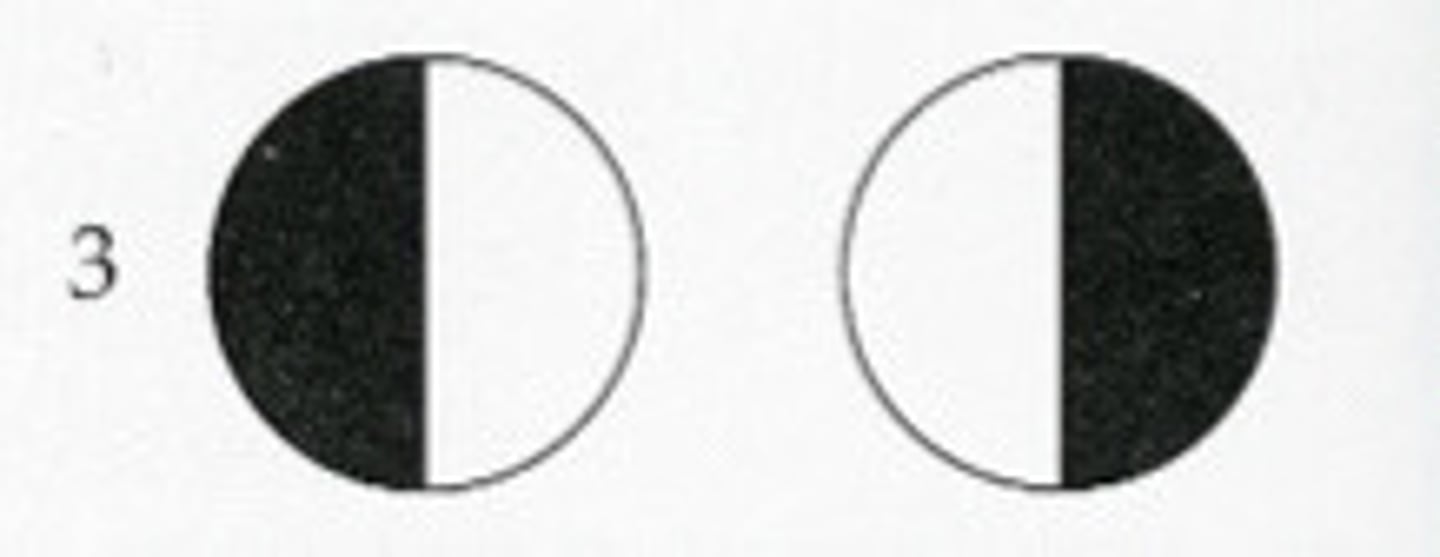
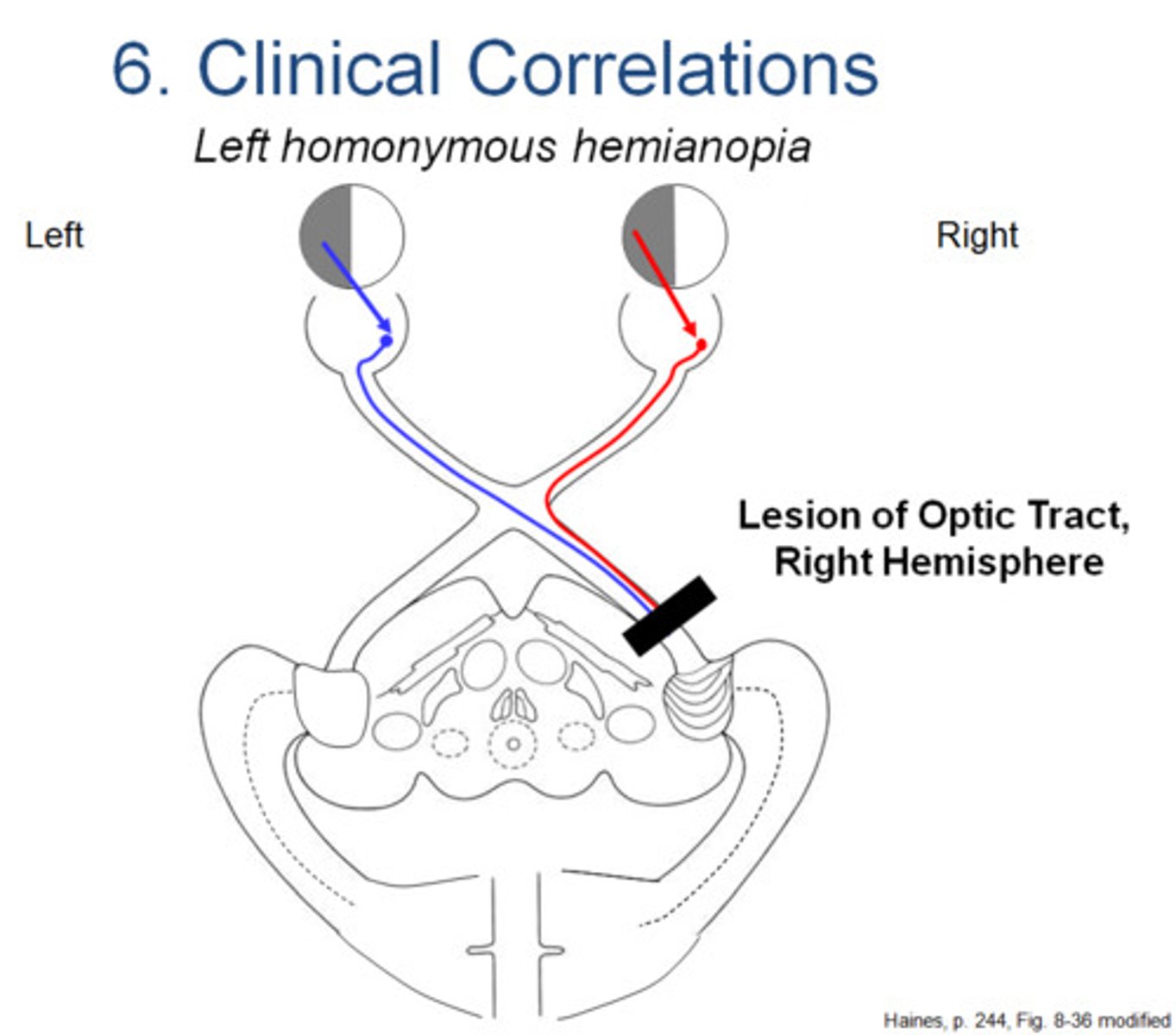
homonymous hemianopia
-lesion to the optic tract and Lateral geniculate nucleus (LGN)
-lesions include infarct to anterior choroidal arteries supplying optic tract, demyelination, or tumors; or lesions to the LGN
superior homonymous quadrantanopia
"Pie in the sky" - Damage to inferior optic radiation; Lesions of the optic radiations include infarcts, tumors, demyelination, trauma, and hemorrhage
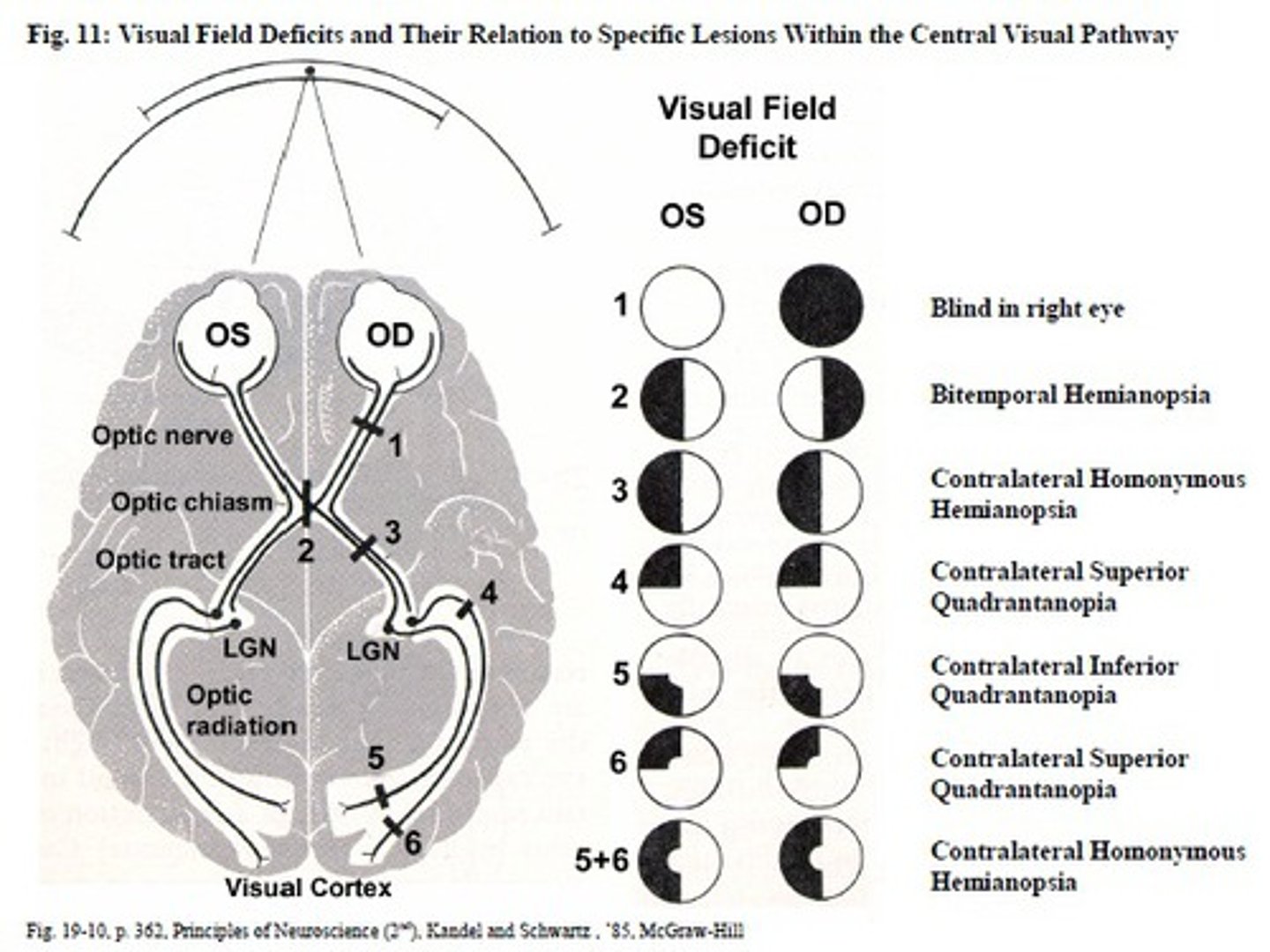
inferior homonymous quadrantanopia
"Pie on the floor" - Damage to superior optic radiation; Lesions of the optic radiations include infarcts, tumors, demyelination, trauma, and hemorrhage

damage to cortex with macular sparing
what causes this visual deficit

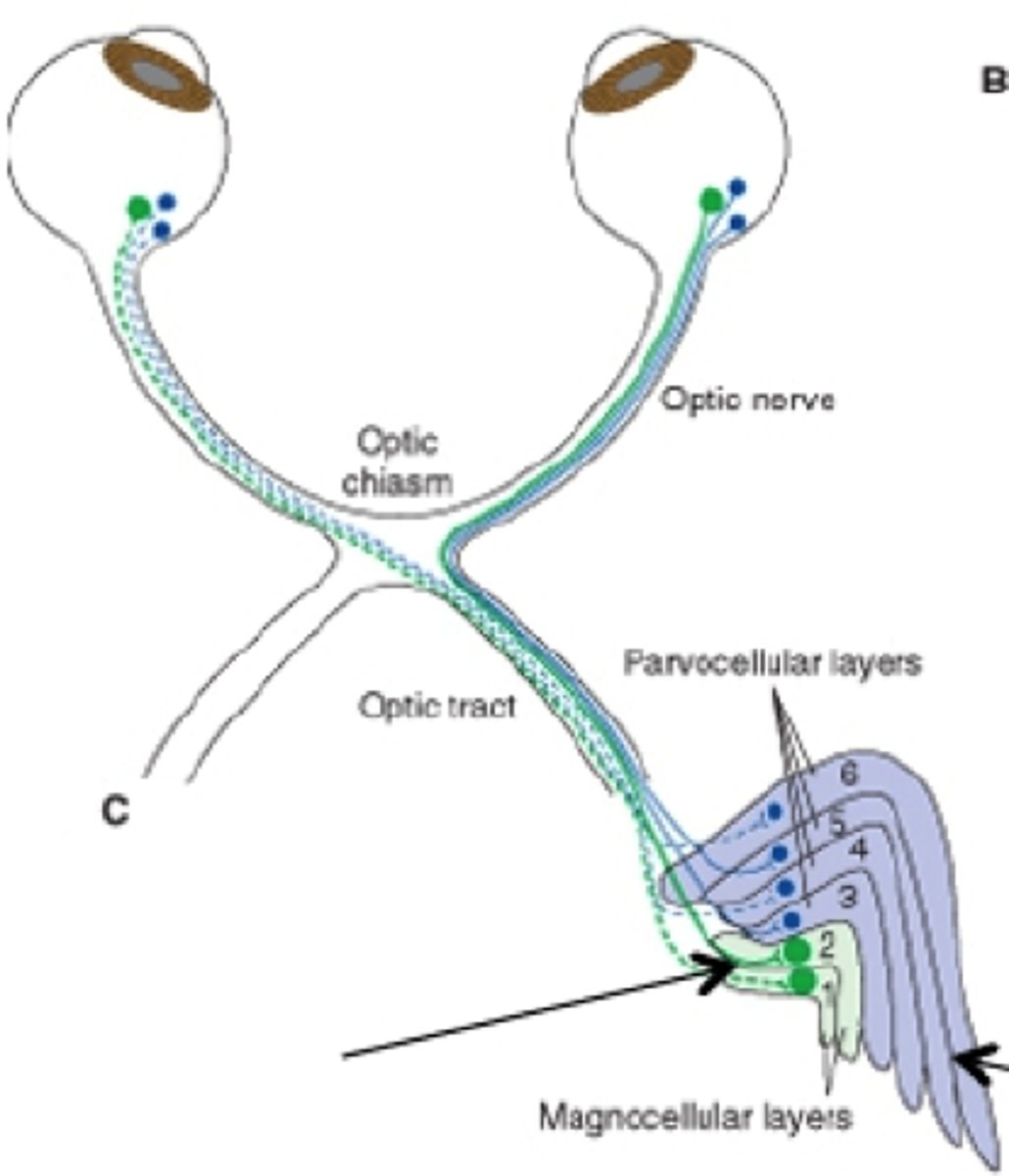
magnocellular layers
-layers 1 and 2 or LGN
-contain large neuron cell bodies
parvocellular layers
-layers 3-6 of LGN
-contain small cell bodies
Y retinal fibers
-fibers (mostly from rods) that terminate in the Magnocellular layers of the LGN
X retinal fibers
-fibers from cones that terminate in the parvocellular layers of the LGN
the ipsilateral temporal retina
layers 2,3, and 5 of the LGN receive input from
