Lower Respiratory Tract Infections
1/72
Earn XP
Description and Tags
One of the most frequent reasons people go to a doctor or clinic worldwide
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
What are the common pathogens that cause acute bronchitis?
~90% of cases are respiratory viruses
rarely bacterial!
Bronchitis is the inflammation of the:
epithelial lining of the large airways
What is the hallmark symptom of acute bronchitis?
Cough
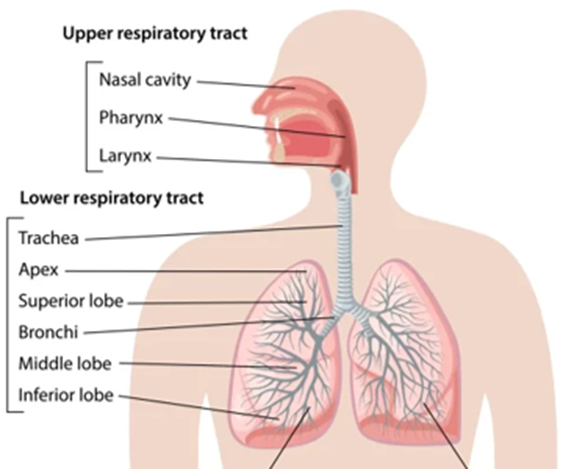
Location of lower Respiratory Tract Infection (LRTI) vs upper?
lower - airways and lungs below the trachea
upper would be nose & throat
What test is gold standard to diagnose acute bronchitis?
Acute bronchitis is mostly diagnosed clinically, meaning based on symptoms, not tests…
it starts like a URI (cold) that is a dry cough that later becomes productive cough —
RULE OUT ASTHMA, COPD, PNEUMONIA
Goal of actute bronchitis treatment? What can we use?
symptom management…. acute bronchitis is self-limiting!!
note pharmacological in image… mucinex and dextromethorphan don’t do much
Use of antibiotics is STRONGLY DISCOURAGED in acute bronchitis…when would we actually use?
if persistent fever/sx>5-7 days, or if predisposed to bacterial infections (immunocompromised)
What is the main difference in etiology of acute vs chronic bronchitis?
chronic is often bacterial!!
List the common pathogens that may cause chronic bronchitis:
h. influenzae
moraxella catarrhalis
strep pneumo
(FYI) ——————————————————
Describe the pathogenesis of chronic bronchitis: why does excess mucus occur? Why does scarring/fibrosis occur?
Breathing in irritants or infections for a long time (like smoke) damages →
The airway walls get thicker and the cells that make mucus (goblet cells) increase.
The mucus glands get bigger, so much more mucus is produced.
That extra mucus builds up in the small airways and can plug them, making it harder to breathe.
Over time, this ongoing irritation can cause tissue damage, scarring, and fibrosis in the lungs.
What is the hallmark symptom of chronic bronchitis?
productive cough
One situation of 1st 20 slides that is one of the BIGGEST THINGSTO KNOW for antibiotic treatment of chronic bronchitis standpoint is
-T/F - We can use abx in cases of acute exacerbations of chronic bronchitis
TRUE
there ARE situations where you want to use antibiotics in ACUTE exacerbations of CHRONIC bronchitis … not same as acute bronchitis!
What is the definition of chronic bronchitis?
Presence of a chronic productive cough for more than 3 consecutive months of the year for 2 consecutive years
How do we treat chronic bronchitis?
nonpharm + optimization of COPD therapy (if present), vaccines, and SABA
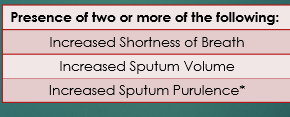
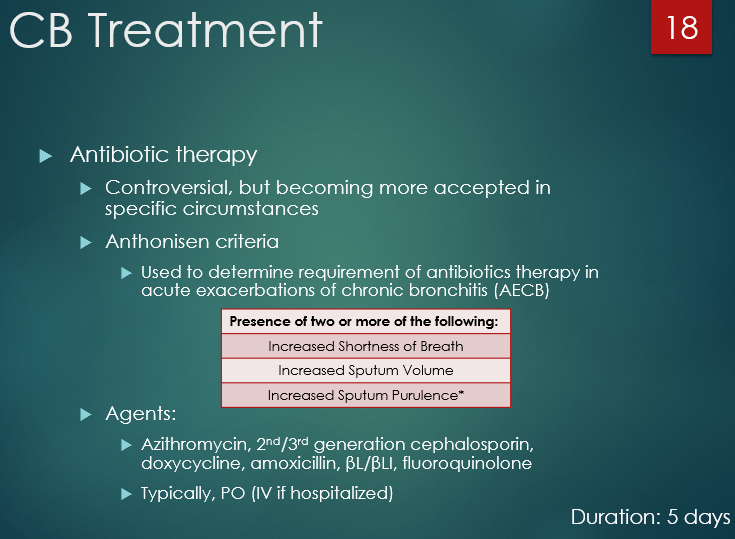
What are the Anthonisen criteria?
Presence of two or more of the following:
increased SOB
increased sputum volume
increased sputum purulence*
*some references require presence of this item for treatment
When do we initiate antibiotics for (acute exacerbation of) chronic bronchitis? What abx can we use to treat chronic bronchitis?
when 2/3 of Anthonisen criteria met
uAzithromycin, 2nd/3rd generation cephalosporin, doxycycline, amoxicillin, βL/βLI, fluoroquinolone , usually PO
What is bronchiolitis?
uAcute viral infection of the small airways (bronchioles)
Most common pathogen in brochiolitis:
RSV (75% of cases)
What are the s/s of bronchiolitis? How is it diagnosed?
diagnose based on sx -
starts like a cold then cough + fast/troubled breathing
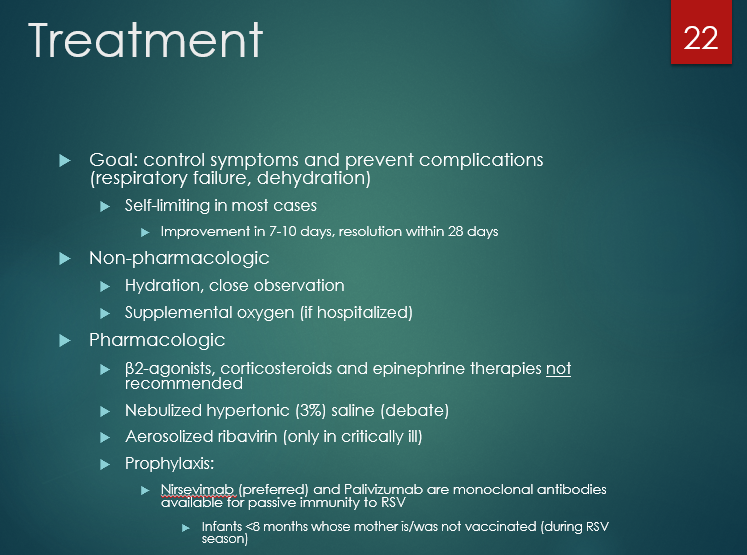
How do we treat bronchiolitis?
mainly supportive care (fluids/hydration/oxygen if hospitalized)
-(see image) COPD-like therapy not recommended but often inappropriately used
Leading infectious causes of death in adults and children worldwide
pneumonia
What is pneumonia (e.g., it is an infection of the _____ of the lungs)? What is the main complication we see?
infection of the alveoli of the lungs that results in inflammation and fluid accumulation within the lungs
What are the three main modes of pneumonia acquisition? Which is major?
direct inhalation of droplets
aspiration of oropharyngeal contents
hematogenous spread from another infection site
Define CAP
•Pneumonia developing outside the hospital or < 48 hours after hospital admission
Define HAP
Pneumonia developing > 48 hours after hospital admission
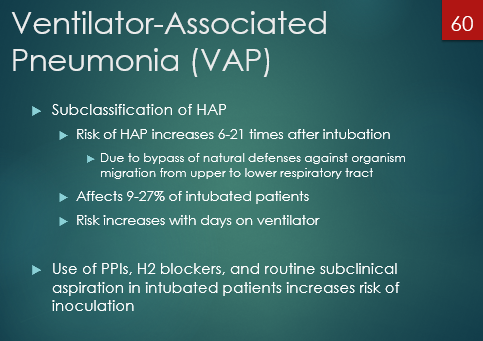
Define VAP
Pneumonia developing > 48 hours after endotracheal intubation
(FYI) most important of the pneumonias— why??