the contralateral nasal retinaa
layers 1, 4, and 6 of the LGN recieve input from
monocular
the neurons in the LGN are
binocular
the neurons in the striate cortex are
ocular dominance columns
-axons at the LGN terminate in separate, alternating layers called
stereopsis
-mixing of pathways at striate cortex; improves our ability to have depth perception
retinogeniculate pathway
•Parallel pathways
•Convey distinct types of information to initial stages of cortical processing
ventral , magnocellular layer of LGN
-contain large neurons that carry info from rods
-M-retinal ganglion cells terminate here
magnocellular layer of LGN
lesion here reduces ability to perceive rapidly changing stimuli
dorsal multi-layers (parvocellular layers of LGN)
-contains small neurons that carry information from cones
-P-retinal ganglion cells terminate here
parvocellular layers of LGN
lesion here results in loss of visual acuity and color perception
bilateral consensual closing of eyelids
corneal reflex: tactile stimulation of the cornea should result in
•Ophthalmic division of CN V to spinal trigeminal nucleus
afferent response of corneal reflex
CN VII via facial nucleus
efferent response of corneal reflex
intermediolateral column-->sympathetic trunk-->superior cervical ganglion
pathway of sympathetic innervation to the eye
internal carotid artery
CN V1
sympathetic fibers travel with ______, then hop on ______ to enter orbit
-pupil dilation (iris radial muscle)
-eyelide elevation (superior tarsal muscle)
function of sympathetics to the eye
pretectal neurons-->edinger-westphal nucleus
-fibers travel to ciliary ganglion via CN III
-postganglionic fibers travel to eye via ciliary nerve
pathway of the parasympathetic innervation to the eyes
pupil constriction and lens focus
action of parasympathetics to the eye
-light impinges on retina
-impulses pass from CN II to pretectal nuclei
-secondary impulses pass to bilateral edinger-westphal nucleus
-signals pass back through CN III parasympathetic nerves
-sphincter of both iris/pupil constricts
pupillary light reflex in light
light reflex inhibited, permits pupil dilation
pupillary light reflex in darkness
Marcus Gunn Pupil (Relative Afferent Pupillary Defect)
swinging the flashlight into the R eye causes appropriate consensual response; however, introducing light to the left eye causes relatively large pupils

aniscoria
unequal pupils
horner syndrome
symptoms:
•Pupil constriction (miosis)
•Drooping eyelid (ptosis)
•Lack of sweating (anhidrosis)
Congenital Horner's Syndrome
-horner's syndrome from perinatal damage to sympathetic trunk
central horner's syndrome
horner's syndrome from between hypothalamus and sympathetic axons
peripheral horner's syndrome
horner's syndrome that result from lesion to sympathetic trunk, superior cervical ganglion, or carotid artery
hereditary horner syndrome
autosomally dominant inherited horner syndrome
oculomotor nerve lesion
pupil dilation; eye deviates inferiorly and laterally due to muscle paralysis; resulting in double vision; eyelid droops (ptosis); blurred vision due to loss of accommodation
Argyll Robertson pupil
-small, irregular and asymmetrical pupils that fail to react to light but constrict on accommodation
-accommodation intact
-often seen in CNS syphilis or diabetes
argyll-robertson pupil
potentially caused by lesions to the pretectal nuclei in the midbrain
Adie Tonic Pupil
•Sluggish, segmental pupillary responses to light but constrict on accommodation
•Typically, unilateral and common in females
-accommodation intact
adie-tonic pupil
caused by degeneration of ciliary ganglia and postganglionic parasympathetic
holmes-adie syndrome
adie-tonic pupil is aka