CAP - 500,000 hospitalizations, 20B in healthcare spending, ~50k deaths per year
What are some of the risk factors for CAP? List a few:
>65 y/o
DM
comorbidities (pulm, CV, renal)
smoking/alcohol
What is the main etiology of CAP? Viral? Bacterial?
about a 50-50 split viral vs bacterial
What is the most common CAP pathogen?
S. pneumoniae (35%)
List the common CAP pathogens: (he said will be a NAPLEX and exam question)
strep pneumo
M. pneumo
C. pneumo
L. pneumo
h. influenzae
How can we kind of differentiate bacterial vs viral pneumonia (CAP) based on sx?
bacterial has more of an abrupt onset wheras viral is more gradual… bacterial usually much more severe in sx
List a few of the s/s of CAP
abrupt onset of fever, chills, dyspnea, and productive cough
rust colored sputum, hemoptysis
pleuritic chest pain (know your different chest pains!)
pleuritic - sharp pain in chest worse with inspiration/cough
cardiac - pressure/squeezing not effected by breathing
How to distinguish viral vs bacterial CAP based on procalcitonin
procalcitonin only elevated in bacterial … much more specific than white blood cell count
Atypical pneumonia
pneumonia caused by an atypical organism (e.g. M. pneumoniae and C. pneumoniae)
How would CAP look on a physical exam?
tachypena, tachycardia, hypoxia
inspiratory crackles, diminished breath souds
chest wall retraction
- if pt resents w/ pneumonialike symptoms, you should initiate antibiotic therapy… but what do we use procalcitonin for?
for DEESCALATION purposes… we are not using it to decide whetehr to start antibiotics!
(reason - takes time to peak… cann take 6-24 hours for procalcitonin to peak… but bacterial is abrupt onset so can be sticky if we were using it for that….)
uProcalcitonin <____ ng/mL suggests a “low” likelihood of bacterial etiology
uProcalcitonin <0.25 ng/mL suggests a “low” likelihood of bacterial etiology
What to now about urinary antigen testing
very good PPVs… (positive predictive values).. not very good NPVs…
(meaning if test positive - prob real…. if negative→ does not rile anything out reliably)
What two pathogens are urinary antigen testing available for?When do we actually do this in practice?
strep pneumo
legionella pneumophilia
rec’d for severe cap or (legionella) if in certain travel areas or outbreaks
What to know about sputum cultures for pathogen identification in CAP
low sensitivity and specificity…but are cases where it is recommended (see image)
(how do we even know the sputum is coming from the alvioli of the lungs? how do we know it hasn’t picked up contaminants along the way?)
(FYI) explain why MRSA nasal PCR has a good NPV but poor PPV
99% neg predictive value bc if its not in your nose its not in lungs
shitty PPV because its prob just in your nose
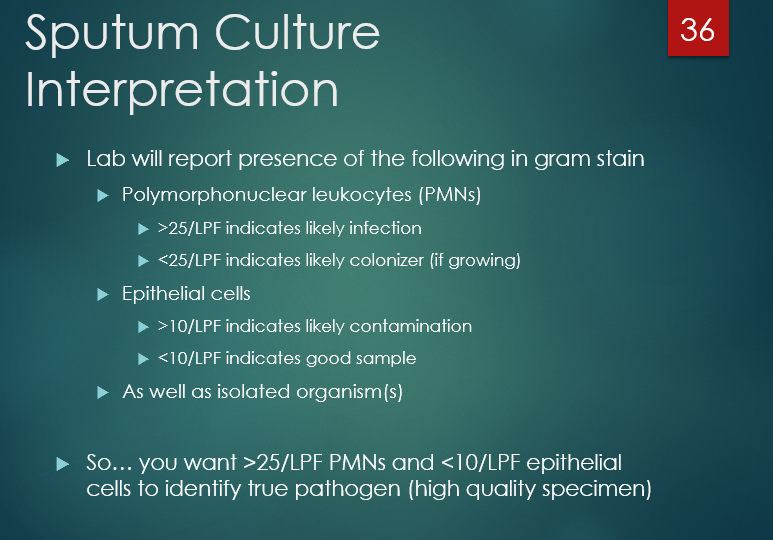
The lab culture will report the presence of the following in gram stain:
PMN count
Epithelial cells
how can we interpret?
PMN:
>25/ LPF = likely infection
<25/ LPF= likely colonizer
Epithelial:
>10/LPF = likely contamination
<10 /LPF = goodsample
uSo… you want >25/LPF PMNs and <10/LPF epithelial cells to identify true pathogen (high quality specimen)
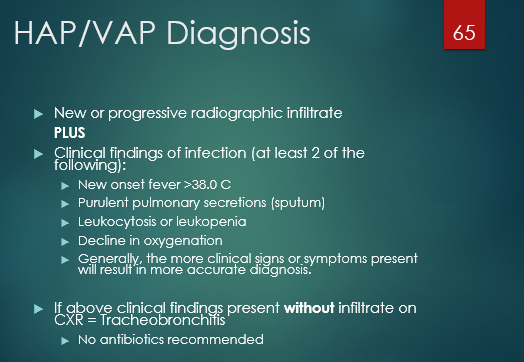
How is pneumonia diagnosed?
What two things are needed for pneumonia diagnosis?
Clinical diagnosis + radiographic evidence
Signs/symptoms consistent with pneumonia (sx + WBC > 12,000; hypoxemia (ABG) elevated procalcitonin)
Chest X-ray findings consistent with pneumonia
What is the gold standard imaging test for pneumonia?
Chest X-ray
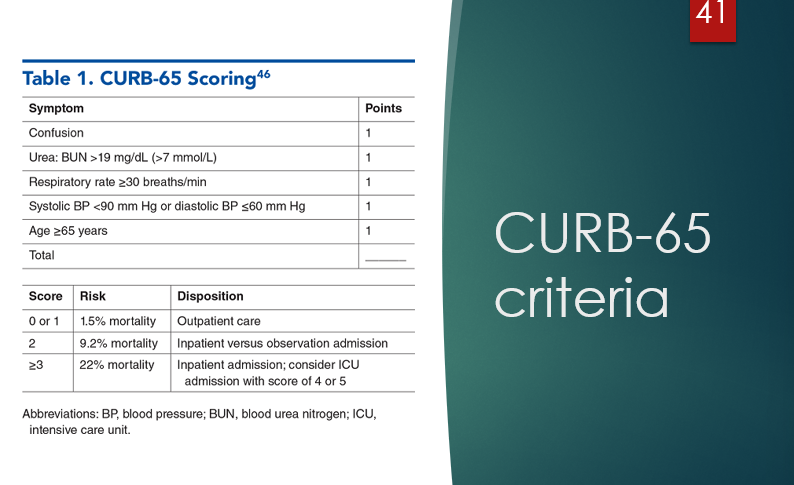
What is the CURB-65 Criteria? List the criteria and what scores would mean… why do we do this?
(WILL come up on exam and in practice)
this is how decisions are made from an admissions standpoint generally 2 or more = treat inpatient….. if less than that we can be treat outpatient
Yes = 1 point
Confusion
BUN >19
Resp. rate ≥ 30 breaths/min
Syst BP <90 or diastole ≤ 60
age ≥ 65
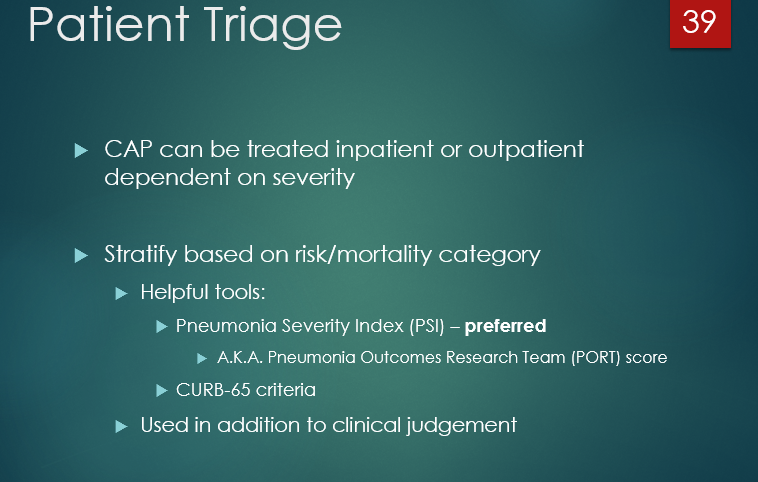
What is the preferred triage method for determining if CAP is to be treated inpatient or outpatient?
A. CURB-65
B. PSI
B. Pneumonia Severity Index (PSI) – preferred
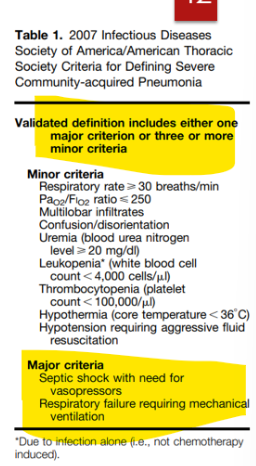
How do we define CAP as severe?
What are the major criteria for CAP?
(“will not be tested on minor - just know major”)
Severe = 1 major or 3+ minor criteria present
MAJOR:
septic shock with need for vasopressors
respiratory failure requiring mechanical ventilation
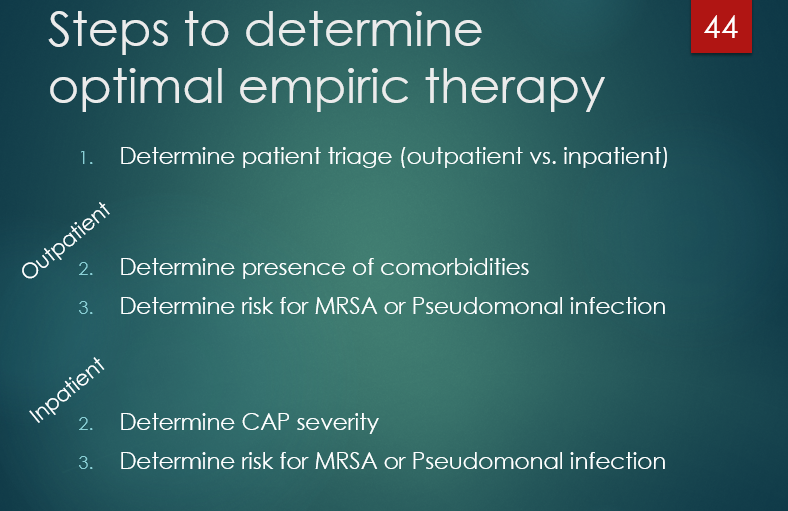
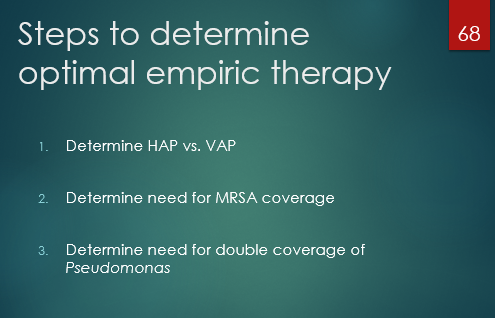
If looking at a case question - what are the things we should be asking?
Step 1 is always determine triage
what are steps 2 and 3 if outpatient?
what about steps 2-3 if need admitted?
1- DETERMINE TRIAGE.
If outpatient-
(2) - comorbidity check
(3) - determing MRSA and pseudomonal risk
if inpatient -
(2) - determine CAP severity
(3) - determine risk for MRSA or pseudomonal infection
fyi - What are the respiratory fluoroquinolones?
Levaquin and Avelox
Respiratory fluoroquinolones are the ones with good coverage of Streptococcus pneumoniae (a major cause of pneumonia).
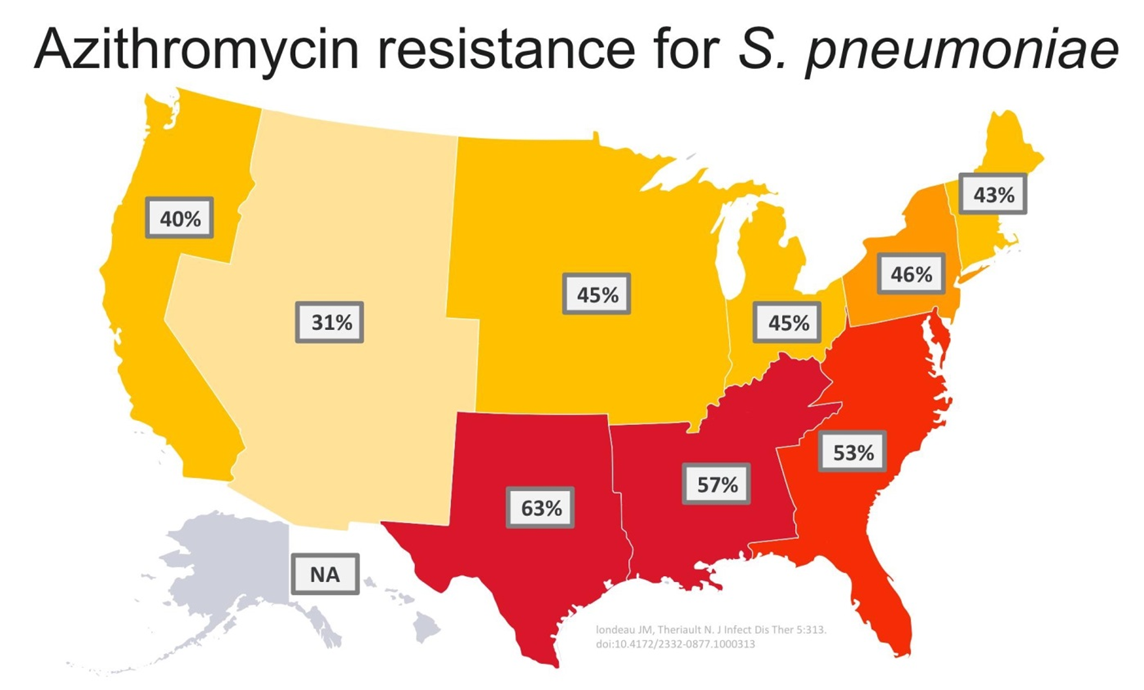
When should we use macrolidesas monotherapy based on local s. pneumo resistance?
pretty much never at this point
What do we do if CAP pt tests positive for flu
give oseltamivir despite when flu came about
If a patient with CAP tests positive for flu, why are we giving antibiotic therapy?
-because viral infection is MAJOR risk factor for bacterial infection
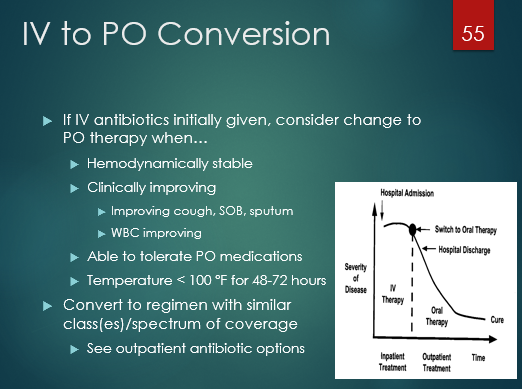
In inpatient when do we transition to oral?
hemodynamically stable (BP, HR normal)
clinically improving (sx improving, WBC improving)
obv can tolerate PO
temp <100 for 48-72h
T/F - treatment of HAP and VAP is basically the same
true
Strongest predisposing factor for HAP
mechanical ventillation
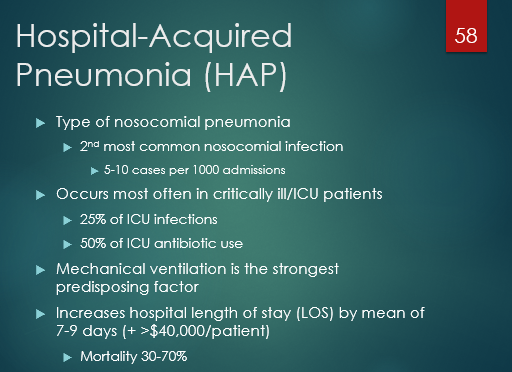
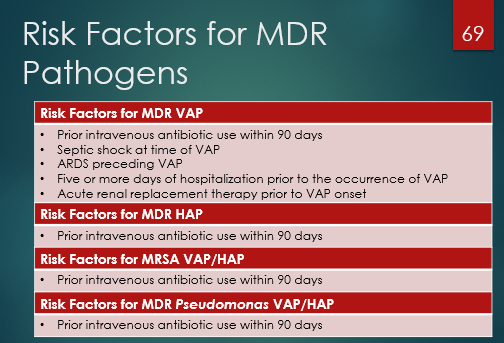
What are some big risk factors for HAP? List at least two.
intubation (6-21x risk), acid suppressing agents
also (low yield)
uWitnessed aspiration
uCOPD, ARDS, or coma
uAdministration of antacids, H2 antagonists, or PPIs
uSupine position
uEnteral nutrition, nasogastric tube
uReintubation, tracheostomy, or patient transport
uHead trauma, ICP monitoring
uAge > 60 years
see image
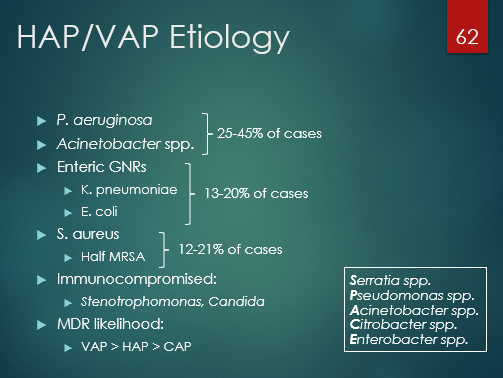
Which enteric gram negatives are the main ones in HAP/VAP etiology?
SPACE pathogens…
Serratia
Psuedomonas
Acinetobacter
Citrobacter
Enterobacter
List some of the pathogens involved in the etiology of HAP/VAP
SPACE grm negs + s. aureus
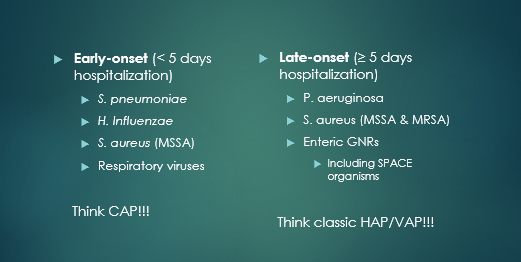
Differentiate early onset HAP/VAP vs late… how would we treat (what to think about)?
early = < 5 days in hospital… treat like CAP
late = 5 or more days in hosp… think hospital/resistant organisms
*early-onset = better prognosis, less chance of drug resistance. Late = usually resistant bugs
difference between diagnosis of CAP vs HAP/VAP - general
CAP is more loose/more reliant on symptoms and Dr. judgemnt…
HAP/VAP requires infiltrate on CXR and 2 or more clinical signs
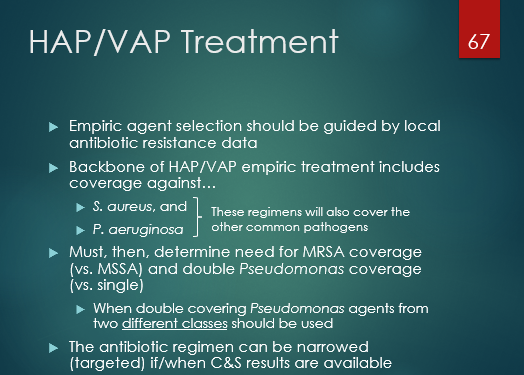
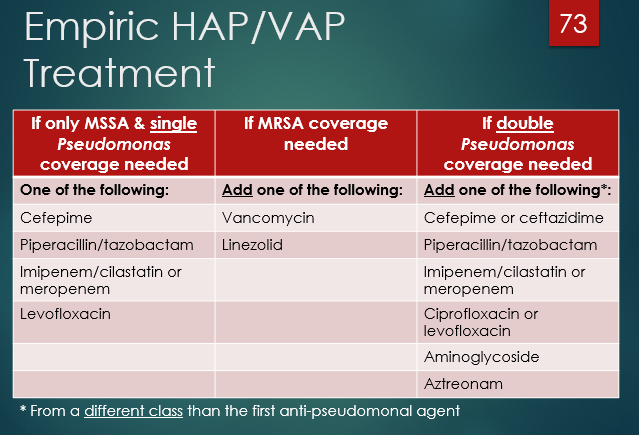
Any time you are treating a HAP/VAP case, you need to AT LEAST make sure you are providing coverage of what organisms?
s. aureus
p. aeruginosa
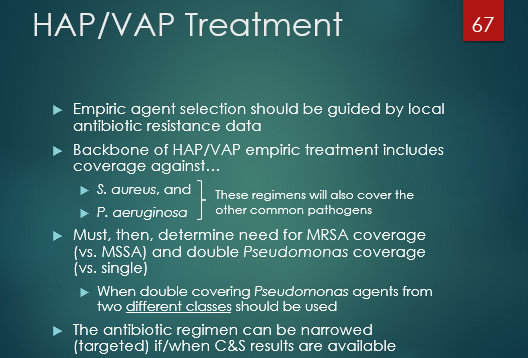
“too much of class got this wrong on last2 exams”- when double covering pseudomonas, TWO AGENTS with coverage are needed. What is an important caviat?
THESE NEED TO BE OF DIFFERENT CLASSES! Vanco counts as a B-lactam as well
add algorithm
add
In empiric HAP treatment, when do we cover MRSA?
uCover MRSA ALWAYS (See 2) and image
Patient with risk factor for MDR/MRSA, or
In units where >20% of S. aureus isolates are methicillin resistant, …… EVERYWHERE
Prevalence of MRSA is unknown, or
Patient at high risk for mortality
Need for ventilatory support or septic shock
uOtherwise, cover MSSA
In empiric VAP treatment -when do we DOUBLE cover pseudomonas?
uDouble cover Pseudomonas if…
uPatient with risk factor for MDR, or
uIn unit where >10% of gram-negative isolates are resistant to an agent being considered for monotherapy, or
uSusceptibility rates are unknown
uOtherwise, single cover Pseudomonas
know the logic
add
Duration recommended for pretty much all cases of HAP & VAP
7 days
What is aspiration pneumia?
uAspiration causes physical damage/chemical burn to protective mucosal lining of respiratory tract
like falling and scraping knee… u don’t always get skin infection, but it puts you at risk bc you’re destroying that physical barrier… just like scarping your knee it rarely truly causes something to worry about
T/F - aspiration pneumonia is one of the most overtreated things you’ll see from stewardship perspective
true
What are the risk factors for aspiration pneumonia?
anything that causes aspiration or impaired consciousness (remember kaminski enteric access endo lectures about aspiration risks with tubes)
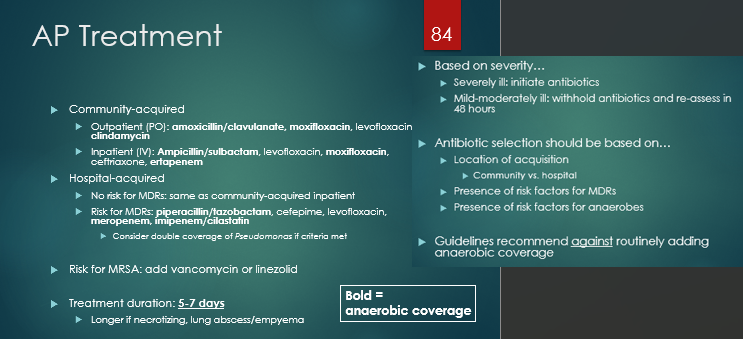
How do we treat aspiration pneumonia?
withhold abx and re-assess unless severely ill…
(see image - guidelines have no consensus…he said DO NOT MEMORIZE…. just treat like CAP if community acquired; if HAP treat like hospital acq, etc)